
Abstract
A series of studies have revealed that IL-6 has pleiotropic activity in various cells and that its deregulated expression is responsible for the development of multiple autoimmune inflammatory diseases. A humanized antibody against the IL-6 receptor, tocilizumab, has exhibited outstanding therapeutic efficacy against rheumatoid arthritis, juvenile idiopathic arthritis, Castleman’s disease, and other autoimmune inflammatory diseases, leading to its clinical use for treatment of several diseases. These findings indicate that overproduction of IL-6 is responsible for the pathogenesis of autoimmune inflammatory diseases, in which an imbalance between Th17 cells and regulatory T cells and autoantibodies play central roles. Recent studies have suggested that IL-6 blockade therapy can rectify these underlying immunological abnormalities in autoimmunity. However, the causes of deregulated IL-6 production in these diseases remain unknown. A novel IL-6-regulating molecule, Arid5a, specifically stabilizes IL-6 mRNA and sustains its overproduction; thus, Arid5a plays an important role in promoting inflammation and autoimmune diseases. Indeed, in Arid5a-knockout mice, experimental autoimmune encephalomyelitis does not develop, and lipopolysaccharide stimulation does not induce elevated expression of IL-6. Arid5a can counteract the destabilizing effect of a regulatory RNase, Regnase-1, on IL-6 mRNA; Regnase-1 knockout mice spontaneously develop various fatal autoimmune diseases. Further analyses of these RNA-binding proteins as well as other regulatory molecules for IL-6 expression are expected to elucidate the molecular mechanisms underlying deregulated synthesis of IL-6, and facilitate investigations of the pathogenesis of specific diseases.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
Introduction
Interleukin 6 (IL-6), a prototypical cytokine with redundant and pleiotropic activities, contributes to host defense against infections and tissue injuries by inducing the acute-phase response and activating immune responses and hematopoiesis. However, excessive or continuous IL-6 production plays a pathological role in an acute severe life-threatening complication, the so-called cytokine storm, and in various chronic autoimmune inflammatory diseases.
A humanized anti-IL-6 receptor (IL-6R) monoclonal antibody (Ab), tocilizumab, was developed on the basis of the idea that IL-6 blockade represents a novel therapeutic strategy for such diseases. Worldwide, clinical trials have proven that tocilizumab is highly efficacious for the treatment of intractable autoimmune inflammatory diseases, including rheumatoid arthritis (RA), systemic and polyarticular juvenile idiopathic arthritis (JIA), and Castleman’s disease, leading to its approval for the treatment of these diseases. Moreover, numerous reports regarding off-label use of tocilizumab strongly suggest that an IL-6 blockade strategy is a promising therapeutic approach for treatment of other diseases. In this chapter, we will highlight the pathological role of IL-6 in autoimmune inflammatory diseases, offer perspectives on the future of IL-6 blockade therapy, and discuss the mechanisms potentially responsible for deregulated IL-6 overexpression.
Pleiotropic Function of IL-6
The gene encoding B cell stimulatory factor 2 (BSF-2), which induces the differentiation of activated B cells into Ab-producing cells, was successfully cloned in 1986 [1]. Later, BSF-2 was found to be identical to hepatocyte-stimulating factor, hybridoma growth factor, and interferon (IFN)-β2, and the molecule was subsequently renamed IL-6 [2]. Human IL-6 consists of 212 amino acids with a 28–amino acid signal peptide and a core protein of about 20 kDa. Natural IL-6 is 21–26 kDa with glycosylation, although the glycosyl moiety does not affect its biological activity.
Effect of IL-6 in Immune Response
IL-6, originally identified as BSF-2, promotes the differentiation of activated B cells into immunoglobulin (Ig)-producing plasma cells. IL-6 also acts as a growth factor for myeloma cells, and some myeloma cells spontaneously produce IL-6 [3]. Moreover, IL-6 promotes the survival of the plasmablasts, cells that secrete immunoglobulin or pathological autoantibodies, e.g., anti-aquaporin 4 (AQP4) in patients with neuromyelitis optica (NMO) [4]. Thus, continuous overexpression of IL-6 results in autoantibody production as well as hypergammaglobulinemia.
IL-6 also affects T cells. IL-6 is one of the factors that determine how naïve CD4+ T cells differentiate into particular effector T cell subsets. IL-6 in combination with transforming growth factor (TGF)-β preferentially induces differentiation into Th17 cells, whereas IL-6 inhibits TGFβ-induced regulatory T cell (Treg) development. The resultant predominance of Th17 cells over Treg cells may be responsible for the breakdown of immunological tolerance, and may therefore be pathologically involved in the development of autoimmune inflammatory diseases [5]. Indeed, in several autoimmune disease models, IL-6 blockade at the priming step suppresses the development of the imbalance in antigen-specific effector T cell subsets, and thus development of the autoimmune diseases themselves, irrespective of the antigens used for immunization [6–8]. IL-6 also promotes T follicular helper cell differentiation as well as production of IL-21, which also promotes immunoglobulin synthesis [9].
Effect of IL-6 in Acute-Phase Response
IL-6 is a major regulator of the initiation of acute-phase responses. IL-6 induces hepatocytes to produce acute-phase proteins such as C-reactive protein (CRP), serum amyloid A (SAA), fibrinogen, hepcidin, and α1-antichymotrypsin, whereas it inhibits the production of fibronectin, albumin, and transferrin [10]. CRP and SAA are biological markers of inflammation occurring somewhere in the body. Administration of tocilizumab completely normalizes the serum levels of these proteins, indicating that their synthesis depends primarily on IL-6 [11, 12]. Increased levels of acute-phase proteins signal a state of emergency and contribute to host defense, whereas continuous expression of high levels of SAA or hepcidin leads to complications of chronic inflammatory diseases, such as amyloid A amyloidosis or anemia, respectively [12, 13].
Other Effects of IL-6
IL-6 also acts on other cells [2, 14]. IL-6 produced by bone-marrow stromal cells stimulates synovial fibroblasts to express the receptor activator of the nuclear factor kappa beta (NF-κB) ligand (RANKL), which is indispensable for the differentiation and activation of osteoclasts. Osteoclast activation leads to bone resorption and osteoporosis [15]. IL-6 also promotes production of vascular endothelial growth factor by fibroblasts, leading to angiogenesis and increased vascular permeability, which are pathological features of inflammatory lesions observed in synovial tissues of RA and in other conditions [16]. IL-6 promotes the production of collagen in dermal fibroblasts and their differentiation into myofibroblasts, which are predominantly responsible for skin fibrosis in patients with systemic sclerosis (SSc) [17]. Moreover, IL-6 can interact with vascular endothelial cells, the endocrine system including the hypothalamic–pituitary–adrenal axis, neuropsychological systems, and other systems.
IL-6 Signaling Systems
The IL-6 signaling cascade is triggered by binding of IL-6 to its specific receptor, IL-6R [18]. The receptor constitutes the IL-6-binding chain, which exists in two different forms, 80 kDa transmembrane IL-6R and 50–55 kDa soluble IL-6R (sIL-6R) [18, 19], and the 130 kDa gp130 constitutes the signal-transducing chain [20]. The expression of transmembrane IL-6R is limited to cells such as hepatocytes and leukocytes, whereas sIL-6R is present in blood and tissue fluid. After IL-6 binding to either transmembrane IL-6R or sIL-6R, the resultant complex induces homodimerization of gp130 [21] and triggers a downstream signal cascade. The pleiotropic effects of IL-6 are due to the broad range of gp130 expression on various cells [22]. IL-6R is the specific receptor for IL-6, whereas the signal-transducing chain gp130 is shared by other members of the IL-6 family of cytokines, including leukemia inhibitory factor, oncostatin M, ciliary neurotrophic factor, IL-11, cardiotrophin 1, cardiotrophin-like cytokine, IL-27, and IL-35. The findings that all IL-6 family members use the same molecule (gp130) for signal transduction resolved a long-standing mystery regarding why these cytokines exhibit functional redundancy [18, 22, 23].
Activation of gp130 leads in turn to activation of two downstream signaling cascades, the Janus kinase (JAK)-signal transducer and activator of transcription 3 (STAT3) pathway and the JAK-SH2-domain-containing protein tyrosine phosphatase-2-mitogen-activated protein kinase pathway. Various IL-6-responsive genes are induced by activation of the transcription factor STAT3, which also controls the expression of suppressor of cytokine signaling 1 (SOCS1) and SOCS3. In this context, SOCS1 binds to tyrosine-phosphorylated JAK [24], and SOCS3 binds to tyrosine-phosphorylated gp130 [25], thereby terminating IL-6 signaling via a negative-feedback loop.
Regulatory Mechanisms of IL-6 Synthesis
In the serum of healthy individuals, the IL-6 level is less than 5 pg/ml; however, the IL-6 concentration increases dramatically during emergent events such as infections and tissue injuries. At sites of infections, neutrophils, monocytes, and macrophages promptly produce IL-6 following through recognition of components of exogenous pathogens via pathogen-associated molecular pattern receptors [26]. In cases of non-infectious inflammation caused by burns or trauma, IL-6 is produced by these immune cells through the stimulation of damage-associated molecular patterns, which are released from damaged or dying cells. Besides immune-competent cells, other types of cells, including endothelial cells, mesenchymal cells, fibroblasts, and cancer cells, are also able to synthesize IL-6 [14].
When the emergent stimuli are completely removed from the host, the signal transduction cascade by IL-6-mediated activation is terminated through negative regulatory systems such as ligand-induced internalization, degradation of gp130, and recruitment of SOCS [24, 25], leading to normalization of the CRP level in serum. Accordingly, synthesis of IL-6 is tightly regulated at the transcriptional and post-transcriptional level.
Transcriptional and Post-transcriptional Regulation of IL-6
Several factors regulate the fate of IL-6 mRNA at either the transcriptional or post-transcriptional stage. The promoter region of the human IL-6 gene includes binding sites for cis-regulatory elements such as activator protein 1, interferon regulatory factor 1, a CCAAT enhancer binding protein β (C/EBPβ, also termed NF-IL6), specificity protein 1, and NF-κB [27, 28]. Stimulation of Toll-like receptor (TLR) with bacterial or viral pathogen components, or pro-inflammatory cytokines such as IL-1, IL-6, and TNF-α, can activate cis-regulatory elements, leading to IL-6 synthesis, whereas several microRNAs (miRs) directly or indirectly down-regulate IL-6 transcription. For instance, miR-155 interacts with the 3′-untranslated regions (UTR) of C/EBPβ to suppress C/EBPβ expression, whereas miR146a/b targets IL-1 receptor-associated kinase 1 to indirectly inhibit IL-6 transcription.
In general, the mechanisms of post-transcriptional regulation of cytokine expression target either the 5′-UTR of mRNAs to modulate initiation of translation or the 3′-UTR of mRNAs to modulate their stability [29, 30]. Several recently identified RNA-binding proteins and miRs regulate the stability of IL-6 mRNA [27, 28]. For instance, miR-26a binds to the 3′-UTR of IL-6 mRNA in hepatocellular carcinoma, suppressing the expression of STAT3 target genes. In addition, open reading frame 57 of Kaposi sarcoma-associated herpes virus competes with miR-608a for binding to the IL-6 mRNA, thereby stabilizing it.
One of the RNA-binding proteins that influence IL-6 expression, regulatory RNase-1 (Regnase-1, also known as Zc3h12a), interacts with the 3′-UTR of IL-6 mRNA, leading to its destabilization at steady state [31]. Regnase-1-deficient mice spontaneously develop autoimmune diseases with splenomegaly and lymphadenopathy. On the other hand, stimulation of IL-1R/TLR causes phosphorylation of Regnase-1 by the inhibitor of NF-κB (IκB) kinase complex, leading to its ubiquitination and degradation. The degradation of Regnase-1 is required for expression of IL-6 mRNA; however, re-expression of Regnase-1, which is induced by NF-κB activation, prevents excessive IL-6 production [32].
We recently identified an RNA-binding protein, AT-rich interactive domain-containing protein 5a (Arid5a), which interacts with the 3′-UTR and selectively stabilizes the IL-6 mRNA but not TNF-α or IL-12 mRNA [33]. Expression of Arid5a is dramatically upregulated in T cells under Th17-skewing conditions and in macrophages stimulated by lipopolysaccharide (LPS), IL-1β, and IL-6. Thus, there exists a positive-feedback loop between IL-6 and Arid5a. In untreated RA patients, expression of Arid5a is elevated in CD4+ T cells in the peripheral blood, whereas tocilizumab treatment decreases Arid5a expression [34]. Furthermore, Arid5a-deficient mice exhibit reduced serum IL-6 levels upon LPS challenge, and fail to develop experimental autoimmune encephalomyelitis. Arid5a counteracts the destabilizing function of Regnase-1 on IL-6 mRNA, suggesting not only that the balance between Arid5a and Regnase-1 is an important determinant of the stability of IL-6 mRNA, but also that the predominance of Arid5a expression over Regnase-1 promotes inflammatory processes and development of autoimmune diseases [27, 35] (Fig. 1).

Regulatory mechanism of IL-6 production. In the innate immune response, pathogen-associated molecular patterns are recognized by pathogen recognition receptors, leading to expression of pro-inflammatory cytokines. For example, Toll-like receptor (TLR)-4 recognizes lipopolysaccharide (LPS), which is a component of the outer membrane of Gram-negative bacteria; TLR4 activates the nuclear factor of kappa beta (NF-κB) signaling pathway and promotes the transcription of IL-6 mRNA. Regnase-1 promotes IL-6 mRNA degradation, whereas Arid5a inhibits the destabilizing effect of Regnase-1. The balance between Arid5a and Regnase-1 is important for the regulation of IL-6 mRNA. IRAK1 IL-1 receptor-associated kinase 1, MyD88 myeloid differentiation primary response 88, TRAF6 tumor necrosis factor receptor-associated factor 6, Ub ubiquitination, NEMO NF-κB essential modulator, IKK inhibitor of NF-κB kinase, AP-1 activator protein 1, IRF1 interferon regulatory factor 1, MRE multiple response element, C/EBPβ CCAAT enhancer binding protein β, SP-1 specificity protein 1, UTR untranslated region, miR microRNA
Pathological Role of IL-6 in Autoimmune Inflammatory Diseases
As described elsewhere, the immediate and transient expression of IL-6 contributes to host defense against infections and tissue injuries. However, deregulated excessive IL-6 synthesis during this protective process or persistent IL-6 production leads to the development of a severe acute life-threatening complication, the so-called cytokine storm or chronic autoimmune inflammatory diseases, respectively. The association of IL-6 with disease development was first demonstrated in a case of benign heart tumor, cardiac myxoma. The cultured fluid from the myxoma tissue of a patient, who had presented with fever, polyarthritis, an elevated CRP level, anemia, and hypergammaglobulinemia with positivity for anti-nuclear factor, was found to contain a large quantity of IL-6 [36]. Subsequently, excessive IL-6 expression was also detected in the synovial fluids of RA, swollen lymph nodes of Castleman’s disease, myeloma cells [3], and peripheral blood cells or infiltrating cells in tissues involved in various other autoimmune inflammatory diseases [14, 37]. The extent of the elevation of the serum IL-6 level depends on the particular disease and its disease severity, but in cytokine storms such as those associated with septic shock, the concentration can reach as high as the microgram per milliliter level [38].
IL-6-Targeting Strategies: A New Era for the Treatment of Autoimmune Inflammatory Diseases
In view of the pathological role of IL-6 in various autoimmune inflammatory diseases, IL-6 targeting was evaluated as a novel therapeutic strategy against these diseases [37]. Tocilizumab, a humanized anti-IL-6R monoclonal Ab of the IgG1 class, was generated by grafting the complementarity-determining regions of a mouse anti-human IL-6R Ab onto human IgG1 [39]. This Ab can block IL-6-mediated signal transduction by inhibiting IL-6 binding to both transmembrane IL-6R and sIL-6R. Numerous worldwide clinical trials verified the outstanding efficacy and tolerable safety of tocilizumab, leading to its current approval for the treatment of RA in more than 130 countries; systemic JIA (sJIA) in Japan, India, the USA, and the EU; and polyarticular JIA and Castleman’s disease in Japan and India [27, 40, 41].
Efficacy of Tocilizumab in Rheumatoid Arthritis
RA is an autoimmune disease characterized by systemic and joint inflammation, which causes joint destruction, dramatically reduces activity of daily living (ADL) and quality of life (QOL), and shortens lifespan [42]. Clinical trials demonstrated that tocilizumab effectively suppresses disease activity and protects against progression of joint destruction, as well as ameliorating the effect of RA on ADL and QOL [43]. Although other biologics are currently used to treat RA, including TNF inhibitors, an inhibitor of T cell stimulation, and a B cell depleting agent, tocilizumab appears to be the most powerful with regard to suppression of disease activity. Tocilizumab is the only biologic proven to be more efficacious as a monotherapy than the anchor disease-modifying antirheumatic drug, methotrexate (MTX). TNF inhibitors require the concomitant use of MTX to achieve their maximal effect, but tocilizumab monotherapy exhibited no clinically relevant inferiority to tocilizumab combination therapy with MTX [44]. Moreover, direct comparison of monotherapy with tocilizumab and adalimumab, a fully human anti-TNF-α Ab, demonstrated that tocilizumab was superior to adalimumab, as determined by various indices of disease activity [45]. On the basis of these findings, in the newest RA management recommendation by the European League Against Rheumatism, tocilizumab was positioned as the first-line biologic, especially in patients for whom biological monotherapy must be initiated [46]. Furthermore, because of the suppressive effects of tocilizumab in the synthesis of acute-phase proteins such as SAA and hepcidin, it is appropriate to select tocilizumab for cases of RA complicated by amyloid A amyloidosis or anemia associated with chronic disorders [43].
Efficacy of Tocilizumab in Systemic Juvenile Idiopathic Arthritis
sJIA is a subtype of chronic childhood arthritis that leads to joint destruction, functional disability, and growth impairment, accompanied by systemic inflammation [47]. IL-6 is markedly elevated in the blood of sJIA patients, and the IL-6 level is well correlated with disease activity. In a phase III trial of Japanese 56 patients with sJIA, 91 %, 86 %, and 68 % of the patients exhibited American College of Rheumatology (ACR) Pedi responses of 30 %, 50 %, and 70 %, respectively, at week 6 [48]. Subsequently, in a global phase III trial, 112 children with active sJIA randomly received placebo or tocilizumab. At week 12, the primary endpoint (absence of fever + improvement of 30 % or greater in at least three of the six variables in the ACR core set for JIA) was met in significantly more patients in the tocilizumab-treated group than in the placebo group (85 % vs. 24 %) [49]. At week 52, 82 % and 59 % of the patients who received tocilizumab attained improvements of 70 % and 90 %, respectively. The striking responsiveness of sJIA to tocilizumab has led to widespread recognition that we have started a new era in the treatment of this disease, long considered to be one of the most intractable juvenile diseases [50].
Efficacy of Tocilizumab in Castleman’s Disease
Castleman’s disease is a lymphoproliferative disease with benign hyperplastic lymph nodes characterized by follicular hyperplasia and capillary proliferation accompanied by endothelial hyperplasia [51]. Deregulated IL-6 expression in transgenic mice produces a syndrome resembling Castleman’s disease [52], whereas IL-6 blockade inhibits inflammatory manifestations in these animals [53]. IL-6 is highly expressed in germinal center B cells of hyperplastic lymph nodes of patients with Castleman’s disease, and surgical removal of a solitary involved lymph node leads to clinical improvement and reduced serum IL-6 concentrations [54]. In two open-label clinical trials of tocilizumab for Castleman’s disease, the drug exerted a significant ameliorative effect with regard to clinical symptoms and laboratory findings [55, 56].
Efficacy of Tocilizumab in Other Autoimmune Inflammatory Diseases
Case reports, series, and pilot studies of the off-label applications of tocilizumab have produced favorable outcomes, indicating that tocilizumab may be used for the treatment of multiple conditions including autoimmune diseases, chronic inflammatory diseases, and autoinflammatory diseases [27, 40, 41]. The results accumulated so far strongly suggest that IL-6 blockade represents an innovative therapeutic strategy for SSc, large-vessel vasculitis, amyloid A amyloidosis, NMO, adult-onset Still’s disease (AOSD), and cytokine release syndrome (CRS).
SSc is a connective tissue disorder characterized by tissue fibrosis, vasculopathy, and immune abnormalities [57]. Several lines of evidence suggest that IL-6 is a potential therapeutic target cytokine in SSc. First, IL-6 is expressed at high levels in patient serum and involved skin, and the serum level is well correlated with the severity of skin symptoms. Second, IL-6 promotes collagen production and expression of α-smooth muscle actin by dermal fibroblasts, as well as endothelial cell activation and apoptosis in endothelial cell–neutrophil co-cultures. Moreover, in models of SSc induced by bleomycin, IL-6 blockade by administration of anti-IL-6R Ab suppresses myofibroblast activation, resulting in reduced dermal fibrosis [58]. We observed the beneficial effects of tocilizumab for two patients with SSc [59]. Histological analyses revealed thinning of collagen fiber bundles and reduction of activated myofibroblasts in the dermis after a 6-month treatment, suggesting that IL-6 blockade strategy is a promising approach for the treatment of SSc.
The pathological role of IL-6 has been well documented in large-vessel vasculitis, e.g., giant cell arteritis (GCA) and Takayasu arteritis (TA) [60]. Serum concentrations of IL-6 are elevated at the onset and during clinical relapse of GCA and TA, and tissue-infiltrating cells produce major quantities of IL-6 and IFN-γ in patients with both diseases. Tocilizumab treatment has resulted in rapid and prominent beneficial effects in patients with GCA and TA who had been refractory to conventional treatment regimens [40, 41]. Moreover, tocilizumab monotherapy induced disease remission in five patients with GCA. These results strongly suggest that IL-6 inhibition represents a promising therapeutic strategy for large-vessel vasculitis.
A serious complication of chronic inflammatory diseases is amyloid A amyloidosis, in which amyloid fibril deposition causes progressive deterioration in various organs [12]. Sustained high concentrations of SAA, an amyloid fibril precursor protein, correlate with progression of renal amyloid diseases. Tocilizumab is the most powerful known inhibitor of SAA production. Case studies of amyloid A amyloidosis complicated by RA, JIA, vasculitis syndrome, Behcet’s disease, and latent tuberculosis have revealed the striking clinical effect of tocilizumab on gastrointestinal symptoms and renal function [12, 40, 41].
NMO is a chronic inflammatory disorder predominantly affecting the spinal cord and optic nerves. In this disease, autoantibodies directed against the astrocyte water-channel protein, AQP4, play a pathologic role [61]. Several studies have reported a significant increase of IL-6 in the cerebrospinal fluid of patients with NMO. Moreover, the population of plasmablasts with the CD19intCD27highCD38highCD180negative phenotype is elevated in the peripheral blood of NMO patients, and anti-AQP4 Abs are produced by these plasmablasts [4]. IL-6 increases the survival of plasmablasts, as well as AQP4 Ab secretion, whereas tocilizumab reduces the survival of these cells. Clinical improvement and reduction of serum levels of anti-AQP4 Abs have been reported in several NMO patients who were refractory to conventional treatment regimens [62, 63].
AOSD, a chronic inflammatory disease characterized by four cardinal symptoms (spiking fever, evanescent maculopapular rash, arthritis, and leukocytosis) pathologically resembles sJIA and is considered to be an adult-onset type of sJIA [64]. As expected, numerous case studies and pilot studies have shown that tocilizumab treatment improved clinical symptoms and signs in AOSD patients who had been refractory to conventional treatment [40, 41]. These favorable results also indicate that, just as for sJIA, tocilizumab may become a first-line biologic for the treatment of AOSD.
CRS is a potentially fatal immune reaction, which is sometimes induced by hyperactivation of T cells after T cell–engaging therapies [65]. Serum levels of IL-6, IL-10, and IFN-γ are significantly elevated in patients with CRS. Two recent reports showed that CRS—which occurred in two patients with acute lymphoblastic leukemia (ALL) treated with chimeric antigen receptor-modified T cells with specificity for CD19 (CTL019 cells) and in one ALL patient treated with blinatumomab, a CD19/CD3-bispecific Ab that engages the T cell receptor—could be abrogated by a single injection of tocilizumab [66, 67]. These findings indicate that IL-6 inhibition represents an innovative therapeutic approach for T cell–mediated CRS or other complications with hypercytokinemia, such as systemic inflammatory response syndrome, septic shock, macrophage activation syndrome, and hemophagocytic syndrome.
The beneficial effects of tocilizumab strongly suggest that it will be widely applicable for the treatment of chronic autoimmune inflammatory diseases and acute systemic inflammatory complications. However, further clinical evaluations are essential in order to determine additional indications for tocilizumab therapy. A list of ongoing clinical trials of tocilizumab registered at ClinicalTrials.gov is provided in Table 1.
Mechanisms Through Which Tocilizumab Is Efficacious in Various Autoimmune Inflammatory Diseases
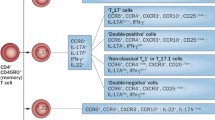
The efficacy of tocilizumab in amyloid A amyloidosis and anemia associated with chronic disorders can be explained by its suppression of the responsible proteins, SAA and hepcidin, respectively, but the mechanisms through which tocilizumab is efficacious in various phenotypically different autoimmune inflammatory diseases remain incompletely understood [68]. As observed in NMO, tocilizumab treatment could decrease autoantibody (anti-AQP4) production by acting on plasmablasts [4, 62]. IL-21 promotes plasma cell differentiation and preferentially induces IgG4 production [9]. One study demonstrated that tocilizumab treatment causes a selective reduction in IL-21 production of memory/activated T cells, leading to a reduction in the serum levels of IgG4-specific anti-citrullinated peptide Ab in RA patients [69]. Several recent reports demonstrated that tocilizumab therapy led to an increase in the number of Treg cells in peripheral blood CD4+ T cell fractions in RA patients [70–72] (Fig. 2). These effects may account for the correction of immunological abnormalities. In addition, the treatment reportedly resulted in improvement in various other biomarkers related to inflammation, bone and cartilage metabolism, angiogenesis, glucose metabolism, fibrosis, etc. These findings indicate that the clinical effects of tocilizumab are mediated by several mechanisms. Another possible explanation for the prominent effect of tocilizumab is that the primary cause of successfully treated diseases is deregulated synthesis of IL-6, but that phenotypic differences arise because of differences in the cell populations that produce IL-6. Thus, to facilitate investigations of the pathogenesis of specific diseases, it will be necessary to elucidate the mechanisms responsible for excessive or continuous IL-6 production.

IL-6-targeted therapy can rectify immunological abnormalities. Although the pathogenesis of autoimmune inflammatory diseases is not fully understood, an imbalance between effector CD4+ T cell subsets (Th17 ± Th1/Treg↑) and autoantibodies play central roles in their development. (a) Overexpression of IL-6 may lead to an imbalance in effector T cell subsets (Th17/Treg↑), whereas tocilizumab therapy can rectify the imbalance. (b) IL-6, acting in an autocrine or paracrine manner, increases the survival of plasmablasts that produce autoantibodies, whereas tocilizumab treatment decreases the survival of these cells, leading to the suppression of autoantibody synthesis. TGFβ transforming growth factor β, Treg regulatory T cells, ROR retinoid-related orphan receptor, Foxp3 forkhead box p3
Concluding Remarks
Tocilizumab was developed on the basis of a comprehensive view of the IL-6-mediated signaling system, the pathological significance of IL-6 in various diseases, and progress in bioengineering techniques. Tocilizumab is now positioned as a first-line biologic for the treatment of moderate to severe RA and sJIA, and is the only drug approved for Castleman’s disease. This great success has resulted in a paradigm shift in the treatment of these diseases, and has accelerated the development of other various IL-6 inhibitors [73]. Within the next decade, we anticipate that IL-6 inhibitors will be widely used for the treatment of various diseases currently considered to be intractable; as a result, some of these diseases will no longer be refractory to therapy.
Although fundamental research on the IL-6-mediated signaling pathway was able to solve the long-standing mystery regarding why cytokines exhibit redundant and pleiotropic activity, another mystery persists regarding why IL-6 is excessively or continuously expressed in various diseases. Accurate and detailed analyses of the proteins such as Arid5a and Regnase-1 and miRs that regulate IL-6 synthesis will be helpful in solving this mystery. Clarification of the mechanism(s) involved will inspire the identification of more specific target molecules and investigations into the pathogenesis of specific diseases.
References
Hirano T, Yasukawa K, Harada H et al (1986) Complementary DNA for a novel human interleukin (BSF-2) that induces B lymphocytes to produce immunoglobulin. Nature 324:73–76
Kishimoto T (1989) The biology of interleukin-6. Blood 74:1–10
Kawano M, Hirano T, Matsuda T et al (1988) Autocrine generation and requirement of BSF-2/IL-6 for human multiple myelomas. Nature 332:83–85
Chihara N, Aranami T, Sato W et al (2011) Interleukin 6 signaling promotes anti-aquaporin 4 autoantibody production from plasmablasts in neuromyelitis optica. Proc Natl Acad Sci U S A 108:3701–3706
Kimura A, Kishimoto T (2010) IL-6: regulator of Treg/Th17 balance. Eur J Immunol 40:1830–1835
Fujimoto M, Serada S, Mihara M et al (2008) Interleukin-6 blockade suppresses autoimmune arthritis in mice by the inhibition of inflammatory Th17 responses. Arthritis Rheum 58:3710–3719
Serada S, Fujimoto M, Mihara M et al (2008) IL-6 blockade inhibits the induction of myelin antigen-specific Th17 cells and Th1 cells in experimental autoimmune encephalomyelitis. Proc Natl Acad Sci U S A 105:9041–9046
Haruta H, Ohguro N, Fujimoto M et al (2011) Blockade of interleukin-6 signaling suppresses not only th17 but also interphotoreceptor retinoid binding protein-specific Th1 by promoting regulatory T cells in experimental autoimmune uveoretinitis. Invest Ophthalmol Vis Sci 52:3264–3271
Ma CS, Deenick EK, Batten M et al (2012) The origins, function, and regulation of T follicular helper cells. J Exp Med 209:1241–1253
Heinrich PC, Castell JV, Andus T (1990) Interleukin-6 and the acute phase response. Biochem J 265:621–636
Nishimoto N, Terao K, Mima T et al (2008) Mechanisms and pathologic significances in increase in serum interleukin-6 (IL-6) and soluble IL-6 receptor after administration of an anti-IL-6 receptor antibody, tocilizumab, in patients with rheumatoid arthritis and Castleman disease. Blood 112:3959–3964
Tanaka T, Hagihara K, Hishitani Y et al (2011) Tocilizumab for the treatment of AA amyloidosis. In: Isil Adadan G (ed) Amyloidosis – an insight to disease of systems and novel therapies. INTECH Open Access Publisher, Rijeka, pp 155–170
Nemeth E, Rivera S, Gabayan V et al (2004) IL-6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J Clin Invest 113:1271–1276
Akira S, Taga T, Kishimoto T (1993) Interleukin-6 in biology and medicine. Adv Immunol 54:1–78
Hashizume M, Hayakawa N, Mihara M (2008) IL-6 trans-signalling directly induces RANKL on fibroblast-like synovial cells and is involved in RANKL induction by TNF-alpha and IL-17. Rheumatology (Oxford) 47:1635–1640
Nakahara H, Song J, Sugimoto M et al (2003) Anti-interleukin-6 receptor antibody therapy reduces vascular endothelial growth factor production in rheumatoid arthritis. Arthritis Rheum 48:1521–1529
Duncan MR, Berman B (1991) Stimulation of collagen and glycosaminoglycan production in cultured human adult dermal fibroblasts by recombinant human interleukin 6. J Invest Dermatol 97:686–692
Kishimoto T, Akira S, Taga T (1992) Interleukin-6 and its receptor: a paradigm for cytokines. Science 258:593–597
Yamasaki K, Taga T, Hirata Y et al (1988) Cloning and expression of the human interleukin-6 (BSF-2/IFN beta 2) receptor. Science 241:825–828
Hibi M, Murakami M, Saito M et al (1990) Molecular cloning and expression of an IL-6 signal transducer, gp130. Cell 63:1149–1157
Murakami M, Hibi M, Nakagawa N et al (1993) IL-6-induced homodimerization of gp130 and associated activation of a tyrosine kinase. Science 260:1808–1810
Taga T, Kishimoto T (1997) Gp130 and the interleukin-6 family of cytokines. Annu Rev Immunol 15:797–819
Kishimoto T, Taga T, Akira S (1994) Cytokine signal transduction. Cell 76:253–262
Naka T, Narazaki M, Hirata M et al (1997) Structure and function of a new STAT-induced STAT inhibitor. Nature 387:924–929
Schmitz J, Weissenbach M, Haan S et al (2000) SOCS3 exerts its inhibitory function on interleukin-6 signal transduction through the SHP2 recruitment sites of gp130. J Biol Chem 275:12848–12856
Bianchi ME (2007) DAMPs, PAMPs and alarmins: all we need to know about danger. J Leukoc Biol 81:1–5
Kang S, Tanaka T, Kishimoto T (2015) Therapeutic uses of anti-interleukin-6 receptor antibody. Int Immuno l27:21–2910.1093/intimm/dxu081
Wolf J, Rose-John S, Garbers C (2014) Interleukin-6 and its receptors: a highly regulated and dynamic system. Cytokine 70:11–2010.1016/j.cyto.2014.05.024
Anderson P (2008) Post-transcriptional control of cytokine production. Nat Immunol 9:353–359
Chen CY, Shyu AB (1995) AU-rich elements: characterization and importance in mRNA degradation. Trends Biochem Sci 20:465–470
Matsushita K, Takeuchi O, Standley DM et al (2009) Zc3h12a is an RNase essential for controlling immune responses by regulating mRNA decay. Nature 458:1185–1190
Iwasaki H, Takeuchi O, Teraguchi S et al (2011) The IkappaB kinase complex regulates the stability of cytokine-encoding mRNA induced by TLR-IL-1R by controlling degradation of Regnase-1. Nat Immunol 12:1167–1175
Masuda K, Ripley B, Nishimura R et al (2013) Arid5a controls IL-6 mRNA stability, which contributes to elevation of IL-6 level in vivo. Proc Natl Acad Sci U S A 110:9409–9414
Saito Y, Kagami SI, Sanayama Y et al (2014) At-rich-interactive domain-containing protein 5A functions as a negative regulator of retinoic acid receptor-related orphan nuclear receptor γt-induced Th17 cell differentiation. Arthritis Rheum 66:1185–119410.1002/art.38324
Tanaka T, Kishimoto T (2014) The biology and medical implications of interleukin-6. Cancer Immunol Res 2:288–294
Hirano T, Taga T, Yasukawa K et al (1987) Human B-cell differentiation factor defined by an anti-peptide antibody and its possible role in autoantibody production. Proc Natl Acad Sci U S A 84:228–231
Kishimoto T (2005) Interleukin-6: from basic science to medicine-40 years in immunology. Annu Rev Immunol 23:1–21
Waage A, Brandtzaeq P, Halstensen A et al (1989) The complex pattern of cytokines in serum from patients with meningococcal septic shock. Association between interleukin 6, interleukin 1, and fatal outcome. J Exp Med 169:333–338
Sato K, Tsuchiya M, Saldanha J et al (1993) Reshaping a human antibody to inhibit the interleukin 6-dependent tumor cell growth. Cancer Res 3:851–856
Tanaka T, Narazaki M, Kishimoto T (2012) Therapeutic targeting of the interleukin-6 receptor. Annu Rev Pharmacol Toxicol 52:199–219
Tanaka T, Narazaki M, Ogata A, Kishimoto T (2014) A new era for the treatment of inflammatory autoimmune diseases by interleukin-6 blockade strategy. Semin Immunol 26:88–96
Mclnnes IB, Schett G (2011) The pathogenesis of rheumatoid arthritis. N Engl J Med 365:2205–2219
Tanaka T, Hishitani Y, Ogata A (2014) Monoclonal antibodies in rheumatoid arthritis: comparative effectiveness of tocilizumab with tumor necrosis factor inhibitors. Biologics 8:141–153
Dougados M, Kissel K, Sheeran T et al (2013) Adding tocilizumab or switching to tocilizumab monotherapy in methotrexate inadequate responders: 24-week symptomatic and structural results of a 2-year randomised controlled strategy trial in rheumatoid arthritis (ACT-RAY). Ann Rheum Dis 72:43–50
Gabay C, Emery P, van Vollenhoven R et al (2013) Tocilizumab monotherapy versus adalimumab monotherapy for treatment of rheumatoid arthritis (ADACTA): a randomised, double-blind, controlled phase 4 trial. Lancet 381:1541–1550
Smolen JS, Landewe R, Breedveld FC et al (2014) EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update. Ann Rheum Dis 73:510–515
Yokota S, Tanaka T, Kishimoto T (2012) Efficacy, safety and tolerability of tocilizumab in patients with systemic juvenile idiopathic arthritis. Ther Adv Musculoskelet Dis 4:387–397
Yokota S, Imagawa T, Mori M et al (2008) Efficacy and safety of tocilizumab in patients with systemic-onset juvenile idiopathic arthritis: a randomised, double-blind, placebo-controlled, withdrawal phase III trial. Lancet 371:998–1006
De Benedetti F, Brunner HI, Ruperto N et al (2012) Randomized trial of tocilizumab in systemic juvenile idiopathic arthritis. N Engl J Med 367:2385–2395
Sandborg C, Mellins ED (2012) A new era in the treatment of systemic juvenile idiopathic arthritis. N Engl J Med 367:2439–2440
Schulte KM, Talat N (2010) Castleman’s disease – a two compartment model of HHV8 infection. Nat Rev Clin Oncol 7:533–543
Brandt SJ, Bodine DM, Dunbar CE et al (1990) Dysregulated interleukin 6 expression produces a syndrome resembling Castleman’s disease in mice. J Clin Invest 86:592–599
Katsume A, Saito H, Yamada Y et al (2002) Anti-interleukin 6 (IL-6) receptor antibody suppresses Castleman’s disease like symptoms emerged in IL-6 transgenic mice. Cytokine 20:304–311
Yoshizaki K, Matsuda T, Nishimoto N et al (1989) Pathogenic significance of interleukin-6 (IL-6/BSF-2) in Castleman’s disease. Blood 74:1360–1367
Nishimoto N, Sasai M, Shima Y et al (2000) Improvement in Castleman’s disease by humanized anti-interleukin-6 receptor antibody therapy. Blood 95:56–61
Nishimoto N, Kanakura Y, Aozasa K et al (2005) Humanized anti-interleukin-6 receptor antibody treatment of multicentric Castleman disease. Blood 106:2627–2632
Gabrielli A, Avvedimento EV, Krieg T (2009) Scleroderma. N Engl J Med 360:1989–2003
Kitaba S, Murota H, Terao M et al (2012) Blockade of interleukin-6 receptor alleviates disease in mouse model of scleroderma. Am J Pathol 180:165–176
Shima Y, Kuwahara Y, Murota H et al (2010) The skin of patients with systemic sclerosis softened during the treatment with anti-IL-6 receptor antibody tocilizumab. Rheumatology (Oxford) 49:2408–2412
Unizony S, Stone JH, Stone JR (2013) New treatment strategies in large-vessel vasculitis. Curr Opin Rheumatol 25:3–9
Sahraian MA, Radue EW, Minagar A (2013) Neuromyelitis optica: clinical manifestations and neuroimaging features. Neurol Clin 31:139–152
Araki M, Aranami T, Matsuoka T et al (2013) Clinical improvement in a patient with neuromyelitis optica following therapy with the anti-IL-6 receptor monoclonal antibody tocilizumab. Mod Rheumatol 23:827–831
Araki M, Matsuoka T, Miyamoto K et al (2014) Efficacy of the anti-IL-6 receptor antibody tocilizumab in neuromyelitis optica: a pilot study. Neurology 82:1302–1306
Gerfaud-Valentin M, Jamilloux Y, Iwaz J et al (2014) Adult-onset Still’s disease. Autoimmun Rev 13:708–722
Lee DW, Gardner R, Porter DL et al (2014) Current concepts in the diagnosis and management of cytokine release syndrome. Blood 124:188–195
Grupp SA, Kalos M, Barrett D et al (2013) Chimeric antigen receptor-modified T cells for acute lymphoid leukemia. N Engl J Med 368:1509–1518
Teachey DT, Rheingold SR, Maude SL et al (2013) Cytokine release syndrome after blinatumomab treatment related to abnormal macrophage activation and ameliorated with cytokine-directed therapy. Blood 121:5154–5157
Tanaka T (2013) Can IL-6 blockade rectify imbalance between Tregs and Th17 cells? Immunotherapy 5:695–697
Carbone G, Wilson A, Diehl SA et al (2013) Interleukin-6 receptor blockade selectively reduces IL-21 production by CD4 T cells and IgG4 autoantibodies in rheumatoid arthritis. Int J Biol Sci 9:279–288
Samson M, Audia S, Janikashvili N et al (2012) Brief report: inhibition of interleukin-6 function corrects Th17/Treg cell imbalance in patients with rheumatoid arthritis. Arthritis Rheum 64:2499–2503
Pesce B, Soto L, Sabugo F et al (2013) Effect of interleukin-6 receptor blockade on the balance between regulatory T cells and T helper type 17 cells in rheumatoid arthritis patients. Clin Exp Immunol 171:237–242
Thiolat A, Semerano L, Pers YM et al (2014) Interleukin-6 receptor blockade enhances CD39+ regulatory T cell development in rheumatoid arthritis and in experimental arthritis. Arthritis Rheum 66:273–283
Jones SA, Scheller J, Rose-John S (2011) Therapeutic strategies for the clinical blockade of IL-6/gp130 signaling. J Clin Invest 21:3375–3383
Conflict of Interest
T. Kishimoto holds a patent for tocilizumab and has received royalties for Actemra. T. Tanaka has received a grant and payment for lectures including service on speaker’s bureaus from Chugai Pharmaceutical Co., Ltd. S. Kang declares no conflict of interest. The Department of Clinical Application of Biologics of Osaka University Graduate School of Medicine is an endowment department, supported with an unrestricted grant from Chugai Pharmaceutical Co., Ltd.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is distributed under the terms of the Creative Commons Attribution Noncommercial License, which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Copyright information
© 2015 The Author(s)
About this paper
Cite this paper
Kishimoto, T., Kang, S., Tanaka, T. (2015). IL-6: A New Era for the Treatment of Autoimmune Inflammatory Diseases. In: Nakao, K., Minato, N., Uemoto, S. (eds) Innovative Medicine. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55651-0_11
Download citation
DOI: https://doi.org/10.1007/978-4-431-55651-0_11
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-55650-3
Online ISBN: 978-4-431-55651-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)