
Abstract
Purpose
2-[18F]Fluoro-2-deoxy-D-glucose (FDG)–positron emission tomography (PET)/computed tomography (CT) has been suggested as an imaging modality to diagnose polymyalgia rheumatica (PMR). However, the applicability of FDG-PET/CT remains unclear, especially following glucocorticoid administration. This study aimed to investigate the diagnostic accuracy of FDG-PET/CT before and during prednisolone treatment, as well as following short-term prednisolone discontinuation.
Methods
Treatment naïve suspected PMR patients were clinically diagnosed at baseline and subsequently had an FDG-PET/CT performed. Patients diagnosed with PMR were administered prednisolone following the first FDG-PET/CT and had a second FDG-PET/CT performed after 8 weeks of treatment. Subsequently, prednisolone was tapered with short-term discontinuation at week 9 followed by a third FDG-PET/CT at week 10. An FDG-PET/CT classification of PMR/non-PMR was applied, utilizing both the validated Leuven score and a dichotomous PMR score. The final diagnosis was based on clinical follow-up after 1 year.
Results
A total of 68 and 27 patients received a final clinical diagnosis of PMR or non-PMR. A baseline FDG-PET/CT classified the patients as having PMR with a sensitivity/specificity of 86%/63% (Leuven score) and 82%/70% (dichotomous score). Comparing the subgroup of non-PMR with inflammatory diseases to the PMR group demonstrated a specificity of 39%/54% (Leuven/dichotomous score). After 8 weeks of prednisolone treatment, the sensitivity of FDG-PET/CT decreased to 36%/41% (Leuven/dichotomous score), while a short-term prednisolone discontinuation increased the sensitivity to 66%/60%.
Conclusion
FDG-PET/CT has limited diagnostic accuracy for differentiating PMR from other inflammatory diseases. If FDG-PET/CT is intended for diagnostic purposes, prednisolone should be discontinued to enhance diagnostic accuracy.
Trial registration
ClinicalTrials.gov (NCT04519580). Registered 17th of August 2020.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Diagnosing polymyalgia rheumatica (PMR) can be difficult, and it has been reported that 10–30% of patients are misclassified by rheumatologists at the initial evaluation [1,2,3]. To address this issue, several classification criteria have been developed, but neither these nor a clinical diagnosis alone have exhibited a high diagnostic performance [4,5,6,7,8,9,10]. As a result, specific diagnostic tests are currently unavailable, and an accurate diagnosis still relies on clinical follow-up [11,12,13]. Another common clinical issue is that 50% of patients with suspected PMR are administered prednisolone prior to rheumatologic assessment [14]. This can mask the symptoms of PMR as well as important differential diagnoses. Consequently, patients may require a prednisolone taper to confirm or reject the PMR diagnosis [15,16,17].
2-[18F]Fluoro-2-deoxy-D-glucose (FDG)–positron emission tomography (PET)/computed tomography (CT) has recently been suggested as a potential imaging modality for diagnosing PMR [11, 12]. It has been argued that a characteristic FDG-uptake pattern at specific musculoskeletal sites may be pathognomonic for PMR [18]. Several FDG-PET/CT scores and algorithms have been developed, which assess FDG uptake in the most characteristic sites around the shoulders, hips, and spine [11, 12, 19,20,21,22,23,24]. In particular, the Leuven composite score has shown promising results with a sensitivity of 85% and specificity of 88% for the PMR diagnosis, which has recently been validated in two additional studies [11, 12, 25]. However, in all three studies, the control groups primarily comprised patients without inflammatory diseases. Such patients may not demonstrate increased musculoskeletal FDG uptake due to their state of limited inflammation, resulting in inflated diagnostic performances of FDG-PET/CT. Furthermore, only the original study by Henckaerts et al. had a prospective design, whereas the validation studies were performed on retrospective cohorts. Consequently, there is a need for prospective studies including individuals with other inflammatory diseases to ensure a comprehensive evaluation. Moreover, the applicability of FDG-PET/CT for diagnosing patients with PMR after the commencement of prednisolone needs clarification, particularly whether patients should be discontinued in prednisolone prior to the FDG-PET/CT scan.
The aim of this study was to investigate the diagnostic accuracy of FDG-PET/CT in patients suspected of PMR and further to evaluate the effects of prednisolone treatment and short-term prednisolone discontinuation.
Material and methods
Patient population and design
Consecutive patients suspected of PMR were prospectively included between September 2020 and June 2022 from the Departments of Rheumatology at Aarhus University Hospital, Horsens Regional Hospital, and Silkeborg Regional Hospital in Denmark. To assess all potential patients with PMR, rapid referral clinics were established for all individuals suspected of PMR, and general practitioners were informed about this new service through information meetings and advertisements in newsletters dedicated to general practitioners. After referral, all patients were evaluated in the clinics preferably within 1 week. Inclusion criteria for the study were as follows: patients suspected of PMR, aged over 50, and experiencing proximal muscle pain. The exclusion criteria were as follows: any glucocorticoid treatment within the last 3 months; a medical history of PMR or giant cell arteritis (GCA); any other inflammatory rheumatic disease; symptoms of cranial GCA including headache, jaw claudication, scalp tenderness, or sight disturbances; and any active malignant cancers within the past 5 years (except basal cell carcinoma [26]).
The study design is graphically depicted in Supplementary Figure S1. At baseline, all patients had their medical history taken, lab work; were clinically examined, had vascular ultrasound as well as ultrasound of shoulders and hips performed; and were initially clinically diagnosed by the treating clinician. Subsequently, all patients had an FDG-PET/CT performed within days and before initiation of prednisolone treatment. Patients diagnosed with GCA subsequently to the FDG-PET/CT were excluded from the final analyses. Patients with a clinical diagnosis of solely PMR were administered 15 mg of prednisolone with a gradual taper (Supplementary Figure S1). If an adequate treatment response was not achieved within 2–4 weeks, based on lab work and telephone consultations at week 1 and week 4, the prednisolone dose was increased to 25 mg daily. Additionally, patients experiencing incomplete remission at week 1 underwent an additional telephone consultation along with lab work to assess whether an early increase in prednisolone dosage at week 2 was indicated. After 8 weeks of prednisolone treatment, a second clinical visit was performed consisting of a clinical examination, lab work, and a second FDG-PET/CT. Patients in clinical remission at week 8 were tapered to 5 mg prednisolone for 1 week followed by prednisolone discontinuation for a week. At week 10, during the temporary treatment discontinuation, a similar clinical visit was conducted including a third FDG-PET/CT. Prednisolone was subsequently restarted and tapered according to standard care [27]. Patients with incomplete remission at week 8 or relapse during prednisolone discontinuation continued or restarted prednisolone administration and were withdrawn from the week 10 visit, since this visit aimed at evaluating the effect of a short-term prednisolone discontinuation. At the 1-year follow-up, an experienced rheumatologist (KKK, ITH, BDN, CMS, SGK, JBN) determined the final diagnosis, including patients withdrawn from previous visits, considering the initial baseline diagnosis and the progression of the disease during the first year. This 1-year diagnosis served as the reference standard in this study. Patients initially diagnosed with other conditions, GCA or cancer, at the baseline visit received a telephone consultation and a medical chart review after 1 year to confirm their alternative diagnosis.
The study has been registered at the ClinicalTrials.gov database 17th of August 2020 (NCT04519580). Study data was collected and managed using REDCap electronic data capture tools hosted at Aarhus University [28, 29]
PMR activity
At each visit, the clinician independently assessed whether PMR patients were in remission or relapsed based on their clinical expertise, since a widely accepted scoring system for relapse is lacking. The PMR activity score (PMR-AS) was assessed: PMR-AS score < 7 indicating low PMR activity, 7–17 representing medium disease activity, and a score of more than 17 indicating high disease activity [30].
Blood samples
At baseline, laboratory tests were performed to investigate potential differential diagnoses. These tests included assessment of creatine kinase; p-25-hydroxy vitamin D2 + D3; thyroid-stimulating hormone; Ca2 + ; M-component; kappa and lambda chains; immunoglobulin A, G, and M; rheumatoid factor; anti-citrullinated-protein-antibody; and erythrocyte sedimentation rate (ESR). Routine tests were conducted at each visit including C-reactive protein (CRP), creatinine, alanine aminotransferase, alkaline phosphatase, platelet count, hemoglobin, white blood cell count, absolute neutrophil count, and absolute lymphocyte count.
FDG-PET/CT scan procedure
Before the FDG-PET/CT scans, patients underwent a minimum fasting period of 6 h, except for diabetic patients who fasted for a minimum of 4 h. Patients received an intravenous infusion of 4 MBq FDG per kilogram body weight 60 min before undergoing a scan from the vertex of the skull to the mid-thigh using an integrated PET/CT scanner with continuous bed motion (Siemens Biograph Vision). Images were reconstructed using 4 iterations, 5 subsets, and 2-mm Gaussian post-processing filter, in matrix size 440 × 440. During the study, the FDG-PET/CT protocol was updated, and patients were subsequently instructed to have their arms down during the scan, aligning with the latest recommendation [31, 32]. An initial low-dose CT was performed for attenuation correction and anatomic mapping.
FDG-PET/CT evaluation
Two experienced nuclear medicine specialists (LCG and KR) and a trained medical doctor (AWN) independently evaluated the baseline, 8-week, and 10-week FDG-PET/CT scans blinded from the clinical diagnosis, clinical data, and scanning date. In accordance with standard daily procedures for FDG-PET/CT evaluation, each evaluator initially provided a binary classification of PMR (PMR yes/no) for each patient based on their regular practice, and any discrepancies were resolved through discussion between AWN, LCG, and KR. Furthermore, 12 different anatomic sites were evaluated for FDG uptake: shoulder joints, sternoclavicular joints, ischial tuberosities, hip joints, greater trochanters, and cervical/lumbar interspinous bursae. The FDG uptake was visually graded for each site and compared to liver uptake; 0, no uptake; 1, uptake lower than liver; 2, uptake equal to or higher than liver [11]. A summed PET-PMR score was calculated for each patient using the Leuven score and a cut-off of 16 or above was considered positive for PMR [11].
Sample size
Based on the only other prospective FDG-PET study in this research area, approximately 99 patients should be enrolled to obtain 95% confidence interval (95% CI) at baseline for a sensitivity of 85% (95% CI, 76–91) and a 95% CI for a specificity of 87% (95% CI, 79–93) [11].
Statistics
Clinical and FDG-PET/CT data between groups were compared with Student’s t-test or Mann–Whitney U test for continuous variables and chi-square statistics or a Fisher’s exact test for categorical variables. Sensitivity and specificity were calculated for a positive FDG-PET/CT using the Leuven score as well as the dichotomous diagnostic score. The interrater variability of the Leuven score between the three FDG-PET/CT raters was assessed with intraclass correlation coefficient (ICC) based on a mean-rating, absolute-agreement, two-way mixed-effects model [33]. An ICC estimate within the range of < 0.50, 0.50–0.75, 0.75–0.90, and > 0.90 corresponds to reliability levels categorized as poor, moderate, good, and excellent, respectively [34]. Repeated measurements within the same individuals were assessed using repeated measures ANOVA followed by a Bonferroni post hoc test. Statistical analyses were performed using STATA (version 17, StataCorp, USA). Two-tailed p-values less than 0.05 were considered statistically significant.
Results
Patient characteristics
After 1 year of follow-up, a final diagnosis of isolated PMR was established in 68 patients, while 27 patients were diagnosed with another condition (Fig. 1). The 1-year diagnoses of the 27 non-PMR patients were as follows: reactive inflammatory conditions (n = 8), osteoarthritis (n = 8), rheumatoid arthritis (n = 3), paraneoplastic syndrome (n = 2), chronic pain condition (n = 2), peripheral artery disease (n = 1), adverse event to medication (n = 1), hyperthyroidism (n = 1), and unspecific hip pain (n = 1). Patients experiencing reactive inflammatory conditions presented with PMR mimicking symptoms for durations ranging from 2 to 28 weeks (median 11 weeks). These conditions included PMR-like symptoms following COVID-19 vaccine treated with NSAID (n = 1); symptoms emerging after diverticulitis and urinary tract infection resolving without treatment (n = 1); mild PMR symptoms along with elevated CRP, which resolved spontaneously without a history of infection or vaccine (n = 2); symptoms following COVID-19 infection treated with steroid injections and later with methotrexate and adalimumab (n = 1); and asymmetrical arthritis managed with prednisolone (n = 1). Furthermore, two patients were initially diagnosed with PMR and were treated with prednisolone for 8 weeks (n = 2), after which the medication was discontinued without relapsing symptoms. Subsequent evaluation regarded the symptoms as reactive, associated to a urinary infection and a COVID-19 vaccine (Supplementary Figure S2). In general, the patients with a confirmed clinical diagnosis of PMR after 1 year were more likely to have bilateral shoulder pain, restricted range of shoulder motion, and experience shoulder joint tenderness at baseline examination (Table 1). Compared to non-PMR, the group diagnosed with PMR had significantly higher baseline levels of CRP, global physician VAS score, and patient-reported pain VAS score. Consequently, the PMR-AS was significantly different between the groups. Moreover, individuals with a 1-year clinical diagnosis of PMR were more likely to have a clinical baseline diagnosis of PMR with a sensitivity/specificity of 93%/82% as well as meeting the clinical ACR/EULAR classification criteria at baseline, demonstrating a sensitivity/specificity of 79%/70% for the PMR diagnosis (Table 2).
Among the included patients, the first FDG-PET/CT was performed a median of 3 days after the primary visit (range 1–12 days). The first FDG-PET/CT confirmed GCA in 2 patients, who were excluded from the analyses (Fig. 1). Excluding the GCA patients, complete remission was achieved on 15 mg prednisolone in all but 10 patients. Among these, 9 patients had their dosage escalated to 20–25 mg within the initial 4 weeks, while 1 patient continued with a 15 mg dosage. Over the course of the 1-year follow-up period, 5 patients (7%) who were initially clinically diagnosed with PMR had their initial diagnosis revised (Fig. 1, Supplementary Figure S2). Additionally, among the 26 patients initially clinically diagnosed with other medical conditions, 4 of them (15%) experienced a diagnostic shift to PMR following the 1-year follow-up period (Fig. 1, Supplementary Figure S3).

Flow chart of study flow. AF, Atrial fibrillation; PMR, polymyalgia rheumatica; GCA, giant cell arteritis; FDG-PET/CT, 2-[18F]fluoro-2-deoxy-D–glucose positron emission tomography/computed tomography
FDG-PET/CT data
The Leuven score demonstrated a baseline sensitivity/specificity of 86%/63%, whereas the dichotomous score had a sensitivity/specificity of 82%/70% using the 1-year follow-up diagnosis as the reference standard (Table 2). A subgroup analysis in the non-PMR group showed that 8 out of 13 patients (62%) with inflammatory diseases (reactive inflammatory conditions, rheumatoid arthritis, and paraneoplastic syndrome) had a positive Leuven score, whereas this was only the case in 2 out of 14 patients with other conditions (14%) (p = 0.02). Applying the dichotomous score, 6 out of 13 patients (46%) with non-PMR inflammatory diseases were rated with a positive FDG-PET/CT compared to 1 out of 14 (7%) with other conditions (p = 0.03). In a subgroup analysis, comparing the group of inflammatory controls to the PMR group, the Leuven score showed a specificity of 39%, while the dichotomous score exhibited a specificity of 54% (Table 2). Further baseline characteristics of the inflammatory controls are presented in Table 1.
At week 8, all PMR patients had been tapered to 10–15 mg prednisolone daily and the Leuven score significantly decreased compared to baseline, whereas a short-term prednisolone discontinuation resulted in a significant increase at week 10 (Fig. 2). As a result, the sensitivity of a positive PET Leuven score/dichotomous score was reduced to 36%/41% at week 8 and subsequently improved to 66%/60% at week 10 (Table 3). The interrater reliability for the Leuven score showed the best agreement at baseline (ICC, 0.87 [CI 95%, 0.65–0.93]), the lowest during prednisolone treatment at week 8 (ICC, 0.66 [CI 95%, 0.13–0.85]), and a good level of agreement at week 10 (ICC, 0.79 [CI 95%, 0.36–0.91]).

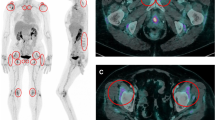
FDG-PET/CT Leuven score of patients with a 1-year diagnosis of PMR at diagnosis, after 8 weeks of prednisolone treatment, and during short-term discontinuation. A Scatter plot of the Leuven score at baseline, week 8, and week 10 for PMR patients. Black vertical lines marking interquartile ranges with connective lines between medians. Grey lines connecting observations between the three time points for each individual. Dashed line marks the Leuven cut-off value of 16. B PET scan of a PMR patient at the three time points
Upon subgrouping PMR patients at the 10-week visit into those experiencing relapse and those still in remission after steroid discontinuation, it was observed that the relapse group had a significantly higher proportion of Leuven positive individuals at week 8 (Fig. 3). Despite the divergence in PET results at week 8, both groups exhibited a low clinical disease activity including a PMR-AS below 7 (Supplementary Table S1). At week 10, the relapse patients exhibited more severe symptoms of PMR and had a tendency towards a higher proportion of Leuven positive individuals (p = 0.051) (Fig. 3). Comparing these two groups at baseline, the only significant difference observed was related to shoulder joint palpation tenderness (Supplementary Table S1).

FDG-PET/CT Leuven score progression of patients with a 1 year-diagnosis of PMR divided into patients with relapse or remission after short-term prednisolone discontinuation. Scatterplot of the FDG-PET/CT Leuven score at baseline, week 8, and week 10 for PMR patients with relapse and remission at 10 weeks. Black vertical lines marking interquartile ranges with connective lines between medians. Grey lines connecting observations between the three time points for each individual. Dashed line marks cut-off value for Leuven score. The table under the scatter plots shows Leuven score and proportions of positive individuals. At 8 weeks, one relapsing individual missed the FDG-PET/CT (scanner breakdown). IQR, interquartile range
Discussion
This is the first study to demonstrate that FDG-PET/CT has limited capability for differentiating PMR from other inflammatory diseases. Furthermore, we provide pioneering data showing the effect of prednisolone for the diagnostic accuracy of FDG-PET/CT in PMR.
The sensitivities of the Leuven composite score and the dichotomous score resembled the previously reported sensitivities, ranging between 85 and 91% for the Leuven score, in prednisolone naïve patient cohorts of suspected PMR [11, 12, 25]. The dichotomous score was introduced to reflect the diagnostic procedure in a routine clinical setting, where the Leuven score may not be applied. This rationale also guided the decision not to incorporate maximal standard uptake value analyses in this study, as such analyses are not recommended for diagnostic purposes [32]. In our study, the specificity of the two scoring methods was remarkably lower compared with the previously reported specificities ranging between 84 and 98% for the Leuven score [11, 12, 25]. This can be explained by a greater proportion of non-PMR patients with other inflammatory diseases within this study (48% vs 19–32%), who exhibit a closer resemblance to patients with PMR. These patients displayed FDG-PET/CT scans that more frequently were positive compared to controls with other conditions. As a result, this subgroup of patients might be predisposed to overtreatment. This was exemplified by one patient with a reactive disease who presented with typical symptoms of PMR as well as a Leuven positive FDG-PET/CT (Supplementary Figure S1, C). The FDG-PET/CT images exhibited a less typical pattern of PMR with extensive uptake along muscle tendons, prompting deliberation within the nuclear physician team. However, following discussion, it was ultimately determined that this pattern bore a resemblance to PMR. Nonetheless, subsequent follow-up revealed the condition to be a reactive response to a COVID-19 vaccine [35]. Therefore, other inflammatory diseases may in general exhibit a less typical FDG-uptake pattern and scoring systems designed to capture this are warranted.
This study is the first to demonstrate the effect of prednisolone for the diagnostic sensitivity of FDG-PET/CT in PMR. A controlled reduction in prednisolone dose, followed by a short-term discontinuation, significantly enhanced the diagnostic sensitivity of FDG-PET/CT for PMR. This underscores the importance of discontinuing prednisolone in patients suspected of PMR before undergoing a confirmative FDG-PET/CT scan, particularly considering that prednisolone treatment for 8 weeks approximately halved the diagnostic sensitivity and reduced the interrater reliability. Previous studies have implied that the diagnostic accuracy of FDG-PET/CT for PMR diminishes with the administration of glucocorticoids. However, none of these studies was explicitly designed to investigate the direct impact of prednisolone on diagnostic accuracy or whether prednisolone should be tapered prior to the FDG-PET/CT [19, 23, 24, 36, 37]. In the study by Brinth et al. [23], a retrospective comparative analysis was conducted including individuals suspected of PMR as well as individuals with other diseases. The results revealed a sensitivity of 81% for the Leuven score among patients who had not been exposed to prednisolone, as opposed to a 24% sensitivity in the group undergoing glucocorticoid treatment. A few studies have reported similar retrospective data from cohorts of PMR patients, demonstrating elevated FDG uptake and a higher number of sites with FDG uptake in steroid-naive patients [19, 24, 37]. Blockmans et al. [36] have conducted a prospective study with repeated PET scans in a cohort of confirmed PMR patients. The data of 22 patients demonstrated a reduction in FDG uptake around the shoulder, hips, and processi spinosi following 3 months of prednisolone treatment. However, this study did not investigate diagnostic accuracy and the effect of prednisolone discontinuation. Given that many patients will already have commenced glucocorticoid treatment prior to FDG-PET/CT referral, our study suggests to taper prednisolone to 5 mg for 1 week, followed by a 1-week discontinuation, before performing FDG-PET/CT scans to increase the diagnostic accuracy and improve interrater consistency. However, it is essential to acknowledge that this suggestion is based on study participants receiving prednisolone for precisely 8 weeks before the short-term taper and discontinuation.
The subgroup analysis, comparing patients in remission after 10 weeks against those with relapse symptoms, revealed that the FDG-PET/CT could not distinguish between these two groups at baseline. However, at 8 weeks, the relapse group exhibited a higher Leuven score, resulting in a higher proportion of individuals with a positive Leuven score. This phenomenon was present despite the fact that CRP levels remained within the normal range for both groups, and both cohorts displayed a low disease activity as indicated by a PMR-AS score of less than 7. Overall, our results imply that FDG-PET/CT signs of PMR may be present prior to the onset of symptoms and elevation of the CRP level in patients with PMR.
PMR patients with relapse at week 10 exhibited clinical and biochemical signs indicative of relapse, in contrast to the remission group. Furthermore, the relapse group showed a tendency towards a higher proportion of Leuven positive individuals compared to the remission group, but this difference was not statistically significant. This result may be underestimated since 10 patients, who experienced incomplete remission or relapse, were unable to complete the short-term prednisolone discontinuation. Nevertheless, it might indicate that patients should ideally undergo prednisolone cessation until they exhibit relapse symptoms to improve the diagnostic accuracy of a subsequent FDG-PET/CT. However, larger studies are needed to confirm this statement.
There are limitations in this study. Similarly, to all previous studies, the clinicians responsible for determining the final PMR diagnosis after 1 year were not blinded for the FDG-PET/CT results due to legal and ethical considerations. However, in this study, the clinical PMR diagnosis was intentionally established prior to the conduction of FDG-PET/CT scans. Among the patients initially diagnosed with PMR, no alterations in diagnosis occurred during the initial 8-week period of prednisolone treatment, except for two patients who were subsequently diagnosed with cancer and two patients with coexisting GCA. Consequently, the final diagnosis rested predominantly on the clinical assessment conducted prior to the FDG-PET/CT, coupled with the evaluation of the response to prednisolone treatment. Another general limitation shared with all previous studies is the absence of systematic documentation regarding pre-screening exclusions before clinical assessment. Consequently, we cannot completely eliminate the risk of a selection bias within this cohort. However, the implementation of rapid referral clinics ensured the inclusion of a unique cohort that represents the entirety of the PMR population. The general practitioners were actively encouraged to refer all suspected PMR individuals to our rapid access clinics. This ensured that the composition of the control group closely resembled what has been previously reported in studies evaluating the rapid access strategy [38]. Thus, we believe that the extent of selection bias typically encountered in hospital-based cohorts might not have been as pronounced in this investigation compared to studies that apply the conventional referral procedure, where only approximately 25% of the entire PMR population is referred from primary care [14]. Finally, in this study, we opted to evaluate the FDG-PET/CT images using only the Leuven score as well as a dichotomous score. Although other less validated scoring methods have been developed, these mainly rely on retrospective data or have selected control groups not necessarily comprising suspected PMR patients [12, 19,20,21,22,23,24]. As a result, we considered the Leuven score to be the most reliable scoring method.
Conclusion
This is the first prospective study performing FDG-PET/CT in treatment naïve patients suspected of PMR and including the effect of prednisolone treatment and a short-term discontinuation. The study shows that FDG-PET/CT has limited diagnostic accuracy for differentiating PMR from other inflammatory diseases. Furthermore, we provide pioneering data showing that prednisolone treatment considerably reduces the diagnostic sensitivity of FDG-PET/CT for PMR, whereas a short-term discontinuation can increase the sensitivity, although it remains below the pre-treatment level.
Data availability
Data are available on reasonable request.
References
Gonzalez-Gay MA, Garcia-Porrua C, Salvarani C, Olivieri I, Hunder GG. The spectrum of conditions mimicking polymyalgia rheumatica in Northwestern Spain. J Rheumatol. 2000;27:2179–84.
Owen CE, Buchanan RR, Hoi A. Recent advances in polymyalgia rheumatica. Intern Med J. 2015;45:1102–8. https://doi.org/10.1111/imj.12823.
Paltta J, Suuronen S, Pirilä L, Palomäki A. Differential diagnostics of polymyalgia rheumatica in a university hospital in Finland. Scand J Rheumatol. 2023;52:689–95. https://doi.org/10.1080/03009742.2023.2215044.
Dasgupta B, Cimmino MA, Kremers HM, Schmidt WA, Schirmer M, Salvarani C, et al. 2012 Provisional classification criteria for polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Arthritis Rheum. 2012;64:943–54. https://doi.org/10.1002/art.34356.
Chuang TY, Hunder GG, Ilstrup DM, Kurland LT. Polymyalgia rheumatica: a 10-year epidemiologic and clinical study. Ann Intern Med. 1982;97:672–80. https://doi.org/10.7326/0003-4819-97-5-672.
Jones JG, Hazleman BL. Prognosis and management of polymyalgia rheumatica. Ann Rheum Dis. 1981;40:1–5. https://doi.org/10.1136/ard.40.1.1.
Bird HA, Esselinckx W, Dixon AS, Mowat AG, Wood PH. An evaluation of criteria for polymyalgia rheumatica. Ann Rheum Dis. 1979;38:434–9. https://doi.org/10.1136/ard.38.5.434.
Healey LA. Polymyalgia rheumatica and the American Rheumatism Association criteria for rheumatoid arthritis. Arthritis Rheum. 1983;26:1417–8. https://doi.org/10.1002/art.1780261201.
Ozen G, Inanc N, Unal AU, Bas S, Kimyon G, Kisacik B, et al. Assessment of the New 2012 EULAR/ACR clinical classification criteria for polymyalgia rheumatica: a prospective multicenter study. J Rheumatol. 2016;43:893–900. https://doi.org/10.3899/jrheum.151103.
Lee KA, Kim HS, Lee SH, Kim HR. Diagnostic performance of the 2012 EULAR/ACR classification criteria for polymyalgia rheumatica in Korean patients. Int J Rheum Dis. 2020;23:1311–7. https://doi.org/10.1111/1756-185x.13923.
Henckaerts L, Gheysens O, Vanderschueren S, Goffin K, Blockmans D. Use of 18F-fluorodeoxyglucose positron emission tomography in the diagnosis of polymyalgia rheumatica-a prospective study of 99 patients. Rheumatology (Oxford). 2018;57:1908–16. https://doi.org/10.1093/rheumatology/kex376.
van der Geest KSM, van Sleen Y, Nienhuis P, Sandovici M, Westerdijk N, Glaudemans A, et al. Comparison and validation of FDG-PET/CT scores for polymyalgia rheumatica. Rheumatology (Oxford). 2022;61:1072–82. https://doi.org/10.1093/rheumatology/keab483.
Nielsen AW, Hemmig AK, de Thurah A, Schmidt WA, Sattui SE, Mackie SL, et al. Early referral of patients with suspected polymyalgia rheumatica - a systematic review. Semin Arthritis Rheum. 2023;63: 152260. https://doi.org/10.1016/j.semarthrit.2023.152260.
Donskov AO, Mackie SL, Hauge EM, Toro-Gutiérrez CE, Hansen IT, Hemmig AK, et al. An international survey of current management practices for polymyalgia rheumatica by general practitioners and rheumatologists. Rheumatology (Oxford). 2023. https://doi.org/10.1093/rheumatology/keac713.
Auzary C, Le Thi HD, Delarbre X, Sbai A, Lhote F, Papo T, et al. Subacute bacterial endocarditis presenting as polymyalgia rheumatica or giant cell arteritis. Clin Exp Rheumatol. 2006;24:S38-40.
Meudec L, Jelin G, Goossens J, Forien M, Jacquier H, Dieudé P, et al. Whipple disease mimicking polymyalgia rheumatica with initial response to tocilizumab. Intern Med J. 2021;51:2151–2. https://doi.org/10.1111/imj.15281.
El Hasbani G, Taher AT, Abi-Ghanem AS, Nassif S, Bizri AR, Uthman I. Polymyalgia rheumatica-like presentation in a case of diffuse large B-cell lymphoma: a diagnostic pitfall. J Int Med Res. 2021;49:3000605211018595. https://doi.org/10.1177/03000605211018595.
Yuge S, Nakatani K, Yoshino K, Koyama T. Diagnosing polymyalgia rheumatica on (18)F-FDG PET/CT: typical uptake patterns. Ann Nucl Med. 2018;32:573–7. https://doi.org/10.1007/s12149-018-1269-5.
Sondag M, Guillot X, Verhoeven F, Blagosklonov O, Prati C, Boulahdour H, et al. Utility of 18F-fluoro-dexoxyglucose positron emission tomography for the diagnosis of polymyalgia rheumatica: a controlled study. Rheumatology (Oxford). 2016;55:1452–7. https://doi.org/10.1093/rheumatology/kew202.
Owen CE, Poon AMT, Yang V, McMaster C, Lee ST, Liew DFL, et al. Abnormalities at three musculoskeletal sites on whole-body positron emission tomography/computed tomography can diagnose polymyalgia rheumatica with high sensitivity and specificity. Eur J Nucl Med Mol Imaging. 2020;47:2461–8. https://doi.org/10.1007/s00259-020-04731-z.
Flaus A, Amat J, Prevot N, Olagne L, Descamps L, Bouvet C, et al. Decision tree with only two musculoskeletal sites to diagnose polymyalgia rheumatica using [(18)F]FDG PET-CT. Front Med (Lausanne). 2021;8: 646974. https://doi.org/10.3389/fmed.2021.646974.
Ikuma D, Sawa N, Yamanouchi M, Oba Y, Mizuno H, Suwabe T, et al. Diagnostic value of 18F-FDG positron emission tomography and computed tomography for differentiating polymyalgia rheumatica and rheumatoid arthritis: using classification and logistic regression tree (CART) analysis. Mod Rheumatol. 2023. https://doi.org/10.1093/mr/road051.
Brinth LS, Hansen A, Jensen DV, Madsen OR, Broholm R, Krakauer M. Diagnostic value of composite and simplified FDG-PET/CT scores in polymyalgia rheumatica and the influence of recent glucocorticoid treatment-a retrospective diagnostic cohort study. Diagnostics (Basel). 2023;13:514. https://doi.org/10.3390/diagnostics13030514.
Casadepax-Soulet C, Benali K, Crestani B, Piekarski E, Mahida B, Ebstein E, et al. Fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography in polymyalgia rheumatica: an observational study. Clin Exp Rheumatol. 2023;41:1456–62. https://doi.org/10.55563/clinexprheumatol/kqyki5.
Moreel L, Boeckxstaens L, Betrains A, Van Hemelen M, Vanderschueren S, Van Laere K, et al. Diagnostic accuracy and validation of (18)F-fluorodeoxyglucose positron emission tomography scores in a large cohort of patients with polymyalgia rheumatica. Front Med (Lausanne). 2022;9:1026944. https://doi.org/10.3389/fmed.2022.1026944.
Duncan JR, Carr D, Kaffenberger BH. The utility of positron emission tomography with and without computed tomography in patients with nonmelanoma skin cancer. J Am Acad Dermatol. 2016;75:186–96. https://doi.org/10.1016/j.jaad.2016.01.045.
Dejaco C, Singh YP, Perel P, Hutchings A, Camellino D, Mackie S, et al. 2015 Recommendations for the management of polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Ann Rheum Dis. 2015;74:1799–807. https://doi.org/10.1136/annrheumdis-2015-207492.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–81. https://doi.org/10.1016/j.jbi.2008.08.010.
Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95: 103208. https://doi.org/10.1016/j.jbi.2019.103208.
Leeb BF, Bird HA. A disease activity score for polymyalgia rheumatica. Ann Rheum Dis. 2004;63:1279–83. https://doi.org/10.1136/ard.2003.011379.
Dejaco C, Ramiro S, Bond M, Bosch P, Ponte C, Mackie SL, et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice: 2023 update. Ann Rheum Dis. 2023. https://doi.org/10.1136/ard-2023-224543.
Slart R. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur J Nucl Med Mol Imaging. 2018;45:1250–69. https://doi.org/10.1007/s00259-018-3973-8.
Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86:420–8. https://doi.org/10.1037/0033-2909.86.2.420.
Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15:155–63. https://doi.org/10.1016/j.jcm.2016.02.012.
Nielsen AW, Hansen IT, Gormsen LC, Hauge EM, Keller KK. Self-limiting reactive disease mimicking polymyalgia rheumatica following Moderna COVID-19 vaccine. Scand J Rheumatol. 2022;51:411–3. https://doi.org/10.1080/03009742.2022.2070959.
Blockmans D, De Ceuninck L, Vanderschueren S, Knockaert D, Mortelmans L, Bobbaers H. Repetitive 18-fluorodeoxyglucose positron emission tomography in isolated polymyalgia rheumatica: a prospective study in 35 patients. Rheumatology (Oxford). 2007;46:672–7. https://doi.org/10.1093/rheumatology/kel376.
Camellino D, Paparo F, Morbelli SD, Pesce G, Bauckneht M, Bagnasco M, et al. Clinical and FDG-PET/CT correlates in patients with polymyalgia rheumatica. Clin Exp Rheumatol. 2022;40:78–85. https://doi.org/10.55563/clinexprheumatol/4r78yg.
Frølund LL, Våben C, Dam M, Kjær SG, Nielsen BD, Østgård RD, et al. Fast track clinic for early diagnosis of polymyalgia rheumatica: Impact on symptom duration and prednisolone initiation. Joint Bone Spine. 2021;88: 105185. https://doi.org/10.1016/j.jbspin.2021.105185.
Acknowledgements
The authors wish to express their gratitude to our study nurses (Marie Bækmark Kjær, Else Sloth Rousing, Mette Fomsgaard, Tina Majbritt Thygesen, Agnete Aagaard Jensen, and Maja Krogh) for their indispensable contribution in patient recruitment and data collection.
Funding
Open access funding provided by Aarhus University Hospital This work was supported by the Danish Rheumatism Association, Frimodt-Heineke’s Foundation, Aase and Ejnar Danielsen’s Foundation, A.P. Moller Foundation, and Regional Hospital Central Jutland Research Foundation. In addition, AWN and KKK have received grants from the Health Research Foundation of Central Denmark and Aarhus University Hospital for research in PMR.
Author information
Authors and Affiliations
Contributions
All authors played a substantial role in shaping the study, contributing to its conception and design, data acquisition, data analyses, and data interpretation. AWN, ITH, BDN, SGK, JBN, CMS, and KKK were responsible for conducting the study visits, including data collection. AWN, LCG, and KR conducted the data analyses. Statistical analyses and data interpretation were carried out by AWN, with guidance from EMH, LCG, and KKK. All authors provided feedback on earlier drafts of the manuscript and gave their approval for the final version. AWN is acting as a guarantor for the study.
Corresponding author
Ethics declarations
Ethics approval
This study complies with the Declaration of Helsinki and the study protocol was approved by the Regional Scientific Ethical Committee for the Central Denmark Region (reference number 1–10-72–99-19) and the Internal List of Research Projects in Central Denmark Region—former Danish Data Protection Agency (reference number: 1–16-02–166-19).
Consent to participate
Informed written consent was obtained from all individual participants included in this study.
Competing interests
AWN, ITH, SGK, JB-N, CMS, LCG, and KK have nothing to declare. BDN has received speaking fees unrelated to this manuscript from Novartis an AbbVie. EMH has received grants unrelated to this manuscript from Novo Nordic Foundation, Roche, Novartis, and personal fees from AbbVie, Sanofi, SOBI, Merck Sharp & Dohme, and Union Chimique Belge.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nielsen, A.W., Hansen, I.T., Nielsen, B.D. et al. The effect of prednisolone and a short-term prednisolone discontinuation for the diagnostic accuracy of FDG-PET/CT in polymyalgia rheumatica—a prospective study of 101 patients. Eur J Nucl Med Mol Imaging 51, 2614–2624 (2024). https://doi.org/10.1007/s00259-024-06697-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-024-06697-8