
Abstract
Over half of patients diagnosed with acute myeloid leukemia (AML) are 65 years or older. We examined patient characteristics, treatment patterns, and survival among elderly patients in routine clinical practice. We utilized a retrospective cohort analysis of first primary AML patients in the linked Surveillance, Epidemiology, and End Results (SEER)-Medicare database. Patients were diagnosed between January 1, 2000 and December 31, 2009, >66 years, and continuously enrolled in Medicare Part A and B in the year prior to diagnosis. Kaplan-Meier curves and Cox proportional hazards regression assessed overall survival by treatment. There were 3327 (40 %) patients who received chemotherapy within 3 months of diagnosis. Treated patients were more likely younger, male, and married, and less likely to have secondary AML and poor performance indicators and comorbidity score compared to untreated patients. In multivariate survival analysis, treated patients exhibited a significant 33 % lower risk of death compared to untreated patients. Significant survival benefits were noted with receipt of intensive and hypomethylating agent (HMA) therapies compared to no therapy. A survival benefit with allogeneic hematopoietic stem cell transplantation was seen in younger Medicare patients. This real-world study showed that about 60 % of elderly AML patients remain untreated following diagnosis. Use of anti-leukemic therapy was associated with a significant survival benefit in this elderly cohort.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A disproportionate number of newly diagnosed acute myeloid leukemia (AML) occurs in elderly patients, and it is also the leading cause of mortality from leukemia in the USA [1, 2]. The median age at diagnosis is 66 years, and incidence increases with age with over half of the patients diagnosed at age 65 or older[3]. The use of chemotherapy has increased over time but fewer than half of elderly patients receive anti-leukemic therapy and their outcomes remain dismal [4–6]. After successful induction of remission, disease relapse is inevitable in the majority of cases without and despite additional post-remission therapy [7]. Without treatment, patients succumb to their illness within weeks to months of diagnosis [8].
Treatment efficacy and tolerability have been shown to deteriorate markedly with age [4]. Conventional chemotherapy treatments for AML may be highly toxic, usually requiring prolonged inpatient treatment [6]. For this reason, the NCCN guidelines describe separate treatment recommendations for patients older than 60 years based on performance status, cytogenetic or molecular mutation, and comorbid conditions rather than relying on chronologic age alone [7]. For medically fit older adults, treatment with a combination of an anthracycline and standard dose cytarabine is recommended rather than other chemotherapy regimens or supportive care alone. For older adults with poor physical function and/or unfavorable risk disease, supportive care alone or less intensive chemotherapy with DNA hypomethylating agents or low-dose cytarabine is recommended. The use of allogeneic hematopoietic stem cell transplantation (HSCT) is considered a potential cure for AML, but its use is limited in older patients because of significant baseline comorbidities and increased transplant-related morbidity and mortality [9, 10]. Nonetheless, data from the Swedish Acute Leukemia Registry show that most patients up to 80 years actually tolerate and benefit from intensive treatment, despite deteriorating organ function [11, 12].
Although patients 65 years or older represent the majority of patients with cancer in the USA, a minority of them are enrolled in randomized clinical trials (RCTs). In fact, several studies have shown that only 1– % of elderly cancer patients are participating in clinical trials, thus providing a limited evidence base in which to evaluate treatment efficacy and safety in this population [13–15]. The most frequently cited factors for clinical trial ineligibility were advanced age or the presence of significant comorbidity [16]. In order to address the need for additional data in this population, given the limited clinical trial participation, the increased incidence of AML due to the aging population, and the limited treatment options, we used population-based data to examine Medicare beneficiaries following their diagnosis of AML. The information obtained provides an important context for identifying opportunities to improve the quality of treatment strategies and evaluate the benefits of new treatments under investigation.
Methods
Data sources
Patients were identified from the linkage of two data sources, the Surveillance, Epidemiology, and End Results (SEER) program database from the National Cancer Institute and the Medicare enrollment and claims files from the Centers for Medicare and Medicaid Services. Details of the linked SEER-Medicare database have been published elsewhere [17]. Briefly, the database combines clinical, demographic, cancer diagnosis, and cause of death information with claims data for adults age 65 and older enrolled in Medicare Parts A and B. SEER is a nationally representative collection of 18 population-based registries of all incident cancers from diverse geographic areas covering approximately 26 % of the US population. All incident cancer patients reported to the SEER registries are cross-matched with a master file of Medicare enrollment [18]. All Medicare beneficiaries receive Part A coverage (inpatient care, skilled nursing, home health care, and hospice care). Approximately 95 % of beneficiaries subscribe to Part B, which covers physician services and outpatient care. The SEER-Medicare linkage included all Medicare eligible persons appearing in the SEER data through 2009 and their Medicare claims for Part A (inpatient) and Part B (outpatient and physician services) through 2010. Institutional review board approval was waived because the SEER-Medicare data lack personal identifiers.
Study population
Patients were eligible for inclusion in the study if diagnosed with first primary AML between January 1, 2000 and December 31, 2009, at least 66 years of age, and continuously enrolled in Medicare Parts A and B in the 12 months prior to diagnosis. Patients were excluded if their date of death was recorded prior to or the same month as diagnosis, if they were enrolled in a health maintenance organization (HMO) at any time during the 12 months prior to diagnosis (because complete claims data were unavailable for these patients), and if they had two or more claims for chemotherapy prior to diagnosis (to ensure that the cases were previously untreated).
Study variables
SEER program registries routinely collect data on patient demographics (age, race/ethnicity, residence, and socioeconomic status [income and education per census tract]); primary tumor site, tumor morphology, and stage at diagnosis; first course of treatment; and follow-up for vital status. AML diagnosis was based on the International Classification of Disease for Oncology (3rd edition, ICD-O-3) histology codes in the SEER data. Median annual household income at the census tract level, and percentage of adults aged 25 or older with at least some college education at the ZIP code level in the SEER data were used as a proxy for socioeconomic status.
Risk status in AML is based on cytogenetics and molecular abnormalities, which were not available in the SEER data. Prior myelodysplastic syndrome (MDS) or myeloproliferative neoplasm (MPN) that transforms into AML has also poor prognostic features and occurs more commonly among elderly patients [19]. In the absence of cytogenetic data, prior MDS or MPN was used as a proxy for high-risk patients and was identified using diagnosis codes in Medicare Parts A and B claims files prior to AML diagnosis. SEER also does not include measures of performance status, such as Eastern Cooperative Oncology Group. Instead, we used Medicare claims to identify several indictors of poor performance status (PPI) [20], including the use of oxygen and related respiratory therapy supplies, wheelchair and supplies, home health agency services, and skilled nursing facility services that occurred 12 months prior to AML cancer diagnosis.
To assess baseline comorbidity burden, we utilized the National Cancer Institute (NCI) comorbidity index [21] to identify the 15 non-cancer comorbidities from the Charlson Comorbidity Index [22]. The index accounts for the number and seriousness of the conditions and a higher score indicates a greater burden of comorbid disease. Diagnosis and procedure codes were identified from Medicare claims 1 year prior to diagnosis and must appear on at least two different claims that are more than 30 days apart to ensure that “rule out” diagnoses are not counted as comorbid conditions.
Chemotherapy administration was identified using International Classification of Disease (9th revision), Clinical Modification (ICD-9-CM) diagnosis codes and procedural codes, and Healthcare Common Procedural Coding System (HCPCS) “J” codes were used to identify the specific drug administered [23]. The absence of these claims indicated lack of treatment. The first chemotherapy claim within 3 months from diagnosis indicated the start of therapy. Patients were classified into treatment groups based on all chemotherapy administered during the first 60 days after treatment initiation. Chemotherapy agent definition was not possible in approximately 70 % of patients who received therapy because chemotherapy was administered during inpatient stays which are paid based on ICD-9 diagnosis or procedure codes only and not chemotherapy codes. Medicare claims files were also searched for ICD-9-CM and HCPCS codes to identify patients undergoing allogeneic HSCT anytime during follow-up.
Overall survival was measured from date of diagnosis to date of death. The date of death was assigned by using the Medicare date or SEER date of death if Medicare date was missing. All other patients were assumed to be alive at the end of the follow-up period (December 31, 2010), although they may have been censored earlier for other reasons such as the development of a second primary cancer or Medicare claims no longer available.
Statistical analysis
All statistical analyses were performed using SAS software, version 9.1.3 (SAS Institute Inc., Cary, NC). Demographic and clinical characteristics were summarized descriptively by treatment status (treated vs. not treated) and treatment type. Chi-square test for categorical variables and ANOVA or t test for continuous variables determined differences between groups. We considered a p value < .05 to be statistically significant.
In the overall survival analyses, we made comparisons between the treated and not treated patients, between treated patients receiving HSCT and those who did not, and between those receiving low-dose therapy with a DNA methyltransferase (DNMT) inhibitor (azacitidine or decitabine (HMA therapy)), those receiving aggressive induction therapy (cytarabine + anthracycline (intensive therapy)), and those not receiving treatment. Kaplan-Meier survival curves and corresponding log rank tests examined unadjusted overall survival by treatment group. Since timing of treatment initiation differed between patients, the relationship between treatment and survival was evaluated using a Cox regression model with treatment as a time-dependent factor. In the time-varying Cox model, all patients belong to the “not treated” group and only switched to the “treated” group at the time of treatment receipt. Other confounders included in the Cox model were selected a priori from baseline demographic and clinical characteristics..
To assess the risk of early death (30-day mortality and 60-day mortality) after diagnosis, we also used a Cox regression model with treatment as a time-dependent factor. The treated group was limited to patients who received treatment within 30 days after diagnosis to minimize the introduction of immortal time bias in the analysis (period of follow-up time during which death cannot occur) [24].
As a sensitivity exercise for the comparison between HMA therapy, intensive therapy, and no treatment, we also conducted a propensity score-matched survival analysis. Multinomial logistic regression was used to calculate a propensity score—the conditional probability that each patient would be assigned to a specific treatment group given the patient’s pretreatment variables [25, 26]. Pairwise matching was conducted where each patient receiving HMA therapy was matched to one untreated patient and each patient receiving intensive therapy was matched to one untreated patient. Matching variables were age, sex, race, marital status, education, geographic region, year diagnosed, prior MDS, poor performance indicators, and comorbidity score. Matched survival analysis was completed using the Cox proportional hazards regression model, stratifying on the matched pair. Factors that were still found to be significantly different after matching (age, geographic region, and year diagnosed) were included as covariates in the Cox proportional hazards models.
In the survival models, follow-up was calculated beginning on the date of diagnosis up until the first occurrence of a censoring event: date of death, development of a second primary tumor, the last date for which Medicare claims are available, or the end of the follow-up period (December 31, 2010).
Results
Treatment trends over time
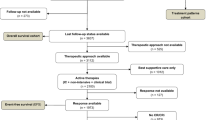
Of the 8336 patients who met all study criteria, 3327 (40 %) received treatment with chemotherapy within 3 months of diagnosis and 5009 (60 %) did not (Table 1). Treatment rates increased over the study time period from 35 % in 2000 to 50 % in 2009 (Fig. 1). Treated patients were younger at diagnosis with mean age of 75 compared to those not receiving treatment (81 years; p < .0001). Fifty-two percent of untreated patients were over the age of 80 compared to 20 % in the treated group (p < .0001). Treated patients were also more likely to be male (55 vs. 50 %), married (61 vs. 47 %), and have lower incidence of secondary AML (15 vs. 19 % prior MDS or MPN), were less likely to have PPI (7 vs. 17 %), and had lower comorbidity burden (p < .0001) than untreated patients.

Treatment status by year of diagnosis
The median unadjusted overall survival was 2.5 months for the overall population and was longer for treated patients (5.0 months) compared to that for untreated patients (1.5 months; log rank p < .0001; Fig. 2a). As the observed overall survival was not significantly different between patients initiating therapy between 0–30 days, 30–60 days, and 60–90 days from diagnosis, all treated patients were analyzed as a single cohort. In multivariate survival analysis (Table 2), treated patients exhibited a 33 % lower risk of death compared to untreated patients (hazard ratio (HR) = 0.67; 95 % confidence interval (CI) = 0.64–0.71). Increasing age, increasing comorbidity score, and PPI were significantly associated with higher mortality risks. Prognosis also improved over time with a 7–12 % reduction in mortality during the years 2002–2004 (HR = 0.93; 95 % CI = 0.87–0.99), 2005–2007 (HR = 0.88; 95 % CI = 0.82–0.93), and 2008–2009 (HR = 0.90; 95 % CI = 0.84–0.97) compared to that during 2000–2001 (data not shown).

a Unadjusted overall survival by treatment status. b Unadjusted overall survival by treatment type. c Unadjusted overall survival among treated patients with and without HSCT
We conducted exploratory subgroup analyses on the impact of treatment versus no treatment to examine whether specific prognostic subgroups benefited more or less from treatment (Supplementary Table S1). Receipt of treatment had a larger impact on mortality risk in the subgroup without a prior MDS (35 % reduction in mortality) compared to the subgroup with a prior MDS (20 % reduction in mortality). Treated patients in the younger age cohort, female gender, with presence of PPI, and NCI comorbidity score 1+ exhibited greater reductions in mortality compared to their subgroup counterparts. Marital status subgroups showed similar benefits with receipt of treatment.
The multivariate analysis of factors predicting early death is shown in Table 2. The median time to treatment initiation was 17 days. There were 1747 (24 %) of patients who died within 30 days of diagnosis and 3429 (47 %) that died within 60 days of diagnosis. Stratifying by treatment status, 210 (9 %) treated patients and 1537 (31 %) untreated patients died within 30 days of diagnosis. Treated patients had a 66 % lower likelihood of early death within 30 days of diagnosis and a 44 % lower likelihood of early death within 60 days of diagnosis compared to the untreated cohort. Other factors associated with increased risk of early death include older age, unmarried, higher comorbidity burden, and presence of poor performance indicators.
Outcomes according to treatment modality
Patients receiving intensive therapy were younger (mean age 73 vs. 78 and 81), were more likely male (62 vs. 59 and 50 %), were married (71 vs. 61 and 47 %), had less secondary AML (7 vs. 21 and 19 % with prior MDS), were less likely to have PPIs (2 vs. 9 and 17 %), and had lower comorbidity score compared to those receiving HMA therapy and not treated, respectively (Table 3). Similarities in age, comorbidity burden, and proportion with high-risk disease were noted in HMA therapy and not treated patients. The median unadjusted overall survival (Fig. 2b) was longer for patients treated with intensive therapy (18.9 months) compared to that with HMA therapy (6.6 months) and not treated (1.5 months; log rank p < .0001). After adjusting for all covariates in the survival model, a 67 % reduction in mortality was observed among patients treated with intensive therapy and a 50 % reduction in mortality was observed among patients treated with HMA therapy, compared to not treated (Table 4). The propensity score-matched survival analysis demonstrated similar risk reductions for both intensive (62 % reduction in mortality) and HMA (59 % reduction in mortality) regimens compared to patients who were not treated. Increasing age, increasing comorbidity score, and presence of PPIs were associated with significant increases in mortality. In a subset analysis stratified by age, similar mortality risk reductions with receipt of intensive and HMA therapies were maintained in the younger (≤75) and older (>75) cohorts (data not shown).
Effect of allogeneic stem cell transplantation on survival
Among treated patients, there were 276 (8 %) who underwent HSCT therapy and 3051 (92 %) who did not (Table 3). HSCT patients were younger at diagnosis with mean age of 73 compared to the non-HSCT group (75 years; p < .0001). Seventy percent of HSCT patients compared to 55 % of non-HSCT patients were under the age of 75 at diagnosis. HSCT patients were also more likely to be male (62 vs. 55; p = 0.0228). There were no statistical differences in comorbidity burden, PPI, or prior MDS between both groups. Figure 2c shows that the unadjusted median overall survival was higher for HSCT (9.7 months) compared to the non-HSCT group (4.7 months; log rank p ≤ 0.0001). In multivariate survival analysis (Table 5), treated patients who underwent HSCT had a significant 21 % lower risk of death compared to those who did not receive HSCT. Increasing age, male gender, unmarried, prior MDS, PPI, and increasing comorbidity score were significantly associated with higher risks of post-treatment mortality. In an exploratory subset analysis stratified by age, the survival benefit with HSCT was only demonstrated in the younger age cohort ≤75 years old, and no difference in mortality risks was noted in the older age cohort >75 years (Table 5).
Discussion
Although therapy use has increased over time, this large observational study of Medicare beneficiaries showed that currently, about 50 % of elderly AML patients remain untreated following diagnosis, which represents an unmet need. We observed a significant survival benefit with receiving anti-leukemic therapy, even among the HMA therapy group who had similar characteristics to the untreated patients. Further, improved survival after receiving intensive therapy compared to HMA therapy was noted after adjustment for confounding variables. However, when patients were matched on sex, race, marital status, education, prior MDS, PPI, and comorbidity score, we found mortality risk reductions of a similar magnitude with receiving both regimens. Overall, these real-world results provide further support that age alone should not deter the use of guideline-recommended therapies particularly because of the high disparities in outcomes between treatment receipt and palliative care.
Results from our observational study have been supported in prior RCTs involving elderly patients. Over 20 years ago, the European Organization for Research and Treatment of Cancer (EORTC) Leukemia Group demonstrated an improvement in complete remission rate and overall survival for AML patients aged 65 years or older immediately treated with induction chemotherapy compared to supportive measures only [27]. Significant clinical improvements in outcomes have also been demonstrated in elderly patients following HMA therapy. When compared to best supportive care (BSC) or low-dose cytarabine (LDAC), treatment with decitabine was associated with a significantly higher CR rate plus CRp rate, a trend toward improvement in median overall survival and a 20 % reduction in the risk of death [28]. In comparison, two separate studies compared the effects of azacitidine against conventional care regimens (CCRs) including BSC, LDAC, and conventional induction chemotherapy. In oligoblastic AML (<30 % blasts), azacitidine treatment was associated with significant improvements in median OS and 2-year survival, albeit no improvement in complete remission rate was observed [29]. In patients with >30 % blasts, preliminary reports showed a trend toward improvement in median OS, a 15 % reduction in the risk of death, improved 1-year survival, and no differences in the CR rate plus CRp rate [30]. No significant safety concerns were raised in these studies following HMA therapy.
Our results confirm data from other registry-based analyses that showed that elderly AML patients who received treatment exhibited a lower early death rate compared to untreated patients or palliation [11, 12, 31]. Although our multivariate analysis demonstrated a greater reduction in mortality in patients receiving aggressive induction chemotherapy compared to HMA therapy, both therapeutic options appeared to be equally better than supportive measures when the cohorts were properly matched for relevant cofounders.
Only 8 % of patients receiving chemotherapy underwent subsequent HSCT therapy. Chronologic age appears to be the driving factor in receiving HSCT. HSCT therapy was associated with a 20 % lower risk of death compared to patients receiving chemotherapy only, and the survival benefit was more pronounced among the younger cohort (≤75 years) with a 37 % reduction in mortality risk. Although myeloablative allogeneic HSCT is rarely recommended in older patients with significant comorbidities, reduced-intensity conditioning (RIC) allogeneic HSCT is encouraging when used as post-remission therapy [9, 10, 32]. The NCCN guidelines consider RIC allogeneic HSCT an additional option for patients 60 years or older as post-remission therapy in those who achieved complete response from induction therapy [7]. Although our observations are at best hypothesis generating, they raise the question of whether allogeneic HSCT provides therapeutic benefit to AML patients older than 75 years of age. Prospective and well-controlled clinical trials are needed to define the role of allogeneic HSCT as post-remission therapy in this cohort of patients.
In the current study, receipt of treatment varied by gender, marital status, income, and geographic region, similar to patterns observed in prior oncology research [33–35].Our results also demonstrate that married AML patients were more likely to receive therapy and had higher survival compared to unmarried patients, even after adjusting for known confounders [35]. These results highlight the importance of marital status, likely as a surrogate of social-economic support in patients with AML, and confirm results from previous reports focusing on solid tumor malignancies. Further research is warranted to better quantify how nonclinical factors such as social support contribute to receipt of cancer therapy and outcomes.
The finding that patients receiving intensive therapy were younger, were more likely male, were married, had less secondary AML, were less likely to have PPIs, and had lower comorbidity score compared to those receiving HMA therapy and no treatment may reflect a belief among physicians that elderly patients are frailer and less able to tolerate aggressive or more toxic treatments [4, 36–38]. These observations are in agreement with previously reported patterns of treatment selection. For example, in two recent randomized trials where pre-selection of CCR was performed prior to randomization, subjects assigned to aggressive treatment modalities were a median of 5–8 years younger than their counterparts assigned to less intensive regimens [29, 30]. Elderly patients also have diverse attitudes toward cancer treatment; some desire aggressive treatment modalities while others decline therapies offered by their oncologist [39, 40]. These age disparities in treatment patterns are associated with higher mortality [4, 5], and our results provide further support that demographic factors such as age should not discourage the use of guideline-recommended therapies.
Strengths and limitations
Use of the SEER-Medicare data for this type of analysis has several strengths, including the large sample size from a population-based registry and the diverse geographic representation of AML patients in the USA. The database includes longitudinal data with claims for covered services from the time a person is eligible for Medicare until the date of death regardless of residence or service area.
The results of the comparative effectiveness analysis should be interpreted with caution due to the large amount of missing data and resulting small sample size of treatment groups. Induction chemotherapy with curative intent in the outpatient setting is applied to very select elderly AML patients, and our findings may not be representative of the general patient population receiving intensive induction therapy. Conventional chemotherapy treatments for AML are highly toxic [8] and generally requires inpatient treatment. Inpatient stays are paid based on ICD-9 diagnosis or procedure codes only, and therefore, we were unable to define the type of chemotherapy received for 70 % of the treated cohort without the specific chemotherapy J code. Further, dose selection was at the discretion of the physician and dosing information could not be determined retrospectively from available data within the claims dataset.
The SEER registry does not collect baseline molecular and cytogenetic information for leukemia, and our surrogate for stage (including claims for prior MDS as a marker of disease severity) may not adequately assess stage in all patients in our study. The SEER-Medicare data did not contain remission status prior to HSCT, and type of prior anti-AML therapy was not known for the majority of patients receiving transplant. In addition, the SEER data does not include measures of performance status, and using Medicare claims to identify several indictors of poor performance may also be subject to bias. Performance status influences clinicians’ decisions to treat or the specific regimen to administer. Information regarding treatment patterns and characteristics of patients enrolled in health maintenance organizations (HMOs) or fee-for-service plans was not available since Medicare does not collect these data. Treatment patterns, prognosis, and complications may differ between these alternative health care plans and Medicare enrollees, and this would be a productive area for additional evaluation.
Conclusion
Overall, these real-world results provide further support that age alone should not deter the use of guideline-recommended therapies in AML. Our results highlight the benefit of treatment in contrast to palliative therapy in this underserved patient population of elderly AML patients and suggest that anti-leukemic regimens should be strongly considered in the majority of older patients. But, even with treatment, outcomes remain dismal, and given this important unmet medical need, many new agents are currently in development for older patients with AML [41–44]. Our findings provide an important context for therapeutic selection that occurs in older patients with AML in the USA. Moving forward, it will be important to identify patients less likely to be treated at diagnosis and design clinical trials to address the therapeutic challenges that exist in this cohort of patients.
References
Yamamoto JF, Goodman MT (2008) Patterns of leukemia incidence in the United States by subtype and demographic characteristics, 1997-2002. Cancer Causes Control 19:379–390
Siegel R, Naishadham D, Jemal A (2013) Cancer statistics, 2013. CA Cancer J Clin 63:11–30
National Cancer Institute. SEER Stat Fact Sheets: Acute Myeloid Leukemia. Bethesda, MD:. Available from URL: http://seer.cancer.gov/statfacts/html/amyl.html. Accessed November 2013
Appelbaum FR, Gundacker H, Head DR et al (2006) Age and acute myeloid leukemia. Blood 107:3481–3485
Kantarjian H, O’Brien S, Cortes J et al (2006) Results of intensive chemotherapy in 998 patients age 65 years or older with acute myeloid leukemia or high-risk myelodysplastic syndrome: predictive prognostic models for outcome. Cancer 106:1090–1098
Lang K, Earle CC, Foster T et al (2005) Trends in the treatment of acute myeloid leukaemia in the elderly. Drugs Aging 22:943–955
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Acute Myeloid Leukemia Version 2.2014. Available from URL: http://www.nccn.org/professionals/physician_gls/PDF/aml.pdf. Accessed 30 Aug 2014
Williams JP, Handler HL (2000) Antibody-targeted chemotherapy for the treatment of relapsed acute myeloid leukemia. Am J Manag Care 6:S975–S985
Herr AL, Labopin M, Blaise D et al (2007) HLA-identical sibling allogeneic peripheral blood stem cell transplantation with reduced intensity conditioning compared to autologous peripheral blood stem cell transplantation for elderly patients with de novo acute myeloid leukemia. Leukemia 21:129–135
Storb R (2007) Can reduced-intensity allogeneic transplantation cure older adults with AML? Best Pract Res Clin Haematol 20:85–90
Juliusson G (2011) Older patients with acute myeloid leukemia benefit from intensive chemotherapy: an update from the Swedish Acute Leukemia Registry. Clin Lymphoma Myeloma Leuk 11(Suppl 1):S54–S59
Juliusson G, Antunovic P, Derolf A et al (2009) Age and acute myeloid leukemia: real world data on decision to treat and outcomes from the Swedish Acute Leukemia Registry. Blood 113:4179–4187
Murthy VH, Krumholz HM, Gross CP (2004) Participation in cancer clinical trials: race-, sex-, and age-based disparities. JAMA 291:2720–2726
Hutchins LF, Unger JM, Crowley JJ et al (1999) Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N Engl J Med 341:2061–2067
Gross CP, Murthy V, Li Y et al (2004) Cancer trial enrollment after state-mandated reimbursement. J Natl Cancer Inst 96:1063–1069
Mengis C, Aebi S, Tobler A et al (2003) Assessment of differences in patient populations selected for excluded from participation in clinical phase III acute myelogenous leukemia trials. J Clin Oncol 21:3933–3939
Warren JL, Klabunde CN, Schrag D et al (2002) Overview of the SEER-medicare data: content, research applications, and generalizability to the United States elderly population. Med Care 40:IV-3–IV-18
Potosky AL, Riley GF, Lubitz JD et al (1993) Potential for cancer related health services research using a linked Medicare-tumor registry database. Med Care 31:732–748
Vardiman JW, Thiele J, Arber DA et al (2009) The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood 114:937–951
Davidoff AJ, Tang M, Seal B et al (2010) Chemotherapy and survival benefit in elderly patients with advanced non-small-cell lung cancer. J Clin Oncol 28:2191–2197
Klabunde CN, Legler JM, Warren JL et al (2007) A refined comorbidity measurement algorithm for claims-based studies of breast, prostate, colorectal, and lung cancer patients. Ann Epidemiol 17:584–590
Charlson ME, Pompei P, Ales KL et al (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Warren JL, Harlan LC, Fahey A et al (2002) Utility of the SEER-medicare data to identify chemotherapy use. Med Care 40:IV-55-–IV-61
Suissa S (2008) Immortal time bias in pharmaco-epidemiology. Am J Epidemiol 167:492–499
Kurth T, Walker AM, Glynn RJ et al (2006) Results of multivariable logistic regression, propensity matching, propensity adjustment, and propensity-based weighting under conditions of nonuniform effect. Am J Epidemiol 163:262–270
Rosenbaum PR, Rubin DB (1983) The central rose of the propensity score in observational studies for causal effects. Biometrika 70:41–55
Lowenberg B, Zittoun R, Kerkhofs H et al (1989) On the value of intensive remission-induction chemotherapy in elderly patients of 65+ years with acute myeloid leukemia: a randomized phase III study of the European Organization for Research and Treatment of Cancer Leukemia Group. J Clin Oncol 7:1268–1274
Kantarjian HM, Thomas XG, Dmoszynska A et al (2012) Multicenter, randomized, open-label, phase III trial of decitabine versus patient choice, with physician advice, of either supportive care or low-dose cytarabine for the treatment of older patients with newly diagnosed acute myeloid leukemia. J Clin Oncol 30:2670–2677
Fenaux P, Mufti GJ, Hellstrom-Lindberg E et al (2010) Azacitidine prolongs overall survival compared with conventional care regimens in elderly patients with low bone marrow blast count acute myeloid leukemia. J Clin Oncol 28:562–569
Dombret H, Seymour JF, Butrym A et al (2014) Results of a Phase 3, Multicenter, Randomized, Open-Label Study of Azacitidine (AZA) vs Conventional Care Regimens (CCR). In: Older Patients with Newly Diagnosed Acute Myeloid Leukemia (AML). 19th Congress of the European Hematology Association Milan, Italy
Oran B, Weisdorf DJ (2012) Survival for older patients with acute myeloid leukemia: a population-based study. Haematologica 97:1916–1924
Estey E, de Lima M, Tibes R et al (2007) Prospective feasibility analysis of reduced-intensity conditioning (RIC) regimens for hematopoietic stem cell transplantation (HSCT) in elderly patients with acute myeloid leukemia (AML) and high-risk myelodysplastic syndrome (MDS). Blood 109:1395–1400
Wang M, Burau KD, Fang S et al (2008) Ethnic variations in diagnosis, treatment, socioeconomic status, and survival in a large population-based cohort of elderly patients with non-Hodgkin lymphoma. Cancer 113:3231–3241
Shavers VL, Brown ML (2002) Racial and ethnic disparities in the receipt of cancer treatment. J Natl Cancer Inst 94:334–357
Aizer AA, Chen MH, McCarthy EP et al (2013) Marital status and survival in patients with cancer. J Clin Oncol 31:3869–3876
Juliusson G, Billstrom R, Gruber A et al (2006) Attitude towards remission induction for elderly patients with acute myeloid leukemia influences survival. Leukemia 20:42–47
Buchner T, Hiddemann W, Berdel W et al (2002) Acute myeloid leukemia: treatment over 60. Rev Clin Exp Hematol 6:46–59, discussion 86-7
Nabhan C, Smith SM, Helenowski I et al (2012) Analysis of very elderly (>/=80 years) non-hodgkin lymphoma: impact of functional status and co-morbidities on outcome. Br J Haematol 156:196–204
Oxnard GR, Fidias P, Muzikansky A et al (2007) Non-small cell lung cancer in octogenarians: treatment practices and preferences. J Thorac Oncol 2:1029–1035
Dale DC (2003) Poor prognosis in elderly patients with cancer: the role of bias and undertreatment. J Support Oncol 1:11–17
Dohner H, Lubbert M, Fiedler W et al (2014) Randomized, phase 2 trial of low-dose cytarabine with or without volasertib in AML patients not suitable for induction therapy. Blood 124:1426–1433
Lancet JE, Cortes JE, Hogge DE et al (2014) Phase 2 trial of CPX-351, a fixed 5:1 molar ratio of cytarabine/daunorubicin, vs cytarabine/daunorubicin in older adults with untreated AML. Blood 123:3239–3246
Burnett AK, Russell NH, Hills RK et al (2012) Addition of gemtuzumab ozogamicin to induction chemotherapy improves survival in older patients with acute myeloid leukemia. J Clin Oncol 30:3924–3931
Castaigne S, Pautas C, Terre C et al (2012) Effect of gemtuzumab ozogamicin on survival of adult patients with de-novo acute myeloid leukaemia (ALFA-0701): a randomised, open-label, phase 3 study. Lancet 379:1508–1516
Acknowledgments
The authors would like to thank Dr. Michelle Byrtek for statistical consult and thoughtful review of the manuscript. This study used the linked SEER-Medicare database. We acknowledge the efforts of the Applied Research Program, NCI (Bethesda, MD), the Office of Information Services and the Office of Strategic Planning, Health Care Financing Administration (Baltimore, MD), Information Management Services, Inc. (Silver Spring, MD), and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-Medicare database. The interpretation and reporting of these data are the sole responsibility of the authors.
Conflict of interest
This study was funded by Genentech, Inc. through a contract with Q.D. Research, Inc. Dr. Medeiros received research funding from Roche-Genentech for clinical research activities and honorarium for advisory board participation. Dr. Reyes and Dr. Hurst are employees of Genentech and shareholders of Roche. Dr. Satram-Hoang, Dr. Hoang, and Mr. Momin work for Q.D. Research in a research and consulting capacity.
Author information
Authors and Affiliations
Corresponding author
Additional information
Bruno C. Medeiros and Sacha Satram-Hoang contributed equally to this work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Table S1
(DOCX 16 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article

Cite this article
Medeiros, B.C., Satram-Hoang, S., Hurst, D. et al. Big data analysis of treatment patterns and outcomes among elderly acute myeloid leukemia patients in the United States. Ann Hematol 94, 1127–1138 (2015). https://doi.org/10.1007/s00277-015-2351-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-015-2351-x