
Abstract
Background
Impingement syndrome, a common cause of shoulder pain, often leads to functional limitations. Manual thoracic therapy is frequently employed as a non-surgical intervention, but its efficacy remains debated. This review assesses the impact of manual thoracic therapy on pain reduction and functional improvement in impingement syndrome.
Methods
A systematic review of randomized clinical trials was conducted, focusing on studies that applied manual thoracic therapy to patients with impingement syndrome. The primary outcomes were pain reduction and functional improvement. Studies were evaluated for methodological quality using the PEDro scale, with scores ≥ 6 indicating high quality.
Results
Nine studies met the inclusion criteria. All studies demonstrated high methodological quality (PEDro score ≥ 6). Pain reduction was consistent across studies, with an NPRS score reduction of 0.6 to 1.5 points immediately after treatment and up to 3.2 points at follow-up. Functionality improvements were statistically significant in some studies. However, the results showed limited homogeneity, and the majority of studies did not report substantial differences between intervention and placebo groups.
Conclusion
This review suggests that manual thoracic therapy may lead to pain reduction in impingement syndrome, with some evidence of functional improvement. However, the variability in manual therapy techniques and the limitations in research methodologies indicate a need for further controlled studies. These findings underscore the potential of manual therapy as a supplementary treatment but also highlight the necessity for more robust clinical trials to fully ascertain its effectiveness in clinical practice.
Graphic abstract

Zusammenfassung
Hintergrund
Ein Impingement-Syndrom, eine weit verbreitete Ursache für Schulterschmerzen, führt oft zu funktionellen Einschränkungen. Häufig wird die manuelle thorakale Therapie als nichtchirurgische Intervention eingesetzt, aber ihre Wirksamkeit ist weiterhin umstritten. In der vorliegenden Übersicht werden die Auswirkungen manueller thorakaler Therapie auf die Schmerzreduktion und funktionelle Verbesserung beim Impingement-Syndrom untersucht.
Methoden
Dazu wurde eine systematische Übersicht über randomisierte klinische Studien erstellt, hierbei lag der Fokus auf Studien, in denen manuelle thorakale Therapie bei Patienten mit Impingement-Syndrom angewendet wurde. Die primären Endpunkte waren Schmerzreduktion und funktionelle Verbesserung. Mithilfe der Skala der Physiotherapy Evidence Database (PEDro-Skala) wurden die Studien in Bezug auf methodische Qualität untersucht, wobei Werte ≥ 6 eine hohe Qualität anzeigen.
Ergebnisse
Die Einschlusskriterien wurden von 9 Studien erfüllt. Alle Studien wiesen eine hohe methodische Qualität auf (PEDro-Score ≥ 6). Über alle Studien hinweg war die Schmerzreduktion konsistent – mit einer Reduktion des Werts auf der Numeric Pain Rating Scale (NPRS) von 0,6 auf 1,5 Punkte unmittelbar nach Behandlung und von bis zu 3,2 Punkten bei der Nachuntersuchung. Die funktionelle Verbesserung war in einigen Studien statistisch signifikant. Jedoch wiesen die Ergebnisse nur eine begrenzte Homogenität auf, und in der Mehrzahl der Studien wurden keine wesentlichen Unterschiede zwischen den Interventions- und den Placebogruppen beschrieben.
Schlussfolgerung
Den Ergebnissen der vorliegenden Übersicht zufolge kann manuelle thorakale Therapie zu einer Schmerzreduktion bei einem Impingement-Syndrom führen, auch bestehen einige Hinweise auf eine funktionelle Verbesserung. Allerdings zeigen die Variabilität bei den Techniken der manuellen Therapie und die Limitationen bei der wissenschaftlichen Methodik, dass Bedarf an weiteren kontrollierten Studien besteht. Diese Ergebnisse unterstreichen das Potenzial der manuellen Therapie als einer ergänzenden Behandlung, aber auch die Notwendigkeit robusterer klinischer Studien, um ihre Wirksamkeit in der klinischen Anwendung vollständig zu ermitteln.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Shoulder impingement syndrome is emerging as a complex and multidimensional pathology, involving a variety of etiological and biomechanical factors [2, 13]. Characterized by compression of subacromial structures, the syndrome leads to a clinical picture of pain, weakness, and paresthesia in the upper limb. Originally described by Adam in 1852 [34], the pathology was widely disseminated and characterized by the work of Charles Neer in 1972 [17], highlighting the reduction of subacromial space as a key element in the pathogenesis of the syndrome [13]. The classification of subacromial conflict syndrome, developed by Neer in 1983 [18], divides the condition into three stages based on the patient’s age, clinical signs, and the evolution of the pathology. These stages range from edema and inflammation, typical in individuals under 25 years, to fibrosis and tendinitis in patients aged 25 to 40 years, up to the development of bone spurs and tendon ruptures in individuals over 40 years. It is important to note that impingement syndrome can be further classified based on the nature of the conflict, distinguishing between primary conflict, secondary conflict, and internal impingement [14, 37]. These subclassifications are based on differences in etiology and clinical presentation, such as the abnormal relationship between the rotator cuff and the coracoacromial arch in primary conflict, glenohumeral or scapulothoracic instability in secondary conflict, and contact between the greater tuberosity and the posterior–superior face of the glenoid in internal impingement [12, 33]. In addition, a significant link has been identified between impingement syndrome and various biomechanical factors such as alterations in scapular kinematics, abnormal muscle activation, and incorrect posture [1, 4, 19, 21, 23, 25, 26]. Recent studies have emphasized how increased thoracic kyphosis can contribute to the pathology, altering scapular mechanics and reducing the subacromial space [33]. This systematic review focuses on exploring the efficacy of manual therapy techniques, particularly those applied to the thoracic district, in patients with subacromial conflict syndrome [27, 29, 32]. The objective is to assess how these interventions influence pain, functionality, scapular kinematics, and muscle strength compared to other therapeutic methods or the absence of treatment [27, 28, 31]. Considering the importance of regional interdependence and the influence of scapular kinematics in the syndrome, this review offers a critical and updated evaluation of therapeutic options, with a particular focus on the short- and long-term outcomes of different therapeutic approaches [5,6,7,8,9,10,11, 22, 24, 30, 35].
Materials and methods
This systematic review was carried out following the methodological guidance contained in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist [20]. The protocol was published in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42023491212.
Research method
Search strategy
An electronic bibliographic search was conducted in three databases: PubMed, Cochrane Central Register of Controlled Trials, PEDro database. The P.I.C.O.(M.) strategy was used to formulate the research question of the review. The search was conducted up to January 20, 2024, with no date restriction and no linguistic limits. The search terms used were as follows:
((shoulder pain [MeSH terms]) OR (shoulder impingement) OR (rotator cuff related shoulder pain) OR (shoulder impingement syndrome [MeSH terms])) AND ((thoracic) OR (spine)) AND ((manipulation) OR (manual therapy) OR (joint mobilization) OR (musculoskeletal manipulations [MeSH terms])). PubMed
((shoulder pain) OR (shoulder impingement) OR (rotator cuff related shoulder pain) OR (shoulder impingement syndrome)) AND ((thoracic) OR (spine)) AND ((manipulation) OR (manual therapy) OR (joint mobilization) OR (musculoskeletal manipulations)). Cochrane Central
(shoulder pain, shoulder impingement, thoracic, spine, manual therapy, mobilization, joint mobilization, manipulation). PEDro
Study selection criteria
Inclusion criteria
Inclusion criteria population: adult subjects > 18 years old, both males and females, with a diagnosis of impingement syndrome after recognized clinical tests. Specific shoulder pathologies (adhesive capsulitis, surgical operations, dislocations).
Intervention: mandatory: any manual therapy technique applied to the thoracic district. Optional: manual therapy to the shoulder, cervical spine, massage therapy, or therapeutic exercise. Exclusively manual therapy to the shoulder, cervical spine, and use of instrumental physical therapies.
Outcomes: pain, shoulder functionality, scapular kinematics, muscle activity.
Studies: randomized clinical trials (RCTs).
Exclusion criteria
Observational studies, secondary studies, pilot studies.
Study selection process
The records retrieved from database searching were collected and imported into EndNote V.X9 (Clarivate Analytics, Philadelphia, PA, USA). Duplicates were removed through the Endnote deduplicator tool. In the screening phase, two reviewers independently read all titles and abstracts, excluding articles that did not answer the research question. A third reviewer intervened to reach a final decision on the list of articles to be read in full text. The study selection process and the reasons for exclusion were recorded and presented in the PRISMA flow diagram.
Data extraction and assessment
The methodological quality of the intervention studies included in the review was assessed by the researchers using the PEDro scale tool [3, 15]. The results of the assessment were entered in a table, the fulfilment of the criterion was indicated with “yes,” and the absence of the specific item in the analyzed study with “no.” Two independent reviewers, both of whom were experts in the field, were involved in the quality assessment. In cases of disagreement, a third reviewer with extensive research and practice experience was called upon to intervene. Training was provided by a third physiotherapist experienced in research methodology. Summary tables and graphs of the extracted data from all included studies and a narrative summary were provided.
Data analysis
The reviewers independently extracted data from the studies and summarized them in a summary table. The following data were extracted: author, year, participants, treatment description, and outcome.
For the final analysis, we considered the “NA” items as items not reported and described by the authors.
Results
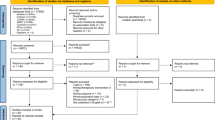
From the initial search, 140 articles were retrieved. Specifically, 28 articles were found in PubMed, 72 in PEDro, and 40 in Cochrane. Of these articles, 76 were removed as duplicates, resulting in a total of 64 articles. With the first reading of titles and abstracts, 37 studies were removed. After the full reading of the remaining studies, 18 studies were eliminated for not meeting the inclusion criteria. Thus, 9 articles were included in the review (Table 1). The entire study selection process is outlined in the PRISMA statement flow diagram (Fig. 1), which details the excluded studies and the reasons for their exclusion.

Flow diagram. (Adapted from Page et al. [38], PRISMA [39]; CC BY 4.0, https://creativecommons.org/licenses/by/4.0/deed.de)
Haik et al. (2014) [7].
Both the thoracic spinal manipulation (TSM) impingement group and the sham TSM impingement group reported statistically significant average reductions (0.6 points) in post-intervention pain, regardless of the treatment received (p = 0.04). 60% of the TSM group reported pain improvement compared to 36% in the placebo therapy. The TSM impingement group showed an increase in scapular lateral rotation of 1.7° (p < 0.001) during arm elevation and 1.1° during lowering (p = 0.019) after the intervention. The asymptomatic TSM group demonstrated a 2.2° (p < 0.001) increase in scapular lateral rotation in arm elevation post-intervention, where the placebo group improved by only 1° (p = 0.05). The asymptomatic TSM group also reported a 1.9° (p < 0.001) increase in lateral scapular rotation and a 0.9° (p = 0.002) change in scapular tilt during elevation and 1.1° (p = 0.002) during lowering post-intervention. No dropouts were reported.
Kardouni et al. (2014) [10].
Following manipulation, both pain (numeric pain rating scale [NPRS] score) and functionality (Penn Shoulder Score) improved in both groups over time (p < 0.001). The NPRS score decreased by 1.1 points from pre-treatment to post-treatment and by 1.5 points from pre-treatment to follow-up. The Penn Shoulder Score improved by 10.1 points from pre-intervention to follow-up. No differences were observed in the global rating of change (GROC) scale between the two groups. A correlation was found between the pressure pain threshold (PPT) in the lower trapezius of the unaffected shoulder and the pre-treatment Penn Score in the SMT group (p = 0.009).
Kardouni et al. (2015) [9].
No differences were observed between groups in thoracic excursion, pain (NPRS), or functionality (Penn Shoulder Score). The average NPRS scores decreased by 1 point from pre-treatment to post-treatment, and by 1.2 points from pre-treatment to follow-up (24–48 h later). The Penn Shoulder Score improved by 9.1 points from pre-treatment to follow-up. Both groups showed a mean change in scapular internal rotation of 0.9° (p = 0.003) during elevation and 0.8° (p = 0.041) during lowering post-intervention. No significant differences in thoracic excursion were noted in either group post-treatment.
Riley et al. (2015) [22].
Immediately post-intervention, no statistically significant differences were observed regarding functionality (shoulder pain and disability index [SPADI]) and pain (NPRS), irrespective of the message or intervention. A difference of 0.9 points in NPRS was noted between pre-treatment and follow-up (p < 0.001), but no differences were found immediately post-treatment. For the SPADI scale, an eight-point difference was noted between pre-treatment and follow-up (p < 0.001).
Haik et al. (2016) [6].
No significant differences in pain (NPRS) were observed between the two groups. The TSM group showed a 0.8-point difference on day 2 pre-intervention and 0.9 points on day 2 post-intervention. No significant differences were noted between the two groups for the functionality scales disabilities of the arm, shoulder, and hand (DASH) and Western Ontario rotator cuff index (WORC; p > 0.5). Data collected on scapular kinematics revealed a mean difference in both groups during arm elevation, of 2.6° (p < 0.01) in lateral scapular rotation on day 2 pre-intervention and 4.1° (p < 0.01) post-intervention. The sham TSM group showed improvement (p = 0.04) compared to the TSM group in anterior scapular tilt during arm elevation. During arm lowering, the TSM group demonstrated improved lateral rotation (p = 0.01) on day 2 pre-intervention, post-intervention, and at follow-up. Regarding muscle activity, differences in the upper trapezius were observed, with greater activity in the sham TSM group on day 2 post-intervention (p < 0.01) and at follow-up (p < 0.01). Both groups showed decreased activity in the lower trapezius (p < 0.1) on day 2 pre-intervention, with the sham group showing this decrease post-intervention and the TSM group at follow-up. Increased activity in the upper trapezius was noted in the sham TSM group at follow-up (p < 0.01), and a decrease in the lower trapezius in the sham TSM group on day 2 pre-intervention, post-intervention, and at follow-up in the TSM group (p < 0.01).
Da Silva et al. (2019) [24].
Following the intervention, a significant increase in range of motion (ROM) in flexion (p < 0.01) and abduction (p < 0.01) of the painful shoulder was observed in the manipulation group (MG), and also in abduction of the non-painful shoulder (p = 0.03). The placebo group demonstrated a significant increase in ROM in flexion of the affected shoulder (p = 0.03) and in abduction (p < 0.01). No particular differences in pain were observed between groups, with a time-effect reduction in pain in both groups (−0.53 cm MG; −0.37 cm PG).
Land et al. (2019) [11].
All three groups experienced a significant decrease in pain from the initial assessment to the 12th week (p = 0.04). The upper thoracic intervention group showed improvement from baseline to the 6th week in the SPADI scale (p = 0.007), passive internal rotation (p < 0.001), and posterior shoulder range (p = 0.004). The posterior shoulder intervention group showed improvement from baseline to the 6th week in the SPADI scale (p = 0.03), passive internal rotation (p = 0.005), and posterior shoulder range (p = 0.01). The upper thoracic intervention group maintained improvements until the 12th week regarding the SPADI scale (p = 0.006) and passive internal rotation (p = 0.02). The posterior shoulder intervention group maintained only passive internal rotation (p = 0.04). A significant improvement in the SPADI scale was maintained until the 6‑month follow-up after treatment in both the upper thoracic (p = 0.05) and posterior shoulder intervention groups (p = 0.02).
Grimes et al. (2019) [5].
Following manipulation, no significant differences were observed in pain, functionality, or satisfaction (p > 0.05). No differences in scapular kinematics, pectoralis minor length, or isometric force of the middle trapezius, lower trapezius, or serratus anterior (p > 0.05) were observed between the two groups.
Hunter et al. (2022) [22].
The MET-only group showed significant improvements in pain and disability (DASH, SPADI, VAS) compared to the placebo group at discharge (DASH: −8.4, p = 0.003; SPADI: −14.7, p = 0.0; VAS: −15.5, p = 0.001), at 6 months (DASH: −11.1, p = 0.04; SPADI: −14.9, p = 0.010; VAS: −14.1, p = 0.02), and at 12 months (DASH: −13.4, p = 0.013; SPADI: −19, p = 0.005; VAS: −17.3, p = 0.01). The MET + STM group showed improvements in disability but not in pain at discharge (DASH: −8.2, p = 0.006; SPADI: −13.5, p = 0.02) and at 6 months (DASH: −9.0, p = 0.024; SPADI: −12.4, p = 0.041). Regarding the patient-specific functional scale (PSFS), the MET-only group improved compared to placebo at discharge (1.3, p = 0.03) and at 12 months (1.8, p = 0.008), while the MET + STM group improved at 12 months (1.7, p = 0.02). No differences were observed between the MET-only and MET + STM groups in terms of thoracic flexion–extension ROM or thoracic posture.
Risk of bias
The methodological quality with which the studies were conducted and the risk of bias to which they are subjected were assessed by means of the PEDro scale, as shown in Table 2. “Yes” was indicated as fulfilment of the criterion and “no” as the absence of the specific item in the study analyzed.
Pedro scale: 1 eligibility criteria were specified; 2 subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received); 3 allocation was concealed; 4 the groups were similar at baseline regarding the most important prognostic indicators; 5 there was blinding of all subjects; 6 there was blinding of all therapists who administered the therapy; 7 there was blinding of all assessors who measured at least one key outcome; 8 measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups; 9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analyzed by “intention to treat;” 10 the results of between-group statistical comparisons are reported for at least one key outcome; 11 the study provides both point measures and measures of variability for at least one key outcome.
The first item was included for completeness with respect to the Delphi list [36], but is not included in the final count, which is based on ten, from requirement number 2 to number 11. If the criterion is fulfilled, one point is awarded, otherwise it has a value of zero. The authors of the PEDro scale divide clinical studies into four categories, linked to the score obtained: low quality when it varies between 0 and 3; medium quality if it is 4 or 5; high quality if it is 6 to 8; excellent quality with a score of 9 or 10.
Discussion
The objective of this review was to evaluate whether manual therapy techniques applied to the thoracic district can provide benefits in terms of pain or functionality in patients with impingement syndrome. This review also included studies where, in addition to thoracic manual therapy, therapeutic exercise was performed or part of the treatment was directly dedicated to the shoulder, as this is the standard approach for patients with subacromial conflict syndrome. In the majority of the studies [7, 9,10,11, 22, 24], only manipulative techniques at the thoracic level were applied. Riley’s study [22] associated a “row” type reinforcement exercise, Land’s study [11] a supine postural exercise, and Hunter’s study [8] performed a muscle energy technique (MET). Six studies [5,6,7, 9, 10, 24] used a sham manipulation as a control group, described in the study by Michener et al. [16] as a valid comparative tool. The four outcomes investigated by this review are pain, functionality, scapular kinematics, and muscle activation. Regarding pain, all authors agree that following treatment, the intervention groups do not show substantial differences compared to placebo groups. However, in all studies, there was a reduction in pain (NPRS) between 0.6 and 1.5 points in the immediate post-treatment period, with a maximum of 3.2 in the follow-up. Specifically, Haik’s study [7] reported a difference of 0.6 points NPRS post-intervention, Kardouni’s study [10] 1.1 points NPRS post-treatment, and 1.5 at the 24/48 h follow-up. Kardouni’s second study [9] had a 1-point NPRS difference post-treatment and 1.2 at the 24/48 h follow-up. Riley’s study [22] found an average difference of 0.9 points NPRS between pre-treatment and 6/9 days follow-up. Haik’s second study [6] found a difference of 0.8 points on the second day of intervention and 0.9 immediately after the second intervention. Land’s study [11] found a 3.6-point NPRS reduction after 12 weeks of treatment. Da Silva’s study [24], which used the VAS scale, achieved a 0.53-cm reduction. Finally, Hunter’s study [8] demonstrated a VAS pain reduction of 1.5 cm at discharge, 1.4 at the 6‑month follow-up, and 1.7 at the 12-month follow-up. For some authors, the average reduction in scores describing pain is attributed to the factor of time; this would explain the similarity with the scores of various placebo groups. Authors who conducted trials with analysis of outcomes immediately after treatment believe that the reduction in pain is caused by the placebo effect, patient positioning, interaction with a healthcare professional, or mobilization within the range of motion. For the outcome of functionality, as with pain, the majority of studies agree that intervention groups and placebo groups do not show differences. However, in some studies there have been statistically significant changes in assessment scale scores post-treatment or during follow-up. Specifically, Kardouni’s studies [9, 10] show a decreased Penn Shoulder Scale score by 10.1 and 9.1 points, respectively, in the 24/48 h follow-up. Riley’s study [22] achieved an 8‑point improvement in the SPADI scale between pre-treatment and 6/9 days follow-up. Land’s study [11] found a 32-point improvement in the SPADI scale in the thoracic intervention group at 12 weeks, and the results were maintained up to the 12-month follow-up. Hunter’s study [8] found an improvement in the DASH and SPADI scales both at discharge with 8.4 and 14.7 points of difference, at the 6‑month follow-up with 11.1 and 14.9 points of difference, and at 12 months with 13.4 and 19 points of difference compared to the placebo group, respectively. Regarding the outcome of scapular kinematics, there was heterogeneity in results, as some studies had significant changes, while others found no differences. Haik’s study [7] reported improvements following manual therapy in both symptomatic and asymptomatic groups, with the symptomatic group showing an increase of 1.7° in lateral scapular rotation during elevation and 1.1° during lowering. The asymptomatic group showed an increase of 2.2° in lateral scapular rotation during elevation and 1.9° during lowering. The asymptomatic group also showed an increase of 0.9° in scapular tilt during elevation and 1.1° during lowering. Kardouni’s study [9] reported scapular improvements in medial rotation of 0.9° in both groups during elevation and 0.8° during lowering. Haik’s second study [6] found an increase in lateral scapular rotation of 2.6° during elevation, improving to 4.6° after the second treatment. This improvement in lateral rotation was also observed during lowering by 4°, improving to 5.3° after the second intervention. Da Silva’s study [24] measured shoulder range of motion globally, indicating significant improvements in flexion and abduction movements by 3.5° and 8.0°, respectively, as well as improved abduction by 2.0° in the non-painful shoulder. Land’s study [11] reported an improvement in passive internal shoulder rotation of 17.0° at 6 weeks and 19.8° at 12 weeks. The last outcome, muscle activity, was measured in Haik’s study [6], where increased activity of the upper trapezius and decreased activity of the lower trapezius were observed following manipulative therapy, in both flexion and lowering arm movements. Grimes’s study [5] found no differences in isometric strength of the trapezius or serratus anterior muscles or in the length of the pectoralis minor muscle after performing manipulations. Some results obtained from various studies are described by the authors as “statistically significant but not clinically important,” as minimal variations in pain and functionality scales or a few degrees in scapular range of motion can be important statistically but hardly translate into real changes in clinical practice. This review aims to verify the efficacy of thoracic manual therapy not to completely replace the standard treatment but more to integrate it within it and understand whether applying these techniques can speed up the healing process and pain reduction in patients.
Strengths and limitations
This systematic review of randomized clinical trials on manual thoracic therapy for impingement syndrome is characterized by high methodological quality, as all included studies scored ≥ 6 on the PEDro scale, indicating a low risk of bias. The review examined diverse outcomes, including pain, functionality, scapular kinematics, and muscle activation. A consistent reduction in pain (NPRS score between 0.6 and 1.5 points immediately post-treatment and up to 3.2 points in follow-ups) was observed across studies, despite no substantial differences between intervention and placebo groups. Statistically significant improvements in functionality scores were noted in some studies during post-treatment and follow-up periods. Several studies reported improvements in scapular kinematics, such as increases in lateral rotation and tilt of the scapula, and changes in muscle activity, particularly in the trapezius muscles, in response to manual therapy. The evidence was synthesized narratively, not quantitatively, limiting the ability to comprehensively measure the effect size. The variability in manual therapy techniques, due to differing levels of training and execution capabilities of therapists, could impact treatment effectiveness. The inability to apply treatments blindly and the experience of the practitioner pose challenges in objectifying research in this field. The reliance on self-administered questionnaires or self-evaluations for assessing outcomes introduces subjectivity into the results. The review highlighted limited homogeneity in the results, questioning the therapeutic approach to impingement syndrome through thoracic manual therapy. The review aims not to replace but to supplement standard treatment, by assessing whether thoracic manual therapy can accelerate the healing process and pain reduction in patients. Future studies with more treatments and controlled randomized designs are suggested to verify the efficacy in a setting more similar to real clinical practice.
Clinical practice
This review on manual thoracic therapy for impingement syndrome shows high methodological quality and a consistent reduction in pain across studies. However, it faces limitations like variability in treatment application and reliance on self-evaluations for outcomes. These findings suggest potential benefits of manual therapy in clinical practice but highlight the need for further research with more controlled designs to confirm efficacy.
Conclusion
This review indicates that manual thoracic therapy may reduce pain in impingement syndrome, but due to methodological limitations and variability in treatment application, further research is needed to confirm its efficacy in clinical practice.
References
Boccolari P, Pantaleoni F, Donati D, Tedeschi R (2024) Non-surgical treatment of oblique diaphyseal fractures of the fourth and fifth metacarpals in a professional athlete: a case report. Int J Surg Case Rep 115:109256. https://doi.org/10.1016/j.ijscr.2024.109256
Braman JP, Zhao KD, Lawrence RL et al (2014) Shoulder impingement revisited: evolution of diagnostic understanding in orthopedic surgery and physical therapy. Med Biol Eng Comput 52:211–219. https://doi.org/10.1007/s11517-013-1074-1
Cashin AG, McAuley JH (2020) Clinimetrics: physiotherapy evidence database (PEDro) scale. J Physiother 66:59. https://doi.org/10.1016/j.jphys.2019.08.005
Catellani I, Arcuri P, Vita F et al (2024) An overview of rehabilitation approaches for focal hand dystonia in musicians: a scoping review. Clin Rehabil. https://doi.org/10.1177/02692155231225705
Grimes JK, Puentedura EJ, Cheng MS, Seitz AL (2019) The comparative effects of upper thoracic spine thrust manipulation techniques in individuals with subacromial pain syndrome: a randomized clinical trial. J Orthop Sports Phys Ther 49:716–724. https://doi.org/10.2519/jospt.2019.8484
Haik MN, Alburquerque-Sendín F, Camargo PR (2017) Short-term effects of thoracic spine manipulation on shoulder impingement syndrome: a randomized controlled trial. Arch Phys Med Rehabil 98:1594–1605. https://doi.org/10.1016/j.apmr.2017.02.003
Haik MN, Alburquerque-Sendín F, Silva CZ et al (2014) Scapular kinematics pre- and post-thoracic thrust manipulation in individuals with and without shoulder impingement symptoms: a randomized controlled study. J Orthop Sports Phys Ther 44:475–487. https://doi.org/10.2519/jospt.2014.4760
Hunter I, Bradshaw C, McLeod A et al (2022) Energetics and biomechanics of uphill, downhill and level running in highly-cushioned carbon fiber Midsole plated shoes. J Sports Sci Med 21:127–130. https://doi.org/10.52082/jssm.2022.127
Kardouni JR, Pidcoe PE, Shaffer SW et al (2015) Thoracic spine manipulation in individuals with subacromial impingement syndrome does not immediately alter thoracic spine kinematics, thoracic excursion, or scapular kinematics: a randomized controlled trial. J Orthop Sports Phys Ther 45:527–538. https://doi.org/10.2519/jospt.2015.5647
Kardouni JR, Shaffer SW, Pidcoe PE et al (2015) Immediate changes in pressure pain sensitivity after thoracic spinal manipulative therapy in patients with subacromial impingement syndrome: a randomized controlled study. Man Ther 20:540–546. https://doi.org/10.1016/j.math.2014.12.003
Land H, Gordon S, Watt K (2019) Effect of manual physiotherapy in homogeneous individuals with subacromial shoulder impingement: a randomized controlled trial. Physiother Res Int 24:e1768. https://doi.org/10.1002/pri.1768
Lanfranchi E, Fairplay T, Tedeschi R (2023) A case report: pain in the hand and tingling of the upper limb may be a symptom of a schwannoma in the supraclavicular region. Int J Surg Case Rep 110:108664. https://doi.org/10.1016/j.ijscr.2023.108664
Ludewig PM, Cook TM (2002) Translations of the humerus in persons with shoulder impingement symptoms. J Orthop Sports Phys Ther 32:248–259. https://doi.org/10.2519/jospt.2002.32.6.248
Luime JJ, Koes BW, Hendriksen IJM et al (2004) Prevalence and incidence of shoulder pain in the general population; a systematic review. Scand J Rheumatol 33:73–81. https://doi.org/10.1080/03009740310004667
Maher CG, Sherrington C, Herbert RD et al (2003) Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther 83:713–721
Michener LA, Kardouni JR, Lopes Albers AD, Ely JM (2013) Development of a sham comparator for thoracic spinal manipulative therapy for use with shoulder disorders. Man Ther 18:60–64. https://doi.org/10.1016/j.math.2012.07.003
Neer CS (1972) Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am 54:41–50
Neer CS (1983) Impingement lesions. Clin Orthop Relat Res: 70–77
Otoshi K, Takegami M, Sekiguchi M et al (2014) Association between kyphosis and subacromial impingement syndrome: LOHAS study. J Shoulder Elbow Surg 23:e300–e307. https://doi.org/10.1016/j.jse.2014.04.010
Page MJ, Moher D, Bossuyt PM et al (2021) PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ 372:n160. https://doi.org/10.1136/bmj.n160
Phadke V, Camargo P, Ludewig P (2009) Scapular and rotator cuff muscle activity during arm elevation: a review of normal function and alterations with shoulder impingement. Rev bras fisioter 13:1–9. https://doi.org/10.1590/S1413-35552009005000012
Riley SP, Cote MP, Leger RR et al (2015) Short-term effects of thoracic spinal manipulations and message conveyed by clinicians to patients with musculoskeletal shoulder symptoms: a randomized clinical trial. J Man Manip Ther 23:3–11. https://doi.org/10.1179/2042618613Y.0000000066
Santandrea S, Benassi M, Tedeschi R (2023) Comparison of short-stretch bandage and long-stretch bandage for post-traumatic hand edema. Int J Surg Case Rep 111:108854. https://doi.org/10.1016/j.ijscr.2023.108854
da Silva AC, Santos GM, de Marques CMG, Marques JLB (2019) J Chiropr Med 18:19–26. https://doi.org/10.1016/j.jcm.2018.10.001 (Not Available)
Tedeschi R (2023) Case report: integrating aerobic activity in post-surgical management of plurifragmentary distal clavicle fractures—a holistic approach to pain modulation and recovery. Int J Surg Case Rep 113:109024. https://doi.org/10.1016/j.ijscr.2023.109024
Tedeschi R (2023) Unveiling the potential of trigger point therapy: exploring its efficacy in managing muscular spasticity—a scoping review. MLTJ 13:564–573. https://doi.org/10.32098/mltj.04.2023.07
Tedeschi R (2023) Briser le cycle nocebo : stratégies pour améliorer les résultats en podiatrie. Douleurs : Évaluation – Diagnostic – Traitement 24:241–247. https://doi.org/10.1016/j.douler.2023.10.006
Tedeschi R (2023) Assessment of postural control and proprioception using the delos postural proprioceptive system. Reabilitacijos Mokslai: Slauga Kineziterapija Ergoterapija 2:96–112. https://doi.org/10.33607/rmske.v2i29.1428
Tedeschi R (2024) An overview and critical analysis of the graston technique for foot-related conditions: a scoping review. Manuelle Medizin. https://doi.org/10.1007/s00337-023-01018-w
Tedeschi R (2023) Can beneficial frequencies in physiotherapy help treatment? Scoping Review, Rwanda Medical Journal 80:88–94. https://doi.org/10.4314/rmj.v80i2.8
Tedeschi R, Berti L, Platano D (2023) Transcranial direct current stimulation (tDCS) in managing pain and recovery: a clinical case of radial capitellum fracture. Int J Surg Case Rep 114:109120. https://doi.org/10.1016/j.ijscr.2023.109120
Tedeschi R, Giorgi F (2023) What is known about the regentK regenerative treatment for ruptured anterior cruciate ligament? A scoping review. Manuelle Medizin 61:181–187. https://doi.org/10.1007/s00337-023-00953-y
Timmons MK, Thigpen CA, Seitz AL et al (2012) Scapular kinematics and subacromial-impingement syndrome: a meta-analysis. J Sport Rehabil 21:354–370. https://doi.org/10.1123/jsr.21.4.354
Todd RB (1842) The cyclopædia of anatomy and physiology. Prov Med J Retrosp Med Sci 5:197. https://doi.org/10.1136/bmj.s1-5.114.197
Turolla A, Guccione AA, Tedeschi R, Pillastrini P (2023) Is clinical research as helpful to clinicians as it could be? Phys Ther. https://doi.org/10.1093/ptj/pzad060
Verhagen AP, de Vet HC, de Bie RA et al (1998) The delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by delphi consensus. J Clin Epidemiol 51:1235–1241. https://doi.org/10.1016/s0895-4356(98)00131-0
van der Windt DA, Koes BW, de Jong BA, Bouter LM (1995) Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 54:959–964. https://doi.org/10.1136/ard.54.12.959
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Funding
Open access funding provided by Alma Mater Studiorum - Università di Bologna within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
R. Tedeschi, D. Platano, G. Melotto and D. Danilo declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies mentioned were in accordance with the ethical standards indicated in each case.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Protocol registration
PROSPERO (CRD42023491212)

Scan QR code & read article online
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tedeschi, R., Platano, D., Melotto, G. et al. Effectiveness of manual thoracic therapy in treating impingement syndrome: a systematic review. Manuelle Medizin 62, 178–186 (2024). https://doi.org/10.1007/s00337-024-01040-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00337-024-01040-6
Keywords
- Impingement syndrome
- Manual thoracic therapy
- Pain reduction
- Shoulder dysfunction
- Musculoskeletal rehabilitation