
Abstract
Little is known regarding a correlation of hemodynamics at rest or exercise capacity with echocardiographic parameters in patients with pulmonary hypertension (PH). To clarify these potential correlations, we performed transthoracic echocardiography, right heart catheterization, and cardiopulmonary exercise testing in 53 patients with pulmonary arterial hypertension (PAH) and chronic thromboembolic pulmonary hypertension (CTEPH). Left ventricular end-diastolic dimension (LVDd), early diastolic velocity of the septal mitral annulus (septal e′), tricuspid regurgitation peak gradient (TRPG), and tricuspid annular plane systolic excursion (TAPSE) were significantly correlated with cardiac index (LVDd; r = 0.477, P < 0.001, septal e′; r = 0.463, P = 0.001, TRPG; r = − 0.455, P = 0.001 and TAPSE; r = 0.406, P = 0.003, respectively). Multiple regression analysis revealed that LVDd and septal e′ were significantly associated with cardiac index (CI) and stroke volume index at rest. Among the exercise capacity markers evaluated, TAPSE, TRPG, and LVDd were significantly correlated with peak oxygen uptake (TAPSE; r = 0.534, P < 0.001, TRPG; r = − 0.466, P = 0.001 and LVDd; r = 0.411, P = 0.002, respectively). Multiple regression analysis showed that TAPSE was significantly associated with peak oxygen uptake (VO2). In PAH and CTEPH patients, LVDd and septal e′ were significantly associated with CI at rest, whereas TAPSE was significantly associated with peak VO2. Echocardiographic parameters may predict the prognostic factors of PAH and CTEPH patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Several specific therapies have been introduced for the treatment of pulmonary arterial hypertension (PAH) and chronic thromboembolic pulmonary hypertension (CTEPH), and patient conditions have been assessed repeatedly in detail. [1,2,3,4,5,6] Noninvasive techniques such as echocardiography and MRI are used for assessing the severity of PAH or CTEPH [7,8,9,10,11,12,13,14]. Echocardiography is a particularly convenient method in routine medical care, and measures several parameters helpful for evaluating cardiac function [15, 16]. In particular, in the assessment of right cardiac function, the tricuspid regurgitation peak gradient (TRPG) is useful for estimating the pulmonary artery pressure (PAP), whereas tricuspid annular plane systolic excursion (TAPSE), a well-known prognostic factor of PAH, is a measure of the systolic function of the right ventricle (RV) [17,18,19]. In addition, echocardiography and MRI have proven to be valuable tools in estimating right-to-left ventricular interaction and diastolic dysfunction of the left ventricle (LV) associated with deleterious increases in RV pressure [20,21,22].
Cardiac index (CI), which is obtained during right heart catheterization, and peak oxygen uptake (VO2), which is assessed through cardiopulmonary exercise testing (CPET), are established prognostic factors of PAH [23]. However, details of the correlation between these invasively acquired prognostic factors and noninvasive echocardiographic parameters are still not enough in patients with PAH and CTEPH. Accordingly, we investigated the potential relationship among hemodynamics at rest, exercise capacity, and the echocardiographic parameters routinely measured at rest in patients with PAH and CTEPH.
Materials and methods
Patients and study design
We retrospectively enrolled 53 consecutive patients with PAH and CTEPH who were referred to our institution for the first time between April 1, 2012 and May 31, 2016 (Fig. 1). All patients underwent transthoracic echocardiography, right heart catheterization, and CPET. Patients were diagnosed as having pulmonary hypertension (PH) when right heart catheterization demonstrated a mean PAP of ≥ 25 mmHg and a pulmonary arterial wedge pressure (PAWP) of ≤ 15 mmHg. Patients with obstructive or restrictive lung disease, left heart disease, or congenital heart disease were excluded. This study was approved by the human research ethics committees of Nagoya University Hospital (no. 2016-0275).

Flowchart of the inclusion process. PH pulmonary hypertension; PAH pulmonary arterial hypertension; CTEPH chronic thromboembolic pulmonary hypertension; CHD congenital heart disease; PH-lung pulmonary hypertension associated with lung disease; PH-LHD pulmonary hypertension associated with left heart disease
Hemodynamic studies
All patients underwent right heart catheterization via right internal jugular vein with a 6-French Thermodilution catheter (Goodman Co. LTD, Nagoya, Japan) to obtain the pulmonary arterial wedge pressure (PAWP), PAP, RV, and right atrial (RA) pressures. Mixed venous oxygen saturation and arterial oxygen saturation were measured in blood taken from each main PA and radial artery. Cardiac output was calculated by indirect Fick method and estimated VO2 values were calculated by LaFarge equation: males, VO2 (mL/min/m2) = [138.1 − (11.49 × logeage) + (0.378 × HR)] × BSA; females, VO2 (mL/min/m2) = [138.1 − (17.04 × logeage) + (0.378 × HR)] × BSA. Pulmonary vascular resistance (PVR) was calculated using the standard formula: PVR = 80 × (mean PAP − mean PAWP)/cardiac output.
Cardiopulmonary exercise testing
All 53 patients underwent exercise testing at a progressively increasing work rate to maximum tolerance on a cycle ergometer. The test was performed according to the American Thoracic Society guidelines [24]. Specifically, 3 min of warm-up was performed with a 10-W loading, followed by a 10-W/min ramp-incremental protocol. Carbon dioxide output (VCO2), VO2, and minute ventilation (VE) were measured continuously on a breath-by-breath basis using an Ergospirometry Oxycon Pro (Carefusion Germany, 234, GmbH, Hochberg, Germany).
Echocardiography
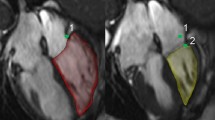
Two-dimensional, M-mode, Doppler echocardiographic images were acquired (iE33, Philips Healthcare, Eindhoven, The Netherlands) and examined according to the guidelines of the American Society of Echocardiography [25, 26]. Patients were examined in the left decubitus position through parasternal long-axis, short-axis, and apical views. The left ventricular internal dimensions at end diastole (LVDd) and end systole (LVDs) were measured in the standard parasternal long-axis view at the level of the mitral valve leaflet tips obtained from two-dimensional echocardiographic images. End diastole was defined as the frame in the cardiac cycle in which the respective LV dimension is the largest. The peak velocity of tricuspid regurgitation was measured by using continuous-wave Doppler echocardiography. Doppler imaging of the mitral valve was performed in the apical four-chamber view. Peak E and peak A wave velocities were obtained from the mitral inflow velocity image. TAPSE was measured using M-mode echocardiography with the cursor placed at the tricuspid lateral annulus in the apical four-chamber view. TAPSE is defined by the total excursion of the tricuspid annulus from its highest position after atrial ascent to the peak descent during ventricular systole. Tissue Doppler echocardiography was performed in the apical four-chamber view, with the tissue sampling volume located at the septal side of the mitral annulus, and the early diastolic velocity wave (e′) was measured.
Statistical analysis
Categorical variables are presented as numbers and percentages (%). Continuous variables are presented as mean ± standard deviation or medians. Pearson correlation was used to assess the strength of the relationship between two variables. We performed stepwise multiple regression analysis to evaluate factors that affected CI, stroke volume index (SVI), and peak VO2. Variables including clinical and laboratory findings, and hemodynamic and echocardiographic parameters were selected on the basis of a significant univariate relation (P < 0.05). A P value of < 0.05 was considered to be statistically significant. All statistical analyses were conducted by using the SPSS statistical software program (SPSS version 18.0 for Windows, SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics
Table 1 shows patient characteristics. The mean age of the patients was 53.7 years, and 16 (30%) were men. Among 53 patients, 23 patients had PAH and 30 had CTEPH. Of these 53 patients, 12 (23%) were already receiving oral PH-specific drug therapy prescribed in a referral hospital. The remaining 41 (77%) patients were treatment naive. 19 (36%) were in WHO functional class III/IV.
Hemodynamics at rest and echocardiography
The mean TRPG and TAPSE in 53 patients were 74.1 mmHg and 17.3 mm, respectively, highly indicative of severe PH (Table 2). As patients who had left heart disease had been excluded from the enrollment, the LV internal dimension, LV wall thickness, and left atrial dimension (LAD) of our patients were all within normal limits. In our PH patients, the septal e′ was decreased and E/A ratio was reduced, both suggesting impaired left ventricular relaxation. Meanwhile, overall hemodynamic data from our patient population suggested severe PH with low cardiac output.
Correlations of echocardiographic parameters and hemodynamics at rest are shown in Fig. 2 and Supplement 3. TRPG was significantly and positively correlated with mean PAP, while LVDd and TAPSE were significantly and negatively correlated with mean PAP. LVDd, septal e′, and TAPSE were significantly and positively correlated with CI and SVI, while TRPG was significantly and negatively correlated with CI and SVI.

a Relation of cardiac index (CI) to left ventricular end-diastolic dimension (LVDd), early diastolic velocity of the septal mitral annulus (septal e′), tricuspid annular plane systolic excursion (TAPSE), and pressure gradient of tricuspid regurgitation (TRPG). b Relation of stroke volume index (SVI) to LVDd, e′, TAPSE, and TRPG
Then, stepwise multiple regression analysis was performed to analyze which factors influenced CI, a well-known prognostic marker for PAH, in our patients. Among the variables including clinical and laboratory findings, hemodynamic and echocardiographic parameters, the independent variables used in this analysis, were selected on the basis of a significance of univariate analysis: age, brain natriuretic peptide (BNP), mean PAP, E, septal e′, LVDd, TAPSE, and TRPG. We also included heart rate (HR) as an independent variable for clinical importance. SvO2 was excluded from the analysis because it was included in the formula of Fick method. The result indicated that LVDd and septal e′ were significantly associated with CI at rest (Table 3).
In addition, we analyzed SVI which is an important determinant of CI. Stepwise multiple regression analysis was performed incorporating same independent variables used in CI analysis, except HR. The result indicated that LVDd, septal e′, and BNP were significantly associated with SVI, which was compatible with the result of CI (Table 4).
Exercise capacity and echocardiography
No complication was observed during CPET. The values for peak VO2 indicated severe exercise intolerance in these patients (Table 2). In terms of relationships between parameters of echocardiography and exercise capacity, LVDd and TAPSE were significantly and positively correlated with peak VO2, and TRPG was significantly and negatively correlated with peak VO2 (Fig. 3).

Relation of peak oxygen uptake (VO2) to left ventricular end-diastolic dimension (LVDd), early diastolic velocity of the septal mitral annulus (septal e′), tricuspid annular plane systolic excursion (TAPSE), and pressure gradient of tricuspid regurgitation (TRPG)
To identify parameters predictive of peak VO2, which is indicative of prognosis in patients with PH, we performed stepwise multiple regression analysis. Among the variables including clinical and laboratory findings, hemodynamic and echocardiographic parameters, the independent variables used in this analysis were World Health Organization functional class (WHO-FC), BNP, heart rate, CI, mean PAP, SvO2, LVDd, TAPSE, and TRPG. Among those, TAPSE and SvO2 were significantly associated with peak VO2 (Table 5).
Discussion
In the present study, LVDd and septal e′ in patients with PAH and CTEPH were significantly associated with CI and SVI. TAPSE was significantly associated with peak VO2.
In our present patients with PH, echocardiographic parameters of LV at diastole reflected CI, a key prognostic factor of PAH. As PH progresses, direct or sequential interaction between the RV and LV leads to impaired LV filling. In the direct interaction, the LV cavity is compressed owing to leftward bowing of the ventricular septum, causing impaired LV filling, reduced LV preload, and low cardiac output [21]. In the sequential mechanism, an increased RV afterload decreases RV output, with consequent decreases in LV preload and LV output [27]. These hemodynamic changes due to underfilling of the LV, regardless of the underlying mechanism, result in decreased LV output. Therefore, the echocardiographic parameter LVDd is a good representative of the LV end-diastolic volume, and a decreased e′ indicates an abnormality in LV relaxation.
LVDd was reduced and strongly correlated with SVI and CI in our PAH and CTEPH patients, which is comparable to the study using MRI in patients with PAH [21]. In their study, LV end-diastolic volume was decreased and the LV end-diastolic volume index was strongly correlated with SVI. Eccentricity index measured by echocardiography is used to evaluate LV compression for hemodynamic assessment in PH patients [7]. However, our study indicated that LVDd by itself, which is typically and easily measured during routine echocardiographic examinations, could also be a highly useful parameter that is indicative of CI. Estimated cardiac output can be directly measured by echocardiography. However, LVDd can be more easily measured with less observer bias; thus LVDd also could be a useful marker to assess the severity of patients with PAH and CTEPH. In addition, septal e′ was significantly associated with SVI and CI in our patients with PH, which may indicate abnormal early diastolic underfilling of the LV. In an MRI study of PAH, the filling rate at the time of maximal septal curvature was found to be significantly correlated with the LV end-diastolic volume [21]. In another study, patients with CTEPH who were evaluated before undergoing pulmonary endarterectomy demonstrated LV diastolic dysfunction, which was likely reflective of low LV preloading and underfilling [27]. In our study, mitral E velocity and E/A ratio were decreased to similar levels that were reported in patients with CTEPH by Gurudevan et al. [27]. In addition, the same group reported lateral e′—but not septal e′—improved soon after pulmonary endarterectomy. In our study, whether the reduced septal e′ represents LV underfilling or true LV diastolic dysfunction remains unclear. Nonetheless, our results suggest that evaluation of LV as well as RV functions is important in PH patients.
Peak VO2 during exercise is an important prognostic factor in PAH patients [23]. In the present study, low TAPSE, indicating systolic RV dysfunction and low SvO2, was significantly associated with low peak VO2. Sharma et al. reported a study of dobutamine stress transthoracic echocardiography in patients with PAH, in which both tricuspid annular systolic velocities (s′) measured at rest and after dobutamine stress were strongly correlated with peak VO2. [28] Additionally, TAPSE at rest was also significantly correlated with peak VO2. These previous results and our results together indicate that RV function is strongly associated with exercise capacity and that assessment of RV systolic function using echocardiography is informative regarding exercise capacity in patients with PAH and CTEPH.
Our study had several limitations. Because it was carried out in the context of current clinical practices, we were unable to perform echocardiography, right heart catheterization, and CPET all on the same day. Right heart catheterization was performed within a median 15 days before and after echocardiography and median 17 days before and after CPET, and each patient received the same drugs with the same dose throughout all examinations. In addition, we evaluated lateral e′, total RV linear measurements, fractional area change, Doppler tissue imaging-derived tricuspid lateral annular systolic velocity wave, RV index of myocardial performance, and longitudinal strain only in limited patients. Therefore, although septal e′ is an established relaxation marker in left-sided heart failure, its usage as a marker for the abnormal LV relaxation, specifically in patients with PAH and CTEPH, remains unclear. Furthermore, because we excluded PH patients with left heart disease, chronic lung disease, or congenital heart disease, future studies are warranted to evaluate whether our results could be applied to PH patients with these comorbidities. Finally, we evaluated patients only at the time of their first admission to our hospital. How each echocardiographic parameter changes as a consequence of patient’s condition remains to be assessed in future.
In conclusion, we demonstrated that, in patients with PAH and CTEPH, LVDd and septal e′ were significantly associated with CI, whereas TAPSE was significantly associated with peak VO2. Our results indicate that evaluating both LV and RV functions is important in PAH and CTEPH patients. Furthermore, echocardiography—particularly several simple parameters measured frequently in clinical practice—is useful in predicting CI obtained through invasive techniques at rest and peakVO2 during exercise obtained by great physical effort.
References
Dalonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT, Levy PS, Pietra GG, Reid LM, Reeves JT, Rich S, Vreim CE, Williams GW, Wu M (1991) Survival in patients with Primary Pulmonary Hypertension: results from a National Prospective Registry. Ann Intern Med 115:343–349
Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, Yaici A, Weitzenblum E, Cordier JFO, Chabot F, Dromer C, Pison C, Reynaud-Gaubert M, Haloun A, Laurent M, Hachulla E, Simonneau G (2006) Pulmonary arterial hypertension in France—results from a national registry. Am J Respir Crit Care Med 173:1023–1030
Benza RL, Miller DP, Gomberg-Maitland M, Frantz RP, Foreman AJ, Coffey CS, Frost A, Barst RJ, Badesch DB, Elliott CG, Liou TG, McGoon MD (2010) Predicting survival in pulmonary arterial hypertension insights from the registry to evaluate early and long-term pulmonary arterial hypertension disease management (REVEAL). Circulation 122:164–172
Farber HW, Miller DP, Poms AD, Badesch DB, Frost AE, Muros-Le Rouzic E, Romero AJ, Benton WW, Elliott CG, McGoon MD, Benza RL (2015) Five-year outcomes of patients enrolled in the REVEAL registry. Chest 148:1043–1054
Tahara N, Dobashi H, Fukuda K, Funauchi M, Hatano M, Ikeda S, Joho S, Kihara Y, Kimura T, Kondo T, Matsushita M, Minamino T, Nakanishi N, Ozaki Y, Saji T, Sakai S, Tanabe N, Watanabe H, Yamada H, Yoshioka K, Sasayama S (2016) Efficacy and safety of a novel endothelin receptor antagonist, Macitentan, in Japanese patients with pulmonary arterial hypertension. Circ J 80:1478–1483
Hatano M, Yamada H, Fukuda K, Yoshioka K, Funauchi M, Kuwana M, Sata M, Taniguchi M, Nakanishi N, Saito T, Saji T, Sasayama S (2015) Effects of the endothelin receptor antagonist bosentan on hemodynamics and exercise capacity in Japanese patients with mildly symptomatic pulmonary arterial hypertension. Heart Vessels 30:798–804
Raymond RJ, Hinderliter AL, Willis PW, Ralph D, Caldwell EJ, Williams W, Ettinger NA, Hill NS, Summer WR, de Boisblanc B, Schwartz T, Koch G, Clayton LM, Jobsis MM, Crow JW, Long W (2002) Echo cardiographic predictors of adverse outcomes in primary pulmonary hypertension. J Am Coll Cardiol 39:1214–1219
Benza R, Biederman R, Murali S, Gupta H (2008) Role of cardiac magnetic resonance imaging in the management of patients with pulmonary arterial hypertension. J Am Coll Cardiol 52:1683–1692
van de Veerdonk MC, Marcus JT, Westerhof N, de Man FS, Boonstra A, Heymans MW, Bogaard HJ, Noordegraaf AV (2015) Signs of right ventricular deterioration in clinically stable patients with pulmonary arterial hypertension. Chest 147:1063–1071
Austin C, Alassas K, Burger C, Safford R, Pagan R, Duello K, Kumar P, Zeiger T, Shapiro B (2015) Echocardiographic assessment of estimated right atrial pressure and size predicts mortality in pulmonary arterial hypertension. Chest 147:198–208
Peacock AJ, Crawley S, McLure L, Blyth K, Vizza CD, Poscia R, Francone M, Iacucci I, Olschewski H, Kovacs G, Noordegraaf AV, Marcus JT, van de Veerdonk MC, Oosterveer FPT (2014) Changes in right ventricular function measured by cardiac magnetic resonance imaging in patients receiving pulmonary arterial hypertension-targeted therapy the EURO-MR study. Circ Cardiovasc Imaging 7:107–114
Doutreleau S, Canuet M, Enache I, Di Marco P, Lonsdorfer E, Oswald-Mammoser M, Charloux A (2016) Right heart hemodynamics in pulmonary hypertension—an echocardiography and catheterization study. Circ J 80:2019–2025
Kasai H, Matsumura A, Sugiura T, Shigeta A, Tanabe N, Yamamoto K, Miwa H, Ema R, Sakao S, Tatsumi K (2016) Mean pulmonary artery pressure using echocardiography in chronic thromboembolic pulmonary hypertension. Circ J 80:1259–1264
Hayabuchi Y, Ono A, Kagami S (2016) Pulmonary annular motion velocity assessed using doppler tissue imaging—novel echocardiographic evaluation of right ventricular outflow tract function. Circ J 80:168–176
Amano H, Abe S, Hirose S, Waku R, Masuyama T, Sakuma M, Toyoda S, Taguchi I, Inoue T, Tei C (2017) Comparison of echocardiographic parameters to assess right ventricular function in pulmonary hypertension. Heart Vessels. https://doi.org/10.1007/s00380-017-0991-6
Hioka T, Kaga S, Mikami T, Okada K, Murayama M, Masauzi N, Nakabachi M, Nishino H, Yokoyama S, Nishida M, Iwano H, Sakakibara M, Yamada S, Tsutsui H (2017) Overestimation by echocardiography of the peak systolic pressure gradient between the right ventricle and right atrium due to tricuspid regurgitation and the usefulness of the early diastolic transpulmonary valve pressure gradient for estimating pulmonary artery pressure. Heart Vessels 32:833–842
Hachulla E, Gressin V, Guillevin L, Carpentier P, Diot E, Sibilia J, Kahan A, Cabane J, Frances C, Launay D, Mouthon L, Allanore Y, Tiev KP, Clerson P, de Groote P, Humbert M (2005) Early detection of pulmonary arterial hypertension in systemic sclerosis—a French nationwide prospective multicenter study. Arthritis Rheum 52:3792–3800
Forfia PR, Fisher MR, Mathai SC, Housten-Harris T, Hemnes AR, Borlaug BA, Chamera E, Corretti MC, Champion HC, Abraham TP, Girgis RE, Hassoun PM (2006) Tricuspid annular displacement predicts survival in pulmonary hypertension. Am J Respir Crit Care Med 174:1034–1041
Yock PG, Popp RL (1984) Noninvasive estimation of right ventricular systolic pressure by doppler ultrasound in patients with tricuspid regurgitation. Circulation 70:657–662
Mori S, Nakatani S, Kanzaki H, Yamagata K, Take Y, Matsuura Y, Kyotani S, Nakanishi N, Kitakaze M (2008) Patterns of the interventricular septal motion can predict conditions of patients with pulmonary hypertension. J Am Soc Echocardiogr 21:386–393
Gan CTJ, Lankhaar JW, Marcus JT, Westerhof N, Marques KM, Bronzwaer JGF, Boonstra A, Postmus PE, Vonk-Noordegraaf A (2006) Impaired left ventricular filling due to right-to-left ventricular interaction in patients with pulmonary arterial hypertension. Am J Physiol Heart Circ Physiol 290:H1528–H1533
Swift AJ, Rajaram S, Capener D, Elliot C, Condliffe R, Wild JM, Kiely DG (2015) Longitudinal and transverse right ventricular function in pulmonary hypertension: cardiovascular magnetic resonance imaging study from the ASPIRE registry. Pulm Circ 5:557–564
Wensel R, Opitz CF, Anker SD, Winkler J, Hoffken G, Kleber FX, Sharma R, Hummel M, Hetzer R, Ewert R (2002) Assessment of survival in patients with primary pulmonary hypertension importance of cardiopulmonary exercise testing. Circulation 106:319–324
American Thoracic Society; American College of Chest Physicians (2003) ATS/ACCP statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med 167:211–277
Lang RMBL, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D, Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 28(1–39):e14
Rudski LG, Lai WW, Afilalo J, Hua LQ, Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK, Schiller NB (2010) guidelines for the echocardiographic assessment of the right heart in adults: a Report from the American Society of Echocardiography Endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr 23:685–713
Gurudevan SV, Malouf PJ, Auger WR, Waltman TJ, Madani M, Raisinghani AB, DeMaria AN, Blanchard DG (2007) Abnormal left ventricular diastolic filling in chronic thromboembolic pulmonary hypertension—true diastolic dysfunction or left ventricular underfilling? J Am Coll Cardiol 49:1334–1339
Sharma T, Lau EMT, Choudhary P, Torzillo PJ, Munoz PA, Simmons LR, Naeije R, Celermajer DS (2015) Dobutamine stress for evaluation of right ventricular reserve in pulmonary arterial hypertension. Eur Respir J 45:700–708
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Takahisa Kondo, Naoki Okumura, and Shiro Adachi belong to the department that has been provided endowment from Actelion Pharmaceuticals Japan, Ltd.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Nakano, Y., Okumura, N., Adachi, S. et al. Left ventricular end-diastolic dimension and septal e′ are predictors of cardiac index at rest, while tricuspid annular plane systolic excursion is a predictor of peak oxygen uptake in patients with pulmonary hypertension. Heart Vessels 33, 521–528 (2018). https://doi.org/10.1007/s00380-017-1086-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-017-1086-0