
Abstract
Introduction
More than 100 surgical techniques are described for hallux valgus (HV) correction, but the most appropriate technique remains debatable. The aim of this study was to develop and conduct a “living systematic review” for the outcome of surgically treated HV.
Materials and methods
The “living systematic review” was conducted per the PRISMA-P and PICOS guidelines and is the basis for the German AWMF S2e guideline “Hallux valgus” (033-018). Four common databases and the grey-literature were searched. Eligible were studies on adult patients comparing either two different primary surgical interventions or the same primary surgical intervention for different hallux valgus severities. The main outcome parameters were the osseous correction potential and the patient rated outcome.
Results
Out of 3022 studies, 46 studies (100 arms) were included. The meta-analysis included 31 studies (53 arms). The IMA (1933 procedures) improved on average by 7.3°, without significant group differences. The HVA (1883 procedures) improved on average by 18.9°, with significantly better results for third generation MIS (21.2°). The AOFAS (1338 procedures) improved on average by 33.8 points without significant group differences. The meta-regression revealed constant AOFAS scores over time. 69%/39% of the correction potential for the IMA/HVA could be explained by the preoperative values and 82% of the AOFAS improvement by the preoperative AOFAS scores.
Conclusion
Open and minimally invasive techniques are powerful tools to correct hallux valgus deformity. Third generation MIS procedures revealed a possible superiority for the correction of the HVA. The AOFAS improvement appeared to be constant over time.
Level of evidence
Level I; living systematic review and meta-analysis of prospective comparative studies (level II) and randomized controlled trials (level I).
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Hallux valgus (HV) is one of the most common forefoot deformities, characterized by a lateral deviation of the great toe and a medial deviation of the first metatarsal bone [1]. After failed conservative treatment, surgery can realign the first ray [2]. According to Mann and Coughlin, HV can be divided into three grades based on the intermetatarsal angle (IMA) and hallux valgus angle (HVA) measured on dorso-plantar weightbearing radiographs: mild (IMA < 11°, HVA < 20°), moderate (IMA 11–16°, HVA 20–40°), and severe (IMA > 16°, HVA > 40°) [1]. Overall, more than one hundred surgical techniques are described for HV correction. These can be grouped into distal-, diaphyseal-, or proximal osteotomies, and arthrodesis.
More recently, percutaneous and minimally invasive surgical techniques have gained increasing recognition, because of the potential advantages of better range of motion (ROM) and less soft tissue trauma [3, 4]. Until now, three generations of minimally invasive HV surgery have been developed. The first generation, reported in 1991, was the Reverdin Isham technique, which was performed without internal fixation [5]. The second generation is the Bösch osteotomy [6], using Kirschner wires for fixation [7]. The minimally invasive chevron and akin (MICA) described by Vernois and Redfern represents the third generation, using screws for fixation [8,9,10]. Recently, an adaptation variant of this technique was described, using a metaphyseal extra-articular transverse and akin osteotomy (META) [11].
Although the type of surgical procedure is traditionally chosen according to the severity of the HV deformity [10, 12], the decision remains up to the surgeon’s preference [13]. Up to date, a consensus on the most appropriate treatment approach is still missing. Traditionally, mild deformities are addressed by distal osteotomies, moderate deformities by shaft osteotomies, and severe deformities by proximal osteotomies or arthrodesis [14].
The aim of this study was to (1) develop a “living systematic review” for the outcome of surgically treated hallux valgus and to (2) apply and analyze this search strategy for the timeframe from Jan 1st 2012 to Jan 31st 2023. The “living systematic review” is the basis for regular (5-year interval) updates of the German AWMF S2e guideline “Hallux valgus” (033-018). The two primary outcome variables are the osseous correction and the patient rated outcome.
Materials and methods
The living systematic review is the basis for regular (5-year interval) updates of the German AWMF S2e guideline “Hallux valgus” (033-018). The herein developed and applied systematic review was conducted per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-P) guidelines [15]. The study was a-priori registered at Prospero (CRD42021261490). The PICOS criteria were changed throughout the review process. Due to the large number of studies available, only original comparative studies, prospective or randomized controlled trials, were included. This amendment was reported to Prospero.
Search strategy
MEDLINE (PubMed), Scopus, Central, and EMBASE were searched from inception to Jan 31st 2023. For the current analysis, studies prior to Jan 1st 2012 were excluded. A grey literature search was performed in both Scopus and EMBASE including conference proceedings. Additionally, all references of the studies included were hand-searched. The search strategy comprised of the following principal strategies: Hallux valgus AND Surgery. The detailed search strategy is outlined in Supplement 1.
The in- and exclusion criteria were designed according to the Population, Intervention, Comparison, Outcomes and Study (PICOS) criteria and are summarized in Table 1 [16].
Other etiologies, such as trauma or revision surgery, were excluded. Studies were allowed to perform accompanying interventions to the lesser metatarsals, such as Weil osteotomy/DMMO or toe deformity corrections.
Study selection and data extraction
The resulting datasets of each database were exported to EndnoteTM (Vs. 20.1; Fa. Clarivate) and duplicates were removed according to their standard algorithm. The final dataset was imported into CovidenceTM (Melbourne, Australia), in which the complete study selection process was conducted.
Two intendent reviewers (SE, SFB) conducted the whole study selection and data extraction process. In case of disagreement at the stage of title/abstract screen, the studies were moved to full-text screen. Disagreement at the stage of full text-search was resolved by discussion with a third reviewer (HP).
Table 2 shows the data extracted from all qualified primary studies which were recorded on separate data extraction sheets. For the radiologic and clinical data, these were assessed for each time point presented. Radiographic measurements must have been conducted on weightbearing radiographs.
Risk of bias assessment
The risk of bias assessment was conducted by two independent reviewers (FTS, SFB). For original studies, the level of evidence was rated per the recommendations of Wright et al. [17]. RCTs were assessed per the The Risk of Bias 2 (RoB 2) tool [18]. In case of a non-randomized prospective study, the Newcastle–Ottawa scale was used to assess risk of bias [19].
Study analysis Jan 1st 2012–Jan 31st 2023
The aim was to perform a meta-analysis to compare the efficacy of different treatment strategies for hallux valgus surgery. Efficacy was defined as the osseous correction and the patient rated outcome per the individual surgical procedures. A multi-step study selection process was performed to identify those studies eligible for a meta-analysis.
First, all studies were grouped per their primary comparator, i.e. comparison of two different surgical procedures or different severities. Then all studies were pooled per their surgical procedures. These were categorized per the anatomical location into open distal, shaft, proximal, or arthrodesis and MIS procedures. The individual studies within each category were then assessed for sufficient comparability. Studies were considered sufficiently comparable if the surgical procedure followed similar biomechanical principles. The studies were transferred into a single data extraction Excel-sheet (Vs. 16.73, Microsoft, Redmond, Washington, USA), listing all radiographic and patient rated outcome measures assessed per the individual studies. For the radiological as well as the patient rated outcome parameters, the time of evaluation was noted.
Only studies comparing different surgical procedures were eligible for a further meta-analysis. Studies comparing different degrees of severity were excluded as the principal grouping resembles a selection bias for the further meta-analysis. The principle meta-analysis was done for all studies per the different surgical techniques. In case of follow-up studies, the initial study was included in the meta-analysis. For the osseous correction, no baseline evaluation was performed as only RCTs and prospective studies were included, which most often defined the degree of deformity as an inclusion criterion. This selection bias limits the significance of the degree of preoperative deformity per the different surgical procedures. Therefore, the osseous correction was defined as the difference between the initial and follow-up values. This was done for all radiographic parameters assessed and separated for the type of surgical procedure and follow-up period. Furthermore, any patient rated outcome measure of any other objective outcome parameter was assessed, if presented in at least three studies.
Finally, a meta-regression was performed to investigate the influence of the follow-up duration and initial deformity (IMA, HVA) on the primary outcome parameters, i.e. improvement of the IMA, HVA, and AOFAS score.
Data synthesis and statistics
Statistical analyses were performed using R 4.05 and the package “meta” version 5.6 to estimate the pooled pre-post differences for IMA, HVA, DMAA, and AOFAS. Heterogeneity among studies was assessed using I2 test. Effect sizes were compared by osteotomy applying the random effects model. Individual and pooled effect sizes with associated 95% CI were displayed in Forest plots. Studies without SD were excluded from pooled calculations, but were included in forest plots. Confidence intervals for individual studies are based on t-distributions. Missing baseline and final mean and SD data were calculated by approximation according to Luo et al. and Shi et al., respectively, as recommended by Cochrane [20, 21]. To minimize bias, change from baseline SD were imputed assuming a rather conservative correlation between baseline and final values of r = 0.4, however, results were confirmed in a sensitivity analysis with r = 0.75. Subgroup analysis and meta-regression analyses were conducted to investigate the source of variability between studies. This included follow-up time and baseline values. The presence of publication bias was visually assessed by Funnel plots to measure the asymmetry quantitatively with Egger’s test assuming p values less than 0.05 as significant publication bias. Trim-fill analysis was applied to adjust for potential publication bias.
Results
Search
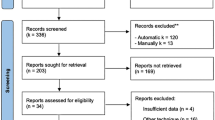
The study selection process is outlined in Fig. 1. After removal of duplicates, a total of 3022 studies were screened for title and abstract and 378 for full-text. 46 primary studies [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67] met the herein defined eligibility criteria. 40 studies [22, 24,25,26,27,28,29,30,31,32,33,34,35, 37,38,39,40,41, 43, 45,46,47,48, 50,51,52,53,54,55,56,57, 59,60,61,62,63,64,65,66,67] compared different surgical procedures and six studies [23, 36, 42, 44, 49, 58] the same surgical intervention for different severities of hallux valgus deformity.

PRISMA flow chart
Studies overview
Theses 46 studies (100 arms) [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67] were assessed for their suitability to be included in the meta-analysis (Fig. 2). The cohort consisted of 40 studies comparing different surgical therapies [22, 24,25,26,27,28,29,30,31,32,33,34,35, 37,38,39,40,41, 43, 45,46,47,48, 50,51,52,53,54,55,56,57, 59,60,61,62,63,64,65,66,67], 30 of which were RCTs [22, 24, 25, 27,28,29,30,31, 33, 34, 37, 39, 40, 46,47,48, 50,51,52,53,54,55,56, 59, 61, 62, 64,65,66,67]. Ten studies were prospective comparative cohort or matched group analyses [26, 32, 35, 38, 41, 43, 45, 57, 60, 63], and six studies compared the same surgical procedure at varying degrees of hallux valgus severity [23, 36, 42, 44, 49, 58], all of which were prospective studies. The risk of bias assessment, separate for RCTs (ROB2) and non-randomized prospective trials (Newcastle-Ottawa-Scale), is presented in Supplement 2. Overall, no RCT had a low, 28 RCTs a moderate [22, 24, 25, 28,29,30,31, 33, 34, 37, 39, 40, 46, 47, 50,51,52,53,54,55,56, 59, 61, 62, 64,65,66,67], and two studies a high risk of bias [27, 48]. The Newcastle-Ottawa-Scale per the 16 prospective non-randomized studies resulted in a mean total quality score 6 ± 1 equaling moderate risk of bias [23, 26, 32, 35, 36, 38, 41,42,43,44,45, 49, 57, 58, 60, 63]. Overall, 23 studies (33 arms) included at least one arm with an open distal Chevron osteotomy [25, 28, 29, 36, 37, 39, 40, 42, 43, 45, 46, 50, 51, 53,54,55,56, 58,59,60,61, 65, 67], 16 studies (23 arms) an open Scarf osteotomy [22, 24, 29, 32, 33, 37, 44, 47, 49,50,51,52, 57, 60, 62, 64], three studies (3 arms) an open proximal Chevron osteotomy [34, 46, 55], four studies (5 arms) an open TMT I fusion [30, 31, 35, 43]. Six studies (6 arms) included a 2nd generation MIS [33, 39, 40, 53, 54, 61], and seven studies (9 arms) a 3rd generation MIS procedure [26, 28, 32, 38, 41, 47, 64], and 11 studies (16 arms) other, incomparable procedures for hallux valgus [22, 23, 25, 27, 30, 31, 34, 62, 63, 65, 66]. One study group [32] was contacted throughout the review process, as they did not report on the actual follow-up period. The authors stated to have a mean follow-up of two years, however they could not provide the mean ± SD. Therefore, the follow-up was defined as 2 years.

Overview of the eligible studies. Yellow: Open Chevron osteotomy; Grey: Other open distal osteotomies; Orange: Open Scarf osteotomy; Red: Other open shaft osteotomies; Blue: Proximal first metatarsal osteotomies; Salmon: Open first tarso-metatatarsal arthrodesis; Dark green: Second generation MIS; Light green: Third generation MIS (MICA, PECA, MIS Scarf); t: Preoperative/Final follow-up; tt: Pre/Postoperative; ttt: preoperativ/postoperative/Final follow-up; zzz: Preoperative; z: Postoperative; zz: Final follow-up; *: incomplete
Meta-analysis
Per the above outlined criteria, 31 studies, comprising of 53 study arms were included in the final meta-analysis [22, 24,25,26, 28,29,30, 32,33,34,35, 37,38,39, 41, 43, 45,46,47, 50, 52,53,54,55,56, 60,61,62, 64, 65, 67]. Excluded were all six studies comparing different severity [23, 36, 42, 44, 49, 58], four studies on surgical procedures incomparable to the remaining procedures [27, 48, 63, 66], two follow-up studies [31, 40], and one study each that presented the outcome data only in a graph [51], assessed incomparable outcome parameters [57], or did not report outcomes separately for the groups [59]. Of the resulting 31 studies, one study arm had to be excluded in eight studies because of incomparable surgical procedures [22, 25, 29, 30, 34, 50, 62, 65].
The IMA, HVA, and the AOFAS were the only outcome parameters assessed by at least three studies. The IMA/HVA/AOFAS were assessed preoperative and at some point postoperatively by 29 studies [22, 24,25,26, 28,29,30, 32,33,34,35, 37,38,39, 41, 45,46,47, 50, 52,53,54,55,56, 61, 62, 64, 65, 67] (49 arms)/30 studies (51 arms) [22, 24,25,26, 28,29,30, 32,33,34,35, 37,38,39, 41, 43, 45,46,47, 50, 52,53,54,55,56, 61, 62, 64, 65, 67]/ and 23 studies (41 arms) [22, 30, 32,33,34,35, 37,38,39, 46, 47, 53, 55, 56, 60,61,62, 64, 65]. These studies were eligible for a further meta-analysis. The authors have also tried to conduct a summative analysis of the complication rates. Due to a high heterogeneity in the definition of minor and major complications, no meaningful analysis could be conducted.
Among the 31 studies included, 23 studies (38 arms) were RCTs [22, 24, 25, 28,29,30, 33, 34, 37, 39, 46, 47, 50, 52,53,54,55,56, 61, 62, 64, 65, 67], all with moderate risk of bias per the ROB2 tool and eight studies (15 arms) [26, 32, 35, 38, 41, 43, 45, 60] were non-randomized prospective trials with a mean Newcastle-Ottawa-Scale of 6 ± 2 resulting in moderate risk of bias. The patients mean age was 50 ± 9 years, 88 ± 19% were female and the mean follow-up was 34 ± 37 months. The results of the meta-analysis for the IMA (Fig. 3A), HVA (Fig. 3B), and AOFAS (Fig. 3C) are summarized in Fig. 3. The individual forest-plots are presented in Supplement 3. Based on 1933 procedures, the IMA values improved on average by 7.3 (CI 95%: 6.7°; 7.9°), without significant differences between the different osteotomy groups. Based on 1883 procedures, the HVA improved on average by 18.9° (CI 95%: 17.3°; 20.4°). Third MIS generation procedures resulted in a significantly better HVA correction (21.2° (CI 95%: 19.2°; 23.2°) compared to all other procedures. Based on 1338 procedures, the AOFAS score improved on average by 33.8 points (CI 95%: 30.5; 37.0). No significant differences were observed between the different procedures.

Abbreviated summary of the meta-analysis for the IMA, HVA, and AOFAS. IMA intermetatarsal angle, HVA hallux valgus angle, AOFAS American Orthopaedic Foot and Ankle Society Score
Overall, the meta-analysis revealed substantial heterogeneity between studies and subgroups (> 90%, p < 0.001) except for the AOFAS Chevron proximal (I2: 0%, p = 0.555) which included only two studies (see Forest Plots). Funnel plots were symmetric for DMAA (Egger’s test p = 0.79) and AOFAS (p = 0.065), but were asymmetric for IMA (p < 0.0001) and HVA (p = 0.03). When the Trim-fill method was applied, the adjusted IMA Pre-Post difference was 5.90° [95% CI 5.16°; 6.63°] (18 additional studies), and the HVA Pre-Post difference was 20.21° [95% CI 18.98°; 22.63°] (9 additional studies). Within the sensitivity analyses, we were also able to confirm the results with higher correlation values between the pre and post values.
Meta-regression
Finally, the authors tried to assess the influence of the follow-up duration and initial deformity (IMA, HVA) on the primary outcome parameters, i.e. improvement of the IMA, HVA, and AOFAS score.
Firstly, the studies included were analyzed to see if the follow-up duration has an influence on the correction potential (difference pre- and post-operative values of IMA and HVA). Overall, there appears to be only a limited causal relationship, which was predominantly triggered by six studies. The AOFAS score showed no considerable change over time.
Secondly, a possible influence of the preoperative values (IMA, HVA, AOFAS) on the correction potential (difference pre- and post-operative values of IMA and HVA) was assessed. 69%/39% of the correction potential for both, IMA and HVA, could be explained by the respective preoperative values. For the improvement of the AOFAS, 82% could be explained by the preoperative AOFAS score (Fig. 4).

Meta-regression plotted and individual per studies. IMA intermetatarsal angle, HVA hallux valgus angle, AOFAS American Orthopaedic Foot and Ankle Society Score, pre-OP preoperative, MIS minimal invasive surgery
Discussion
This systematic review and meta-analysis aimed to develop a “living systematic review” for the outcome of surgically treated hallux valgus, focusing on the osseous correction and the patient rated outcome, separately for the surgical procedure used. The results of this meta-analysis showed that the osseous correction, measured by IMA and HVA, and postoperative clinical outcome, based on the AOFAS score, did not differ significantly for the included surgical procedures, except for significantly higher correction of HVA in 3rd MIS generation procedures. All surgical procedures showed a significant postoperative improvement of the AOFAS score by a mean of 33.8 points, which was well above the MCID (AOFAS 7.9) [68]. The improvement was best explained by the low pre-operative AOFAS scores in patients undergoing surgery for symptomatic hallux valgus.
The severity of the hallux valgus deformity may be classified into ‘mild’, ‘moderate’ and ‘severe’ [1]. Interestingly, the traditional classification proposed by Mann and Coughlin, has not been applied uniformly throughout the studies included herein. The upper limits of the IMA for mild/moderate/severe ranged between 9° [54]/12° [47]/17° [55, 56] and 15° [45]/20° [27, 29, 50, 65]/20° [29, 50, 54] degrees. This limits the comparability between studies. Journals and authors should agree on a uniform definition for hallux valgus deformities. With novel imaging modalities emerging, a uniform definition should also include the distal metatarsal articular angle and the rotation of the first metatarsal, to more clearly define the pathology.
The preoperative IMA/HVA differed widely between each procedure. Contrary to expectations, a correlation between the preoperative IMA/HVA and the surgical procedure, i.e. more proximal techniques for more severe deformities, could not be shown. Since no differences in the osseous correction potential per the different surgical procedures could be detected, the question arises whether the correction potential of the presumably more powerful, proximal techniques was underestimated. One reason could be the inclusion of less severe deformities into this group as evidenced by missing correlation between preoperative angles and surgical procedure. Secondly, a source of bias could be the number of studies included. A substantially lower number of studies reported on TMT 1 arthrodesis (n = 3; arms: n = 4; patients: n = 161) patients), compared to distal chevron- (n = 14; arms: n = 17; patients: n = 639), proximal chevron (n = 3; arms: n = 3; patients: n = 137), scarf-osteotomy (n = 11; arms: n = 13; patients: n = 537), MIS2nd generation (n = 5; arms: n = 5; patients: n = 161) and MIS 3rd generation (n = 7; arms: n = 9; patients: n = 347). Thirdly, due to the small number of studies included in the arthrodesis group, a single study reporting inferior outcomes has a pronounced effect on the final result, which was the case for the study of Klemola et al. [43]. Finally, the choice of the surgical procedure cannot be solely based on the preoperative IMA and HVA. Factors such as instability of the medial column, severe rotational malalignment of the MT I and TMT I arthritis represent main indications for a TMT 1 arthrodesis [69,70,71].
Over the last decade there is a trend towards minimally invasive hallux valgus surgery [10, 72, 73]. In our meta-analysis, 3rd MIS generation showed significantly more correction of HVA compared to the other techniques, whereas there were no differences in the correction of IMA and improvement of AOFAS scores. The 2nd MIS generation did not show improved clinical or radiological outcomes compared with the open techniques. This may be due to the fact, that the 3rd MIS generation always includes an akin osteotomy, which has a profound influence on the HVA. An akin procedure was not regularly performed in the included studies with open procedures. A subgroup analysis solely including open procedures with an akin osteotomy was not possible due to missing data. This could bias the results of better HVA correction compared to open procedures. One current meta-analysis compared open versus minimally invasive hallux valgus surgery, including 22 studies, of which eight were RCTs [74]. IMA, HVA, DMAA and the AOFAS score were assessed. Including all 22 studies, there was no significant difference in clinical and radiological outcomes between open and MIS hallux valgus surgery. However, in the subgroup analysis the 2nd MIS generation showed significantly lower postoperative IMA, the 3rd MIS generation significantly lower postoperative HVA compared to open techniques. The AOFAS score was significantly higher in the MIS group, when only RCTs were included. The authors concluded that MIS was more effective than open surgery in the treatment of hallux valgus. When looking at the data presented here, the mid- and long-term results of further RCTs must be awaited before suggesting any superiority of minimally invasive hallux valgus surgery.
The performed meta-regression analysis revealed a tendency towards loss of correction for the IMA and HVA with increasing follow up period, independent of the surgical procedure. However, the AOFAS score was not affected by the follow up duration. The average degree of IMA and HVA correction resulted in a significant improvement of the AOFAS, well above the MCID. Overall, the number of studies with longer follow up was significantly lower, so that only a certain trend could be observed. Similar results were presented in a meta-analysis by Kaufmann et al. comparing MIS distal chevron and MIS reverdin isham osteotomies [41]. In this study, a longer follow up period resulted in a radiological loss of correction (IMA;HVA), which did not influence the AOFAS score. Hence, a certain loss of correction over time might not have a significant impact on the clinical outcome in terms of the AOFAS score.
Overall, each meta-analysis revealed a significant heterogeneity for each parameter assessed. There appears to be a rather broad correction range for each osteotomy individually. This could be due to the initial deformity or the individual surgeons’ skills.
From the visual analysis of the Funnel plots, it appears that the pooled IMA correction potential presented here may have been overestimated because a substantial number of studies with lower pre-post difference for symmetry are missing. Conversely, the pooled HVA correction potential may have been underestimated because studies with higher HVA correction values are missing.
Only comparative studies published after 2012 were included. The number of studies dealing with hallux valgus correction, i.e. single arm studies, is immense and was not included into the current systematic review. Due to a low methodological quality, many studies were excluded for final analysis. As a result, the number of included studies per surgical procedure varies considerably.
In the meantime, indication for surgery is not solely based on traditional radiographic parameters such as IMA and HVA. Simultaneous derotation of the first ray is recognized as one of the key elements in treating hallux valgus to reduce the risk of recurrence [73, 75,76,77,78]. Many studies continue to assess only IMA and HVA and do not include metatarsal rotation. Additionally, the DMAA should be measured to detect a pathological joint line, as this significantly influences the recurrence rate [79]. In this meta-analysis, evaluation of the DMAA per surgical procedure was not possible due to the small number of studies including DMAA measurements. The bony morphology must also be considered, since the width of the first metatarsal affects the possibility of maximum translation. Further studies should include these parameters, in order to enable a more differentiated analysis.
Another limitation is the fact that the surgical techniques may be substantially modified by the individual surgeon based on personal experience and preference (e.g. orientation of osteotomy, extent of lateral soft tissue release). This makes comparison of the same technique between different studies difficult.
Another concern is a missing standardized categorization of postoperative complications into minor and major ones. The data of complications in the included studies differ widely—in some studies recurrence was specified as a complication, in others it was not. Therefore, an evaluation of complications depending on the surgical procedure could not be assessed. Recently, it has been tried to establish a modified Clavien-Dindo classification, which does allow for a considerably more detailed assessment of complications than the traditional grouping into minor and major complications [80]. Such a classification should be defined and regularly applied to enable comparability between surgical procedures in the future.
Conclusion
According to the current evidence, both open and minimally invasive techniques are powerful tools to correct hallux valgus deformity with significantly improved radiological and clinical outcome parameters. Third generation MIS procedures revealed a possible superiority for the correction of the HVA without measurable impact of outcome. Independent of the surgical technique applied, there is a considerable improvement of the AOFAS score which appears to be constant over time, while there is a tendency for loss of correction of the radiologic parameters. We as a community must define uniform reporting strategies for diagnosis, classification, and outcome to increase the comparability between studies.
Data sharing
Data can be shared if necessary.
References
Coughlin MJ, Jones CP (2007) Hallux valgus: demographics, etiology, and radiographic assessment. Foot Ankle Int 28(7):759–777. https://doi.org/10.3113/FAI.2007.0759
Matar HE, Platt SR (2021) Overview of randomised controlled trials in hallux valgus surgery (2,184 patients). Foot Ankle Surg 27(4):351–356. https://doi.org/10.1016/j.fas.2020.04.013
Lai MC, Rikhraj IS, Woo YL, Yeo W, Ng YCS, Koo K (2018) Clinical and radiological outcomes comparing percutaneous chevron-akin osteotomies vs open scarf-akin osteotomies for hallux valgus. Foot Ankle Int 39(3):311–317. https://doi.org/10.1177/1071100717745282
Trnka HJ, Krenn S, Schuh R (2013) Minimally invasive hallux valgus surgery: a critical review of the evidence. Int Orthop 37(9):1731–1735. https://doi.org/10.1007/s00264-013-2077-0
Isham SA (1991) The Reverdin-Isham procedure for the correction of hallux abducto valgus. A distal metatarsal osteotomy procedure. Clin Podiatr Med Surg 8(1):81–94 (not available)
Bernasconi A, Rizzo M, Izzo A, Vallefuoco S, Russo AP, Rossi V et al (2023) Bosch osteotomy for hallux valgus correction: results at a mean 10-year follow-up. Arch Orthop Trauma Surg 143(3):1293–1300. https://doi.org/10.1007/s00402-021-04259-3
Bosch P, Wanke S, Legenstein R (2000) Hallux valgus correction by the method of Bosch: a new technique with a seven-to-ten-year follow-up. Foot Ankle Clin 5(3):485–498 (v-vi)
Vernois J, Redfern DJ (2016) Percutaneous surgery for severe hallux valgus. Foot Ankle Clin 21(3):479–493. https://doi.org/10.1016/j.fcl.2016.04.002
Harrasser N, Hinterwimmer F, Baumbach SF, Pfahl K, Glowalla C, Walther M et al (2023) The distal metatarsal screw is not always necessary in third-generation MICA: a case-control study. Arch Orthop Trauma Surg 143(8):4633–4639. https://doi.org/10.1007/s00402-022-04740-7
Nunes GA, de Carvalho KAM, Ferreira GF, Filho MVP, Baptista AD, Zambelli R et al (2023) Minimally invasive Chevron Akin (MICA) osteotomy for severe hallux valgus. Arch Orthop Trauma Surg 143(9):5507–5514. https://doi.org/10.1007/s00402-023-04849-3
Lewis TL, Lau B, Alkhalfan Y, Trowbridge S, Gordon D, Vernois J et al (2023) Fourth-generation minimally invasive hallux valgus surgery with metaphyseal extra-articular transverse and akin osteotomy (META): 12 month clinical and radiologic results. Foot Ankle Int 44(3):178–191. https://doi.org/10.1177/10711007231152491
Izzo A, Vallefuoco S, Basso MA, Ray R, Smeraglia F, Cozzolino A et al (2023) Role of lateral soft tissue release in percutaneous hallux valgus surgery: a systematic review and meta-analysis of the literature. Arch Orthop Trauma Surg 143(7):3997–4007. https://doi.org/10.1007/s00402-022-04693-x
Ferrari J, Higgins JP, Prior TD (2004) Interventions for treating hallux valgus (abductovalgus) and bunions. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD000964.pub2
Deutsche Gesellschaft für Orthopädie und Orthopädische Chirurgie (DGOOC). Hallux valgus. 2014. https://register.awmf.org/assets/guidelines/033-018l_S2e_Hallux_Valgus_2014-04_abgelaufen_02.pdf
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Rev Esp Cardiol (Engl Ed) 74(9):790–799. https://doi.org/10.1016/j.rec.2021.07.010
da Costa Santos CM, de Mattos Pimenta CA, Nobre MR (2007) The PICO strategy for the research question construction and evidence search. Rev Lat Am Enfermagem 15(3):508–511. https://doi.org/10.1590/s0104-11692007000300023
Wright JG, Swiontkowski MF, Heckman JD (2003) Introducing levels of evidence to the journal. J Bone Joint Surg Am 85(1):1–3 (not available)
Sterne JAC, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I et al (2019) RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366:l4898. https://doi.org/10.1136/bmj.l4898
Wells GA, Wells G, Shea B, Shea B, O'Connell D, Peterson J, et al., editors. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses2014.
Luo D, Wan X, Liu J, Tong T (2018) Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res 27(6):1785–1805. https://doi.org/10.1177/0962280216669183
Shi J, Luo D, Weng H, Zeng XT, Lin L, Chu H et al (2020) Optimally estimating the sample standard deviation from the five-number summary. Res Synth Methods 11(5):641–654. https://doi.org/10.1002/jrsm.1429
Avcu B, Akalin Y, Cevik N, Öztürk A, Sahin N, Öztas S et al (2017) Scarf osteotomy or Mau osteotomy for correction of moderate to severe hallux valgus deformity: a prospective, randomized study. Eur Res J 4(1):6–15. https://doi.org/10.18621/eurj.302186
Biz C, Fosser M, Dalmau-Pastor M, Corradin M, Roda MG, Aldegheri R et al (2016) Functional and radiographic outcomes of hallux valgus correction by mini-invasive surgery with Reverdin-Isham and Akin percutaneous osteotomies: a longitudinal prospective study with a 48-month follow-up. J Orthop Surg Res 11(1):157. https://doi.org/10.1186/s13018-016-0491-x
Boychenko AV, Solomin LN, Belokrylova MS, Tyulkin EO, Davidov DV, Krutko DM (2019) Hallux valgus correction with rotational scarf combined with adductor Hallucis tendon transposition. J Foot Ankle Surg 58(1):34–37. https://doi.org/10.1053/j.jfas.2018.07.012
Buciuto R (2014) Prospective randomized study of chevron osteotomy versus Mitchell’s osteotomy in hallux valgus. Foot Ankle Int 35(12):1268–1276. https://doi.org/10.1177/1071100714550647
Choi JY, Kim BH, Suh JS (2021) A prospective study to compare the operative outcomes of minimally invasive proximal and distal chevron metatarsal osteotomy for moderate-to-severe hallux valgus deformity. Int Orthop 45(11):2933–2943. https://doi.org/10.1007/s00264-021-05106-1
Di Giorgio L, Sodano L, Touloupakis G, De Meo D, Marcellini L (2016) Reverdin-Isham osteotomy versus Endolog system for correction of moderate hallux valgus deformity: a randomized controlled trial. Clin Ter 167(6):e150–e154. https://doi.org/10.7417/CT.2016.1960
Dragosloveanu S, Popov VM, Cotor DC, Dragosloveanu C, Stoica CI (2022) Percutaneous chevron osteotomy: a prospective randomized controlled trial. Medicina (Kaunas). https://doi.org/10.3390/medicina58030359
Elshazly O, Abdel Rahman AF, Fahmy H, Sobhy MH, Abdelhadi W (2019) Scarf versus long chevron osteotomies for the treatment of hallux valgus: a prospective randomized controlled study. Foot Ankle Surg 25(4):469–477. https://doi.org/10.1016/j.fas.2018.02.017
Faber FW, Mulder PG, Verhaar JA (2004) Role of first ray hypermobility in the outcome of the Hohmann and the Lapidus procedure. A prospective, randomized trial involving one hundred and one feet. J Bone Joint Surg Am 86(3):486–495. https://doi.org/10.2106/00004623-200403000-00005
Faber FW, van Kampen PM, Bloembergen MW (2013) Long-term results of the Hohmann and Lapidus procedure for the correction of hallux valgus: a prospective, randomised trial with eight- to 11-year follow-up involving 101 feet. Bone Joint J 95-B(9):1222–1226. https://doi.org/10.1302/0301-620X.95B9.31560
Frigg A, Zaugg S, Maquieira G, Pellegrino A (2019) Stiffness and range of motion after minimally invasive chevron-akin and open scarf-akin procedures. Foot Ankle Int 40(5):515–525. https://doi.org/10.1177/1071100718818577
Giannini S, Cavallo M, Faldini C, Luciani D, Vannini F (2013) The SERI distal metatarsal osteotomy and Scarf osteotomy provide similar correction of hallux valgus. Clin Orthop Relat Res 471(7):2305–2311. https://doi.org/10.1007/s11999-013-2912-z
Glazebrook M, Copithorne P, Boyd G, Daniels T, Lalonde KA, Francis P et al (2014) Proximal opening wedge osteotomy with wedge-plate fixation compared with proximal chevron osteotomy for the treatment of hallux valgus: a prospective, randomized study. J Bone Joint Surg Am 96(19):1585–1592. https://doi.org/10.2106/JBJS.M.00231
Gutteck N, Wohlrab D, Zeh A, Radetzki F, Delank KS, Lebek S (2013) Comparative study of Lapidus bunionectomy using different osteosynthesis methods. Foot Ankle Surg 19(4):218–221. https://doi.org/10.1016/j.fas.2013.05.002
Hofstaetter SG, Schuh R, Trieb K, Trnka HJ (2012) Modified chevron osteotomy with lateral release and screw fixation for treatment of severe hallux deformity. Z Orthop Unfall 150(6):594–600. https://doi.org/10.1055/s-0032-1327933
Jeuken RM, Schotanus MG, Kort NP, Deenik A, Jong B, Hendrickx RP (2016) Long-term follow-up of a randomized controlled trial comparing scarf to chevron osteotomy in hallux valgus correction. Foot Ankle Int 37(7):687–695. https://doi.org/10.1177/1071100716639574
Jowett CRJ, Bedi HS (2017) Preliminary results and learning curve of the minimally invasive chevron akin operation for hallux valgus. J Foot Ankle Surg 56(3):445–452. https://doi.org/10.1053/j.jfas.2017.01.002
Kaufmann G, Dammerer D, Heyenbrock F, Braito M, Moertlbauer L, Liebensteiner M (2019) Minimally invasive versus open chevron osteotomy for hallux valgus correction: a randomized controlled trial. Int Orthop 43(2):343–350. https://doi.org/10.1007/s00264-018-4006-8
Kaufmann G, Mortlbauer L, Hofer-Picout P, Dammerer D, Ban M, Liebensteiner M (2020) Five-year follow-up of minimally invasive distal metatarsal chevron osteotomy in comparison with the open technique: a randomized controlled trial. J Bone Joint Surg Am 102(10):873–879. https://doi.org/10.2106/JBJS.19.00981
Kaufmann G, Weiskopf D, Liebensteiner M, Ulmer H, Braito M, Endstrasser F et al (2021) Midterm results following minimally invasive distal chevron osteotomy: comparison with the minimally invasive reverdin-isham osteotomy by means of meta-analysis. In Vivo 35(4):2187–2196. https://doi.org/10.21873/invivo.12490
Kiyak G, Esemenli T (2019) Should we use intermetatarsal angle as primary determinant to define the limits of distal chevron osteotomy? J Foot Ankle Surg 58(5):880–885. https://doi.org/10.1053/j.jfas.2018.12.031
Klemola T, Leppilahti J, Laine V, Pentikainen I, Ojala R, Ohtonen P et al (2017) Effect of first tarsometatarsal joint derotational arthrodesis on first ray dynamic stability compared to distal chevron osteotomy. Foot Ankle Int 38(8):847–854. https://doi.org/10.1177/1071100717706153
Lamo-Espinosa JM, Flórez B, Villas C, Pons-Villanueva J, Bondía JM, Aquerreta JD et al (2015) The relationship between the sesamoid complex and the first metatarsal after hallux valgus surgery without lateral soft-tissue release: a prospective study. J Foot Ankle Surg 54(6):1111–1115. https://doi.org/10.1053/j.jfas.2015.07.022
Lechler P, Feldmann C, Köck FX, Schaumburger J, Grifka J, Handel M (2012) Clinical outcome after Chevron-Akin double osteotomy versus isolated Chevron procedure: a prospective matched group analysis. Arch Orthop Trauma Surg 132(1):9–13. https://doi.org/10.1007/s00402-011-1385-3
Lee KB, Cho NY, Park HW, Seon JK, Lee SH (2015) A comparison of proximal and distal Chevron osteotomy, both with lateral soft-tissue release, for moderate to severe hallux valgus in patients undergoing simultaneous bilateral correction: a prospective randomised controlled trial. Bone Joint J-B 97(2):202–207. https://doi.org/10.1302/0301-620X.97B2.34449
Lee M, Walsh J, Smith MM, Ling J, Wines A, Lam P (2017) Hallux valgus correction comparing percutaneous chevron/akin (PECA) and open scarf/akin osteotomies. Foot Ankle Int 38(8):838–846. https://doi.org/10.1177/1071100717704941
Ling SKK, Wu YM, Li C, Lui TH, Yung PS (2020) Randomised control trial on the optimal duration of non-weight-bearing walking after hallux valgus surgery. J Orthop Translat 23:61–66. https://doi.org/10.1016/j.jot.2020.04.009
Loh B, Chen JY, Yew AK, Chong HC, Yeo MG, Tao P et al (2015) Prevalence of metatarsus adductus in symptomatic hallux valgus and its influence on functional outcome. Foot Ankle Int 36(11):1316–1321. https://doi.org/10.1177/1071100715595618
Mahadevan D, Lines S, Hepple S, Winson I, Harries W (2016) Extended plantar limb (modified) chevron osteotomy versus scarf osteotomy for hallux valgus correction: a randomised controlled trial. Foot Ankle Surg 22(2):109–113. https://doi.org/10.1016/j.fas.2015.05.012
Matricali GA, Vermeersch G, Busschots E, Fieuws S, Deschamps K (2014) Prospective randomized comparative study on V-Y and pants-over-vest capsulorraphy in chevron and scarf osteotomy. Acta Orthop Belg 80(2):280–287
Milczarek M, Nowak K, Tomasik B, Milczarek J, Laganowski P, Domzalski M (2021) Additional akin proximal phalanx procedure has a limited effect on the outcome of scarf osteotomy for hallux valgus surgery. J Am Podiatr Med Assoc. https://doi.org/10.7547/20-071
Mosca M, Russo A, Caravelli S, Massimi S, Vocale E, Grassi A et al (2021) Piezoelectric tools versus traditional oscillating saw for distal linear osteotomy in hallux valgus correction: triple-blinded, randomized controlled study. Foot Ankle Surg. https://doi.org/10.1016/j.fas.2021.03.024
Palmanovich E, Ohana N, David S, Small I, Hetsroni I, Amar E et al (2021) Distal chevron osteotomy vs the simple, effective, rapid, inexpensive technique (SERI) for mild to moderate isolated hallux valgus: a randomized controlled study. Indian J Orthop 55(Suppl 1):110–118. https://doi.org/10.1007/s43465-020-00209-0
Park HW, Lee KB, Chung JY, Kim MS (2013) Comparison of outcomes between proximal and distal chevron osteotomy, both with supplementary lateral soft-tissue release, for severe hallux valgus deformity: a prospective randomised controlled trial. Bone Joint J 95-B(4):510–516. https://doi.org/10.1302/0301-620X.95B4.30464
Park YB, Lee KB, Kim SK, Seon JK, Lee JY (2013) Comparison of distal soft-tissue procedures combined with a distal chevron osteotomy for moderate to severe hallux valgus: first web-space versus transarticular approach. J Bone Joint Surg Am 95(21):e158. https://doi.org/10.2106/JBJS.L.01017
Patel S, Garg P, Fazal MA, Shahid MS, Park DH, Ray PS (2019) A comparison of two designs of postoperative shoe on function, satisfaction, and back pain after hallux valgus surgery. Foot Ankle Spec 12(3):228–232. https://doi.org/10.1177/1938640018782608
Pentikainen I, Ojala R, Ohtonen P, Piippo J, Leppilahti J (2014) Preoperative radiological factors correlated to long-term recurrence of hallux valgus following distal chevron osteotomy. Foot Ankle Int 35(12):1262–1267. https://doi.org/10.1177/1071100714548703
Pentikainen I, Piippo J, Ohtonen P, Junila J, Leppilahti J (2015) Role of fixation and postoperative regimens in the long-term outcomes of distal chevron osteotomy: a randomized controlled two-by-two factorial trial of 100 patients. J Foot Ankle Surg 54(3):356–360. https://doi.org/10.1053/j.jfas.2014.08.001
Puchner SE, Trnka HJ, Willegger M, Staats K, Holinka J, Windhager R et al (2018) Comparison of plantar pressure distribution and functional outcome after scarf and Austin osteotomy. Orthop Surg 10(3):255–263. https://doi.org/10.1111/os.12400
Radwan YA, Mansour AM (2012) Percutaneous distal metatarsal osteotomy versus distal chevron osteotomy for correction of mild-to-moderate hallux valgus deformity. Arch Orthop Trauma Surg 132(11):1539–1546. https://doi.org/10.1007/s00402-012-1585-5
Sahin N, Cansabuncu G, Cevik N, Turker O, Ozkaya G, Ozkan Y (2018) A randomized comparison of the proximal crescentic osteotomy and rotational scarf osteotomy in the treatment of hallux valgus. Acta Orthop Traumatol Turc 52(4):261–266. https://doi.org/10.1016/j.aott.2018.02.008
Saxena A, St Louis M (2013) Medial locking plate versus screw fixation for fixation of the Ludloff osteotomy. J Foot Ankle Surg 52(2):153–157. https://doi.org/10.1053/j.jfas.2012.11.005
Torrent J, Baduell A, Vega J, Malagelada F, Luna R, Rabat E (2021) Open vs minimally invasive scarf osteotomy for hallux valgus correction: a randomized controlled trial. Foot Ankle Int 42(8):982–993. https://doi.org/10.1177/10711007211003565
Uygur E, Ozkan NK, Akan K, Cift H (2016) A comparison of Chevron and Lindgren-Turan osteotomy techniques in hallux valgus surgery: a prospective randomized controlled study. Acta Orthop Traumatol Turc 50(3):255–261. https://doi.org/10.3944/AOTT.2016.14.0272
Wester JU, Hamborg-Petersen E, Herold N, Hansen PB, Froekjaer J (2016) Open wedge metatarsal osteotomy versus crescentic osteotomy to correct severe hallux valgus deformity—a prospective comparative study. Foot Ankle Surg 22(1):26–31. https://doi.org/10.1016/j.fas.2015.04.006
Windhagen H, Radtke K, Weizbauer A, Diekmann J, Noll Y, Kreimeyer U et al (2013) Biodegradable magnesium-based screw clinically equivalent to titanium screw in hallux valgus surgery: short term results of the first prospective, randomized, controlled clinical pilot study. BioMed Central. https://doi.org/10.1186/1475-925X-12-62
Chan HY, Chen JY, Zainul-Abidin S, Ying H, Koo K, Rikhraj IS (2017) Minimal clinically important differences for american orthopaedic foot & ankle society score in hallux valgus surgery. Foot Ankle Int 38(5):551–557. https://doi.org/10.1177/1071100716688724
Dietze A, Bahlke U, Martin H, Mittlmeier T (2013) First ray instability in hallux valgus deformity: a radiokinematic and pedobarographic analysis. Foot Ankle Int 34(1):124–130. https://doi.org/10.1177/1071100712460217
Klaue K, Hansen ST, Masquelet AC (1994) Clinical, quantitative assessment of first tarsometatarsal mobility in the sagittal plane and its relation to hallux valgus deformity. Foot Ankle Int 15(1):9–13. https://doi.org/10.1177/107110079401500103
de Cesar NC, Ehret A, Walt J, Chinelati RMK, Dibbern K, de Carvalho KAM et al (2023) Early results and complication rate of the LapiCotton procedure in the treatment of medial longitudinal arch collapse: a prospective cohort study. Arch Orthop Trauma Surg 143(5):2283–2295. https://doi.org/10.1007/s00402-022-04399-0
Ferreira GF, Nunes GA, Banca V, Michaelis LF, Lewis TL, Ray R et al (2024) Minimally invasive hallux valgus surgery using 3D printed patient specific instrumentation. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-024-05383-6
Palmanovich E, Ohana N, Tavdi A, Atzmon R, Feldman V, Brin YS et al (2023) A modified minimally invasive osteotomy for hallux valgus enables reduction of malpositioned sesamoid bones. Arch Orthop Trauma Surg 143(10):6105–6112. https://doi.org/10.1007/s00402-023-04868-0
Ji L, Wang K, Ding S, Sun C, Sun S, Zhang M (2022) Minimally invasive vs. open surgery for hallux valgus: a meta-analysis. Front Surg 9:843410. https://doi.org/10.3389/fsurg.2022.843410
Day J, de Cesar NC, Burssens A, Bernasconi A, Fernando C, Lintz F (2022) A case-control study of 3D vs 2D weightbearing CT measurements of the M1–M2 intermetatarsal angle in hallux valgus. Foot Ankle Int 43(8):1049–1052. https://doi.org/10.1177/10711007221091812
Mahmoud K, Metikala S, Mehta SD, Fryhofer GW, Farber DC, Prat D (2021) The role of weightbearing computed tomography scan in hallux valgus. Foot Ankle Int 42(3):287–293. https://doi.org/10.1177/1071100720962398
Montiel V, Valenti A, Villas C, Valverde C, Alfonso M (2022) Hallux anatomy: much ado about shoes-an attempt to prove that constrictive V-shaped toe-box shoes deform the hallux. Arch Orthop Trauma Surg 142(8):1793–1800. https://doi.org/10.1007/s00402-021-03792-5
Tejero S, Gonzalez-Martin D, Martinez-Franco A, Jimenez-Diaz F, Gijon-Nogueron G, Herrera-Perez M (2023) Intraoperative checking of the first ray rotation and sesamoid position through sonographic assistance. Arch Orthop Trauma Surg 143(4):1915–1922. https://doi.org/10.1007/s00402-022-04359-8
Iyer S, Demetracopoulos CA, Sofka CM, Ellis SJ (2015) High rate of recurrence following proximal medial opening wedge osteotomy for correction of moderate hallux valgus. Foot Ankle Int 36(7):756–763. https://doi.org/10.1177/1071100715577195
Lewis TL, Mason L, Gordon D, Ray R (2022) The Clavien-Dindo complication classification modified for foot and ankle orthopaedic surgery. Foot Ankle Surg 28(6):800–802. https://doi.org/10.1016/j.fas.2022.03.006
Acknowledgements
D.A.F. Scientific Committee: Prof. Dr. Christina Stukenborg-Colsman, MD (christina.stukenborg@diakovere.de), Prof. Dr. Sabine Ochman, MD (sabine.ochman@ukmuenster.de), Prof. Dr. Stefan Rammelt, MD (Stefan.rammelt@uniklinikum-dresden.de), Prof. Dr. Hans Polzer, MD (hans.polzer@med.uni-muenchen.de), Prof. Dr. Natalia Gutteck, MD (natalia.gutteck@uk-halle.de), PD Dr. Norbert Harrasser, MD (norbert.harrasser@atos.de), PD Dr. Christian Plaaß, MD (Christian.plaass@diakovere.de).
Funding
Open Access funding enabled and organized by Projekt DEAL. The study was funded by a D.A.F. research grant of 10.000 Euro.
Author information
Authors and Affiliations
Consortia
Contributions
The study idea, i.e. a living systematic review as scientific basis for the German hallux valgus guidelines, was consented in the whole study group, alongside with the final approval of the paper. ES, SM, BSF were responsible for the study design and conception. ES was responsible for the manuscript preparation. SFT and BSF conducted the systematic review and data extraction. SM performed the statistical analysis. The whole study group participated in the data interpretation. BSF was responsible for finalizing the paper.
Corresponding author
Ethics declarations
Conflict of interest
All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/disclosure-of-interest/ and declare: all authors had financial support from a D.A.F. research grant for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval
Not applicable.
Copyright/license for publication
Granted.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The members of the instutional author group “D.A.F. Scientific Committee” was processed under acknowledgements section.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ettinger, S., Spindler, F.T., Savli, M. et al. Correction potential and outcome of various surgical procedures for hallux valgus surgery: a living systematic review and meta-analysis. Arch Orthop Trauma Surg (2024). https://doi.org/10.1007/s00402-024-05521-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00402-024-05521-0