
Abstract
Purpose
Whether or not young patients with squamous cell carcinoma of oral cavity (OC-SCC) have a difference in prognosis remains a controversy. This study aimed to analyze the clinical characteristics and difference of survival rates between adult patients less than 40 years of age and those 40 years of age and older.
Methods
A retrospective analysis was conducted using the database of patients diagnosed with OC-SCC between 1990 and 2013 in the Sun Yat-sen University Cancer Center, but patients older than 85 years, younger than 18 years, or died within 6 months of diagnosis were excluded. Patients were categorized into two groups: the young group (< 40 years of age) and the older group (≥ 40 years of age). Cox regression, survival and subgroups analyses were performed. The primary endpoints included the rates of 5-year overall survival (OS) and disease-specific survival (DSS).
Results
A total of 1902 OC-SCC patients were identified. The percentage of female in the young group was significantly higher than that in the older group (40.27% vs 31.03%, p < 0.001). This study failed to find the difference in TNM classification or tumor stage between the two groups (p > 0.05). The young group was more likely to receive adjuvant radiotherapy and/or chemotherapy (42.48% vs 26.91%, p < 0.001). The 5-year OS rate (71% vs. 57%, p < 0.001) and DSS rate (72% vs 58%, p < 0.001) in patients under 40 years were significantly higher than those for the older group.
Conclusion
Our findings suggested that OC-SCC in younger patients did not present at a more advanced stage. In addition, young age is an independent predictor for better survival.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Oral cavity cancer (OCC), which anatomically involves the lips, the front two-thirds of the tongue, the gums, the lining inside the cheeks and lips, the floor (bottom) of the mouth under the tongue, the hard palate (bony top of the mouth), and the small area of the gum behind the wisdom teeth [1], is one of the most common subsites of head and neck cancer [2]. Over 90% of cases are squamous cell carcinomas (SCC) [2]. Alcohol and tobacco consumption are considered to be the main risk factors for OCC [4, 5]. Further, OCC was found to be closely related to a high-risk human papillomavirus (HPV) infection [6]. In many parts of Asia, betel quid chewing increases the risk of oral cancer, independently of tobacco and alcohol use [7]. Worldwide, it is estimated that there will be 354,864 new cases of oral cancer and an estimated 177,384 people will die of the disease in 2018, representing close to 2% of cancer deaths. The incidence and mortality rates in men are approximately two times higher than those in women. Notably, OCC tends to cluster in South Asia [7]. In the United States, the incidence rate is highest in individuals aged 55–64 years, with a median age of 63 years. Data estimates from the US for the years 2009–2015 showed that the number of surviving patients of oral cavity and pharynx cancer at 5 years is 65.3%. Most patients (93.4%) are diagnosed at age 45 and above [9]. Traditionally, OCC occurs in the elderly during the 5th through the 7th decades of life; however, it has been reported to be increasing in incidence among younger populations globally, especially in young women [11].
The cause of this increasing trend remains unclear, but we should draw attention to the younger patients. Many published reports have obtained conflicting results. Some studies report that OC-SCC in young patients is more aggressive. Conversely, other studies suggest that younger patients with OC-SCC did not have worse survival. Whether or not the young with OC-SCC have a difference in prognosis remains a controversy. In this single-institution study performed in southern China, we aimed to compare differences in survival between patients aged younger than 40 years and those who were 40 years and older.
Materials and methods
The study was conducted in Sun Yat-sen University Cancer Center (SYSUCC). The medical files, containing a total of 1902 patients who were treated primarily by surgical resection and histologically confirmed in our center from 1990 to 2013, were retrospectively reviewed. All the patients were followed for a minimum of 5 years. Patients were divided into two groups depending on age (patients < 40 years and patients ≥ 40 years). Demographics (age and sex), year of diagnosis (1990–1999, 2000–2009, 2010–2013), habits (alcohol and tobacco use), TNM classification, tumor stage (followed the AJCC Cancer Staging Manual, Seventh Edition), treatment (surgery, chemotherapy, radiotherapy), and survival outcomes were documented (see Table 1), and these factors were compared between patients younger than 40 years and the older patients. P < 0.01 was considered to be statistically significant. For statistical analyses, we used SPSS, version 16.0 software (SPSS Inc., Chicago, IL, USA).
Results
A total of 1902 patients comprised the study cohort. Those who were older than 85 years, younger than 18 years, or died within 6 months of diagnosis were excluded. The clinicopathologic characteristics of the two groups are presented in Table 1. Among these patients, 226 (11.88%) were less than 40 years of age (young group). Overall, the average patient age was 54.6 ± 12.2 years and 33.5 ± 4.7 years in the young group and 57.5 ± 9.9 years in the older group. In the young group, the morbidity rate of females was significantly higher than that in the older group (40.27% vs. 31.03%). The tongue was the most common primary site (64.04%), followed by other parts of the mouth. The tongue SCC in young patients appeared to be more common than in the older group (87.61% vs. 60.83%, p < 0.001). No statistical differences were found between the two groups with regard to tobacco and/or alcohol use. There was no significant difference between the groups concerning TNM classification or tumor stage. Interestingly, compared with the older group, the young group was less likely to undergo surgery alone (94, 41.59% vs. 934, 55.73%, p < 0.001). Young patients tended to receive postoperative adjuvant radiotherapy (RT) and/or chemotherapy (CT) compared with the older group (96, 42.48% vs. 451, 26.91%, p < 0.001).
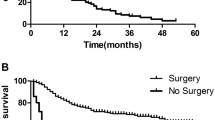
The minimum duration of follow-up time was 5 years. Of 1902 patients, the 5-year overall survival (OS) rate was 59% [95% confidence interval (CI) 56.8–61.2%] and the 5-year disease-specific survival (DSS) rate was 60% (95% CI 57.8–62.2%). The 5-year OS rate was 71% (95% CI 68.0–77.0%) in the young group and 57% (95% CI 54.6–59.4%) in the older group. The 5-year DSS rate was 72% (95% CI 67.0–78.0%) in the young group and 58% (95% CI 55.6–60.4%) in the older group. The OS and DSS between the two groups were compared with Kaplan–Meier plot. The results indicated that there were significant differences between the two groups. Figures 1 and 2 show that both OS and DSS in younger patients with OC-SCC are better than in older patients.

Kaplan–Meier estimate of overall survival between the age groups

Kaplan–Meier estimate of disease-specific survival between the age groups
The univariate and multivariable Cox proportional hazards model for DSS were performed (Table 2). Older age was a significant predictor of worse prognosis at all stages. In addition, other clinically significant worse predictors of DSS in both univariate and multivariable regression included male sex, tumor site (other part of mouth), higher TNM classification, worse tumor stage, and treatment with RT/CT.
The DSS in the young group was consistently favorable [all hazard ratios (HR) except distant metastases M1] across all subgroups (Fig. 3).

Subgroup analyses
Discussion
In many types of cancer, age at diagnosis is viewed as an independent predictor of outcome [11]. In the field of OC-SCC, there is no uniform category of “young” patients and previous analyses were performed using age thresholds ranging from 30 to 45 years of age [12,13,14,15,16,17,18,19]. It is difficult to determine a reasonable cutoff between “young” and “old” adults. Because 40 years of age was used as an age threshold in most of the previous studies, it is reasonable that for our study, a young adult is defined as someone less than 40 years of age. The inconsistent cutoff age for young patients has contributed to the conflicting findings in the literature. Therefore, there is a need for studies to use a standard division.
A review of the reported studies demonstrates that our clinical characteristic findings are in agreement with several previously published large cohort studies [12,13,14,15,16,17,18,19]. First, OC-SCC mainly occurs in men between the 5th and 6th decades of life. Second, the young group exhibited a higher proportion of women compared with adults 40 years and older (40.27% vs. 31.03%, respectively). The findings should heighten the awareness of the occurrence of OC-SCC in young women and merits further investigation. Third, lymph node (28.76%) and distant (0.37%) metastases are not unusual and a majority of patients had early stage disease (Stage I–II, 50.68%). Furthermore, more than half of patients (54.05%) were treated with surgery alone, as surgical treatment is the main treatment method. In the young group, patients were more likely to receive adjuvant RT and/or CT (42.48% vs. 26.91%, p < 0.01). In the findings on site predilection was generally consistent with the previous OC-SCC literature [3, 22, 23]. The young group was more likely to have tongue cancer (87.61% vs. 60.83%, p < 0.01).
Several similar studies have analyzed survival of patients with early-onset OC-SCC (Table 3). More population-based studies with large samples are needed, especially performed in non-western regions to estimate the outcome of OC-SCC in young groups of patients. In this study, it is notable that 11.88% of patients were diagnosed before age of 40 years, a higher rate than that in most studies, particularly those studies from the US and Europe [20, 24,25,26]. Considering that cancers of the oral cavity are highly frequent in southern Asia, the higher proportion in young people might indicate that the sociocultural lifestyle of the population, such as betel quid chewing and the use of tobacco and alcohol, plays an important role in this geographic or regional diversity [27]. In our study, the percentage of patients with early stage (Stage I–II, 50.68%) was lower than in western developed countries [20], but higher than other southern Asian regions (e.g., India, Thailand, Taiwan, and Japan) [11, 14, 17, 19, 28,29,30]. It is suggested that low socioeconomic status or related patient factors (e.g., education, diet, health care, and living conditions) may increase the risk of OC-SCC. A significant difference in survival rates was found among young people between affluent and non-affluent groups [31]. A deeper knowledge of the public on OC-SCC could help avoid exposing people to the risk factors. This means we need to do more to raise awareness by identifying people at risk and taking measures to allow early detection and minimize the undesirable consequences of OC-SCC [32].
Historically, numerous previous reports on this topic found that the biologic behavior of OC-SCC in younger patients was more aggressive compared with that in elderly patients [13, 34]. It has been reported that OC-SCC in young patients had a significantly higher rate of nodal metastases, which resulted in a more advanced tumor stage [20, 34, 35]. In clinicopathologic features, some studies have shown OC-SCC in young patients had a more advanced TNM classification and higher proportion of poorly differentiated tumors [36, 37]. However, reviewing the most recent studies, the treatment outcomes of the young group are heterogeneous and it is possible to confirm that younger patients may have similar or better outcomes than older patients [18, 20, 26, 38,39,40,41,42,43,44]. In our cohort, histopathologic variables, such as tumor TNM, did not show any significant differences between young and old patients. And, it was not possible to confirm a higher rate of nodal metastases. Therefore, it was no surprise that no difference was found in tumor stage between the two groups (p = 0.677). Interestingly, treatment comparisons showed that the younger patients were more likely to receive postoperative adjuvant RT and/or CT, a more aggressive approach than older patients. RT, generally recommended as an adjuvant treatment in head and neck cancers, is preferred for those with evidence of adverse features or advanced stage. For the patients involved in our study, CT alone is not recommended as a postoperative adjuvant therapy without RT. However, in rare cases, personal reasons, for example, misconceptions in irradiation, economic problem and rejection of so many times of radiotherapy fractions, could explain that they underwent CT alone as an adjuvant therapy without RT. It is unclear why young patients undergo intensification. A possible reason is that the young patients were more tolerant to adjuvant therapy than the old group and practitioners probably think young patients could benefit from treatment intensification despite there being no clear indication for adjuvant therapy.
The 5-year OS was 59% and the 5-year DSS rate was 60%. The 5-year OS was 71% in the young group and 57% in the older group. The 5-year DSS was 72% in the young group and 58% in the older group. The higher OS and DSS in young patients showed a significant prognostic advantage in younger patients. In both univariate and multivariable analyses, older age, advanced TNM stage, surgery with RT and/or CT, and RT and/or CT were associated with worse prognosis. In DSS subgroup analyses, the results of the better survival of the young group, as compared with the older group, were that treatment outcome was consistently favorable across all patient subgroups (except distant metastases M1). In clinical practice, age, stage, and site are the most important determinants of treatment selection for patients with OC-SCC [45]. However, these outcome data of the present study suggest that young age alone should not alter treatment.
There are limitations to our study. First, it was conducted at a single institution. Another limitation is lack of matched controls and recurrence or clinicopathologic data (e.g., tumor grade, extracapsular extension, margins, and number of examined lymph nodes). However, despite these limitations, our study is one of the largest studies from a high-risk region of OC-SCC, including the high quality of the data, which enabled us to control for multiple factors and minimize error and bias.
Conclusion
OC-SCC in young adults represents a rare disease, with an increasing incidence, particularly in females. Comparison by age group showed no differences in rates of advanced TNM stage. But young adults are more commonly treated with adjuvant RT and/or CT. Our findings have evidenced that young age at diagnosis is an independent predictor of better survival. Thus, a comprehensive tailoring of treatment on a case-by-case basis according to current guidelines is recommended.
References
Rodríguez-Santamarta T, Rodrigo JP, García-Pedrero JM et al (2016) Prevalence of human papillomavirus in oral squamous cell carcinomas in northern Spain. Eur Arch Otorhinolaryngol 273(12):4549–4559
de Castro JG, Dos SA, Aparecida DAKF et al (2016) Tongue cancer in the young[J]. Curr Opin Oncol 28(3):193–194
Chi AC, Day TA, Neville BW (2015) Oral cavity and oropharyngeal squamous cell carcinoma–an update[J]. CA Cancer J Clin 65(5):401–421
Sankaranarayanan R, Ramadas K, Thara S et al (2013) Long term effect of visual screening on oral cancer incidence and mortality in a randomized trial in Kerala, India[J]. Oral Oncol 49(4):314–321
Chaturvedi P, Singh A, Chien CY et al (2019) Tobacco related oral cancer[J]. BMJ 365:l2142
Hubbers CU, Akgul B (2015) HPV and cancer of the oral cavity[J]. Virulence 6(3):244–248
Guha N, Warnakulasuriya S, Vlaanderen J et al (2014) Betel quid chewing and the risk of oral and oropharyngeal cancers: a meta-analysis with implications for cancer control[J]. Int J Cancer 135(6):1433–1443
Bray F, Ferlay J, Soerjomataram I et al (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin 68(6):394–424
SEER Cancer Stat Facts: oral cavity and pharynx cancer. National Cancer Institute. Bethesda, MD, https://seer.cancer.gov/statfacts/html/oralcav.html.
Patel SC, Carpenter WR, Tyree S et al (2011) Increasing incidence of oral tongue squamous cell carcinoma in young white women, age 18 to 44 years[J]. J Clin Oncol 29(11):1488–1494
Mahmood N, Hanif M, Ahmed A et al (2018) Impact of age at diagnosis on clinicopathological outcomes of oral squamous cell carcinoma patients[J]. Pak J Med Sci 34(3):595–599
Garavello W, Spreafico R, Gaini RM (2007) Oral tongue cancer in young patients: a matched analysis[J]. Oral Oncol 43(9):894–897
Soudry E, Preis M, Hod R et al (2010) Squamous cell carcinoma of the oral tongue in patients younger than 30 years: clinicopathologic features and outcome[J]. Clin Otolaryngol 35(4):307–312
Komolmalai N, Chuachamsai S, Tantiwipawin S et al (2015) Ten-year analysis of oral cancer focusing on young people in northern Thailand[J]. J Oral Sci 57(4):327–334
Sun Q, Fang Q, Guo S (2015) A comparison of oral squamous cell carcinoma between young and old patients in a single medical center in China[J]. Int J Clin Exp Med 8(8):12418–12423
Cariati P, Cabello-Serrano A, Perez-De PM et al (2017) Oral and oropharyngeal squamous cell carcinoma in young adults: a retrospective study in Granada University Hospital[J]. Med Oral Patol Oral Cir Bucal 22(6):e679–e685
Iamaroon A, Pattanaporn K, Pongsiriwet S et al (2004) Analysis of 587 cases of oral squamous cell carcinoma in northern Thailand with a focus on young people[J]. Int J Oral Maxillofac Surg 33(1):84–88
Macek MD (2010) Younger adults with oral cavity squamous cell cancer have a significantly higher 5-year survival rate than do older adults in the united states, controlling for patient- and disease-specific characteristics[J]. J Evid Based Dent Pract 10(3):158–159
Iype EM, Pandey M, Mathew A et al (2001) Oral cancer among patients under the age of 35 years[J]. J Postgrad Med 47(3):171–176
Oliver JR, Wu SP, Chang CM et al (2019) Survival of oral tongue squamous cell carcinoma in young adults[J]. Head Neck 41(9):2960–2968
Gamez ME, Kraus R, Hinni ML et al (2018) Treatment outcomes of squamous cell carcinoma of the oral cavity in young adults[J]. Oral Oncol 87:43–48
Manuel S, Raghavan SK, Pandey M et al (2003) Survival in patients under 45 years with squamous cell carcinoma of the oral tongue[J]. Int J Oral Maxillofac Surg 32(2):167–173
Ibayashi H, Pham TM, Fujino Y et al (2011) Estimation of premature mortality from oral cancer in Japan, 1995 and 2005[J]. Cancer Epidemiol 35(4):342–344
Pabiszczak MS, Wasniewska E, Mielcarek-Kuchta D et al (2013) Variable course of progression of oral cavity and oropharyngeal carcinoma in young adults[J]. Contemp Oncol (Pozn) 17(3):286–290
van Monsjou HS, Lopez-Yurda MI, Hauptmann M et al (2013) Oral and oropharyngeal squamous cell carcinoma in young patients: the Netherlands Cancer Institute experience[J]. Head Neck 35(1):94–102
Udeabor SE, Rana M, Wegener G et al (2012) Squamous cell carcinoma of the oral cavity and the oropharynx in patients less than 40 years of age: a 20-year analysis[J]. Head Neck Oncol 4:28
Krishna RS, Mejia G, Roberts-Thomson K et al (2013) Epidemiology of oral cancer in Asia in the past decade: an update (2000–2012) [J]. Asian Pac J Cancer Prev 14(10):5567–5577
Mathew IE, Pandey M, Mathew A et al (2001) Squamous cell carcinoma of the tongue among young Indian adults[J]. Neoplasia 3(4):273–277
Huang CC, Ou CY, Lee WT et al (2015) Life expectancy and expected years of life lost to oral cancer in Taiwan: a nation-wide analysis of 22,024 cases followed for 10 years[J]. Oral Oncol 51(4):349–354
Yamamoto N, Sato K, Yamauchi T et al (2013) A 5-year activity report from the Oral Cancer Center, Tokyo Dental College[J]. Bull Tokyo Dent Coll 54(4):265–273
Warnakulasuriya S, Mak V, Moller H (2007) Oral cancer survival in young people in South East England[J]. Oral Oncol 43(10):982–986
de Camargo CM, Voti L, Guerra-Yi M et al (2010) Oral cavity cancer in developed and in developing countries: population-based incidence[J]. Head Neck 32(3):357–367
Liao CT, Wang HM, Hsieh LL et al (2006) Higher distant failure in young age tongue cancer patients[J]. Oral Oncol 42(7):718–725
Funk GF, Karnell LH, Robinson RA et al (2002) Presentation, treatment, and outcome of oral cavity cancer: a National Cancer Data Base report[J]. Head Neck 24(2):165–180
Lacy PD, Piccirillo JF, Merritt MG et al (2000) Head and neck squamous cell carcinoma: better to be young[J]. Otolaryngol Head Neck Surg 122(2):253–258
Zhang YY, Wang DC, Su JZ et al (2017) Clinicopathological characteristics and outcomes of squamous cell carcinoma of the tongue in different age groups[J]. Head Neck 39(11):2276–2282
Jeon JH, Kim MG, Park JY et al (2017) Analysis of the outcome of young age tongue squamous cell carcinoma[J]. Maxillofac Plast Reconstr Surg 39(1):41
Hyam DM, Conway RC, Sathiyaseelan Y et al (2003) Tongue cancer: do patients younger than 40 do worse?[J]. Aust Dent J 48(1):50–54
Friedlander PL, Schantz SP, Shaha AR et al (1998) Squamous cell carcinoma of the tongue in young patients: a matched-pair analysis[J]. Head Neck 20(5):363–368
Pitman KT, Johnson JT, Wagner RL et al (2000) Cancer of the tongue in patients less than forty[J]. Head Neck 22(3):297–302
Davidson BJ, Root WA, Trock BJ (2001) Age and survival from squamous cell carcinoma of the oral tongue. Head Neck 23(4):273–279
Lee CC, Ho HC, Chen HL et al (2007) Squamous cell carcinoma of the oral tongue in young patients: a matched-pair analysis[J]. Acta Otolaryngol 127(11):1214–1217
Fan Y, Zheng L, Mao MH et al (2014) Survival analysis of oral squamous cell carcinoma in a subgroup of young patients[J]. Asian Pac J Cancer Prev 15(20):8887–8891
Goldenberg D, Brooksby C, Hollenbeak CS (2009) Age as a determinant of outcomes for patients with oral cancer[J]. Oral Oncol 45(8):e57–e61
Goldenberg D, Mackley H, Koch W et al (2014) Age and stage as determinants of treatment for oral cavity and oropharyngeal cancers in the elderly[J]. Oral Oncol 50(10):976–982
Funding
Research grants from funding agencies (the National Natural Science Foundation of China, No. 81802713 and No. 81672671).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Sun Yat-sen University Cancer Center ethics committee (GZR2018-188) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, S., Lin, Z., Chen, J. et al. Older age is a risk factor associated with poor prognosis of patients with squamous cell carcinoma of the oral cavity. Eur Arch Otorhinolaryngol 277, 2573–2580 (2020). https://doi.org/10.1007/s00405-020-05963-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-020-05963-3