
Abstract
Familial Mediterranean fever (FMF) is an autosomal recessive autoinflammatory disease, linked to mutations in the MEFV gene. The p.E148Q variant, found on exon 2, has an uncertain role in FMF, with debates on whether it is a benign polymorphism or a pathogenic mutation. This study aimed to assess the clinical characteristics and severity of FMF in patients homozygous for the p.E148Q variant and to evaluate the impact of the p.V726A variant in these patients. This retrospective cohort study analyzed data from electronic medical records at Carmel Medical Center, Israel. Patients who underwent genetic testing for FMF from November 2004 to December 2019 and had p.E148Q/p.E148Q or p.E148Q/p.E148Q + p.V726A variants were included. Disease severity was assessed using the Tel Hashomer Key to Severity Score. Statistical analyses compared clinical characteristics and severity between genotype groups. The study included 61 FMF patients, with 24 (39%) having p.E148Q/p.E148Q and 37 (61%) having p.E148Q/p.E148Q + p.V726A variants. The majority (72%) were Druze. Most patients (65.5%) exhibited mild disease, while 31.1% had moderate disease, with no cases of severe disease. Colchicine treatment significantly reduced CRP levels in all patients.
Conclusion: These findings suggest that the p.E148Q variant, whether alone or with p.V726A, generally results in mild to moderate FMF severity, supporting its pathogenic role in particular ethnicity. These results contribute to understanding the clinical significance of the p.E148Q variant and considering the patient’s need for Colchicine treatment.
What is Known: • The role of the p.E148Q variant in FMF is debated, with questions about whether it is a benign polymorphism or a pathogenic mutation. • The prevalence of MEFV variants can vary significantly among different ethnic groups. | |
What is New: • The p.E148Q variant has clinical significance in particular ethnicities, as supported by a significant reduction in CRP levels following colchicine treatment. • The p.E148Q variant, whether alone or with p.V726A, generally results in mild to moderate FMF severity. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Familial Mediterranean fever (FMF; OMIM 249100) is an inherited autosomal recessive autoinflammatory disease characterized by short, self-limited, and recurrent episodes of high fever accompanied by sterile serositis involving the abdomen, chest, and joints [1]. The disease is particularly common in populations of Turkish, Armenian, Jewish-Sephardic, and Arab descent [2].
The diagnosis of FMF is based on clinical symptoms and supported by genetic testing [3]. However, the absence of an appropriate mutation does not preclude the existence of the disease. Proper and early diagnosis is important because early treatment with colchicine can prevent symptomatic attacks and a late but major complication of the disease—systemic amyloidosis [4].
FMF is caused by mutations in the MEFV gene, found on human chromosome 16. This gene encodes the pyrin protein, which plays an important role in the regulation of the inflammatory response. The mutant pyrin results in the activation of the pyrin inflammasome, leading to an increase in inteleukine-1β (IL-1β) production [5, 6]. To date, 399 sequence variants are reported in the MEFV gene according to the INFEVERS database [7]. The most common pathogenic variants are on exon 10 (p.M680I, p.M694V, p.M694I, and p.V726A). Another common variant is p.E148Q, found on exon 2, where glutamine (Q) substitutes for glutamic acid (E), and is considered the most common homozygous variant in patients of Druze origin [2, 8].
There is considerable FMF genotype–phenotype variability; for instance, the p.M694V mutation is associated with a severe phenotype and the onset of renal AA amyloidosis, while the p.V726A mutation is associated with a milder form of the disease [9, 10].
One of the debated topics in FMF research is whether the p.E148Q variant is a benign polymorphism or a disease-causing mutation. This controversy has significant implications for the diagnosis and management of FMF, as the classification of p.E148Q can influence treatment decisions and genetic counselling. Therefore, the main objective of our study was to evaluate the clinical characteristics and disease severity associated with a homozygous p.E148Q variant in different ethnic groups of Arab origin, including Christians, Muslims, and Druze, in addition to Jewish patients. A secondary goal was to examine the contribution of a single allele of the p.V726A mutation to disease severity in homozygous p.E148Q patients, given the high prevalence of this mutation in our FMF patients, and to assess the impact of a well-known FMF mutation within our cohort.
Methods
Study design and source of data
This retrospective, long-term follow-up cohort study was conducted at Carmel Medical Center in Haifa, affiliated with Clalit Health Services (CHS), the largest healthcare provider in Israel. The study utilized data extracted from the electronic medical records of CHS/Carmel Medical Center.
CHS serves a diverse membership across Israel, encompassing a wide range of geographic locations, ethnicities, and socioeconomic backgrounds. CHS maintains comprehensive electronic medical records that are continuously updated with information from pharmaceutical, medical, and administrative sources.
Ethical approval
The study was approved by the Institutional Review Board of Carmel Medical Center (CMC-0009–20) and conducted in accordance with the Declaration of Helsinki. The requirement for individual patient consent forms was waived by the Institutional Review Board due to the retrospective, observational nature of the de-identified data.
Data collection
Data were extracted from CHS’s electronic medical records, including demographic, laboratory, and clinical information. This encompassed patient age, sex, ethnicity, medical history, disease onset, symptoms, frequency and duration of attacks, laboratory tests such as C-reactive protein (CRP) levels, and colchicine treatment and dosage.
Inclusion criteria
All patients who underwent genetic testing for FMF at the hospital’s genetic institute between November 2004 and December 2019 were eligible for inclusion in the study.
Exclusion criteria
Patients with variants other than p.E148Q/p.E148Q or p.E148Q/p.E148Q + p.V726A, as well as those with missing data or information, were excluded from the study.
Disease severity assessment
Disease severity was assessed using the Tel Hashomer Key to Severity Score [3] for each patient (see Supplementary Table 1).
Genetic analysis
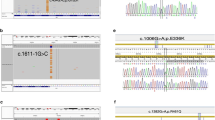
For FMF genotyping, samples were tested for six variants using PRONTO FMF Screen kit (Pronto Diagnostics Ltd, Israel), which is a single-nucleotide primer extension enzyme-linked immunosorbent assay (ELISA) intended for the qualitative, in vitro detection of p.M680I (c.2040 G > C and c.2040 G > A), p.M694V (c.2080 A > G), p.M694I (c.2082 G > A), p.V726A (c.2177 T > C), and p.E148Q (c.442G > C) variants in the MEFV gene from November 2004 until December 2015. NanoChip technology (Savyon Diagnostics Ltd, Israel) was used for FMF genetic testing from January 2016 until the termination of the study. NanoChip technology encompasses an automated platform capable of detecting multiple targets for individual samples and analyzing multiple samples on the same electronic microarray. This method was used for detecting 12 MEFV (NM_000243.2) variants: c.442G > C (p.E148Q) in exon 2, c.1105C > T (p.P369S) in exon 3, and c.1437C > G (p.F479L) in exon 5; as well as the following variants on exon 10: c.2040G > C (p.M680I), c.2040G > A (p.M680I), c.2076_2078del (p.I692del), c.2080A < G (p.M694V), c.2082G > A (p.M694I), c.2084A > G (p.K695R), c.2177T > C (p.V726A), c.2230G > T (p.A744S), and c.2282G > A (p.R761H).
Outcome measures
The primary outcome measure was FMF disease severity as measured by the Tel Hashomer Key to Severity Score among patients homozygous for the p.E148Q variant. The secondary outcome was to compare the severity score in patients homozygous for the p.E148Q variant with or without additional p.V726A mutation.
Statistical analysis
Characteristics were compared between FMF patients with p.E148Q/p.E148Q and p.E148Q/p.E148Q + p.V726A/- MEFV variants. The Mann–Whitney U test was used to compare numerical variables, and the chi-square test and Fisher’s exact tests were used to compare categorical variables, as appropriate. Characteristics were furthermore compared between patients with mild and moderate disease severity according to the Tel Hashomer Key to Severity Score utilizing the Mann–Whitney U test and the chi-square and Fisher’s exact tests, as noted above. CRP levels before and after treatment were compared using the Wilcoxon signed-rank test.
All data were analyzed using R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). In all analyses, p ≤ 0.05 for the two-tailed tests was considered statistically significant.
Results
A total of 134 patients with the p.E148Q homozygous variants were initially enrolled in the study, of which 70 patients with combined homozygous variants (homozygous variants for p.E148Q along with another known homozygous variant for FMF) were excluded. Three patients had missing information and were also excluded. A total of 61 FMF patients were included in the current study of which 24 (39%) had p.E148Q/p.E148Q variant and 37 (61%) had p.E148Q/p.E148Q + p.V726A/- variants. Of all included patients, the median age at FMF onset was 16.0 years (IQR, 8.5–29.5), and 26 (43%) of the patients were male. The largest ethnic group was Druze (n = 44, 72%), followed by Muslims (n = 12, 20%). Regarding the p.E148Q/p.E148Q + p.V726A/- MEFV variant, it is most prevalent in Druze 34 (91.9%). The baseline characteristics of the two genotype groups are summarized in Table 1.
The severity of FMF, assessed by using the Tel Hashomer criteria [3] which was fulfilled by all patients but 2, was generally mild to moderate in both genotype groups. Forty (65.5%) patients had mild disease while 19 (31.1%) of the patients had moderate disease. Two (3.2%) patients had no disease. There were no patients with this variant with severe disease. There was no significant difference in the distribution of severity scores between the two genotype groups (p = 0.71, Table 1).
When stratified by disease severity (Table 2), patients with moderate disease had an earlier age at disease onset (median 9.0 years vs. 18.0 years, p = 0.03) and required higher colchicine doses (median 1.8 mg/day vs. 1.0 mg/day, p < 0.01) compared to those with mild disease. Additionally, patients with moderate severity experienced more frequent attacks (median 2.0 per month vs. 1.0 per month, p = 0.04) as expected. Disease severity did not differ significantly between the two MEFV variant groups.
FMF patients of all ethnic groups had mild disease severity more frequently than moderate severity, except for Muslim patients with the p.E148Q/p.E148Q + p.V726A/- MEFV variant, whose disease severity was most commonly moderate (Fig. 1).

Stacked bar plots of disease severity in FMF patients (n = 59) of different descent, stratified by MEFV mutation
In addition, we noted that colchicine treatment has led to a significant reduction in CRP levels in all homozygous patients to p.E148Q/p.E148Q variant whether they had additional p.V726A mutation or not (Fig. 2 depicts the changes in CRP levels before and after colchicine treatment, stratified by MEFV genotype). However, in the presence of p.V726A mutation, the colchicine dosage was higher (Table 2).

Paired boxplots of CRP levels before and after colchicine treatment, stratified by MEFV mutation
Discussion
Over the years, FMF research has been fraught with debate on whether the pure p.E148Q variant is an insignificant variant [11,12,13,14], a disease-causing variant with low penetrance and mild symptoms [15], or a significant variant in specific ethnic groups [16, 17]. This study aimed to clarify the clinical characteristics and disease severity associated with the p.E148Q variant in FMF patients and contribute to the ongoing debate regarding its pathogenicity.
Our results demonstrated that the p.E148Q variant, whether in the homozygous state (p.E148Q/p.E148Q) or combined with the p.V726A mutation (p.E148Q/p.E148Q + p.V726A), is generally associated with mild to moderate disease severity according to Tel Hashomer Key to Severity Score [3]. Specifically, 40/59 = 67.7% of the patients exhibited mild disease, while 19/59 = 32.2% had moderate disease, and no patients presented with severe disease. This supports the hypothesis that patients who are homozygous for the p.E148Q variant with or without p.V726A may display a clinical FMF phenotype with mild to moderate severity.
Previous studies have yielded mixed results regarding the significance of the p.E148Q variant. For instance, a genetic study from Israel on patients of Jewish-Sephardic descent found similar frequencies of the p.E148Q allele among patients and controls, suggesting it might be a benign polymorphism [11]. Another study from Israel could not provide evidence to support the notion that p.E148Q is a disease-causing variant and not a mere genetic polymorphism, despite the large sample size [18]. Conversely, Aydin et al. reported that Turkish FMF patients with the p.E148Q variant alone presented later in life and had a milder disease course but exhibited similar clinical findings to those with more severe variants [15]. Similarly, Topaloglu et al. found that Turkish patients who are homozygous for p.E148Q and negative for other pathogenic MEFV variants may display a clinical FMF phenotype with moderate to severe disease activity, although the severity may be milder compared to patients with other variants [17].
A study on Egyptian FMF patients uniquely found the p.E148Q variant to be the most frequent MEFV variant (38.6%) in their FMF cohort, associating this variant with abdominal pain, fever, and high serum amyloid A. Notably, in this study, all patients were of Arabic descent, and 57.2% of this group had undefined variants [16].
Our current study strengthens these findings from several cohorts worldwide, suggesting that the p.E148Q variant is associated with a clinical phenotype rather than being a benign variant. The differences observed in different cohorts likely result from the varying prevalence of variants among different ethnic groups. In Israel, while the homozygous p.M694V mutation is the most prevalent among Jews, the p.E148Q variant is the most common among Druze (56%). Among other Arab citizens in Israel (Muslims and Christians), the three most prevalent homozygous mutations are p.V726A, p.M694V, and p.M694I [8]. This may explain the high percentage of Druze patients homozygous for the p.E148Q variant in our current study (72%) in addition to their significant geographical distribution in our region.
In a recent article, Ben-Chetrit et al. discuss the significance of carrying MEFV variants in symptomatic and asymptomatic individuals, since many MEFV gene variants remain unclassified, with around 30% as variants of uncertain significance (VUS). They conclude that only the presence of likely pathogenic variants on both alleles should result in a definitive diagnosis. Otherwise, diagnoses such as probable FMF or FMF-like disease are considered. Additionally, they emphasize that genetic testing is only part of the diagnostic process; a comprehensive evaluation of a patient’s medical history and clinical symptoms is essential for accurate diagnosis and treatment [19].
Adding to the ethnic diversity, the overall disease severity in our study was mild to moderate across all ethnic groups, except for Muslim patients with the p.E148Q/p.E148Q + p.V726A variant, who exhibited predominantly moderate disease severity. This ethnic variability underscores the importance of considering genetic background, in addition to the environmental factors, when evaluating FMF patients.
It is generally known that the addition of another heterozygous variant typically causes more serious disease phenotype in FMF. For instance, the p.V726A ± p.E148Q allele is considered to be associated with severe disease and strongly predisposes to renal amyloidosis, in contrast to an isolated p.E148Q variant [20]. Also, patients homozygous for the complex allele p.E148Q-p.V726A/ p.E148Q-p.V726A, or p.E148Q-p.V726A/ p.V726A compound heterozygotes have more severe disease compared to patients homozygous for p.V726A [18]. Interestingly, in our study, the addition of the p.V726A mutation did not aggravate the clinical phenotype in our cohort. However, knowing that p.V726A is a pathogenic variant, it is possible that with an increased number of patients in the cohort, the number of patients with moderate disease and carrying the p.E148Q/p.E148Q + p.V726A genotype will be significantly higher than those affected with the mild form and homozygous for p.E148Q. The fact that p.E148Q variant may have clinical significance even without additional MEFV mutations is further supported by the significant reduction in CRP levels following colchicine treatment, confirming the pathogenicity of the p.E148Q variant through objective inflammatory markers. In addition, this finding supports the importance of identifying and treating also cases with a mild disease severity.
Our study also examined clinical parameters such as age at disease onset, frequency of attacks, and colchicine dosage. Patients with moderate disease had an earlier onset, more frequent attacks, and required higher doses of colchicine compared to those with mild disease. These findings align with the expected progression of FMF, where earlier onset and higher attack frequency indicate more active disease.
However, our study has several limitations. Its retrospective design and reliance on electronic medical records may not capture all relevant clinical details. Additionally, the genetic analysis did not include the full length of the MEFV gene, potentially missing other pathogenic variants. Future research should include larger, multicenter cohorts and comprehensive genetic testing to validate these results and explore the molecular mechanisms underlying the variable expressivity of the p.E148Q variant.
In conclusion, our study provides valuable insights into the clinical characteristics and disease severity associated with the p.E148Q variant in FMF patients, supporting its pathogenic role in particular ethnicity. The findings suggest that p.E148Q, whether alone or in combination with p.V726A, generally results in mild to moderate disease, responds well to colchicine treatment, and exhibits variability across different ethnic groups. Continued research is essential to fully elucidate the pathogenic nature of the p.E148Q variant and its implications for FMF diagnosis and treatment.
Data availability
All relevant data are reported in the article. The data used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Abbreviations
- FMF :
-
Familial Mediterranean fever
- CHS :
-
Clalit Health Services
- HMOs :
-
Health Maintenance Organizations
- CRP :
-
C-reactive protein
References
Kucuk A, Gezer IA lbayra., Ucar R, Karahan AY avu. Familial Mediterranean fever. Acta medica (Hradec Kral [Internet]. 2014 [cited 2024 Jun 5];57(3):97–104. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/25649364/
Sari I, Birlik M, Kasifoglu T. Familial Mediterranean fever: an updated review. Eur J Rheumatol [Internet]. 2014 Mar 7 [cited 2024 Jun 5];1(1):21–33. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/27708867/
Sohar E, Gafni J PM. Tel Hashomer key to severity score for FMF. In: First international conference of FMF. London, Tel Aviv: Freund Publishing House; 1997.
Alghamdi M. Familial Mediterranean fever, review of the literature. Clin Rheumatol [Internet]. 2017 Aug 1 [cited 2024 Jun 6];36(8):1707–13. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/28624931/
Chae JJ, Cho YH, Lee GS, Cheng J, Liu PP, Feigenbaum L, et al. Gain-of-function Pyrin mutations induce NLRP3 protein-independent interleukin-1β activation and severe autoinflammation in mice. Immunity [Internet]. 2011 May 27 [cited 2024 Jun 6];34(5):755–68. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/21600797/
Park YH, Wood G, Kastner DL, Chae JJ. Pyrin inflammasome activation and RhoA signaling in the autoinflammatory diseases FMF and HIDS. Nat Immunol [Internet]. 2016 Jul 19 [cited 2024 Jun 30];17(8):914–21. Available from: https://pubmed.ncbi.nlm.nih.gov/27270401/
Infevers - Tabular list [Internet]. [cited 2024 Jun 30]. Available from: https://infevers.umai-montpellier.fr/web/search.php?n=1
Sharkia R, Mahajnah M, Zalan A, Athamna M, Azem A, Badarneh K, et al. Comparative screening of FMF mutations in various communities of the Israeli society. Eur J Med Genet [Internet]. 2013 Jul [cited 2024 Jun 6];56(7):351–5. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/23602951/
Cazeneuve C, Sarkisian T, Pêcheux C, Dervichian M, Nédelec B, Reinert P, et al. MEFV-Gene analysis in Armenian patients with familial Mediterranean fever: diagnostic value and unfavorable renal prognosis of the M694V homozygous genotype-genetic and therapeutic implications. Am J Hum Genet [Internet]. 1999 [cited 2024 Jun 6];65(1):88–97. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/10364520/
Dewalle M, Domingo C, Rozenbaum M, Ben-Chétrit E, Cattan D, Bernot A, et al. Phenotype-genotype correlation in Jewish patients suffering from familial Mediterranean fever (FMF). Eur J Hum Genet [Internet]. 1998 [cited 2024 Jun 6];6(1):95–7. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/9781020/
Ben-Chetrit E, Lerer I, Malamud E, Domingo C, Abeliovich D (2000) The E148Q mutation in the MEFV gene: is it a disease-causing mutation or a sequence variant? Hum Mutat 15(4):385–386
Salehzadeh F, Sharghi A, Motayayagheni A, Hosseini Asl S, Mottaghi M, Sarkhanloo S. MEFV gene variant alleles in normal population of Northwest of Iran, which is near to Mediterranean Sea. Genet Res Int [Internet]. 2019 [cited 2024 Jun 6];2019. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/31531243/
Coşkun S, Varol S, Özdemir HH, Çelik SB, Balduz M, Camkurt MA, et al. Association between sequence variations of the Mediterranean fever gene and the risk of migraine: a case-control study. Neuropsychiatr Dis Treat [Internet]. 2016 Aug 29 [cited 2024 Jun 6];12:2225–32. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/27621632/
Bonyadi M, Esmaeili M, Karimi A, Dastgiri S. Common Mediterranean fever gene mutations in the Azeri Turkish population of Iran. Genet Test Mol Biomarkers [Internet]. 2010 Feb 1 [cited 2024 Jun 6];14(1):149–51. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/19929404/
Aydın F, Çakar N, Özçakar ZB, Uncu N, Başaran Ö, Özdel S, et al. Clinical features and disease severity of Turkish FMF children carrying E148Q mutation. J Clin Lab Anal [Internet]. 2019 May 1 [cited 2024 Jun 6];33(4). Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/30714637/
Mansour AR, El-Shayeb A, El Habachi N, Khodair MA, Elwazzan D, Abdeen N, et al. Molecular patterns of MEFV gene mutations in Egyptian patients with familial Mediterranean fever: a retrospective cohort study. Int J Inflam [Internet]. 2019 [cited 2024 Jun 6];2019:2578760. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30915208
Topaloglu R, Batu ED, Yıldız Ç, Korkmaz E, Özen S, Beşbaş N, et al. Familial Mediterranean fever patients homozygous for E148Q variant may have milder disease. Int J Rheum Dis [Internet]. 2018 Oct 1 [cited 2024 Jun 6];21(10):1857–62. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/27457448/
Marek-Yagel D, Bar-Joseph I, Pras E, Berkun Y. Is E148Q a benign polymorphism or a disease-causing mutation? J Rheumatol [Internet]. 2009 Oct [cited 2024 Jun 6];36(10):2372. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/19820229/
Ben-Chetrit E, Touitou I. The significance of carrying MEFV variants in symptomatic and asymptomatic individuals. 2024 [cited 2024 Jul 1]; Available from: https://onlinelibrary.wiley.com/doi/10.1111/cge.14566
Gershoni-Baruch R, Brik R, Shinawi M, Livneh A. The differential contribution of MEFV mutant alleles to the clinical profile of familial Mediterranean fever. Eur J Hum Genet [Internet]. 2002 [cited 2024 Jun 6];10(2):145–9. Available from: https://pubmed-ncbi-nlm-nih-gov.carmelmc.idm.oclc.org/11938447/
Funding
Open access funding provided by Technion - Israel Institute of Technology.
Author information
Authors and Affiliations
Contributions
EOA collected the patient data, analyzed and interpreted the patient data, and was a major contributor in writing the manuscript. LK was a major contributor in writing the manuscript and revising it. JVS analyzed and interpreted the patient data and contributed to the writing of the manuscript. AMB contributed to the writing the manuscript. JH helped in collecting patients, and RB contributed in writing the manuscript. TG contributed in writing the manuscript. MHS analyzed and interpreted the patient data and was a major contributor in writing the manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study was performed in accordance with the principles of the Declaration of Helsinki and was approved by the research ethics committee (institutional review board) of Carmel Medical Center (CMC-0009–20).
Informed consent
“Requirement for individual patient informed consent forms was waived by the Institutional Review Board of Carmel Medical Center (CMC-0009-20) due to the retrospective, observational nature of this de-identified study.”
Consent for publication
All authors reviewed the manuscript, helped in editing it, and approved of its publication.
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Peter de Winter
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Orouk Awaad, E., Khoury, L., van Straalen, J.W. et al. E148Q variant: a familial Mediterranean fever-causing mutation or a sequence variant?. Eur J Pediatr 183, 4499–4506 (2024). https://doi.org/10.1007/s00431-024-05690-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-024-05690-5