
Abstract
Purpose
When brain cancer relapses, treatment options are scarce. The use of molecularly matched targeted therapies may provide a feasible and efficacious way to treat individual patients based on the molecular tumor profile. Since little information is available on this strategy in neuro-oncology, we retrospectively analyzed the clinical course of 41 patients who underwent advanced molecular testing at disease relapse.
Methods
We performed Sanger sequencing, targeted next generation sequencing, and immunohistochemistry for analysis of potential targets, including programmed death ligand 1, cyclin D1, phosphorylated mechanistic target of rapamycin, telomerase reverse transcriptase promoter mutation, cyclin-dependent kinase inhibitor 2A/B deletion, or BRAF-V600E mutation. In selected patients, whole exome sequencing was conducted.
Results
The investigation included 41 patients, of whom 32 had isocitrate dehydrogenase (IDH) wildtype glioblastoma. Molecular analysis revealed actionable targets in 31 of 41 tested patients and 18 patients were treated accordingly (matched therapy group). Twenty-three patients received molecularly unmatched empiric treatment (unmatched therapy group). In both groups, 16 patients were diagnosed with recurrent IDH wildtype glioblastoma. The number of severe adverse events was comparable between the therapy groups. Regarding the IDH wildtype glioblastoma patients, median progression-free survival (mPFS) and median overall survival (mOS) were longer in the matched therapy group (mPFS: 3.8 versus 2.0 months, p = 0.0057; mOS: 13.0 versus 4.3 months, p = 0.0357).
Conclusion
These encouraging data provide a rationale for molecularly matched targeted therapy in glioma patients. For further validation, future study designs need to additionally consider the prevalence and persistence of actionable molecular alterations in patient tissue.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Novel systemic treatment options are urgently needed in the field of neuro-oncology. For glioblastoma patients, clinical outcome remains poor and effective systemic treatment options beyond temozolomide are scarce. Especially at disease recurrence, the standards of care are not well defined (Weller and Le Rhun 2020).
In the 2016 World Health Organization (WHO) Classification of Tumors of the Central Nervous System, a set of molecular markers has been implemented in clinical routine (Louis et al. 2016). With the current fifth edition of the WHO classification, published in 2021, the impact of molecular markers with relevance for diagnosis and treatment for primary brain tumors further increased (Louis et al. 2021). To address intra- and interindividual tumor heterogeneity—a known phenomenon of malignant intracranial tumors (Körber et al. 2019)—personalized molecularly matched therapy strategies are the next logical step in anticancer treatment.
The identification of actionable molecular drivers is increasingly gaining traction for multiple different cancer entities and has become a central part in cancer treatment (Bedard et al. 2020). Next generation sequencing (NGS) techniques, among others (e.g. Sanger sequencing, immunohistochemistry, fluorescence in situ hybridization—FISH) led to a better understanding of brain tumors at the molecular level and resulted in the identification of promising actionable targets—such as BRAF-V600E mutations—revealing novel opportunities for targeted treatment. Despite the progress made over the past years, the therapeutic relevance of both driver mutations and also the increasing number of variants of unknown significance in a cancer-specific context are in their infancy, particularly for brain cancer (Carr et al. 2016). Nevertheless, tumor-agnostic investigations postulate a superior efficacy of a molecularly matched targeted therapy over molecularly unmatched treatments. In a retrospective cancer-agnostic investigation with approximately 1500 patients, Tsimberidou et al. reported higher rates of response and longer overall survival rates for patients with molecularly matched targeted therapy compared to patients who received molecularly unmatched empiric therapy (Tsimberidou et al. 2017). On the other hand, there is an ongoing debate on how far the cancer-agnostic precision oncology approach can be taken, as the cellular context remains important for the vast majority of genomic variants (Photopoulos 2020). In recent years, interdisciplinary tumor boards have begun to implement molecularly based treatment suggestions in the field of neuro-oncology, particularly for the notoriously treatment-resistant relapse of disease. There is a paucity of data regarding the outcome of these treatment suggestions.
In prior clinical glioblastoma trials, targeted treatments failed to improve overall survival in predominantly molecularly unselected patient cohorts (Weller and Le Rhun 2020). However, the known glioblastoma-inherent inter- and intraindividual tumor heterogeneity requires a strong patient selection for the application of personalized molecularly matched targeted therapies. The ongoing N2M2/NOA-20 trial (EudraCT number: 2015-002,752-27) will provide important data about the efficacy of molecularly matched targeted therapies in first-line glioblastoma treatment (Wick et al. 2019).
In our retrospective analysis of recurrent glioma patients, we were curious to determine pilot data on the feasibility of molecularly based treatment suggestions.
Methods
Study design
All patients with recurrent disease under oncologic treatment at the Division of Clinical Neurooncology, Department of Neurology at the University Hospital Essen, who underwent advanced molecular testing from January 2017 until December 2020 were considered eligible for this retrospective analysis. The following inclusion criteria had to be met:
-
(1)
Adult patients diagnosed with recurrent glioma.
-
(2)
Availability of information on the pathohistological brain tumor diagnosis as per the WHO Classification of Tumors of the Central Nervous System from 2016 (Louis et al. 2016).
-
(3)
Performed advanced molecular testing (see below) at the Institute of Neuropathology of the University Hospital Essen or by an external provider of genetic diagnostics and sequencing services.
Decisions to perform advanced molecular analysis for patients with recurrent glioma were made by treating physicians. Data were discussed in the molecular tumor board of the University Hospital Essen and treatment recommendations were based on the criteria for molecularly matched targeted therapy (see below). As most targeted treatments do not have a label for brain cancer, approval for reimbursement by health insurances was requested for each individual patient, which requires an additional medical review by insurances. Before starting therapy, we extensively informed patients about their individual baseline situation, the side effect profile of the corresponding drug, and the available treatment alternatives in detailed individual visits. In a few patients, Karnofsky Performance Score (KPS) was 50% and almost exclusively driven by motor deficits (such as hemiparesis or nonfluent aphasia), whereas the cognitive function was well preserved allowing for the patients to provide reliable informed consent. These patients were considered to receive a further line of treatment, if an estimated life expectancy of at least six months was to be assumed. Treatment response was determined according to the updated response assessment criteria for high-grade gliomas (Wen et al. 2010). Toxicity was assessed according to the Common Terminology Criteria for Adverse Events (CTCAE, Version 5). Magnetic resonance imaging (MRI) scans to ascertain treatment response were performed every 8–12 weeks.
This study was approved by the local ethics committee of the University Duisburg-Essen (application number: 20-9431-BO).
Advanced molecular analysis
We performed immunohistochemistry on programmed death ligand 1 (PD-L1), phosphorylation of mechanistic target of rapamycin (p-mTOR), and cyclin D1, Sanger sequencing for telomerase reverse transcriptase (TERT) promoter, FISH for cyclin-dependent kinase inhibitor 2A/B (CDKN2A/B) deletion, and panel-based NGS including key genetic alterations associated with tumor proliferation such as BRAF-V600E mutation. Furthermore, whole exome sequencing (WES) using Illumina’s NovaSeq 6000 system with a read length of 2 × 100 base pairs and an output of 12 GB per sample with matched WES from blood (germ-line control) were conducted in 18 patients.
Molecularly matched targeted therapy
Molecular alterations were considered actionable, if clinical or compelling preclinical evidence of a predictive benefit from a specific therapy (in any cancer type) had been reported in the past (Pishvaian et al. 2020). Actionability was assessed considering published evidence according to Leichsenring et al. (Leichsenring et al. 2019) as well as the evidence for blood–brain barrier penetration of the molecularly matched targeted drug and the availability in Germany. Also, the patient’s medical history (including standard therapies, off-label therapies, and enrollment into specific clinical trials) was considered. In case of multiple molecularly matched targeted treatment options, a shortlist of ranked therapy options was generated on a case-by-case basis. If no actionable target was detected or molecularly matched targeted treatment could not be performed for other reasons (see below for detailed information), a molecularly unmatched empiric treatment decision was implemented.
Statistics
We used the Kaplan–Meier estimator to assess the survival function from lifetime data. Concerning the evaluation of the progression-free survival (PFS) and overall survival (OS), the time period of interest extended from the time point of latest MRI-defined recurrence before onset of investigated therapy until the next MRI indicating repeat recurrence. Before the initiation of treatment, we ruled out putative pseudoprogression by subsequent MRI and/or positron emission tomography (PET) imaging according to the updated response assessment criteria for high-grade gliomas (Wen et al. 2010). If progression or death had not occurred at the time of analysis (August 31, 2021), the patient was considered censored for survival analysis. For data visualization, GraphPad Prism version 9.2.0 (GraphPad Software Inc., San Diego, USA) and Affinity Designer version 1.9.0 (Serif Europe, West Bridgford, UK) were used.
Results
Patient characteristics
In total, 41 patients received advanced molecular analysis, of whom 18 (44%) received a molecularly matched targeted treatment recommendation (henceforth defined as the matched therapy group) and 23 (56%) were treated according to a molecularly unmatched empiric treatment decision (henceforth defined as the unmatched therapy group). In both groups, 16 patients were diagnosed with recurrent isocitrate dehydrogenase (IDH) wildtype glioblastoma. All patient characteristics are listed in Tables 1, 2. Detailed clinical and molecular information for every single patient from the matched therapy group and the unmatched therapy group is listed in Supplementary Table S1 and Supplementary Table S2. The therapy groups were balanced for age and KPS. In both groups, the investigated treatment was administered between the first and fifth disease recurrence with median treatment onset at second recurrence. In both therapy groups, 61% of the patients had no additional treatment (surgery, radiotherapy, tumor-treating fields) besides systemic medical therapy during the therapy line of interest. Concerning the IDH wildtype glioblastoma patients, 56% in the matched therapy group versus 63% in the unmatched therapy group received no additional treatment during the therapy line of interest.
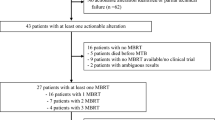
Thirty-one (76%) patients had an actionable molecular target and 18 (44%) were treated with a molecularly matched targeted therapy, whereas 23 (56%) were treated according to a molecularly unmatched empiric treatment decision instead (Fig. 1a). Fifteen from 18 (83%) patients in the matched therapy group had more than one actionable target. In total, eight different molecularly matched targeted treatment schemes were administered (Fig. 1b). Eribulin, a fully synthetic macrocyclic ketone analogue of the marine natural product halichondrin B and a specific inhibitor of TERT-RNA-dependent RNA polymerase, was used in patients with TERT promoter mutation according to published preclinical data (Takahashi et al. 2019). Cabozantinib, a small molecule multi-tyrosine kinase inhibitor against vascular endothelial growth factor receptor (VEGFR) and MET was used in patients with MET amplification, as it was shown to be effective in the treatment of lung cancer (D’Arcangelo et al. 2019). The combination of dabrafenib plus trametinib represents standard of care for BRAF-V600E-mutant melanoma and lung cancer patients (Long et al. 2015; Planchard et al. 2017) and was applied in case of BRAF-V600E mutation on the basis of several case reports in brain tumors (Johanns et al. 2018). Lorlatinib, an orally administered inhibitor of anaplastic lymphoma kinase (ALK) and ROS1, was administered in patients with ALK rearrangement pursuant to the findings observed in lung cancer (Shaw et al. 2020). Palbociclib, a cyclin-dependent kinase 4/6 (CDK4/6) inhibitor, was administered in patients with homozygous CDKNA2/B deletion due to published evidence from its use in metastatic breast cancer (Finn et al. 2016). Pembrolizumab was used in patients with PD-L1 expression due to published evidence from the treatment of glioblastoma (Reardon et al. 2021). Abemaciclib was used on the basis of homozygous CDKN2A/B deletion according to the results of the interim analysis of the Individualized Screening Trial of Innovative Glioblastoma Therapy (INSIGhT) (Wen et al. 2020). Osimertinib, a highly potent small molecule inhibitor of epidermal growth factor receptor (EGFR), was used in the presence of an EGFR mutation as had been used previously in the successful treatment of lung cancer (Soria et al. 2018). In the unmatched therapy group, no actionable target could be detected in ten (44%) patients (Fig. 1c). The reasons for the other 13 patients in the unmatched therapy group with detected actionable molecular targets for not receiving a molecularly matched targeted therapy were lack of reimbursement approval from the health insurance in seven patients, and for six patients currently under active molecularly unmatched empiric treatment, reimbursement for a molecularly matched targeted treatment option was approved by the corresponding health insurance, making it a future treatment recommendation in case of repeat tumor progression (Fig. 1d). In the unmatched therapy group, five different treatment schemes were administered (Fig. 1e). Figure 1f–h shows a synoptical display of the corresponding evidence levels according to Leichsenring et al. (Leichsenring et al. 2019) regarding the use of the molecularly matched targeted therapies. As indicated, most of the applied molecularly matched targeted drugs were based on level C (according to the American Society of Clinical Oncology—ASCO—classification), level III (according to the European Society for Medical Oncology—ESMO—classification) or level m2 (according to the National Center for Tumor Diseases Heidelberg—NCT—classification) evidence (Fig. 1f-h).

Basal characteristics of the molecularly advanced analyzed patient cohort. Eighteen (44%) patients received molecularly matched targeted therapy (matched therapy group) and in 23 (56%) patients a molecularly unmatched empiric treatment decision (unmatched therapy group) was implemented (a). Overall, a total of eight different molecularly matched targeted therapy schemes were administered (b). In the unmatched therapy group ten (43%) patients had no actionable target detected (c), which was—among others—the major cause for not receiving a molecularly matched targeted therapy. For seven patients no reimbursement from the corresponding health insurance could be obtained and in six patients under empiric treatment, molecularly matched targeted treatment was a future recommendation at the time of data cutoff (d). In the unmatched therapy group, five different therapy schemes were administered (e). Treatment decisions in the matched therapy group were mostly made on the basis of evidence from other tumor entities. The corresponding evidence levels according to available classifications from the American Society of Clinical Oncology (ASCO), the European Society for Medical Oncology (ESMO), and the National Center for Tumor Diseases Heidelberg (NCT) are shown in (f–h). AA anaplastic astrocytoma, ALK anaplastic lymphoma kinase, ASCO American Society of Clinical Oncology, CDK4 cyclin-dependent kinase 4, CDKN2A/B cyclin-dependent kinase inhibitor 2A/B, DA diffuse astrocytoma, EGFR epidermal growth factor receptor, ESMO European Society for Medical Oncology, GBM isocitrate dehydrogenase (IDH) wildtype glioblastoma, GBM* IDH mutant glioblastoma, NCT National Center for Tumor Diseases Heidelberg, mTOR mechanistic target of rapamycin, PIK3CA phosphatidylinositol 3-kinase catalytic subunit alpha, PD-L1 programmed death ligand 1, TERT telomerase reverse transcriptase
There were three patients in the matched therapy group with treatment durations of at least 24 weeks (six months). Two of these patients received treatment with the combination of dabrafenib plus trametinib and one patient received treatment with cabozantinib. The patient treated with cabozantinib had the longest duration of treatment in the matched therapy group (48 weeks), he was diagnosed with an IDH mutant glioblastoma and received cabozantinib treatment at second disease recurrence. The patients with the second and third longest duration of treatment in the matched therapy group (40 and 24 weeks) were diagnosed with IDH wildtype glioblastomas and received treatment with the combination of dabrafenib plus trametinib at fourth disease recurrence (patient with the second longest treatment duration) and at first disease recurrence (patient with the third longest treatment duration).
Treatment response
The median progression-free survival (mPFS) for the IDH wildtype glioblastoma patients was 3.8 months in the matched therapy group and 2.0 months in the unmatched therapy group (HR: 2.39, 95% CI: 1.1–5.1, p = 0.0057, Fig. 2a). PFS-6 was 25% (matched therapy group) versus 0% (unmatched therapy group). Median overall survival (mOS) for the IDH wildtype glioblastoma patients was 13.0 months in the matched therapy group versus 4.3 months in the unmatched therapy group (HR: 2.14, 95% CI: 0.94–4.88, p = 0.0357, Fig. 2b).

Kaplan–Meier curves for the isocitrate dehydrogenase (IDH) wildtype glioblastoma patients of the matched and unmatched therapy group and individual outcomes. Median progression-free survival and median overall survival were longer in the matched therapy group compared with the unmatched therapy group for IDH wildtype glioblastoma patients (a, b). Individual progression-free survival for each patient from the matched therapy group is illustrated by the swimmer’s plot in (c). For every patient in the matched therapy group (d) and in the unmatched therapy group (e), the progression-free survival difference between the therapy line of molecularly matched targeted therapy (matched therapy group) or molecularly unmatched empiric treatment (unmatched therapy group) and the prior therapy line is depicted. Each column represents the difference of one single patient of the matched therapy group (d) or the unmatched therapy group (e). A positive value means that the investigated treatment resulted in a prolonged progression-free survival compared to the previously administered treatment. A negative value means that the investigated treatment resulted in a shortened progression-free survival compared to the previously administered treatment. *Data censored at cutoff; AA anaplastic astrocytoma, DA diffuse astrocytoma, GBM isocitrate dehydrogenase (IDH) wildtype glioblastoma, GBM* IDH mutant glioblastoma, mOS median overall survival, mPFS median progression-free survival, Rec recurrence
As shown in Fig. 2c, individual PFS analysis in the matched therapy group revealed longest PFS intervals for treatment with the combination of dabrafenib plus trametinib and for treatment with cabozantinib. The longest PFS (16 months) was observed upon treatment with dabrafenib plus trametinib in an IDH wildtype glioblastoma patient at first recurrence. The poorest outcome was noted for patients treated with palbociclib. Two of three patients who received a combination of dabrafenib plus trametinib and all patients who received a single-drug treatment with cabozantinib or osimertinib had longer PFS durations than mPFS (3.8 months) in the matched therapy group.
Individual PFS differences between the treatment line in which the molecularly matched targeted therapy was administered and the treatment line immediately before revealed a longer PFS under molecularly matched targeted therapy in seven patients with the largest extension in an IDH wildtype glioblastoma patient after treatment with cabozantinib at second disease recurrence (+ 10.1 months). All cabozantinib-treated patients and two of three patients treated with the combination of dabrafenib plus trametinib had a longer PFS under molecularly matched targeted therapy. The most prominent PFS shortening could be observed for a patient after treatment with eribulin (-10.1 months). The individual PFS differences for the matched therapy group are shown in Fig. 2d. Regarding the unmatched therapy group, in only five patients a PFS extension was present. The individual PFS differences for the unmatched therapy group are shown in Fig. 2e.
Toxicity
Treatment-related death occurred neither in the matched therapy group nor in the unmatched therapy group. The number of adverse events of CTCAE grade III or higher was comparable in both groups. Table 3 synoptically displays the toxicity data of all patients subdivided into matched and unmatched therapy group.
Discussion
Our pilot data indicate that molecularly matched targeted brain tumor treatment is well tolerated and associated with prolonged disease control and longer survival compared to patients who received molecularly unmatched empiric therapy or patients with tumors lacking those molecular markers and genomic alterations that were selected for this study. Our retrospective analysis considered in an unbiased way every local glioma patient at disease recurrence whose tumor tissue received advanced molecular diagnostics from January 2017 until December 2020. We observed actionable molecular alterations in 76% of the cases, of whom 44% received molecularly matched targeted treatment. For other solid cancer entities, actionable targets were detected in 26% (pancreatic cancer), 47% (extrahepatic cholangiosarcoma), and 40% (in a tumor-agnostic study by Tourneau et al.) of investigated patients (Pishvaian et al. 2020; Lowery et al. 2018; Le Tourneau et al. 2015). In comparison, the high number of actionable targets in our cohort of glioma patients may implicate a great variety of different molecularly matched targeted treatment options in the field of neuro-oncology. However, it must be taken into account that in some previous trials only molecular alterations within distinct molecular pathways were considered, whereas in our analysis we considered any putatively actionable molecular alteration with report of clinical or compelling preclinical evidence of a predictive benefit from a specific therapy (in any cancer type).
Previous reports on molecularly matched targeted treatment in the field of neuro-oncology had already focused on feasibility, but these studies were conducted in small patient cohorts and/or did not consider toxicity or systematic comparison to a valid control group (Byron et al. 2018; Blumenthal et al. 2016; Kessler et al. 2020). Notably, some of the retrospectively included patients even underwent molecular testing for first-line treatment of glioblastoma (Kessler et al. 2020). Our study revolved around defining treatment options for recurrent glioblastoma. Considering the natural course of disease, the need for rational treatment options is highest at the time of tumor relapse, but there is no standard-of-care treatment available (Weller et al. 2021, 2013; Chaul-Barbosa and Marques 2019). To address this dilemma, every here reported patient received personalized treatment according to advanced molecular analysis and based on molecular tumor board consensus decision. Subsequently, survival times increased by a factor of two to three when molecularly matched targeted treatment was employed. The benefit occurred relative to molecularly unmatched empiric treatment that the respective control group of patients received. Molecularly unmatched empiric treatment in the glioblastoma subcohort resulted in a mPFS of 2.0 months and mOS of 4.3 months, which compares to the survival noted in the lomustine control arm of the REGOMA trial (Lombardi et al. 2019). Notably, the survival times (mPFS and mOS) of glioblastoma patients in our molecularly matched targeted therapy group exceeded any of the reported control arm data considerably, even though most of their clinical courses were more advanced (Batchelor et al. 2013; Wick et al. 2017). Thus, we noted an encouraging therapy response to molecularly matched targeted treatment.
Considering the high diagnostic effort, it must nevertheless be questioned why the effect of molecularly matched targeted treatment has not turned out to be higher. Apparently, the dynamic nature of glioblastoma, including cell and genotype heterogeneity, microenvironmental interactions, subclonal dynamics and plasticity remain a tough competitor in the management of recurrent disease (Qazi et al. 2017; Reinartz et al. 2017; Körber et al. 2019; Barthel et al. 2019; Bi et al. 2020; Schäfer et al. 2019). Furthermore, the blood–brain barrier may impact the efficacy and therapeutic window for the drugs that were used. For the molecularly matched targeted drugs used in this analysis with known ability to effectively pass the blood–brain barrier (e.g. cabozantinib, lorlatinib, abemaciclib, and osimertinib), published evidence indicates safety and clinical benefit in intracranial anticancer activity against brain metastases originating from different cancer entities (Peverelli et al. 2019; Bauer et al. 2020; Tolaney et al. 2020; Park et al. 2020). In this context, it is important to mention that for osimertinib and cabozantinib, the potential of blood–brain barrier penetrance has been investigated exclusively in previous preclinical studies (Colclough et al. 2021; Abdelaziz and Vaishampayan 2017), whereas for abemaciclib and lorlatinib previous human studies have been performed in which the drugs were detected in sufficient concentration in the cerebrospinal fluid (Patnaik et al. 2016; Shaw et al. 2017). We would view molecularly matched targeted therapy as one additional component of modern precision medicine that needs to incorporate clinically robust and relevant predictive biomarkers, innovative therapy monitoring including liquid and frequent tissue biopsies as well as combinatorial and sequential treatment strategies, patient-derived experimental disease models and co-clinical trials, and artificial intelligence-guided predictive computational models (Rajewsky et al. 2020; Aldape et al. 2019). It remains to be questioned whether the effect of molecularly matched targeted treatment can be improved by combining multiple drugs.
The findings of a study by Körber et al.—inclucing analysis of genomes, transcriptomes, and methylomes in paired primary (untreated) and recurrent (following initial treatment) tumor tissue samples from 50 patients with IDH wildtype glioblastoma—imply that standard therapy exerted little selective pressure on (most) recurrent tumors (Körber et al. 2019). Körber et al. postulated that the vast majority of driver mutations were acquired prior to initial diagnosis. These results are in tandem with the results of the study by Barthel et al. In this study, temporally separated DNA sequencing data and matched clinical annotation from 222 glioma patients were analyzed. Based on this analysis, little evidence of recurrence-specific gene alterations was found (Barthel et al. 2019). These findings contrast with the description by Kim et al. of divergent glioblastoma recurrences that share few genetic alterations with the primary tumor (Kim et al. 2015). Johnson et al. reported for low-grade gliomas—based on paired exome sequencing of 23 patients—that in 43% of cases at least half of the mutations in the initial tumor were undetected at recurrence (Johnson et al. 2014). Similar results were shown also by the work of Schäfer et al.: Based on a paired tissue analysis of 34 glioblastoma patients, a clinically relevant longitudinal heterogeneity of molecular target expression was detected leading to the assumption that patient tissue as recent as possible should be used for advanced molecular analysis (Schäfer et al. 2019). However, it is evident that even the most sensitive assay delivers only a snapshot at a distinct time point in the evolution of cancer. Clearly, new models of glioblastoma should address both prevalence and persistence of actionable molecular alterations in patient tissue and should broaden analysis beyond a single treatment-naïve sample at diagnosis to capture the evolution of recurrent, treatment-resistant disease (Qazi et al. 2017). In this study, we attempted to ensure that the molecular testing results were obtained from the recurrent tumor tissue and that treatment according to those alterations was conducted in the same line of treatment. In most patients, however, this approach failed, leaving a great deal of uncertainty as to whether the target was present at the time of treatment. We also need to consider that the patients in our pilot study were heavily pretreated; the majority of patients had received a molecularly matched targeted therapy at higher lines of treatment up to the fifth tumor recurrence. Nonetheless, we observed some particularly well-performing drugs: abemaciclib, a potent CDK4/6 inhibitor with good brain penetration approved for breast cancer, and the combination of dabrafenib/trametinib, a BRAF/mitogen-activated protein kinase kinase (MEK) inhibitor approved for the adjuvant treatment of melanoma with BRAF-V600E or -V600K mutations. There are early indications from other reports that these two drugs act favorably in glioblastoma patients (Wen et al. 2020; Johanns et al. 2018).
Lastly, limitations inherent to the performed analysis should be mentioned. The retrospective study design, small sample size and heterogeneous cohort, inconsistent disease stages, lack of randomization, and diverse types of administered drugs cannot allow simplified conclusions on efficacy. Furthermore, it has to be questioned if the presence of a distinct actionable molecular target is linked per se with a favorable prognosis in brain cancer. For future studies, a putative selection bias has to be ruled out by a matched-pair control cohort. Furthermore, it remains unknown whether a specific target represents the real tumor driver in a specific tumor entity.
However, we have observed a thorough effect of molecularly matched targeted therapy. The data from our pilot study provide a very reasonable rationale for follow-up of a larger cohort of molecularly stratified glioblastoma patients in a prospective controlled trial.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Abdelaziz A, Vaishampayan U (2017) Cabozantinib for the treatment of kidney cancer. Expert Rev Anticancer Ther 17:577–584
Aldape K, Brindle KM, Chesler L, Chopra R, Gajjar A, Gilbert MR, Gottardo N, Gutmann DH, Hargrave D, Holland EC, Jones DTW, Joyce JA, Kearns P, Kieran MW, Mellinghoff IK, Merchant M, Pfister SM, Pollard SM, Ramaswamy V, Rich JN, Robinson GW, Rowitch DH, Sampson JH, Taylor MD, Workman P, Gilbertson RJ (2019) Challenges to curing primary brain tumours. Nat Rev Clin Oncol 16:509–520
Barthel FP, Johnson KC, Varn FS, Moskalik AD, Tanner G, Kocakavuk E, Anderson KJ, Abiola O, Aldape K, Alfaro KD, Alpar D, Amin SB, Ashley DM, Bandopadhayay P, Barnholtz-Sloan JS, Beroukhim R, Bock C, Brastianos PK, Brat DJ, Brodbelt AR, Bruns AF, Bulsara KR, Chakrabarty A, Chakravarti A, Chuang JH, Claus EB, Cochran EJ, Connelly J, Costello JF, Finocchiaro G, Fletcher MN, French PJ, Gan HK, Gilbert MR, Gould PV, Grimmer MR, Iavarone A, Ismail A, Jenkinson MD, Khasraw M, Kim H, Kouwenhoven MCM, LaViolette PS, Li M, Lichter P, Ligon KL, Lowman AK, Malta TM, Mazor T, McDonald KL, Molinaro AM, Nam DH, Nayyar N, Ng HK, Ngan CY, Niclou SP, Niers JM, Noushmehr H, Noorbakhsh J, Ormond DR, Park CK, Poisson LM, Rabadan R, Radlwimmer B, Rao G, Reifenberger G, Sa JK, Schuster M, Shaw BL, Short SC, Smitt PAS, Sloan AE, Smits M, Suzuki H, Tabatabai G, Van Meir EG, Watts C, Weller M, Wesseling P, Westerman BA, Widhalm G, Woehrer A, Yung WKA, Zadeh G, Huse JT, De Groot JF, Stead LF, Verhaak RGW, Glass Consortium (2019) Longitudinal molecular trajectories of diffuse glioma in adults. Nature 576:112–120
Batchelor TT, Mulholland P, Neyns B, Nabors LB, Campone M, Wick A, Mason W, Mikkelsen T, Phuphanich S, Ashby LS, Degroot J, Gattamaneni R, Cher L, Rosenthal M, Payer F, Jurgensmeier JM, Jain RK, Sorensen AG, Xu J, Liu Q, van den Bent M (2013) Phase III randomized trial comparing the efficacy of cediranib as monotherapy, and in combination with lomustine, versus lomustine alone in patients with recurrent glioblastoma. J Clin Oncol 31:3212–3218
Bauer TM, Shaw AT, Johnson ML, Navarro A, Gainor JF, Thurm H, Pithavala YK, Abbattista A, Peltz G, Felip E (2020) Brain penetration of lorlatinib: cumulative Incidences of CNS and non-CNS progression with lorlatinib in patients with previously treated ALK-positive non-small-cell lung cancer. Target Oncol 15:55–65
Bedard PL, Hyman DM, Davids MS, Siu LL (2020) Small molecules, big impact: 20 years of targeted therapy in oncology. Lancet 395:1078–1088
Bi J, Chowdhry S, Wu S, Zhang W, Masui K, Mischel PS (2020) Altered cellular metabolism in gliomas - an emerging landscape of actionable co-dependency targets. Nat Rev Cancer 20:57–70
Blumenthal DT, Dvir A, Lossos A, Tzuk-Shina T, Lior T, Limon D, Yust-Katz S, Lokiec A, Ram Z, Ross JS, Ali SM, Yair R, Soussan-Gutman L, Bokstein F (2016) Clinical utility and treatment outcome of comprehensive genomic profiling in high grade glioma patients. J Neurooncol 130:211–219
Byron SA, Tran NL, Halperin RF, Phillips JJ, Kuhn JG, de Groot JF, Colman H, Ligon KL, Wen PY, Cloughesy TF, Mellinghoff IK, Butowski NA, Taylor JW, Clarke JL, Chang SM, Berger MS, Molinaro AM, Maggiora GM, Peng S, Nasser S, Liang WS, Trent JM, Berens ME, Carpten JD, Craig DW, Prados MD (2018) Prospective feasibility trial for genomics-informed treatment in recurrent and progressive glioblastoma. Clin Cancer Res 24:295–305
Carr TH, McEwen R, Dougherty B, Johnson JH, Dry JR, Lai Z, Ghazoui Z, Laing NM, Hodgson DR, Cruzalegui F, Hollingsworth SJ, Barrett JC (2016) Defining actionable mutations for oncology therapeutic development. Nat Rev Cancer 16:319–329
Chaul-Barbosa C, Marques DF (2019) How we treat recurrent glioblastoma today and current evidence. Curr Oncol Rep 21:94
Colclough N, Chen K, Johnstrom P, Strittmatter N, Yan Y, Wrigley GL, Schou M, Goodwin R, Varnas K, Adua SJ, Zhao M, Nguyen DX, Maglennon G, Barton P, Atkinson J, Zhang L, Janefeldt A, Wilson J, Smith A, Takano A, Arakawa R, Kondrashov M, Malmquist J, Revunov E, Vazquez-Romero A, Moein MM, Windhorst AD, Karp NA, Finlay MRV, Ward RA, Yates JWT, Smith PD, Farde L, Cheng Z, Cross DAE (2021) Preclinical comparison of the blood-brain barrier permeability of osimertinib with other EGFR TKIs. Clin Cancer Res 27:189–201
D’Arcangelo M, Tassinari M, De Marinis D, Delmonte A, Galetta D, Cecere F, Pilotto S, Zanelli F, Bonanno L, Landi L, D’Inca F, Cappuzzo F (2019) ’Phase II single arm study of CABozantinib in non-small cell lung cancer patients with MET deregulation (CABinMET). J Thorac Oncol 14:664
Finn RS, Crown JP, Ettl J, Schmidt M, Bondarenko IM, Lang I, Pinter T, Boer K, Patel R, Randolph S, Kim ST, Huang X, Schnell P, Nadanaciva S, Bartlett CH, Slamon DJ (2016) Efficacy and safety of palbociclib in combination with letrozole as first-line treatment of ER-positive, HER2-negative, advanced breast cancer: expanded analyses of subgroups from the randomized pivotal trial PALOMA-1/TRIO-18. Breast Cancer Res 18:67
Johanns TM, Ferguson CJ, Grierson PM, Dahiya S, Ansstas G (2018) Rapid clinical and radiographic response with combined dabrafenib and trametinib in adults With BRAF-mutated high-grade glioma. J Natl Compr Canc Netw 16:4–10
Johnson BE, Mazor T, Hong C, Barnes M, Aihara K, McLean CY, Fouse SD, Yamamoto S, Ueda H, Tatsuno K, Asthana S, Jalbert LE, Nelson SJ, Bollen AW, Gustafson WC, Charron E, Weiss WA, Smirnov IV, Song JS, Olshen AB, Cha S, Zhao Y, Moore RA, Mungall AJ, Jones SJM, Hirst M, Marra MA, Saito N, Aburatani H, Mukasa A, Berger MS, Chang SM, Taylor BS, Costello JF (2014) Mutational analysis reveals the origin and therapy-driven evolution of recurrent glioma. Science 343:189–193
Kessler T, Berberich A, Casalini B, Druschler K, Ostermann H, Dormann A, Walter S, Hai L, Schlesner M, Herold-Mende C, Jungk C, Unterberg A, Bendszus M, Sahm K, von Deimling A, Winkler F, Platten M, Wick W, Sahm F, Wick A (2020) ’Molecular profiling-based decision for targeted therapies in IDH wild-type glioblastoma. Neurooncol Adv 2:vdz060
Kim H, Zheng S, Amini SS, Virk SM, Mikkelsen T, Brat DJ, Grimsby J, Sougnez C, Muller F, Hu J, Sloan AE, Cohen ML, Van Meir EG, Scarpace L, Laird PW, Weinstein JN, Lander ES, Gabriel S, Getz G, Meyerson M, Chin L, Barnholtz-Sloan JS, Verhaak RG (2015) Whole-genome and multisector exome sequencing of primary and post-treatment glioblastoma reveals patterns of tumor evolution. Genome Res 25:316–327
Korber V, Yang J, Barah P, Wu Y, Stichel D, Gu Z, Fletcher MNC, Jones D, Hentschel B, Lamszus K, Tonn JC, Schackert G, Sabel M, Felsberg J, Zacher A, Kaulich K, Hubschmann D, Herold-Mende C, von Deimling A, Weller M, Radlwimmer B, Schlesner M, Reifenberger G, Hofer T, Lichter P (2019) Evolutionary trajectories of IDH(WT) glioblastomas reveal a common path of early tumorigenesis instigated years ahead of initial diagnosis. Cancer Cell 35(692–704):e12
Le Tourneau C, Delord JP, Goncalves A, Gavoille C, Dubot C, Isambert N, Campone M, Tredan O, Massiani MA, Mauborgne C, Armanet S, Servant N, Bieche I, Bernard V, Gentien D, Jezequel P, Attignon V, Boyault S, Vincent-Salomon A, Servois V, Sablin MP, Kamal M, Paoletti X, Shiva investigators (2015) Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol 16:1324–1334
Leichsenring J, Horak P, Kreutzfeldt S, Heining C, Christopoulos P, Volckmar AL, Neumann O, Kirchner M, Ploeger C, Budczies J, Heilig CE, Hutter B, Frohlich M, Uhrig S, Kazdal D, Allgauer M, Harms A, Rempel E, Lehmann U, Thomas M, Pfarr N, Azoitei N, Bonzheim I, Marienfeld R, Moller P, Werner M, Fend F, Boerries M, von Bubnoff N, Lassmann S, Longerich T, Bitzer M, Seufferlein T, Malek N, Weichert W, Schirmacher P, Penzel R, Endris V, Brors B, Klauschen F, Glimm H, Frohling S, Stenzinger A (2019) Variant classification in precision oncology. Int J Cancer 145:2996–3010
Lombardi G, De Salvo GL, Brandes AA, Eoli M, Ruda R, Faedi M, Lolli I, Pace A, Daniele B, Pasqualetti F, Rizzato S, Bellu L, Pambuku A, Farina M, Magni G, Indraccolo S, Gardiman MP, Soffietti R, Zagonel V (2019) Regorafenib compared with lomustine in patients with relapsed glioblastoma (REGOMA): a multicentre, open-label, randomised, controlled, phase 2 trial. Lancet Oncol 20:110–119
Long GV, Stroyakovskiy D, Gogas H, Levchenko E, de Braud F, Larkin J, Garbe C, Jouary T, Hauschild A, Grob JJ, Chiarion-Sileni V, Lebbe C, Mandala M, Millward M, Arance A, Bondarenko I, Haanen JB, Hansson J, Utikal J, Ferraresi V, Kovalenko N, Mohr P, Probachai V, Schadendorf D, Nathan P, Robert C, Ribas A, DeMarini DJ, Irani JG, Swann S, Legos JJ, Jin F, Mookerjee B, Flaherty K (2015) Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: a multicentre, double-blind, phase 3 randomised controlled trial. Lancet 386:444–451
Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW (2016) The 2016 world health organization classification of tumors of the central nervous system: a summary. Acta Neuropathol 131:803–820
Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, Hawkins C, Ng HK, Pfister SM, Reifenberger G, Soffietti R, von Deimling A, Ellison DW (2021) The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol 23:1231–1251
Lowery MA, Ptashkin R, Jordan E, Berger MF, Zehir A, Capanu M, Kemeny NE, O’Reilly EM, El-Dika I, Jarnagin WR, Harding JJ, D’Angelica MI, Cercek A, Hechtman JF, Solit DB, Schultz N, Hyman DM, Klimstra DS, Saltz LB, Abou-Alfa GK (2018) Comprehensive molecular profiling of intrahepatic and extrahepatic cholangiocarcinomas: potential targets for intervention. Clin Cancer Res 24:4154–4161
Park S, Lee MH, Seong M, Kim ST, Kang JH, Cho BC, Lee KH, Cho EK, Sun JM, Lee SH, Ahn JS, Park K, Ahn MJ (2020) A phase II, multicenter, two cohort study of 160 mg osimertinib in EGFR T790M-positive non-small-cell lung cancer patients with brain metastases or leptomeningeal disease who progressed on prior EGFR TKI therapy. Ann Oncol 31:1397–1404
Patnaik A, Rosen LS, Tolaney SM, Tolcher AW, Goldman JW, Gandhi L, Papadopoulos KP, Beeram M, Rasco DW, Hilton JF, Nasir A, Beckmann RP, Schade AE, Fulford AD, Nguyen TS, Martinez R, Kulanthaivel P, Li LQ, Frenzel M, Cronier DM, Chan EM, Flaherty KT, Wen PY, Shapiro GI (2016) ’Efficacy and safety of Abemaciclib, an inhibitor of CDK4 and CDK6, for patients with breast cancer non-small cell lung cancer, and other solid tumors. Cancer Discov 6:740–753
Peverelli G, Raimondi A, Ratta R, Verzoni E, Bregni M, Cortesi E, Carteni G, Fornarini G, Facchini G, Buti S, Galli L, Tucci M, Prisciandaro M, Procopio G (2019) Cabozantinib in renal cell carcinoma with brain metastases: safety and efficacy in a real-world population. Clin Genitourin Cancer 17:291–298
Photopoulos J (2020) ’The future of tissue-agnostic drugs. Nature 585:16
Pishvaian MJ, Blais EM, Brody JR, Lyons E, DeArbeloa P, Hendifar A, Mikhail S, Chung V, Sahai V, Sohal DPS, Bellakbira S, Thach D, Rahib L, Madhavan S, Matrisian LM, Petricoin EF 3rd (2020) Overall survival in patients with pancreatic cancer receiving matched therapies following molecular profiling: a retrospective analysis of the know your tumor registry trial. Lancet Oncol 21:508–518
Planchard D, Smit EF, Groen HJM, Mazieres J, Besse B, Helland A, Giannone V, D’Amelio AM Jr, Zhang P, Mookerjee B, Johnson BE (2017) Dabrafenib plus trametinib in patients with previously untreated BRAF(V600E)-mutant metastatic non-small-cell lung cancer: an open-label, phase 2 trial. Lancet Oncol 18:1307–1316
Qazi MA, Vora P, Venugopal C, Sidhu SS, Moffat J, Swanton C, Singh SK (2017) Intratumoral heterogeneity: pathways to treatment resistance and relapse in human glioblastoma. Ann Oncol 28:1448–1456
Rajewsky N, Almouzni G, Gorski SA, Aerts S, Amit I, Bertero MG, Bock C, Bredenoord AL, Cavalli G, Chiocca S, Clevers H, De Strooper B, Eggert A, Ellenberg J, Fernandez XM, Figlerowicz M, Gasser SM, Hubner N, Kjems J, Knoblich JA, Krabbe G, Lichter P, Linnarsson S, Marine JC, Marioni JC, Marti-Renom MA, Netea MG, Nickel D, Nollmann M, Novak HR, Parkinson H, Piccolo S, Pinheiro I, Pombo A, Popp C, Reik W, Roman-Roman S, Rosenstiel P, Schultze JL, Stegle O, Tanay A, Testa G, Thanos D, Theis FJ, Torres-Padilla ME, Valencia A, Vallot C, van Oudenaarden A, Vidal M, Voet T, Groups LifeTime Community Working (2020) LifeTime and improving European healthcare through cell-based interceptive medicine. Nature 587:377–386
Reardon DA, Kim TM, Frenel JS, Simonelli M, Lopez J, Subramaniam DS, Siu LL, Wang H, Krishnan S, Stein K, Massard C (2021) ’Treatment with pembrolizumab in programmed death ligand 1-positive recurrent glioblastoma: Results from the multicohort phase 1 KEYNOTE-028 trial. Cancer 127:1620–1629
Reinartz R, Wang S, Kebir S, Silver DJ, Wieland A, Zheng T, Kupper M, Rauschenbach L, Fimmers R, Shepherd TM, Trageser D, Till A, Schafer N, Glas M, Hillmer AM, Cichon S, Smith AA, Pietsch T, Liu Y, Reynolds BA, Yachnis A, Pincus DW, Simon M, Brustle O, Steindler DA, Scheffler B (2017) Functional subclone profiling for prediction of treatment-induced intratumor population shifts and discovery of rational drug combinations in human glioblastoma. Clin Cancer Res 23:562–574
Schafer N, Gielen GH, Rauschenbach L, Kebir S, Till A, Reinartz R, Simon M, Niehusmann P, Kleinschnitz C, Herrlinger U, Pietsch T, Scheffler B, Glas M (2019) Longitudinal heterogeneity in glioblastoma: moving targets in recurrent versus primary tumors. J Transl Med 17:96
Shaw AT, Bauer TM, de Marinis F, Felip E, Goto Y, Liu G, Mazieres J, Kim DW, Mok T, Polli A, Thurm H, Calella AM, Peltz G, Solomon BJ, Investigators CT (2020) First-line lorlatinib or crizotinib in advanced ALK-positive lung cancer. N Engl J Med 383:2018–2029
Shaw AT, Felip E, Bauer TM, Besse B, Navarro A, Postel-Vinay S, Gainor JF, Johnson M, Dietrich J, James LP, Clancy JS, Chen J, Martini JF, Abbattista A, Solomon BJ (2017) Lorlatinib in non-small-cell lung cancer with ALK or ROS1 rearrangement: an international, multicentre, open-label, single-arm first-in-man phase 1 trial. Lancet Oncol 18:1590–1599
Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, Dechaphunkul A, Imamura F, Nogami N, Kurata T, Okamoto I, Zhou C, Cho BC, Cheng Y, Cho EK, Voon PJ, Planchard D, Su WC, Gray JE, Lee SM, Hodge R, Marotti M, Rukazenkov Y, Ramalingam SS, Investigators F (2018) Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med 378:113–125
Takahashi M, Miki S, Fujimoto K, Fukuoka K, Matsushita Y, Maida Y, Yasukawa M, Hayashi M, Shinkyo R, Kikuchi K, Mukasa A, Nishikawa R, Tamura K, Narita Y, Hamada A, Masutomi K, Ichimura K (2019) Eribulin penetrates brain tumor tissue and prolongs survival of mice harboring intracerebral glioblastoma xenografts. Cancer Sci 110:2247–2257
Tolaney SM, Sahebjam S, Le Rhun E, Bachelot T, Kabos P, Awada A, Yardley D, Chan A, Conte P, Dieras V, Lin NU, Bear M, Chapman SC, Yang Z, Chen Y, Anders CK (2020) A phase II study of abemaciclib in patients with brain metastases secondary to hormone receptor-positive breast cancer. Clin Cancer Res 26:5310–5319
Tsimberidou AM, Hong DS, Ye Y, Cartwright C, Wheler JJ, Falchook GS, Naing A, Fu S, Piha-Paul S, Janku F, Meric-Bernstam F, Hwu P, Kee B, Kies MS, Broaddus R, Mendelsohn J, Hess KR, Kurzrock R (2017) ’Initiative for molecular profiling and advanced cancer therapy (IMPACT): an MD anderson precision medicine study. JCO Precis Oncol 1:1–8
Weller M, Cloughesy T, Perry JR, Wick W (2013) Standards of care for treatment of recurrent glioblastoma–are we there yet? Neuro Oncol 15:4–27
Weller M, Le Rhun E (2020) How did lomustine become standard of care in recurrent glioblastoma? Cancer Treat Rev 87:102029
Weller M, van den Bent M, Preusser M, Le Rhun E, Tonn JC, Minniti G, Bendszus M, Balana C, Chinot O, Dirven L, French P, Hegi ME, Jakola AS, Platten M, Roth P, Ruda R, Short S, Smits M, Taphoorn MJB, von Deimling A, Westphal M, Soffietti R, Reifenberger G, Wick W (2021) EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat Rev Clin Oncol 18:170–186
Wen P, Trippa L, Lee E, Fell G, Rahman R, Arrillaga-Romany I, Touat M, McCluskey C, Brunno J, Gaffey S, Drappatz J, Lassman A, Galanis E, Ahluwalia M, Colman H, Nabors L, Hepel J, Elinzano H, Schiff D, Chukwueke U, Beroukhim R, Nayak L, Mcfaline-Figueroa J, Batchelor T, Rinne M, Kaley T, Lu-Emerson C, Bi WL, Arnaout O, Peruzzi P-P, Doherty L, Haas-Kogan D, Tanguturi S, Cagney D, Aizer AA, Welch M, Lavallee M, Fisher-Longden B, Dowling S, Geduldig J, Santagata S, Meredith D, Chiocca EA, Reardon D, Ligon K, Alexander B (2020) ’Preliminary results of the abemaciclib arm in the individualized screening trial of innovative glioblastoma therapy (INSIGhT): a phase II platform trial using Bayesian adaptive randomization. Neuro Oncol 22:44–44
Wen PY, Macdonald DR, Reardon DA, Cloughesy TF, Sorensen AG, Galanis E, Degroot J, Wick W, Gilbert MR, Lassman AB, Tsien C, Mikkelsen T, Wong ET, Chamberlain MC, Stupp R, Lamborn KR, Vogelbaum MA, van den Bent MJ, Chang SM (2010) Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol 28:1963–1972
Wick W, Dettmer S, Berberich A, Kessler T, Karapanagiotou-Schenkel I, Wick A, Winkler F, Pfaff E, Brors B, Debus J, Unterberg A, Bendszus M, Herold-Mende C, Eisenmenger A, von Deimling A, Jones DTW, Pfister SM, Sahm F, Platten M (2019) N2M2 (NOA-20) phase I/II trial of molecularly matched targeted therapies plus radiotherapy in patients with newly diagnosed non-MGMT hypermethylated glioblastoma. Neuro Oncol 21:95–105
Wick W, Gorlia T, Bendszus M, Taphoorn M, Sahm F, Harting I, Brandes AA, Taal W, Domont J, Idbaih A, Campone M, Clement PM, Stupp R, Fabbro M, Le Rhun E, Dubois F, Weller M, von Deimling A, Golfinopoulos V, Bromberg JC, Platten M, Klein M, van den Bent MJ (2017) Lomustine and bevacizumab in progressive glioblastoma. N Engl J Med 377:1954–1963
Acknowledgements
None to declare.
Funding
Open Access funding enabled and organized by Projekt DEAL. None declared.
Author information
Authors and Affiliations
Contributions
Writing and reviewing of the manuscript: LL, TS, CO, TB, DP, JTS, SB, H-US, US, KK, CK, MS, KH, CD, BS, SK, MG. Statistical analysis: LL, SK. Medical data assessment: LL, TB, SK. Conceptualization: LL, BS, SK, MG.
Corresponding author
Ethics declarations
Conflict of interest
Lazaros Lazaridis received honoraria and travel support from Novocure. Teresa Schmidt received honoraria and travel support from Novocure. Jens T. Siveke reports research funding from BMS, Celgene and Roche; consulting and personal fees from AstraZeneca, Bayer, Baxalta, BMS, Celgene, Immunocore, Lilly, Novartis, Roche, Shire; has minor equity in FAPI Holding and Pharma15 (< 3%) and is a member of the Board of Directors for Pharma15 outside the submitted work. Jens T. Siveke is supported by the German Cancer Consortium (DKTK). Sebastian Bauer reports personal fees from Deciphera, grants from Incyte, grants and personal fees from Blueprint Medicines, personal fees from Lilly, grants and personal fees from Novartis, personal fees from Daichii-Sankyo, personal fees from Plexxikon, personal fees from Exelixis, personal fees from Bayer, and others from Pfizer, during the conduct of the study; personal fees from Pharmamar, personal fees from Lilly, personal fees from Roche, and personal fees from GSK, outside the submitted work. Björn Scheffler is supported by the German Cancer Consortium (DKTK) and the DFG-CRU337. Sied Kebir received honoraria and travel support from Novocure. Martin Glas reports honoraria from Roche, Novartis, UCB, Abbvie, Daiichi Sankyo, Novocure, Bayer, Janssen-Cilag, Medac, Merck, Kyowa Kirin; travel support from Novocure and Medac; research grant from Novocure. All remaining authors have declared no conflicts of interest.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the University Duisburg-Essen (August 12, 2020; application number: 20–9431-BO).
Consent to participate
For this type of study (retrospective and anonymous analysis) formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lazaridis, L., Schmidt, T., Oster, C. et al. Precision neuro-oncology: a pilot analysis of personalized treatment in recurrent glioma. J Cancer Res Clin Oncol 149, 3513–3526 (2023). https://doi.org/10.1007/s00432-022-04050-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-022-04050-w