
Abstract
Background
Conventional three-access laparoscopic appendectomy (CLA) is currently the gold standard treatment, however, Single-Port Laparoscopic Appendectomy (SILA) has been proposed as an alternative. The aim of this systematic review/meta-analysis was to evaluate safety and efficacy of SILA compared with conventional approach.
Methods
Per PRISMA guidelines, we systematically reviewed randomised controlled trials (RCTs) comparing CLA vs SILA for acute appendicitis. The randomised Mantel–Haenszel method was used for the meta-analysis. Statistical data analysis was performed with the Review Manager software and the risk of bias was assessed with the Cochrane "Risk of Bias" assessment tool.
Results
Twenty-one studies (RCTs) were selected (2646 patients). The operative time was significantly longer in the SILA group (MD = 7,32), confirmed in both paediatric (MD = 9,80), (Q = 1,47) and adult subgroups (MD = 5,92), (Q = 55,85). Overall postoperative morbidity was higher in patients who underwent SILA, but the result was not statistically significant. In SILA group were assessed shorter hospital stays, fewer wound infections and higher conversion rate, but the results were not statistically significant. Meta-analysis was not performed about cosmetics of skin scars and postoperative pain because different scales were used in each study.
Conclusions
This analysis show that SILA, although associated with fewer postoperative wound infection, has a significantly longer operative time. Furthermore, the risk of postoperative general complications is still present. Further studies will be required to analyse outcomes related to postoperative pain and the cosmetics of the surgical scar.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Acute appendicitis is one of the most common abdominal surgical emergencies [1], and conventional three-access laparoscopic appendectomy (CLA) is currently the gold standard treatment [2]. However, an alternative surgical approach, Single-Port Laparoscopic Appendectomy (SILA), has been proposed recently [3, 4]. SILA aims to improve aesthetics, reduce postoperative pain and hospital stay, and thus lead to a faster return to work and improved quality of life. Potential disadvantages of SILA include loss of triangulation, impaired vision, intra/extra abdominal instrument conflicts, and device cost.
Previous literature reviews analysing the results of low-evidence comparative studies (controlled clinical trials—CCTs) have suggested that the two approaches are comparable but have highlighted the need for analyses of randomised controlled trials (RCTs) to suggest which procedure could be the most appropriate [5,6,7]. Therefore, we performed a systematic literature review and meta-analysis of RCTs to evaluate the safety and efficacy of single-incision laparoscopic appendectomy (SILA) compared with conventional laparoscopic appendectomy.
Materials and methods
A systematic literature review was conducted until October 2nd 2022, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [8]. The research was carried out by analysing the MEDLINE, PubMed, Scopus, and Web of Science databases without language constraints. The registration of protocol was performed on PROSPERO (ID registration CRD42020186856).
Combinations of the following search terms were used: "appendectomy" or "appendectomies, " "single-incision laparoscopic surgery (SILS)", or "single-port laparoscopic surgery", or "single-incision laparoscopic appendectomy", or "conventional 3-port laparoscopic appendectomy" or "conventional laparoscopic surgery" or "multi-incision laparoscopic surgery" or "conventional multiport laparoscopic surgery" or "classic laparoscopic surgery" or "conventional laparoscopic appendectomy" or "single incision" or "single trocar" or "single-port" or "single-port laparoscopic" or "conventional laparoscopic" or "triport laparoscopic" or "one-wound laparoscopic, " and "randomised controlled trial" or "randomised" or "placebo. "
The "Related articles" function of PubMed was used to expand the research and review all eligible studies' reference lists. A manual search was performed through the Google Scholar database to minimise retrieval bias. The search for ongoing clinical studies was performed on ClinicalTrials.gov.
References of all included studies were selected to identify any studies lost during the initial search and were entered into a dataset.
Studies included in this systematic review consider only randomised controlled trials (RCTs) and non-RCTs that have compared conventional laparoscopic appendectomy vs single-port appendectomy for acute appendicitis.
All titles and abstracts were evaluated to identify articles that could be included in the search. Then the full text of these studies was evaluated, and the following information was extracted: year of publication, inclusion criteria, exclusion criteria, and technologies used in the procedure.
The primary outcomes analysed were the following: overall postoperative complications; operative time and incidence of laparotomic conversions.
Secondary outcomes were identified: surgical wound infections; postoperative pain; length of hospital stays, and the cosmetic appearance of skin scars from trocar access holes.
In the analysis of the dichotomous variables, the extracted data were evaluated by Risk Ratio (RR), and in the continuous variables, the data were evaluated by weighted mean differences (WMD) [9].
The randomised Mantel–Haenszel method was used for the meta-analysis. The results obtained were reported in Forest Plot. Higgins index (I2), with its 95% confidence intervals and significant levels of Cochrane Q, were considered as indicators of heterogeneity [10].
Statistical data analysis was performed using the Review Manager meta-analysis software (RevMan version 5.4.1) (Copenhagen: The Nordic Cochrane Center, The Cochrane Collaboration, 2018).
Methodological assessment of the risk of bias was performed with the Cochrane "Risk of Bias" assessment tool for randomised control trials (RCTs) [11].
Systematic review results
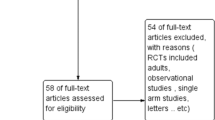
The PRISMA flow chart for the systematic review is shown in Fig. 1.

PRISMA flowchart
The initial literature search identified 1063 potentially relevant articles. After selecting titles and abstracts based on relevance, the remaining 48 articles were further evaluated for eligibility, and 27 others were excluded. The 21 studies included in this meta-analysis are RCTs.
Characteristics of the studies
The 21 studies enrolled 2646 patients with acute appendicitis who have undergone laparoscopic treatment: 1328 SILA and 1318 CLA. Enrolments took place between 2009 and 2018. Most of the studies were performed in populations from Korea (4 RCTs, comprising a total of 551 patients), the USA (3 RCTs, comprising a total of 485 patients), Spain (3 RCTs, comprising a total of 391 patients) and China (3 RCTs, comprising a total of 339 patients); the remaining studies were conducted in Pakistan (340 patients), Argentina (147 patients), India (100 patients), Scotland (77 patients), Japan (68 patients), Turkey (50 patients), Poland (50 patients) and Egypt (48 patients). Fifteen studies reported surgical experience, but the definitions differed between the included studies.
Thirteen studies reported exclusion criteria such as peri-appendicular abscess and/or mass, generalised peritonitis, appendicular tumour or phlegmon, and perforated appendix; RCTs' criteria were not significantly different.
The patients' ages were heterogeneous, so we performed a subgroup analysis. The clinical characteristics of the patients enrolled in the included studies are summarised in Table 1.
Division of the mesoappendix and section of the base of the appendix was performed with various techniques and tools. The types of single-port and tools used for SILA also varied. The technical characteristics of the surgeries performed in the included studies are summarised in Table 2.
The major number of studies do not report the calculation of sample size estimation of patients for randomised controlled trials [12,13,14,15,16,17,18,19]. In few studies the minimal sample size calculation was generically done on the study [20,21,22,23,24]. Differently, other studies [25,26,27,28] reported the same outcome on which was performed the sample size calculation, respectively post-operative complications and postoperative pain; only one study [29] reported respectively the operative time as primary outcome. In conclusion the overall field is underpowered to detect a difference in complications between the two techniques—likely due to the fact that complications are rare.
Study quality assessment
Methodological quality assessment of the RCTs was performed using the RoB 2 (Revised Cochrane risk of bias tool for randomised trials) [30] (Fig. 2). Overall low risk of bias was reported for 71.4% of the studies (15/21), but "blinding" of participants and healthcare personnel was performed in only 2/21 (9.5%) studies [17, 27]. In 14.3% (3/21) of the studies [15, 18, 22], the risk of bias of random sequence generation and allocation was rated as severe, while another 14.3% (3/21) [14, 21, 31] presented some concerns about the risk of bias due to deviation from intended surgeries.

Risk of bias—RCTs
Meta-analysis results
Primary outcomes
Postoperative complications
In 20 RCTs (2306 patients: 1158 SILA group versus 1148 CLA group), overall postoperative morbidity was higher in patients who underwent SILA (92 patients, 7,94%) compared with CLA (83 patients, 7,22%), but the result was not statistically significant (RR = 1,10, 95% CI 0,83 to 1,46; P = 0,52) and heterogeneity was very low (Q = 11,96, P = 0,89; I2 = 0). Subgroup analysis showed that morbidity was smaller in paediatric patients who underwent SILA (5,03%, 16/318) compared with CLA (2,83%, 9/318), but again the result was not statistically significant (RR = 1,73, 95% CI 0,79 to 3,79; P = 0,17) (Fig. 3).

Postoperative complications
Operative time
In 19 RCTs (2234 patients: 1120 with SILA vs 1114 with CLA group), the operative time was significantly longer in SILA than in CLA (MD = 7,32, 95% CI 5,50 to 9,14; P ≤ 0,00001). Heterogeneity was very high (Q = 113,60, P ≤ 0,00001; I2 = 84%). T he same results reported in the subgroup analysis showed statistically significant favour for the CLA group in paediatric patients (MD = 9,80, IC 95% = 6,81 to 12,79; P ≤ 0,00001), (Q = 1,47, P = 0,00006; I2 = 83%), and in adult patients (MD = 5,92, 95% CI 2,05 to 9,80; P = 0,003), (Q = 55,85, P ≤ 0,00001; I2 = 84%) (Fig. 4).

Operative time
Incidence of laparotomic conversions
In 15 RCTs (1611 patients: 811 in the SILA group vs 800 in the CLA group), a higher rate of laparotomic conversion rate was reported in patients who underwent SILA (12, 1,23%) compared to those who undergone CLA (7 patients, 0,87%) but the result was not statistically significant (RR = 1,53, 95% CI 0,68 to 3,45; P = 0,30) and heterogeneity was very low (Q = 2,28, P = 0,89; I2 = 0%). The result was analysable only in adult patients (Fig. 5).

Incidence of laparotomic conversions
Secondary outcomes
Surgical wound infections
In 20 RCTs (2596 patients: 1303 underwent SILA vs 1293 underwent CLA), postoperative wound infections were lower in patients who underwent SILA (47 patients, 3,6%) than in those who underwent CLA (59 patients, 4,56%), but the result was not statistically significant (RR = 0,78, 95% CI 0,53 to 1,15; P = 0,21). Heterogeneity was very low (Q = 13,91, P = 0,53; I2 = 0) (Fig. 6).

Surgical wound infections
Length of hospital stay
Length of hospital stay was reported in 18 RCTs (2197 patients: 1104 underwent SILA vs 1093 underwent CLA). The analysis showed a shorter hospital stay in patients who underwent SILA, but the result was not statistically significant (MD = − 0,006, 95% CI − 0,18 to 0,05; P = 0,27); heterogeneity was very high (Q = 48,63, P = 0,0001; I2 = 65%) (Fig. 7).

Length of hospital stay
Postoperative pain
Sixteen studies reported results on postoperative pain, but we did not summarise the results because different scales and assessment times were used (Table 3) [4, 12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29, 31, 33].
The aesthetic appearance of skin scars of trocar access holes
Only nine studies reported results on the cosmetic appearance of skin scars of trocar access holes, but meta-analysis was not performed because different scales were used in each study (Table 4) [14, 16, 18, 19, 21, 23, 25, 27, 31].
Discussion
This systematic review of the literature pooled the results of 21 RCTs (2646 patients enrolled). It showed that SILA is comparable to CLA in treating acute appendicitis and may have some benefits.
The most important limitation of SILA is reported in the characteristics of thirteen included, studies that reported exclusion criteria as appendicular phlegmon, perforated appendicitis and so on. Very probably this limitation could influence outcomes especially in technically difficult cases. For this reason, SILA needed an extreme accurate selection of patients: uncomplicated appendicitis associated at mild inflammatory status. In fact, the feasibility of SILA can be very low in complicated appendicitis and it is associated with higher rate risk of conversion to laparotomy and at the impossibility to place an abdominal drainage tube [32].
The only significant finding in this analysis are relates to the longer operative time, which increases significantly for SILA, as observed in most single-incision surgeries. In fact, because of intra/extra abdominal instrument conflicts, SILA is relatively difficult to perform, resulting in a significantly longer operative time than CLA. In some studies, a single surgeon performed the procedures [23, 31, 33], while other methods involved multiple surgeons. Due to differences in surgical experience, this may have influenced the statistical results. Furthermore, this longer operative time can be the consequence of limited manpower and extra time needed for the preparation and manipulation of the camera holder [34]. This longer operative time is associated at higher cost [35] and major postoperative pain for muscular stretching at the single umbilical wound [36].
Data regarding overall morbidity showed fewer cases in the CLA (7,22%) group than in the SILA group (7,94%), an advantage especially evident in paediatric patients. However, they showed no statistically significant difference between SILA and CLA (RR = 1,10, 95% CI 0,83 to 1,46; P = 0,52). In contrast, data analysis regarding abdominal wall morbidity, although equally nonsignificant, suggested a lower incidence of postoperative surgical wound infections in patients who underwent SILA. Therefore, SILA can be considered a safe and effective technique.
Hospital stay was lower in patients who underwent SILA. At the same time, the incidence of laparotomy conversions was lower in CLA than in SILA, but the results were not statistically significant in both cases. This heterogeneity of hospital stay is associated with the different timing of oral intake after appendectomy. Previously, the oral intake starts at return of bowel function evaluated during abdominal examination (bowel sound and passage of flatus); differently in other surgical unit with adopted the ERAS program a soft diet is performed as soon as possible (5–7 h post-surgery) independently from the bowel movement [37].
Data on pain were not summarised because of the heterogeneity of scales and assessment times. Although influenced by the above considerations, the RCTs did not show a significantly better outcome regarding postoperative pain or a reduction in the need for analgesics. The same applies to cosmetics data, which are not homogeneous and have yet to be grouped in a forest plot. Cosmetics were assessed in multiple of our studies through fill-in questionnaires based on subjective judgment and not through international rating scales, making cosmetic appearance an impossible outcome to compare.
The financial cost was not compared in the studies included in our meta-analysis. However, it has been pointed out that SILA can be safely performed with the same tools and costs as CLA [29]. High-energy dissection instruments, dedicated angled instruments and commercial single-access port devices were widely used in this study, which, having a high cost, could influence the choice between the two operations. The use of conventional instruments, bipolar coagulation for mesoappendix and limited application of endo stapler for stump transection would significantly lower the cost of the operation. In addition, the solution adopted by Kye et al. [26], Duza et al. [14], Shalaby et al. [12], Mo Kang et al. [21], and Park et al. [31] considers the use of a "homemade" port with a latex surgical glove, which would not affect the budget, unlike commercial single-access ports.
A limitation of the analysis is the need for more data examining the learning curve for SILA. In the studies included in our review, the specification of prior training in SILA was quantified only by Teoh et al. [27] and Lee et al. [28], who considered at least 20 and 10 SILA procedures, respectively, to be necessary to ensure competence in SILA. Frutos et al. [4] and Moriguchi et al. [15] described "previous training in SILA" without further specification, as did Mo Kang et al. [21], which reported only minimal experience in SILA. Golebiewsky et al. [20] and Mori et al. [24] described their experience with both surgical techniques. In an analysis of learning curve, Kim suggested that surgeons can have an adequate surgical skills for SILA after performed 30 appendectomy, furthermore other 90 appendectomy are needed to gain an experienced surgical skills [38].
The present meta-analysis is also limited because the results collected were mainly short-term indicators and needed long-term follow-up results. One of these long-term outcomes is port-site incisional hernia. In fact the literature reported a high rate of incisional hernia rate. In a recent systematic review of literature and meta-analysis performed on single-incision laparoscopic, surgery is associated with a threefold increase in the odds of incisional hernia than conventional laparoscopic surgery (odds ratio 2,83, 95% CI 1,34–5,98, P = 0,006, I2 = 0%) [39], similar results were reported from previous review [40, 41]. For this reason, recommendation to prevent incisional hernias is commonly performed [42].
Moreover, the results included subjective indices such as pain and aesthetic scores, which patients and evaluators easily influence.
Conclusions
In conclusion, this systematic review and meta-analysis show that Single-Port laparoscopic appendectomy do not report any advantage for the SILA, but there is only significantly longer operative time than CLA. Furthermore, it is not free from the risk of postoperative general complications, prolonged hospital stays, and the need for conversion. Probably, the inferiority of SILA than CLA and the complex learning curve are the reasons for which the SILA is uncommon.
Further studies will be required to analyse outcomes related to postoperative pain and the cosmetics of the surgical scar and make cost–benefit assessments.
Data availability
The data used to support the finding of this study are included within the article.
Change history
20 February 2024
A Correction to this paper has been published: https://doi.org/10.1007/s00464-024-10750-w
References
Ferris M, Quan S, Kaplan BS, Molodecky N, Ball CG, Chernoff GW, Bhala N, Ghosh S, Dixon E, Ng S, Kaplan GG (2017) The global incidence of appendicitis: a systematic review of population-based studies. Ann Surg 266(2):237–241
Di Saverio S, Podda M, De Simone B, Ceresoli M, Augustin G, Gori A, Boermeester M, Sartelli M, Coccolini F, Tarasconi A, De’ Angelis N, Weber DG, Tolonen M, Birindelli A, Biffl W, Moore EE, Kelly M, Soreide K, Kashuk J, Ten Broek R, Gomes CA, Sugrue M, Davies RJ, Damaskos D, Leppäniemi A, Kirkpatrick A, Peitzman AB, Fraga GP, Maier RV, Coimbra R, Chiarugi M, Sganga G, Pisanu A, De’ Angelis GL, Tan E, Van Goor H, Pata F, Di Carlo I, Chiara O, Litvin A, Campanile FC, Sakakushev B, Tomadze G, Demetrashvili Z, Latifi R, Abu-Zidan F, Romeo O, Segovia-Lohse H, Baiocchi G, Costa D, Rizoli S, Balogh ZJ, Bendinelli C, Scalea T, Ivatury R, Velmahos G, Andersson R, Kluger Y, Ansaloni L, Catena F (2020) Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg 15(1):27. https://doi.org/10.1186/s13017-020-00306-3
Chong EH, Cho HJ, Jeong SY, Kim WR, Choi SH (2020) Easily applicable single-incision laparoscopic appendectomy using straightforward instrumental alignment and conventional laparoscopic instruments. Surg Laparosc Endosc Percutan Tech 31(1):124–128
Frutos MD, Abrisqueta J, Lujan J, Abellan I, Parrilla P (2013) Randomized prospective study to compare laparoscopic appendectomy versus umbilical single-incision appendectomy. Ann Surg 257(3):413–418. https://doi.org/10.1097/SLA.0b013e318278d225
Nageswaran H, Maw A (2015) SILA: not necessarily the next step? Response to: acute appendicitis can be treated with single-incision laparoscopy: a systematic review of randomized controlled trials. Colorectal Dis 17(7):644
Gill RS, Shi X, Al-Adra DP, Birch DW, Karmali S (2012) Single-incision appendectomy is comparable to conventional laparoscopic appendectomy: a systematic review and pooled analysis. Surg Laparosc Endosc Percutan Tech 22(4):319–327
Markar SR, Karthikesalingam A, Di Franco F, Harris AM (2013) Systematic review and meta-analysis of single-incision versus conventional multiport appendicectomy. Br J Surg 100(13):1709–1718
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg 88:105906
Deeks JJ, Higgins JPT, Altman DG (eds) (2023) Chapter 10: analysing data and undertaking meta-analyses. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (eds) Cochrane handbook for systematic reviews of interventions version 6.4 (updated August 2023). Cochrane. www.training.cochrane.org/handbook
Mantel N, Haenszel W (1959) Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22(4):719–748
Higgins JPT, Li T, Deeks JJ (eds) (2023) Chapter 6: choosing effect measures and computing estimates of effect. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (eds) Cochrane handbook for systematic reviews of interventions version 6.4 (updated August 2023). Cochrane. www.training.cochrane.org/handbook
Rafik Shalaby R, Akle M, Hamed A, Abdalrazek M, Shehata S, Abdelaziz M, Helal A, Anwar H, El-Sherbiny H, Saied A (2020) Modified glove single-port laparoscopic appendectomy versus conventional laparoscopic appendectomy in adolescent age under spinal anaesthesia. J Pediatric Endosc Surg 2:153–161. https://doi.org/10.1007/s42804-019-00038-5
Zahara FT, Malik S, Ahmad I, Zia MI, Anum S (2020) Outcome of single incision versus conventional laparoscopic appendectomy: a single institute based analysis. P J M H S 14(4):1219–1222
Duza G, Davrieux CF, Palermo M, Khiangte E, Azfar M, Rizvi SAA, Trelles N, Zorraquin C, Sbai-Idrissi M, Le Brian AZ (2019) Conventional laparoscopic appendectomy versus single-port laparoscopic appendectomy, a multicenter randomized control trial: a feasible and safe alternative to standard laparoscopy. J Laparoendosc Adv Surg Tech A 29(12):1577–1584. https://doi.org/10.1089/lap.2019.0460
Moriguchi T, Machigashira S, Sugita K, Kawano M, Yano K, Onishi S, Yamada K, Yamada W, Masuya R, Kawano T, Nakame K, Mukai M, Kaji T, Ieiri S (2019) A randomized trial to compare the conventional three-port laparoscopic appendectomy procedure to single-incision and one-puncture procedure that was safe and feasible, even for surgeons in training. J Laparoendosc Adv Surg Tech A 29(3):392–395. https://doi.org/10.1089/lap.2018.0195
Pan Z, Jiang XH, Zhou JH, Ji ZL (2013) Transumbilical single-incision laparoscopic appendectomy using conventional instruments: the single working channel technique. Surg Laparosc Endosc Percutan Tech 23(2):208–211. https://doi.org/10.1097/SLE.0b013e3182827f5d
Perez EA, Piper H, Burkhalter LS, Fischer AC (2013) Single-incision laparoscopic surgery in children: a randomised control trial of acute appendicitis. Surg Endosc 27(4):1367–1371. https://doi.org/10.1007/s00464-012-2617-5
Vilallonga R, Barbaros U, Nada A, Sümer A, Demirel T, Fort JM, González O, Armengol M (2012) Single-port transumbilical laparoscopic appendectomy: a preliminary multicentric comparative study in 87 patients with acute appendicitis. Minim Invasive Surg 2012:492409. https://doi.org/10.1155/2012/492409
SCARLESS Study Group, Ahmed I, Cook JA, Duncan A, Krukowski ZH, Malik M, MacLennan G, McCormack K (2015) Single port/incision laparoscopic surgery compared with standard three-port laparoscopic surgery for appendicectomy: a randomised controlled trial. Surg Endosc 29(1):77–85. https://doi.org/10.1007/s00464-014-3416-y
Golebiewski A, Anzelewicz S, Wiejek A, Lubacka D, Czauderna P (2019) A prospective randomized controlled trial of single-port and three-port laparoscopic appendectomy in children. J Laparoendosc Adv Surg Tech A 29(5):703–709. https://doi.org/10.1089/lap.2018.0560
Kang BM, Choi SI, Kim BS, Lee SH (2018) Single-port laparoscopic surgery in uncomplicated acute appendicitis: a randomised controlled trial. Surg Endosc 32(7):3131–3137. https://doi.org/10.1007/s00464-018-6028-0
Alexander N, Elangovan B, Reddy A, Paramasivam S (2017) Single-incision multiport laparoscopic appendectomy versus conventional laparoscopic appendectomy: a single-centre randomised control study. Int J Sci Study. https://doi.org/10.17354/ijss/2017/162
Carter JT, Kaplan JA, Nguyen JN, Lin MY, Rogers SJ, Harris HW (2014) A prospective, randomised controlled trial of single-incision laparoscopic vs conventional 3-port laparoscopic appendectomy for treatment of acute appendicitis. J Am Coll Surg 218(5):950–959. https://doi.org/10.1016/j.jamcollsurg.2013.12.052
Mori VR, Rufino EJ, Gonzàlez HF, Carballal MMC, Arias EA, Kissler OJJ (2014) Estudio comparativo prospectivo aleatorizado entre apendicectomı ́a laparosco ́ pica por puerto u ́ nico y apendicectomı ́a laparosco ́pica convencional. Cirugi – 1249. Cir Esp. https://doi.org/10.1016/j.ciresp.2013.12.013
Sozutek A, Colak T, Dirlik M, Ocal K, Turkmenoglu O, Dag A (2013) A prospective randomised comparison of the single-port laparoscopic procedure with open and standard 3-port laparoscopic procedures in treating acute appendicitis. Surg Laparosc Endosc Percutan Tech 23(1):74–78. https://doi.org/10.1097/SLE.0b013e3182754543
Kye BH, Lee J, Kim W, Kim D, Lee D (2013) Comparative study between single-incision and three-port laparoscopic appendectomy: a prospective randomised trial. J Laparoendosc Adv Surg Tech A 23(5):431–436. https://doi.org/10.1089/lap.2012.0284.Epub
Teoh AY, Chiu PW, Wong TC, Poon MC, Wong SK, Leong HT, Lai PB, Ng EK (2012) A double-blinded randomised controlled trial of laparoendoscopic single-site access versus conventional 3-port appendectomy. Ann Surg 256(6):909–914. https://doi.org/10.1097/SLA.0b013e3182765fcf
Lee WS, Choi ST, Lee JN, Kim KK, Park YH, Lee WK, Baek JH, Lee TH (2013) Single-port laparoscopic appendectomy versus conventional laparoscopic appendectomy: a prospective randomised controlled study. Ann Surg 257(2):214–218. https://doi.org/10.1097/SLA.0b013e318273bde4
Wu K, Yang L, Wu A, Wang J, Xu S, Zhao H, Huang Z (2015) Single-site laparoscopic appendectomy in children using conventional instruments: a prospective, randomised, control trial. Pediatr Surg Int 31(2):167–171. https://doi.org/10.1007/s00383-014-3636-1
Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC (2023) Chapter 8: assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (eds) Cochrane handbook for systematic reviews of interventions version 6.4 (updated August 2023). Cochrane. www.training.cochrane.org/handbook
Park JH, Hyun KH, Park CH, Choi SY, Choi WH, Kim DJ, Lee S, Kim JS (2010) Laparoscopic vs transumbilical single-port laparoscopic appendectomy; results of prospective randomized trial. J Korean Surg Soc 78:213–218. https://doi.org/10.4174/jkss.2010.78.4.213
Chen Y, Fan Z, Zhang X, Fu X, Li J, Yuan J, Guo S (2023) A brief overview of single-port laparoscopic appendectomy as an optimal surgical procedure for patients with acute appendicitis: still a long way to go. J Int Med Res 51(7):3000605231183781
St Peter SD, Adibe OO, Juang D, Sharp SW, Garey CL, Laituri CA, Murphy JP, Andrews WS, Sharp RJ, Snyder CL, Holcomb GW 3rd, Ostlie DJ (2011) Single-incision versus standard 3-port laparoscopic appendectomy: a prospective randomised trial. Ann Surg 254(4):586–590. https://doi.org/10.1097/SLA.0b013e31823003b5
Kim SJ, Choi BJ, Jeong W, Lee SC (2016) The feasibility of single-port laparoscopic appendectomy using a solo approach: a comparative study. Ann Surg Treat Res 90(3):164–170
Liu J, Chen G, Mao X, Jiang Z, Jiang N, Xia N, Lin A, Duan G (2023) Single-incision laparoscopic appendectomy versus traditional three-hole laparoscopic appendectomy for acute appendicitis in children by senior pediatric surgeons: a multicenter study from China. Front Pediatr 10(11):1224113
Jiang X, Meng HB, Zhou DL, Ding WX, Lu LS (2013) Comparison of clinical outcomes of open, laparoscopic and single port appendicectomies. Ann R Coll Surg Engl 95(7):468–472
Choi BJ, Byun GY, Hwang SB, Lee SR (2016) Feasibility of single port laparoscopic surgery in patients with perforated appendicitis. J Minim Invasive Surg 19(1):19–24
Kim Y, Lee W (2016) The learning curve of single-port laparoscopic appendectomy performed by emergent operation. World J Emerg Surg 5(11):39
Connell MB, Selvam R, Patel SV (2019) Incidence of incisional hernias following single-incision versus traditional laparoscopic surgery: a meta-analysis. Hernia 23(1):91–100. https://doi.org/10.1007/s10029-018-1853-6
Antoniou SA, García-Alamino JM, Hajibandeh S, Hajibandeh S, Weitzendorfer M, Muysoms FE, Granderath FA, Chalkiadakis GE, Emmanuel K, Antoniou GA, Gioumidou M, Iliopoulou-Kosmadaki S, Mathioudaki M, Souliotis K (2018) Single-incision surgery trocar-site hernia: an updated systematic review meta-analysis with trial sequential analysis by the Minimally Invasive Surgery Synthesis of Interventions Outcomes Network (MISSION). Surg Endosc 32(1):14–23
Barutcu AG, Klein D, Kilian M, Biebl M, Raakow R, Pratschke J, Raakow J (2020) Long-term follow-up after single-incision laparoscopic surgery. Surg Endosc 34(1):126–132
Lee GR, Kim JH, Kim CH, Lee YS, Kim JJ (2021) Single-incision laparoscopic appendectomy is a safe procedure for beginners to perform: experience from 1948 cases. Surg Endosc 35(6):2997–3002
Acknowledgements
Study conception and design: R.C. and M.C.C.; Acquisition of data: L.A. and S.A.; Analysis and interpretation of data: M.B. and G.D.T.; Drafting of manuscript: N.V., R.I., and V.M.D.R.; Critical revision of manuscript: A.S., R.C., A.M. and L.P.
Funding
Open access funding provided by Università degli Studi di Perugia within the CRUI-CARE Agreement. This research received no external founding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Roberto Cirocchi, Maria Chiara Cianci, Lavinia Amato, Luca Properzi, Massimo Buononato, Vanessa Menganelli, Giovanni Domenico Tebala, Stefano Avenia, Ruggero Iandoli, Alberto Santoro, Nereo Vettoretto, Riccardo Coletta and Antonio Morabito have no conflicts of in interests or financia ties to disclosure.
Informed consent and ethical approval
Informed consent and ethical approval statement were not necessary for this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cirocchi, R., Cianci, M.C., Amato, L. et al. Laparoscopic appendectomy with single port vs conventional access: systematic review and meta-analysis of randomized clinical trials. Surg Endosc 38, 1667–1684 (2024). https://doi.org/10.1007/s00464-023-10659-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-023-10659-w