
Abstract
Background
Lower socioeconomic status (SES) is associated with lower academic achievement; however, this relationship is understudied in children with chronic kidney disease (CKD). This study examined the relationship between SES and academic performance in children and adolescents with CKD.
Methods
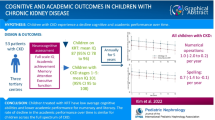
A total of 377 participants aged 6–18 years with CKD stages 1–5 (n = 199), on dialysis (n = 43) or with a kidney transplant (n = 135) were recruited. Five SES measures and a composite SES index were examined for associations with parent-rated average or above average academic performance in numeracy and literacy using multivariable logistic regression.
Results
Participants’ median age was 12.6 years (IQR 8.9–15.5). Adjusted odds ratios (aOR) (95%CI) for better performance in numeracy and literacy, respectively, were 0.71 (0.44–1.15) and 0.75 (0.45–1.23) for children whose caregivers had lower educational attainment; 0.46 (0.26–0.80) and 0.53 (0.30–0.93) for lower household income; 0.52 (0.32–0.85) and 0.44 (0.26–0.73) for caregivers who were unemployed; 0.68 (0.41–1.12) and 0.59 (0.35–1.00) for caregivers with poor self-rated financial status; and 0.93 (0.53–1.64) and 1.00 (0.56–1.79) for caregivers who did not own their own home. Compared with the highest SES index quartile, the aORs for better performance by SES quartile in descending order were 1.24 (0.60–2.54), 0.76 (0.37–1.58), and 0.39 (0.18–0.86) for numeracy and 0.88 (0.41–1.85), 0.77 (0.35–1.66), and 0.32 (0.14–0.72) for literacy. No interactions were identified between SES and CKD stage, child age, or gender.
Conclusions
Across all CKD stages, children from lower SES families are less likely to perform well in literacy and numeracy than those from higher SES households.
Graphical abstract
A higher resolution version of the Graphical abstract is available as Supplementary information

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Children and adolescents with chronic kidney disease (CKD) experience reduced survival, growth, and quality of life outcomes compared to children in the general population [1,2,3,4]. Children with CKD also experience cognition deficits in global cognition as well as the specific domains of executive function, attention, and memory [5]. Reduced academic performance is also observed in children with CKD, particularly for numeracy, reading, and spelling, with children treated with maintenance dialysis most affected [5, 6]. In addition to potential biological causes such as uremia, chronic anemia, hypertension, and reduced cerebral blood flow, other contributors may include missed school days and extra-curricular opportunities because of medical appointments, ongoing hospitalization, and long treatment duration with hemodialysis taking up to 60% of their school contact time [7,8,9]. Furthermore, the educational achievement gap observed in children with CKD may be further exacerbated by other social and economic factors.
Socioeconomic environments are associated with children’s academic achievement and educational attainment in the general population [10, 11]. This may be mediated by factors such as child health and nutrition, parenting styles, parental mental health, living conditions, and access to cognitively stimulating environments [12,13,14]. Academic achievement and educational attainment are important outcomes as they have critical impacts on later health and socioeconomic flourishing [10, 11]. In children with mild to moderate CKD, lower household income and maternal education have been associated with poorer academic achievement [15]. However, the association of family socio-economic status (SES) with academic performance has not been examined across the full spectrum of CKD. Understanding how socioeconomic factors influence educational outcomes in children with CKD is important as these children are already at an academic disadvantage, and factors that may compound this need to be identified to inform targeted interventions. We aimed to examine the association of socioeconomic disadvantage across multiple SES indicators with parent-rated educational outcomes in numeracy and literacy among children and adolescents with CKD, and to determine whether the association between SES and educational outcomes is modified by CKD stage.
Methods
Study design and population
This was a cross-sectional analysis of baseline data from the Kids with CKD (KCAD) study [16]. The KCAD study is a cohort study which takes a life-course approach to examine social and biological determinants of health and wellbeing among children and adolescents with CKD. The KCAD study design and methods have been detailed in the protocol and in previous publications [16,17,18]. From January 2012 to September 2016, families with a child aged 6–18 years with stages I–V CKD, on dialysis, or with a kidney transplant, were recruited through five of eight pediatric nephrology units in Australia and New Zealand. Participants were excluded if they were from families where no one spoke English, if informed consent could not be obtained from caregivers, or if the child was not undertaking formal education.
The Human Research Ethics Committee (HREC) approved this study at all participating centers (The Children’s Hospital at Westmead and Sydney Children’s Hospital (HREC/12/SCHN/159), Lady Cilento Children’s Hospital (HREC/12/QCRH/113), the Royal Children’s Hospital (Royal Children’s Hospital Human Research Ethics Committee: 33229) and Starship Children’s Hospital (New Zealand Health and Disability Ethics Committees: 15/NTB/37). Written informed consent (or assent depending on participant age) was obtained from all participants and/or caregivers.
Exposures
A range of socioeconomic variables were collected as part of the key exposures of the KCAD study, through a self-reported questionnaire completed by the child’s caregiver. For this study, we assessed five measures of SES as exposures similar to our previous publication [16]: educational attainment (defined as primary school or secondary school or trade certificate versus other certificate/diploma or bachelor’s degree or higher education or other education (specification of “other” required in free text section)), gross household income (defined as below versus above the Australian median of $1,250 AUD per week or the New Zealand equivalent), employment status (defined as unemployed versus employed), home ownership (defined as owning a property with or without a mortgage: yes versus no), and perceived financial status, a subjective measure of financial deprivation [16, 19]. For perceived financial status, caregivers were questioned: “Given your current needs and financial responsibilities, would you say that you and your family are (1) Prosperous; (2) Very comfortable; (3) Reasonably comfortable; (4) Just getting along; (5) Poor; or (6) Very poor?”. This variable was dichotomized into (“just getting along”/ “poor”/ “very poor”) compared to (“reasonably comfortable”/ “very comfortable”/ “prosperous”). Consistent with our earlier publication [16], we also examined a global SES variable, a composite measure of the aforementioned SES factors. The global SES variable was generated using principal component analysis (PCA), a data reduction technique which compresses correlated variables into a smaller number of components with minimum loss of information. PCA was applied to all five individual SES variables (with > 10% contributions) to calculate a composite global SES index score [20]. Results of the PCA including the correlation matrix and component eigenvalues used to determine the global socioeconomic index scores can be found in a previous publication [16]. The global SES score was categorized into quartiles for analysis, with the highest quartile reflecting the highest SES.
Outcome
Academic performance in numeracy and literacy was measured by parent-rated performance in Mathematics and English. Caregivers were asked: “Would you say your child’s performance in Mathematics is: well-below average, below average, average, above average?”. This question was repeated for the subject English. Parent-rated academic performance using a similar Likert scale has been shown to have moderate to large correlations with objective measures of academic performance (r is above 0.5) [21]. Other research exploring the precision of parental estimates of child test results also indicate moderate-high correlations with actual test results (r is above 0.5) [22,23,24].
Covariates
Questionnaires were used to collect caregiver and child demographics including child age, sex, date of diagnosis with CKD, cause of CKD, CKD stage, learning difficulties, intellectual disability, ethnicity, postcode, private health insurance, and caregiver age, sex, marital status, and health. Medical information including cause and stage of CKD, medication, and comorbidities were collected through questionnaires and cross-checked with patients’ electronic medical records. Postcodes were used to classify the remoteness of participant locations using Australian Bureau of Statistics Remoteness Structure and the New Zealand Statistical Standard for Geographical Areas [25]. Australian major cities and New Zealand major urban areas were coded as “urban” with remaining cities being coded as “other” [26]. A validated subjective measure of overall health was used to measure caregiver health, with caregivers being asked: “In general, would you say your health is: poor, fair, good, very good, excellent?” [27,28,29]. Categorical variables with few cases were dichotomized into binary variables, including ethnicity (Caucasian versus non-Caucasian), child comorbidities (yes versus no), caregiver heath (poor/fair versus good/very good/excellent), and caregiver marital status (married/de-facto versus other).
Analytical approach
All analyses were undertaken using R v3.6.3. Demographic characteristics were summarized as median (interquartile range (IQR)) for continuous variables and number (percentage) for categorical variables. To examine the association between SES and parent-rated academic performance, separate multivariable logistic regression models were fitted for each exposure: global SES index derived using PCA [16], education, income, employment status, home ownership, and perceived financial status. Due to small numbers for some categories, the 4-point Likert scale used to measure academic performance was collapsed to a binary variable: well-below average/below average versus average/above average (Supplementary Table 1). Covariate selection was based on an assumed causal model, informed by prior literature and expert knowledge and represented in a directed acyclic graph (DAG) (Supplementary Fig. 1). The variables CKD stage (coded as: stages I–V, dialysis, or transplant), child age, child gender, child ethnicity, caregiver age, caregiver marital status, and geographical location were included as forced covariates in all SES models on the basis of being known potential confounders. We also conducted sensitivity analyses adding in variables that may potentially act as mediators in addition to being potential confounders (comorbidities, cause of CKD, duration of CKD, private health insurance, and caregiver health). These variables were not included in the main models due to the risk of underestimating SES effects by controlling for potential mediators [30]. For the main models, we also assessed for interactions between the SES measure and the potential effect modifiers of CKD stage, child age, and child gender, using likelihood ratio tests. Where significant interactions were identified, we stratified the model by the effect modifier. For the association analysis, a p-value < 0.05 was considered statistically significant, and interaction analyses with p-value of p < 0.1 were explored. Given that there were 5 different SES measures, we applied Bonferroni corrections to account for multiple comparisons between CKD stage, gender, and age resulting in a new corrected \(\alpha\)-level of 0.006 for the interaction analyses. Observations with missing values were excluded from the models (percentage missing ranged between 13 and 17%).
Results
Participant characteristics and exposures
Of 528 eligible children and caregivers invited to take part in the study, 377 (71%) consented to participate (Fig. 1). Characteristics of the children and their caregivers are outlined in Table 1. The median age of the children was 12.6 years (IQR 8.9–15.5), 233 (62%) were male, and 220 (58%) were Caucasian. Most of the children had CKD stages I–V (n = 199, 53%), while 11% (n = 43) were on dialysis, and 36% (n = 135) had a kidney transplant. The average time since diagnosis with CKD was 8.2 years (SD: 5.1) and the most common cause of CKD was congenital anomalies of the kidney and urinary tract (n = 127, 34%). Almost two-thirds of the cohort had at least one comorbidity (n = 242, 64%) with the most common being hypertension (n = 120, 32%), followed by growth deficiency (n = 58, 21%), and behavioral issues (n = 58, 15%). Mild to severe caregiver-reported learning difficulties and intellectual disability were reported for 115 (30.5%) and 51 (13.5%) children and adolescents, respectively. The majority of the cohort resided in urban locations (n = 262, 70%), while only 36% (n = 135) had private health insurance. Among primary caregivers, the median age was 43.3 years (IQR 38.9–48.2) and 20% (n = 77) were single.

Recruitment and selection process
In terms of SES, 41% of primary caregivers (n = 156) were unemployed and 49% (n = 183) had weekly household income below $1,250. Over half had a non-trade certificate/diploma qualification, or bachelor’s degree or higher tertiary education, or other education (described by caregivers as “tertiary”) (n = 215, 57%), and around two-thirds owned a property either outright or with a mortgage (n = 255, 68%). For perceived financial status, 45% were comfortable to prosperous (n = 171). The majority of caregivers reported good to excellent health (n = 324, 86%). As expected, compared to caregivers of lower global SES, those in the highest SES quartile were more likely to be employed (n = 85, 100%), have higher education (n = 66, 77%), perceive themselves as comfortable to prosperous (n = 85, 100%), have private health insurance (n = 49, 58%), and have higher weekly household income (n = 85, 100%).
Academic performance outcomes
Overall, parent-rated performance in numeracy and literacy was reported for 347 (92%) and 346 (92%) children, respectively. In the highest SES quartile, the proportion of parents rating their child’s performance as average or above was 59% for numeracy (n = 50) and 65% (n = 55) for literacy. The proportion of children with average or above average academic performance in the lowest SES quartile for numeracy was 50% (n = 43) and literacy was 55% (n = 47).
Table 2 displays academic performance across stages of CKD with additional stratification across stages I–II and III–V. The proportion of children with average or above average performance in numeracy and literacy, respectively, was 77% (n = 82) and 79% (n = 85) for those with CKD stages I–II; 58% (n = 53) and 58% (n = 53) for those with CKD stages III–V; 49% (n = 21) and 58% (n = 25) for those on dialysis; and 59% (n = 79) and 50% (n = 67) for children with a transplant.
Associations between family socioeconomic disadvantage and parent-rated academic performance
Figure 2 shows the association between SES measures and performance in numeracy and literacy adjusted for child age, CKD stage, ethnicity, gender, caregiver age, caregiver marital status, and geographic location. With reference to children from higher SES backgrounds, adjusted ORs (95%CI) for average or above average academic performance among children whose caregivers reported lower education level, lower household income, not being in paid employment, poorer financial status, and lack of home ownership were (i) 0.71 (0.44–1.15), 0.46 (0.26–0.80), 0.52 (0.32–0.85), 0.68 (0.41–1.12), and 0.93 (0.53–1.64), respectively, for numeracy, and (ii) 0.75 (0.45–1.23), 0.53 (0.30–0.93), 0.44 (0.26–0.73), 0.59 (0.35–1.00), and 1.00 (0.56–1.79), respectively, for literacy. With reference to the highest global SES quartile, adjusted ORs (95%CI) for average or above average performance by SES quartile in descending order were 1.24 (0.60–2.54), 0.76 (0.37–1.58), and 0.39 (0.18–0.86) for numeracy, and 0.88 (0.41–1.85), 0.77 (0.35–1.66), and 0.32 (0.14–0.72) for literacy.

Associations between family socioeconomic disadvantage and parent-rated academic performance in numeracy and literacy. Each odds ratio is from a separate regression, adjusted for child age, CKD stage, ethnicity, gender, caregiver age, caregiver marital status, and geographic location. The overall SES index was derived from a principal component analysis on all 5 individual socioeconomic measures to form a composite global SES index, as described in “Methods.” It was a continuous variable that was categorized into quartiles for the regression models, with quartile 4 (highest SES) treated as the reference. In order from top to bottom, reference categories for the individual SES measures are: higher education level (other certificate or diploma/bachelor’s degree or higher/other education), higher income (> $1250 AUD/week), any employment, better financial status (comfortable to prosperous), and home ownership (owned outright/mortgage)
Interactions between SES and child CKD stage, age, and sex
There were no significant interactions between the six different SES measures and the variables of CKD stage, age group, or sex after accounting for multiple testing and comparisons.
Sensitivity analyses
Results for the regression models were similar when adjusted for additional covariates that could act as potential mediators including comorbidities, cause of CKD, duration of CKD, private health insurance, and caregiver health (Table 3). With reference to children from higher SES backgrounds, adjusted ORs (95%CI) for better academic performance among children whose caregivers reported lower education level, lower household income, not being in paid employment, poorer financial status and lack of home ownership were as follows: 0.72 (0.42–1.21), 0.49 (0.27–0.89), 0.52 (0.30–0.89), 0.73 (0.42–1.27), and 0.85 (0.46–1.57) for numeracy, and 0.77 (0.45–1.31), 0.48 (0.26–0.89), 0.39 (0.22–0.68), 0.53 (0.30–0.95), and 0.85 (0.46–1.57) for literacy. With reference to the highest SES index quartile, adjusted ORs (95%CI) for better performance by SES quartile in descending order were 1.02 (0.48–2.17), 0.65 (0.30–1.41), and 0.37 (0.15–0.87) for numeracy, and 0.66 (0.30–1.46), 0.55 (0.24–1.24), and 0.25 (0.10–0.62) for literacy.
Discussion
This study, of nearly 400 children representing all stages of CKD from the majority of pediatric nephrology centers in Australia and New Zealand, indicates that family SES is strongly and consistently associated with academic performance. Across the entire spectrum of CKD stages, children from the lowest quartile of the global SES index were around 60–70% less likely to perform well (average to above average) in numeracy and literacy compared to those from the highest SES quartile. CKD stage, age, and sex of the child did not appear to modify the relationship between SES and academic performance. Key individual drivers of poorer academic performance across SES domains included lower household income, lack of employment, lower self-perceived financial status, and lower education for the primary caregiver.
Research in the general population indicates that children from lower SES families are at risk of reduced academic achievement [14]. They are more likely to experience multiple stressors including poorer nutrition and health, and higher levels of stressful life events which can impact their brain development and key cognitive skills that underpin academic learning, such as problem-solving, working memory, planning, and attention [31,32,33,34]. However, the relationship between SES and academic performance has not been evaluated among children across the full spectrum of CKD. Previous research is limited to stages 3–5 CKD and suggests an association between income and maternal education and academic achievement [15]. Our research extends to children from all stages of CKD including those on kidney replacement therapy (KRT) and examines multiple measures of SES and confounders. We found that SES is associated with poorer achievement among children with CKD, which appeared to be driven largely by a threshold effect involving poorer performance for children in the lowest SES quartile. The lack of interactive effects by CKD stage suggested that socioeconomic disadvantage is equally detrimental to achievement for all children irrespective of the chronicity and severity of kidney disease. These findings are concerning given existing evidence that children with CKD may already have lower than average cognitive abilities and academic performance, with deficits in academic skills, executive function, and visual and verbal memory [5]. Our findings indicate that socioeconomic disadvantage may have additive, pervasive, detrimental effects on academic performance compared to having kidney disease alone.
As SES is a multidimensional construct, individual socioeconomic domains may vary in the strength of their association with academic achievement, and may influence academic outcomes via different mechanisms [12]. In our study, income and employment status showed the strongest associations with academic achievement in children with CKD. This association is consistent with previous research showing that income and employment are both considered markers of material resources [35]. Families with high income and employment may have more resources to support educational needs such as home schooling and tutoring, particularly for children with a chronic illness such as CKD where school absence is common [9, 36]. In contrast, no association was found for caregiver education and academic performance. Evidence from the general population has indicated that caregiver education is a strong predictor of academic performance [14, 37], which has been attributed to factors such as household literacy, caregiver teaching styles, and investment in educational resources [33]. The reasons for our finding are unclear, but may reflect the severity of the chronic illness and its long-lasting, persistent effects on life participation including schooling and education, irrespective of the education status and qualification of parents. Similarly, home ownership was not associated with academic performance in our cohort. Prior research has found that housing is a predictor for academic achievement, particularly for children from low SES backgrounds [37, 38]. Provision of a safe, affordable, stable, and quiet environment is a key strategy suggested for improving education outcomes among children living in poverty [39]. However, details and granularity of these constructs were not examined in our study, but should be a priority for future research.
Given the importance of childhood education for future SES, educational attainment, and health [10, 11], academic interventions should target children with CKD from low SES, with the goal of developing active, robust, and sustainable strategies to monitor progress and promote positive educational outcomes. Ongoing dialogue between caregivers, children, and clinicians, as well as teachers and education support staff is essential in setting attainable goals, particularly as priorities for outcomes can vary between these stakeholders [40]. Formal policies should be implemented to encourage communication in a proactive manner with a focus on prevention (rather than predominantly reactive or ad hoc practices) to ensure children are not precluded from learning opportunities due to factors such as school absences [41]. Strategies may include establishing appropriate electronic and remote leaning support, in addition to caregiver assistance with provision of resources and additional tutoring support. A previous review of academic interventions targeting children from low SES backgrounds found that tutoring, feedback and progress monitoring, and cooperative learning were effective, whereas other strategies including mentoring school personnel, increased resources, and incentive programs required further research [42]. The authors noted that they were unable to explain why some interventions were more effective than others, highlighting that the impact of an intervention will depend on local context. This reinforces that interventions would need to be modified to consider the impact CKD has both on children and their caregivers. To inform interventions, future research should further investigate the relationship between SES and academic performance in children with CKD with a focus on potential mediators. Aside from child health and the physical home environment, cognitive stimulation at home and parenting styles have been suggested to be key mediators between SES and child intellectual development [43].
This study had a number of strengths. Firstly, it was a large, multi-center study including children with varied SES backgrounds across all stages of CKD from 5 out of 8 pediatric nephrology units in Australia and New Zealand. SES is a multi-dimensional construct, and in the general population its associations with academic performance vary in strength across different SES domains [12]. As such, the use of numerous socioeconomic measures and the creation of a global composite index to examine the overall effects of SES across multiple domains is a major strength of this study [20]. We also included a number of potential confounders in our analyses, and built a separate model for variables that could act as mediators in order to avoid overadjustment bias. There are, however, some potential limitations. Given the observational and cross-sectional nature of the study, the impact of SES on academic performance over time could not be assessed, and there is a risk of residual confounding. The outcome measures, literacy and numeracy performance were measured subjectively via caregiver report, not actual test results, which may have introduced some measurement bias. However, similar measures have been shown to be associated with objective measures of academic performance [21]. For the SES exposures, education level and employment status were analyzed for only the primary caregiver, not for other caregivers, and household income was not adjusted for the number of household members, potentially underestimating their effects. There is a risk of selection bias as non-English speaking participants were excluded and 20% of eligible families refused to participate for unspecified reasons which may limit the generalisability of the results. Details on the granularity of comorbidities, premature births, and type and duration of dialysis before transplant were not collected and so the impact of these factors could not be examined. Finally, as the sample size of children on dialysis was small, our analysis may have been limited in its power to detect potential interactions with CKD stage.
Overall, these findings suggest that across illness severity, children with CKD from low SES backgrounds have poorer performance in numeracy and literacy than children who are more socioeconomically advantaged. Given the importance of educational outcomes for future health and socioeconomic attainment, there is a need for interventions targeted towards improving academic performance in children with CKD who are experiencing concurrent socioeconomic disadvantage. Further investigation into the relationship between SES and academic performance among children with CKD should systematically identify potential mediating factors to inform the development of academic interventions.
References
Lopes M, Ferraro A, Koch V (2014) Health-related quality of life of children and adolescents with CKD stages 4–5 and their caregivers. Pediatr Nephrol 29:1239–1247
Kari J (2012) Epidemiology of chronic kidney disease in children. J Nephropathol 1:162–163
Bell LE, Ferris ME, Fenton N, Hooper SR (2011) Health care transition for adolescents with CKD—the journey from pediatric to adult care. Adv Chronic Kidney Dis 18:384–390
Kaufman M, Shemesh E, Benton T (2010) The adolescent transplant recipient. Pediatr Clin North Am 57:575–592
Chen K, Didsbury M, van Zwieten A, Howell M, Kim S, Tong A, Howard K, Nassar N, Barton B, Lah S, Lorenzo J, Strippoli G, Palmer S, Teixeira-Pinto A, Mackie F, McTaggart S, Walker A, Kara T, Craig JC, Wong G (2018) Neurocognitive and educational outcomes in children and adolescents with CKD: a systematic review and meta-analysis. Clin J Am Soc Nephrol 13:387
Moser JJ, Veale PM, McAllister DL, Archer DP (2013) A systematic review and quantitative analysis of neurocognitive outcomes in children with four chronic illnesses. Paediatr Anaesth 23:1084–1096
Tjaden L, Tong A, Henning P, Groothoff J, Craig JC (2012) Children’s experiences of dialysis: a systematic review of qualitative studies. Arch Dis Child 97:395
Lum A, Wakefield CE, Donnan B, Burns MA, Fardell JE, Marshall GM (2017) Understanding the school experiences of children and adolescents with serious chronic illness: a systematic meta-review. Child Care Health Dev 43:645–662
Richardson KL, Weiss NS, Halbach S (2018) Chronic school absenteeism of children with chronic kidney disease. J Pediatr 199:267–271
Cutler DM, Lleras-Muney A, Vogl T (2011) Socioeconomic status and health: dimensions and mechanisms. In: Glied S, Smith P (eds) The Oxford Handbook of Health Economics. Oxford University Press, Oxford, pp 124–163
Backlund E, Sorlie PD, Johnson NJ (1999) A comparison of the relationships of education and income with mortality: the national longitudinal mortality study. Soc Sci Med 49:1373–1384
Bradley RH, Corwyn RF (2002) Socioeconomic status and child development. Annu Rev Psychol 53:371
Blanden J, Gregg P (2004) Family income and educational attainment: a review of approaches and evidence for Britain. Oxf Rev Econ Policy 20:245–263
Sirin SR (2005) Socioeconomic status and academic achievement: a meta-analytic review of research. Rev Educ Res 75:417–453
Harshman LA, Johnson RJ, Matheson MB, Kogon AJ, Shinnar S, Gerson AC, Warady BA, Furth SL, Hooper SR (2019) Academic achievement in children with chronic kidney disease: a report from the CKiD cohort. Pediatr Nephrol 34:689–696
Didsbury M, van Zwieten A, Chen K, James L, Francis A, Kim S, McTaggart S, Walker A, Mackie F, Kara T, Prestidge C, Teixeira-Pinto A, Barton B, Lorenzo J, Lah S, Howard K, Nassar N, Au E, Tong A, Craig J, Wong G (2019) The association between socioeconomic disadvantage and parent-rated health in children and adolescents with chronic kidney disease—the Kids with CKD (KCAD) study. Pediatr Nephrol 34:1237–1245
Francis A, Didsbury MS, van Zwieten A, Chen K, James LJ, Kim S, Howard K, Williams G, Bahat Treidel O, McTaggart S, Walker A, Mackie F, Kara T, Nassar N, Teixeira-Pinto A, Tong A, Johnson D, Craig JC, Wong G (2019) Quality of life of children and adolescents with chronic kidney disease: a cross-sectional study. Arch Dis Child 104:134
Wong G, Medway M, Didsbury M, Tong A, Turner R, Mackie F, McTaggart S, Walker A, White S, Howard K, Kim S, Craig J (2014) Health and wealth in children and adolescents with chronic kidney disease (K-CAD study). BMC Public Health 14:307
Cole K, Daly A, Mak A (2009) Good for the soul: the relationship between work, wellbeing and psychological capital. J Soc Econ 38:464–474
Vyas S, Kumaranayake L (2006) Constructing socio-economic status indices: how to use principal components analysis. Health Policy Plan 21:459–468
Maguin E, Loeber R (1996) How well do ratings of academic performance by mothers and their sons correspond to grades, achievement test scores, and teachers’ ratings? J Behav Educ 6:405–425
Delgado-Hachey M, Miller SA (1993) Mothers’ accuracy in predicting their children’s IQs: its relationship to antecedent variables, mothers’ academic achievement demands, and children’s achievement. J Exp Educ 62:43–59
Hunt JM, Paraskevopoulos J (1980) Children’s psychological development as a function of the inaccuracy of their mothers’ knowledge of their abilities. J Genet Psychol 136:285–298
Miller SA (1986) Parents’ beliefs about their children’s cognitive abilities. Dev Psychol 22:276–284
Australian Bureau of Statistics (2017) Correspondence, 2017 Postcode to 2016 Remoteness Area . Australian Statistical Geography Standard (ASGS) - Volume 5. https://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/1270.0.55.005July%202016?OpenDocument. Accessed 1 January 2021
Statistics New Zealand (2020) Urban Rural 2020 (generalised) . Statistical Standard for Geographic Areas 2018. https://datafinder.stats.govt.nz/layer/104269-urban-rural-2020-generalised/. Accessed 1 January 2021
DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P (2006) Mortality prediction with a single general self-rated health question: a meta-analysis. J Gen Intern Med 21:267–275
Franks P, Gold MR, Fiscella K (2003) Sociodemographics, self-rated health, and mortality in the US. Soc Sci Med 56:2505–2514
Bowling A (2005) Just one question: if one question works, why ask several? J Epidemiol Community Health 59:342–345
Schisterman EF, Cole SR, Platt RW (2009) Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology 20:488–495
Luby J, Belden A, Botteron K, Marrus N, Harms MP, Babb C, Nishino T, Barch D (2013) The effects of poverty on childhood brain development: the mediating effect of caregiving and stressful life events. JAMA Pediatr 167:1135–1142
Hanson JL, Chandra A, Wolfe BL, Pollak SD (2011) Association between income and the hippocampus. PLoS One 6:e18712
Institute of Medicine and National Research Council (2000) From neurons to neighborhoods: the science of early childhood development. The National Academies Press, Washington, DC
Noble KG, Houston SM, Kan E, Sowell ER (2012) Neural correlates of socioeconomic status in the developing human brain. Dev Sci 15:516–527
Duncan GJ, Brooks-Gunn J, Klebanov PK (1994) Economic deprivation and early childhood development. Child Dev 65:296–318
Brooks-Gunn J, Klebanov PK, Liaw F-R (1995) The learning, physical, and emotional environment of the home in the context of poverty: the Infant Health and Development Program. Child Youth Serv Rev 17:251–276
Considine G, Zappala G (2002) The influence of social and economic disadvantage in the academic performance of school students in Australia. J Sociol (Melb) 38:129–148
Haurin DR, Parcel TL, Haurin RJ (2002) Does homeownership affect child outcomes? Real Estate Econ 30:635–666
Cunningham M, MacDonald G (2012) Housing as a platform for improving education outcomes among low-income children. Urban Institute, Washington, DC
Hanson CS, Gutman T, Craig JC, Bernays S, Raman G, Zhang Y, James LJ, Ralph AF, Ju A, Manera KE, Teixeira-Pinto A, Viecelli AK, Alexander SI, Blydt-Hansen TD, Dionne J, McTaggart S, Michael M, Walker A, Carter S, Wenderfer SE, Winkelmayer WC, Bockenhauer D, Dart A, Eddy AA, Furth SL, Gipson DS, Goldstein SL, Groothoff J, Samuel S, Sinha A, Webb NJA, Yap H-K, Zappitelli M, Currier H, Tong A (2019) Identifying important outcomes for young people with CKD and their caregivers: a nominal group technique study. Am J Kidney Dis 74:82–94
Poursanidou K, Garner P, Watson A (2008) Hospital - school liaison: perspectives of health and education professionals supporting children with renal transplants. J Child Health Care 12:253–267
Dietrichson J, Bøg M, Filges T, Klint Jørgensen A-M (2017) Academic interventions for elementary and middle school students with low socioeconomic status: A systematic review and meta-analysis. Rev Educ Res 87:243–282
Guo G, Harris KM (2000) The mechanisms mediating the effects of poverty on children’s intellectual development. Demography 37:431–447
Acknowledgements
The authors would like to thank all participating patients, families, and pediatric nephrology centers in their longstanding support of the study. We would also like to acknowledge pediatric nephrologist Dr. Tonya Kara, our colleague and friend, who passed away during the course of the study.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions National Health and Medical Research BEAT-CKD program grant and the Ludwig Engel Research Fellowship. GW is supported by a NHMRC career development fellowship (APP 1147657) and the Investigator Grant (APP1195414).
Author information
Authors and Affiliations
Contributions
RK was responsible for manuscript drafting, data interpretation, and statistical analysis with the assistance of AVZ, SK, JC, and GW. GW was the chief investigator for the study and was responsible for study conceptualisation and design. ATP, EA, and KB provided guidance with statistical analysis and EA assisted with developing study figures. AVZ, MD, JC, AT, GW, AF, SM, FM, CP, and AW contributed to participant recruitment and together with BB, JL, SL, KH, and NN were consulted on study design. RK, AVZ, and MD were responsible for data collection. All listed authors contributed to data interpretation and provided critical feedback on the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Jonathan C. Craig and Germaine Wong are co-senior authors
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Khalid, R., Van Zwieten, A., Kim, S. et al. Association between socioeconomic status and academic performance in children and adolescents with chronic kidney disease. Pediatr Nephrol 37, 3195–3204 (2022). https://doi.org/10.1007/s00467-022-05515-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-022-05515-3