
Abstract
It is acknowledged that climate change exacerbates social inequalities, and women have been reported as more vulnerable to heat than men in many studies in Europe, including the Czech Republic. This study aimed at investigating the associations between daily temperature and mortality in the Czech Republic in the light of a sex and gender perspective, taking into account other factors such as age and marital status. Daily mean temperature and individual mortality data recorded during the five warmest months of the year (from May to September) over the period 1995–2019 were used to fit a quasi-Poisson regression model, which included a distributed lag non-linear model (DLNM) to account for the delayed and non-linear effects of temperature on mortality. The heat-related mortality risks obtained in each population group were expressed in terms of risk at the 99th percentile of summer temperature relative to the minimum mortality temperature. Women were found generally more at risk to die because of heat than men, and the difference was larger among people over 85 years old. Risks among married people were lower than risks among single, divorced, and widowed people, while risks in divorced women were significantly higher than in divorced men. This is a novel finding which highlights the potential role of gender inequalities in heat-related mortality. Our study underlines the relevance of including a sex and gender dimension in the analysis of the impacts of heat on the population and advocates the development of gender-based adaptation policies to extreme heat.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
With climate change, temperatures in Central Europe are expected to rise (IPCC 2021) and heatwaves to be more frequent and intense (Lhotka et al. 2018; IPCC 2021) during the twenty-first century. The latest data from the Met Office Hadley Centre (CCAG 2022) suggested that recent record-breaking European summers of 2018 (Hoy et al. 2020), 2019 (Xu et al. 2020) or 2021 (Lhotka and Kyselý 2022) may become the norm by 2035.
Exposure to high temperatures may affect human health, as it was shown to cause various heat-related illnesses (Székely et al. 2015; Watts et al. 2019) and may ultimately lead to premature death. Increase of mortality during heatwaves was already observed in many studies (Jonsson and Lundgren 2015; Xu et al. 2016), and heat-related mortality was predicted to increase by the end of the century, in particular in Central Europe (Gasparrini et al. 2017). In the Czech Republic, Urban et al. (2022) showed that, despite a decrease in the impacts of heat on mortality in the 1990s and 2000s compared to the 1980s (Kyselý and Kříž 2008; Kyselý and Plavcová 2012), the heat-related mortality risk was twice as high in the 2010s than in the previous three decades in Prague.
Not all humans are impacted the same way by short- and long-term increase in temperatures. In particular, inequalities in heat-related mortality based on sex, describing the biological and physiological characteristics of an individual, and gender, referring to norms, behaviours, values, and preferences considered appropriate by a society for each sex (Charkoudian and Stachenfeld 2014; Tenglerová et al. 2020; WHO 2021; UN High Commissioner for Refugees 2021), have been observed in many studies. Indeed, women were found at higher risk to die as a result of high temperatures in various European countries, such as in France (Canouï-Poitrine et al. 2006), Italy (Stafoggia et al. 2006; Ellena et al. 2020a), Germany (Gabriel and Endlicher 2011), Spain (Achebak et al. 2018; Marí-Dell’Olmo et al. 2019) and Scotland (Wan et al. 2022). In the Czech Republic, a higher mortality increase was observed in women than in men during the hot summer periods of 1982–2000 (Kyselý 2004), as well as during the four heatwaves of 2003 (Kyselý and Kříž 2008). Hůnová et al. (2017) studied the effects of the summer heatwaves of August 2003 and July 2006 on health in Prague and found a higher mortality risk for women than for men. Several studies were conducted on the effects of hot spells on cardiovascular mortality in the Czech Republic (Kyselý et al. 2011; Davídkovová et al. 2014; Hanzlíková et al. 2015) or regions of the country (Urban et al. 2016) and also found higher excess mortality in females than in males.
Yet, individuals cannot be characterised by their sex and gender only, and a multitude of other criteria, such as age or socioeconomic factors, could be taken into account. Advanced age was identified as an important driver of heat vulnerability (Hajat et al. 2007; Yu et al. 2010; Kenny et al. 2010; Arbuthnott and Hajat 2017; Watts et al. 2019; Son et al. 2019; Watts et al. 2021; de Schrijver et al. 2022; Wan et al. 2022), and elderly women were repeatedly found to be particularly vulnerable to high temperatures (Canouï-Poitrine et al. 2006; Hajat et al. 2007; Yu et al. 2010; Ellena et al. 2020a; Wan et al. 2022). As for socioeconomic status, factors such as the level of education (Hondula et al. 2012; Aubrecht and Özceylan 2013; Klein Rosenthal et al. 2014; Huang et al. 2015; Ellena et al. 2020a, 2020b), the marital status (Fouillet et al. 2006; Gronlund et al. 2015; Ellena et al. 2020a, 2020b; Wan et al. 2022), or the household structure (Seebaß 2017, Ellena et al. 2020a, 2020b) were sometimes found to be modifiers of heat effects.
Understanding differences in population exposure and vulnerability to heat conditions seems to be essential to develop relevant adaptation policies (Putnam et al. 2018). Considering the existing sex and gender inequalities in the society, integrating a sex and gender dimension into the analysis and the discussion is necessary to avoid concealing and to understand the differential impacts of heat on men and women. To date, no study investigated heat-related mortality in the Czech Republic with a primary focus on sex and gender, including combinations of sex with other criteria, such as marital status, as potential drivers of heat vulnerability.
The objective of this study was to quantify heat-related mortality and to identify potential sex and gender inequalities in heat vulnerability in the Czech Republic over the period 1995–2019 (25 years). Hence, differentiated analyses were conducted for men and women, and these categories were also studied while interlinked with the age category and the marital status. Ultimately, the fraction and number of deaths attributable to heat were evaluated in order to account for the actual burden of heat in the total mortality of each population group.
Methods
Study design and data
The study period extended from January 1, 1995, to December 31, 2019, for a total of 25 years, although only the five warmest months of the year (from May 1 to September 30, hereafter called “summer months”) were used in the analysis to focus on the highest temperatures. The study area was the Czech Republic, a 79,000 km2-wide country located in Central Europe, whose population size was relatively constant over the study period (10.3 million inhabitants in 1995 to 10.7 million in 2019) ([dataset] CZSO, Czech Statistical Office 2021). The analysis was chosen to be performed at the scale of the country rather than region- or city-wide, as it was shown that considering areas less populated than Prague in the Czech Republic would not give a robust and significant assessment of the heat-related mortality (Urban et al. 2016). Moreover, as pointed out by Urban et al. (2020), the Czech population is comparable to those of the largest European urban areas (e.g. Paris, London) and most of the Czech population lives within the same climate zone; hence, a nation-wide analysis would provide results comparable to studies from largest European cities.
In order to study the associations between heat and mortality, two types of time series were used: daily mortality and daily average temperature in the country.
The records of individual deaths were provided by the Institute of Health Information and Statistics of the Czech Republic (UZIS) and the Czech Statistical Office (CZSO). A total of 1,079,302 deaths were recorded during the summer months of the study period and were aggregated into daily mortality data. The data was divided by sex as a binary variable: “F” (female) and “M” (male). These two categories were further divided by age and by marital status, according to the following sub-categories: “0–64”, “65–74”, “75–84”, and “85+” for age, and “MAR” (married), “DIV” (divorced), “SIN” (single), and “WID” (widowed) for marital status. No distinction was made between heterosexual marriage and registered partnership in the data (same-sex couples are only entitled to registered partnership since 2006). As the number of deceased involved in registered partnerships (whether married, divorced, or widowed) accounted for less than 0.01% of the data, the results on marital status were analysed and discussed within the scope of heterosexuality only. Marital status was used as an indicator of the individual socioeconomic status; other indicators were not available in the original dataset, because they were either not recorded (i.e. household structure, income) or corrupted (i.e. level of education).
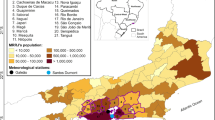
As for temperature, the Czech Hydrometeorological Institute (CHMI) provided records of the daily mean temperature during the study period from 14 stations spread across the Czech Republic (Fig. 1). A similar set of stations was used in previous studies analysing the impact of temperature extremes on mortality in Czech Republic (Kyselý and Kříž 2008; Urban et al. 2017). The temperature records were averaged over the stations to account for the daily mean temperature in the whole country.

Map of the Czech Republic indicating the location of the 14 meteorological stations that provided the daily mean temperature used in this study and the major urban areas
Statistical analysis
The statistical analysis was performed using a time series regression. A generalized linear model (GLM) was applied separately on each population group to estimate group-specific temperature-mortality associations. The error was chosen to follow a quasi-Poisson distribution (Wedderburn 1974), particularly adapted to overdispersed count variables such as mortality (Istiana et al. 2020). To take into consideration the delayed and non-linear effects of thermal conditions on mortality, the temperature-mortality association was modelled using a distributed lag non-linear model (DLNM) (Gasparrini et al. 2010). DLNMs consist in introducing in the GLM a cross-basis matrix that combines two functions describing respectively the temperature-mortality and the lag-mortality associations. The temperature-mortality curve was modelled by a quadratic spline with one internal knot placed at the 75th percentile of summer temperature (“percentile of summer temperature” will hereafter be referred to as “percentile”). The lag-mortality curve was controlled by a natural cubic spline with two internal knots equally spaced on the log scale, and the lag period was extended to 14 days. The number and position of knots in the temperature-mortality space as well as the number of lags in the lag-mortality space were chosen after performing a sensitivity analysis (see Supplementary material, Fig. S1). All combinations of number of lags from 7 to 14, and of position of knots (a single knot at the 50th, 75th, and 90th percentiles and two knots at the 50th and 90th percentiles) were tested, and the best model was selected according to the lowest quasi Akaike information criterion (Akaike 1974, Wedderburn 1974, Bolker 2009).
To analyse the short-term associations between temperature and mortality, time series were adjusted for periodic patterns and a long-term trend. The weekly pattern was controlled by the day of the week (DOW), a 7-level factor variable, while the seasonal pattern was controlled by the day of the year (DOY). The DOY was modelled with a natural cubic spline with two degrees of freedom per year. An interaction (denoted as “:” in the formula below) between the spline and the year was also included to allow the degrees of freedom to vary from one year to another. Long-term trend was controlled by a time variable, modelled with a natural cubic spline with two degrees of freedom (one degree per whole decade).
The model design choices were based on models presented in previous papers (Achebak et al. 2018; Ellena et al. 2020a). Using the same algebraic formulation as Ellena et al. (2020a), the final model designed in this study can be described as follows:
where Yt represents the daily count of deaths, E(.) is the expected value, α is the intercept, cb is the cross-basis matrix, and ns is a natural spline.
The effect of a given temperature on mortality was reported as a relative risk (RR), which expressed the ratio between the mortality risk at the temperature under analysis over the mortality risk at a reference temperature. The reference temperature was defined as the minimum mortality temperature (MMT), i.e. as a point estimate of the temperature within a restricted range between the 50th and 90th percentiles, for which the overall exposure-response curve reached the minimum value (analogous to Tobías et al. 2017, but we did not calculate the MMTs’ confidence intervals). To characterize the overall effect of temperature over the whole lag period, the overall temperature-mortality association was computed by aggregating all the contributions of each lag. The overall RR at the 99th percentile (hereafter noted “99th RR”) was chosen to represent the risk of mortality among the selected population groups associated with extreme heat (analogically to Gasparrini et al. 2015, Achebak et al. 2018, Marí-Dell’Olmo et al. 2019, Ellena et al. 2020a, Petkova et al. 2021). A significance analysis was performed in order to assess the mortality risks differences between men and women. The statistical significance of the difference between two 99th RRs was evaluated by an interaction test according to Altman and Bland's formula (Altman 2003; Altman and Bland 2011):
where Z represents the Z-test, E1 and E2 are the log transformations of the 99th RR estimates of the two groups, and SE1 and SE2 are their respective standard errors. The difference between two 99th RRs was considered significant for a p value smaller than 0.05.
Ultimately, the attributable fraction (AF) and attributable number (AN) of deaths, which respectively represent the portion of deaths among all summer deaths of the study period associated with high temperatures and their absolute number (AN = AF * number of all summer deaths), allowed to express the burden of heat-related mortality upon the total mortality. The AFs and ANs among each population group were calculated for days with daily mean temperature larger than the 95th percentile. Although there is no universally accepted heat wave definition in public health studies, the 95th percentile is generally understood as a threshold of a heat wave according to the WHO and WMO Guidance on Warning System Development (McGregor et al. 2015).
All models and calculations were performed on the software R (version 4.1.2), using the package dlnm (version 2.4.7) developed by Gasparrini (2011) and the function attrdl (attributable risk from distributed lag non-linear models) developed by Gasparrini and Leone (2014).
Results
The 19 time series representing daily mortality from 1995 to 2019 in the Czech Republic in different population groups were modelled using DLNMs with quasi-Poisson family distribution. For each population group, RRs were obtained for the whole range of summer temperature and for 0 to 14 days of lag. The AF and AN of each group were also computed. Table 1 provides a summary of the number of deaths, the mean age, the MMT, the 99th RR, the AF and the AN of each population group.
Sex
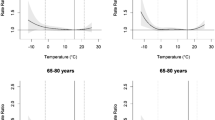
Figure 2 shows different vulnerability to heat between men and women. Indeed, at the 99th percentile, the risks for women were higher than those for men in the first 7 days after exposure, and the mortality displacement was thus larger afterwards (Fig. 2, left). On the whole lag period, the MMT was found lower by 3.8 °C for women (16.2 °C) than for men (20.0 °C). What is more, women presented a higher overall mortality risk than men at temperatures higher than the MMT (Fig. 2, right).

Left: Lag-mortality association between the days of lag and the mortality relative risk (RR) at the 99th percentile of summer temperature (25.5 °C) in the Czech Republic over the period 1995–2019 divided by sex. Right: Overall association between the summer temperature and the mortality relative risk (RR) in the Czech Republic over the period 1995–2019 divided by sex. The purple, orange, and green vertical lines, respectively, represent the minimum mortality temperature (MMT) of women, men, and the total population. The pink vertical line represents the 99th percentile of summer temperature
At the 99th percentile in particular, the 99th RR was significantly higher (p value < 0.01, Figs. 3 and 4) among women (1.25; 95% confidence interval (CI) = 1.21–1.30) than among men (1.16; 95% CI = 1.11–1.20). Sex inequalities in heat vulnerability were also observed through the age and marital status categories. The values of the 99th RRs for women were higher than those for men in five out of eight categories, and those differences were significant for two of them (“85+” and “DIV”). In the three categories for which the 99th RRs were higher for men than for women (“0–64”, “65–74”, and “MAR”), the differences were found insignificant.

Overall relative risk at the 99th percentile of summer temperature (99th RR) in the Czech Republic over the period 1995–2019 divided by population group. Error bars represent the 95% confidence intervals

Heatmaps displaying the p values of interaction tests determining the statistical significance of the relative risks at the 99th percentile of summer temperature differences between men and women in the total population (left), by age group (middle) and by marital status (right). The p values were stratified by thresholds (lower than 1, 0.05, 0.01, 0.001, and 0.0001). The risks difference between two groups was considered significant for p values lower than 0.05. Purple (orange) p values represent population groups for which women (men) obtained a higher mortality risk than men (women)
Age
The risks in each age category presented almost no disparity between men and women, except for the “85+” category (Fig. 3). Indeed, for both sexes, the lowest risks were found among people younger than 75 years old (categories “0–64” and “65–74”). In these two age groups, the 99th RRs were slightly higher for men than for women, but the differences were found insignificant (Fig. 4). For women, the risk grew with age, and the highest risk was found among women older than 85 (1.42; 95% CI = 1.34–1.50). In contrast, the highest risk for men was smaller and was found among men between 75 and 84 (1.25; 95% CI = 1.16–1.34). Women above 85 had a much higher risk than men above 85, and the difference between the 99th RRs of these two categories was significant (p value < 0.01, Fig. 4): 1.42 (95% CI = 1.34–1.50) for women versus 1.18 (95% CI = 1.07–1.30) for men.
Marital status
As for marital status, apart from divorced people, the risks in all the other categories were comparable between men and women (Fig. 3). For both sexes, the lowest risk was obtained among married people, but the 99th RR was slightly higher for married men than for married women: 1.14 (95% CI = 1.03–1.26) and 1.12 (95% CI = 1.04–1.22), respectively, although the difference was found insignificant (Fig. 4). Women had the highest risk when they were divorced (1.40; 95% CI = 1.25–1.56), while men had the highest risk when they were widowed (1.24; 95% CI = 1.14–1.35). Divorced women were found especially vulnerable to heat. Indeed, the 99th RR for divorced women was the second largest among all tested population groups, and it was significantly larger (p value < 0.01, Fig. 4) than for divorced men: 1.40 (95% CI = 1.25–1.56) versus 1.14 (95% CI = 1.03–1.26).
Attributable fractions (AF) and attributable numbers (AN)
The results of AF (Table 1 and Fig. 5) showed that the deaths which occurred during the summer months of the study period among the total population were attributable to heat in 0.70% (95% CI = 0.60–0.79) of the cases. Women were proportionally more affected by heat than men (0.90%; 95% CI = 0.77–1.03 for women versus 0.55%; 95% CI = 0.41–0.68 for men). The smallest AF was found for women younger than 64 (0.27%; 95% CI = 0–0.64) and the highest for women above 85 (1.50%; 95% CI = 1.27–1.72) and divorced women (1.40%; 95% CI = 1.01–1.79). The AFs were found consistent with the 99th RRs as they ranked the categories in the same order in terms of heat vulnerability.

Number of deaths (left) and attributable fraction (AF) (right) by population group in the Czech Republic over the summer months of the period 1995–2019. Error bars represent the 95% confidence intervals
However, ANs (Table 1) provide a different perspective on the overall burden of heat on the total mortality as they show the actual number of deaths attributable to heat between 1995 and 2019, during the summer months. According to the results, more than 7500 (7534; 95% CI = 6468–8602) deaths that occurred among the whole population during the summer months of the study period were attributable to heat. Among them, more women (4762; 95% CI = 4116–5411) died in association to heat than men (3002; 95% CI = 2281–3715). The specific categories for which a large number of deaths was attributable to heat were the widowed women (3314; 95% CI = 2809–3848) and women above 85 years old (2554; 95% CI = 2202–2918).
Discussion
The present study assessed the effects of summer temperatures on mortality in the Czech Republic over 25 years, with results categorised by sex, age, and marital status. The 99th RRs obtained for each category ranged between 1.08 and 1.42, which is in line with similar studies using DLNMs in European countries (Gasparrini et al. 2015; Petkova et al. 2021). Studies conducted in Southern Europe usually obtained higher 99th RRs (Achebak et al. 2018; Marí-Dell’Olmo et al. 2019; Ellena et al. 2020a), which is consistent with warmer climate (Urban et al. 2021).
The results obtained in this study confirmed that heat-related mortality risk differed by analysed category. Our findings validate the already found vulnerability for some specific groups, such as for women in respect to men (Fouillet et al. 2006; Stafoggia et al. 2006; Yu et al. 2010; Gabriel and Endlicher 2011; Huang et al. 2015; Achebak et al. 2018; Marí-Dell’Olmo et al. 2019; Son et al. 2019; Ellena et al. 2020a, 2020b), for elder over young people (Canouï-Poitrine et al. 2006; Hajat et al. 2007; Yu et al. 2010; Kenny et al. 2010; Huang et al. 2015; Arbuthnott and Hajat 2017; Watts et al. 2019; Son et al. 2019; Breil et al. 2021; Wan et al. 2022), and for non-married (i.e. single, divorced, widowed) in respect to married people (Stafoggia et al. 2006; Canouï-Poitrine et al. 2006; Fouillet et al. 2006; Gronlund et al. 2015; Ellena et al. 2020a, 2020b; Wan et al. 2022).
What is more, this study brought new results on heat vulnerability at the intersections of sex with other social categories about a Centre European region. Indeed, with regard to age, the highest risk for men was obtained in the 75–84 category, versus the 85+ category for women. By marital status, men were found to be the most at risk when widowed, while women were found at the highest risk when divorced. The risk obtained for divorced women was significantly higher than for divorced men. As far as we know, this is quite a neglected phenomenon, as a similar finding was only reported in one other study (Ellena et al. 2020a). In the sections below, possible causes of the observed differences in heat vulnerability between individual population groups with a focus on gender and marital status differences are discussed.
Sex and age
Scientific literature suggests that differences in heat vulnerability between sex and age groups might arise from physiological characteristics in thermoregulating abilities between elder men and women. Studies have shown a diminishing ability of thermoregulating the body when growing older (Kenney and Munce 2003) and highlighted the association of advanced age with risk factors such as renal failure, cardiac rhythm disturbance, thrombosis and nervous system dysfunction (McGregor et al. 2015), diabetes, cardiovascular and respiratory diseases (Watts et al. 2019), or the use of medications (Arbuthnott and Hajat 2017). In addition, some studies suggested that women had less capability than men to regulate the temperature of their body under heat stress (Fox et al. 1969; Burse 1979). More recent studies (Charkoudian and Stachenfeld 2014; Yanovich et al. 2020) reported a certain bias and limitations in past research with regard to female thermoregulation and did not find any evidence of a female disadvantage in thermoregulation in situation of exercise or commonly performed activities if factors such as fitness and body size are taken into account. However, as women tend to have in average lower aerobic capacity due to smaller body size, less muscle mass, and more fat mass, they might also be more vulnerable to extreme thermal conditions (Yanovich et al. 2020).
Previous studies found larger vulnerability to heat among people with chronic respiratory and cardiovascular disease (Hajat et al. 2007; Basu 2009; Hanzlíková et al. 2015; Arbuthnott and Hajat 2017), and these findings were confirmed also by the current data (not shown; Vésier 2022). Higher occurrence of chronic disease and poorer health was generally associated with lower socioeconomic levels (Craig 2005; Lawlor and Sterne 2007; Lago et al. 2018; McMaughan et al. 2020). Similarly, although the influence of the socioeconomic level on heat-related mortality was sometimes found insignificant (Urban et al. 2016; Arbuthnott and Hajat 2017; Son et al. 2019), multiple studies (O’Neill et al. 2003; Schwartz 2005; Stafoggia et al. 2006; Basu 2009; Otto et al. 2017; Ellena et al. 2020b; Breil et al. 2021) suggested that low levels of education or low incomes could enhance the vulnerability to heat. Consequently, the larger heat vulnerability of women compared to men may also be partly explained by socioeconomic disparities (Breil et al. 2018).
Such differences might arise from inequalities in the labour market. According to a report by the Czech Statistical Office (CZSO, Czech Statistical Office 2021), the gender pay gap in the Czech Republic was the 5th largest in the European Union in 2018, with men being paid on average 18.9% more than women. This same report also pointed out that women were less professionally active than men, since they were in charge of taking care of children or adults with disabilities in a majority of cases. Women were also more likely to be unemployed (especially when they have children) or to have definite-period or part-time contracts. Consequently, since the pensions’ amount is related to the money earned during active years, female pensioners are disadvantaged: men pensions were about 20% higher than those of women in the Czech Republic in 2010 (Andel 2014). This is in accordance with the fact that among people over 75 years old, 21.6% of women were at risk of poverty or social exclusion in the Czech Republic on average between 2015 and 2019, versus 6.34% of men (Eurostat 2022a).
Therefore, despite living longer, women might be more vulnerable to heat than men due to generally lower quality of life, higher risk of isolation in the last years of their life (our data show that 96% of women in the category 85+ were non-married at the time of death, compared to 59% of men), and general health gap existing between men and women. Indeed, many studies conducted in Europe showed that, despite having a longer life expectancy, women reported more health conditions than men and had proportionally shorter healthy life years (Oksuzyan et al. 2009; Oksuzyan et al. 2010; Dahlin and Härkönen 2013; Romero-Ortuno et al. 2014; Palència et al. 2017). More research is needed to understand the mechanisms underlying this observation, but several hypotheses including biological or behavioural factors (Oksuzyan et al. 2010), lower socioeconomic positions, or the “double burden” of paid work and (unpaid) household work (Dahlin and Härkönen 2013) were raised. This theory is also supported by data (EIGE 2022) on the evolution of the life expectancy and the healthy life years in the Czech Republic between 2004 and 2009 displayed by sex in Fig. 6. It confirmed that the difference by sex in healthy life years was considerably lower than the one in life expectancy (1.7 and 6.2 years on average, respectively, between 2005 and 2019). Hence, elder women were more likely to live more time in a frail state and therefore to be more susceptible to heat.

Evolution of the life expectancy and the healthy life years in the Czech Republic over the period 2004–2019 by sex. The data was provided by the European Institute for Gender Equality (EIGE)
Sex and marital status
The existence of a socioeconomic gap between men and women seems to be especially important when results on heat-related mortality risk according to marital status are considered. In our study, married people were at lower risk of heat-related mortality compared to single, widowed, and divorced. Although widowed people were the oldest among all groups (82 years old, Table 1), single and divorced people were younger than married people (54, 66, and 70 years old, respectively); hence, the largest vulnerability among older population does not fully justify the larger mortality risk of non-married people found in this study.
This was especially true for the group of divorced women. Although they were on average older than divorced men at the time of death (71 and 63 years old, respectively), they were not older than other groups such as widowed women or men (82 and 80 years old, respectively) which yet obtained lower mortality risks. These findings support the hypothesis that differences in heat vulnerability might arise also from other than physiological factors, such as disparities in the respective economic situations of married and non-married people. It was established in numerous studies that married people had lower mortality than non-married people (Hank and Steinbach 2018; Franke and Kulu 2018; Zueras et al. 2020), in that marriage tended to provide a better socioeconomic situation, to encourage healthier behaviours and to prevent from social isolation. Although some studies documented divorced men to be more at risk of health outcomes than divorced women (Hank and Steinbach 2018; Sbarra and Whisman 2022), divorced women were still reporting more health conditions or psychological distress than other women (Haider et al. 2003; Lorenz et al. 2006).
Moreover, as divorced women usually face a larger decrease in their relative income (Symoens et al. 2014; Sbarra and Whisman 2022) and a higher likelihood to obtain the custody of their potential children (Symoens et al. 2014), they are confronted to a larger decline in general living standards than men. In the Czech Republic specifically, 90% of the single adult households with children were run by women in 2013 (CZSO 2015), and on average between 2015 and 2019, 40.8% of the households of one adult with dependent children were at risk of poverty or social exclusion versus 12.28% of the total population (Eurostat 2022b). Consequently, poorer socioeconomic levels, combined with other physiological and demographic factors, may have fostered the larger vulnerability to heat of divorced women.
Limitations
As far as we know, this is the first study investigating the role of individual socioeconomic level on heat-related mortality in the Czech Republic. Our study provides novel findings on heat-related mortality risks with respect to marital status of the deceased and highlights the potential role of gender inequalities in heat-related mortality. Yet, several limitations need to be acknowledged, mostly related to insufficient data availability.
One limitation of the study lies in the country-level design which does not allow for spatial variations of the temperature-mortality relationships and therefore does not necessarily represent associations existing in different regions. Although information about the place of residence of each deceased was available, previous studies for individual cities and regions other than Prague did not usually provide significant and robust results due to small population samples (Urban et al. 2016), and studies comparing Prague with a rural region did not show many significant differences for heat-related mortality (Urban et al. 2014; Urban and Kyselý 2014). In addition, more precise temperature records were not available at the time of the analysis. Indeed, the gridded temperature dataset used in previous Czech studies (Urban et al. 2016; Urban et al. 2020) was only available until 2017, and the station network used in this study was not dense enough to run a proper spatial analysis. Considering the relatively small area and population of the Czech Republic and the fact that the vast majority lives in the same climate zone (Kottek et al. 2006), using the nation-wide mortality data seems to be a reasonable way to obtain robust and statistically significant results compared with those from other studies.
Another limitation is related to the choice of the categories to analyse, which was delimited by the information provided by the individual mortality data. In addition to the date of death, the age, the sex, and the marital status of the deceased which were used in the present study, the original dataset also stated the education level, which would have been a relevant indicator of the socioeconomic level of the deceased. However, because of significant changes in the encoding and recording of this variable in the death records over the study period, the level of education of a large part of the deceased people was classified as “unknown” after 2013 (see Supplementary material, Fig. S2). For this reason, this category was not consistent enough to be included in the analysis. Other information, such as the income, the professional category, or the number of inhabitants in the household, which would be useful for a better understanding of the impact of the socioeconomic level on heat vulnerability, were not recorded. Therefore, marital status was the best available information about the socioeconomic situation of the deceased.
However, even within the selected variables, one needs to interpret their categorisation with caution, as they only provide a simplified view of reality. In particular, it is worth mentioning that the binary differentiation of sex does not allow to account for all the sex and gender identities existing in the population. Similarly, marital status as a legal denomination does not necessarily represent the actual household situation of the deceased. Our results highlight the critical lack of relevant information in the individual mortality datasets and encourage the relevant authorities for collecting data about educational level and other indicators of socioeconomic status for each deceased. Such information would allow a better insight into the role of individual vulnerabilities and (not only) heat-related mortality risks.
Conclusions
In this study, the effects of summer (May–September) daily temperature on mortality in the Czech Republic over the period 1995–2019 were modelled using a quasi-Poisson regression model including a distributed lag non-linear model. The study was conducted with a primary focus on sex and gender inequalities; the analysis was consequently disaggregated between men and women, and both groups were further divided by age and, for the first time in a Czech study, marital status.
This study underlined the higher vulnerability to heat of women compared to men, especially among people over 85 years old and, a quite novel finding, among divorced people. These results were discussed to be driven by combinations of physiological, demographical, and socioeconomic factors. The gender-based health and economic inequalities presented in this study highlight the importance of taking into account these factors when collecting data about mortality, identifying vulnerabilities in the society, and planning efficient mitigation and adaptation strategies to prevent the impacts of climate changes on the public health sector.
Data Availability
Meteorological data used in this study are freely available via the Czech Hydrometeorological Institute's website: https://www.chmi.cz/historicka-data/pocasi/denni-data/Denni-data-dle-z.-123-1998-Sb. The authors are not entitled to share the mortality data with third parties according to the policy of the data provider (the Institute of Health Information and Statistics of the Czech Republic).
References
[dataset] CZSO, Czech Statistical Office (2021) Population change - Czechia: 1919–2020 (absolute figures). In: Czech Demographic Handbook - 2020 https://www.czso.cz/csu/czso/czech-demographic-handbook-2020. Accessed 26 Sep 2022
[dataset] EIGE, European Institute for Gender Equality (2022) Indicator: healthy life years by sex (from 2004 onwards) | Gender Statistics Database. In: European Institute for Gender Equality https://eige.europa.eu/gender-statistics/dgs/indicator/ta_hlthmort_hlth_years__hlth_hlye/line/year:2004,2005,2006,2007,2008,2009,2010,2011,2012,2013,2014,2015,2016,2017,2018,2019,2020/geo:CZ/unit:YR/sex:T,M,W/indic_he:LE_0. Accessed 26 Sep 2022
[dataset] Eurostat (2022a) Persons at risk of poverty or social exclusion by age and sex. https://ec.europa.eu/eurostat/databrowser/view/ILC_PEPS01N__custom_3460274/default/table?lang=en. Accessed 22 Sep 2022
[dataset] Eurostat (2022b) Persons at risk of poverty or social exclusion by income quantile and household composition. https://ec.europa.eu/eurostat/databrowser/view/ILC_PEPS03N__custom_3460515/default/table?lang=en. Accessed 26 Sep 2022
Achebak H, Devolder D, Ballester J (2018) Heat-related mortality trends under recent climate warming in Spain: a 36-year observational study. PLoS Med 15(7):e1002617. https://doi.org/10.1371/journal.pmed.1002617
Akaike H (1974) A new look at the statistical model identification. In: Parzen E, Tanabe K, Kitagawa G (eds) Selected Papers of Hirotugu Akaike. Springer, New York, NY, pp 215–222
Altman DG (2003) Statistics Notes: Interaction revisited: the difference between two estimates. BMJ 326(7382):219–219. https://doi.org/10.1136/bmj.326.7382.219
Altman DG, Bland JM (2011) How to obtain the confidence interval from a P value. BMJ 343(aug08 1):d2090. https://doi.org/10.1136/bmj.d2090
Andel R (2014) Aging in the Czech Republic. Gerontologist 54(6):893–900. https://doi.org/10.1093/geront/gnu047
Arbuthnott KG, Hajat S (2017) The health effects of hotter summers and heat waves in the population of the United Kingdom: a review of the evidence. Environ Health 16(1):119. https://doi.org/10.1186/s12940-017-0322-5
Aubrecht C, Özceylan D (2013) Identification of heat risk patterns in the U.S. National Capital Region by integrating heat stress and related vulnerability. Environ Int 56:65–77. https://doi.org/10.1016/j.envint.2013.03.005
Basu R (2009) High ambient temperature and mortality: a review of epidemiologic studies from 2001 to 2008. Environ Health 8:40. https://doi.org/10.1186/1476-069X-8-40
Bolker B (2009) Dealing with quasi- models in R. https://cran.microsoft.com/snapshot/2022-09-14/web/packages/bbmle/vignettes/quasi.pdf. Accessed 26 Sep 2022
Breil M, Downing C, Kazmierczak A, Mäkinen K, Romanovska L (2018) Social vulnerability to climate change in European cities - state of play in policy and practice. https://doi.org/10.25424/CMCC/SOCVUL_EUROPCITIES
Breil M, Zandersen M, Pishmisheva P, Branth Pedersen A, Romanovska L, Coninx I, Rogger M, Johnson K (2021) ‘Leaving no one behind’ in climate resilience policy and practice in Europe.: overview of knowledge and practice for just resilience. https://doi.org/10.25424/CMCC/JUSTTRANS_EUROPE
Burse RL (1979) Sex differences in human thermoregulatory response to heat and cold stress. Hum Factors 21(6):687–699. https://doi.org/10.1177/001872087912210606
Canouï-Poitrine F, Cadot E, Spira A, Canicule GR (2006) Excess deaths during the August 2003 heat wave in Paris. France Rev Epidemiol Sante Publique 54(2):127–135. https://doi.org/10.1016/s0398-7620(06)76706-2
CCAG, Climate Crisis Advisory Group (2022) Record-breaking heatwave will be an average summer by 2035, latest Met Office Hadley Centre data shows. Climate Crisis Advisory Group https://www.ccag.earth/newsroom/record-breaking-heatwave-will-be-an-average-summer-by-2035-latest-met-office-hadley-centre-data-shows. Accessed 28 Sep 2022
Charkoudian N, Stachenfeld NS (2014) Reproductive hormone influences on thermoregulation in women. Compr Physiol 4:793–804. https://doi.org/10.1002/cphy.c130029
Craig N (2005) Exploring the generalisability of the association between income inequality and self-assessed health. Soc Sci Med 60(11):2477–2488. https://doi.org/10.1016/j.socscimed.2004.11.018
CZSO, Czech Statistical Office (2015) Samoživitelky: Jak žijí a za co utrácejí u nás a v Evropě? https://www.czso.cz/csu/czso/cri/samozivitelky-jak-ziji-a-za-co-utraceji-u-nas-a-v-evrope. Accessed 26 Sep 2022
CZSO, Czech Statistical Office (2021) Focus on men and women 2021. In: Focus on men and women https://www.czso.cz/documents/10180/142141209/30000221.pdf/6c6dfcee-a1e1-4f73-a6a0-8fba06487154?version=1.11. Accessed 28 Mar 2022
Dahlin J, Härkönen J (2013) Cross-national differences in the gender gap in subjective health in Europe: does country-level gender equality matter? Soc Sci Med 98:24–28. https://doi.org/10.1016/j.socscimed.2013.08.028
Davídkovová H, Plavcová E, Kynčl J, Kyselý J (2014) Impacts of hot and cold spells differ for acute and chronic ischaemic heart diseases. BMC Public Health 14(1):480. https://doi.org/10.1186/1471-2458-14-480
de Schrijver E, Bundo M, Ragettli MS, Sera F, Gasparrini A, Franco OH, Vicedo-Cabrera AM (2022) Nationwide Analysis of the heat- and cold-related mortality trends in Switzerland between 1969 and 2017: the role of population aging. Environ Health Perspect 130(3):037001. https://doi.org/10.1289/EHP9835
Ellena M, Ballester J, Mercogliano P, Ferracin E, Barbato G, Costa G, Ingole V (2020a) Social inequalities in heat-attributable mortality in the city of Turin, northwest of Italy: a time series analysis from 1982 to 2018. Environ Health 19(1):116. https://doi.org/10.1186/s12940-020-00667-x
Ellena M, Breil M, Soriani S (2020b) The heat-health nexus in the urban context: a systematic literature review exploring the socio-economic vulnerabilities and built environment characteristics. Urban Clim 34:100676. https://doi.org/10.1016/j.uclim.2020.100676
Fouillet A, Rey G, Laurent F, Pavillon G, Bellec S, Guihenneuc-Jouyaux C, Clavel J, Jougla E, Hémon D (2006) Excess mortality related to the August 2003 heat wave in France. Int Arch Occup Environ Health 80(1):16–24. https://doi.org/10.1007/s00420-006-0089-4
Fox RH, Löfstedt BE, Woodward PM, Eriksson E, Werkstrom B (1969) Comparison of thermoregulatory function in men and women. J Appl Physiol 26(4):444–453. https://doi.org/10.1152/jappl.1969.26.4.444
Franke S, Kulu H (2018) Mortality differences by partnership status in England and Wales: the effect of living arrangements or health selection? Eur J Population 34(1):87–118. https://doi.org/10.1007/s10680-017-9423-7
Gabriel KMA, Endlicher WR (2011) Urban and rural mortality rates during heat waves in Berlin and Brandenburg. Germany Environ Pollut 159(8–9):2044–2050. https://doi.org/10.1016/j.envpol.2011.01.016
Gasparrini A (2011) Distributed lag linear and non-linear models in R: The Package dlnm. J Stat Softw 43(8):10.18637/jss.v043.i08
Gasparrini A, Armstrong B, Kenward MG (2010) Distributed lag non-linear models. Statist Med 29(21):2224–2234. https://doi.org/10.1002/sim.3940
Gasparrini A, Guo Y, Hashizume M, Kinney PL, Petkova EP, Lavigne E, Zanobetti A, Schwartz JD, Tobias A, Leone M, Tong S, Honda Y, Kim H, Armstrong BG (2015) Temporal variation in heat–mortality associations: a multicountry study. Environ Health Perspect 123(11):1200–1207. https://doi.org/10.1289/ehp.1409070
Gasparrini A, Guo Y, Sera F, Vicedo-Cabrera AM, Huber V, Tong S, de Sousa Zanotti Stagliorio Coelho M, Nascimento Saldiva PH, Lavigne E, Matus Correa P, Valdes Ortega N, Kan H, Osorio S, Kyselý J, Urban A, JJK J, NRI R, Pascal M, Goodman PG et al (2017) Projections of temperature-related excess mortality under climate change scenarios. Lancet Planet Health 1(9):e360–e367. https://doi.org/10.1016/S2542-5196(17)30156-0
Gasparrini A, Leone M (2014) Attributable risk from distributed lag models. BMC Med Res Methodol 14(1):55. https://doi.org/10.1186/1471-2288-14-55
Gronlund CJ, Berrocal VJ, White-Newsome JL, Conlon KC, O’Neill MS (2015) Vulnerability to extreme heat by socio-demographic characteristics and area green space among the elderly in Michigan, 1990–2007. Environ Res 136:449–461. https://doi.org/10.1016/j.envres.2014.08.042
Haider M, Jacknowitz A, Schoeni R (2003) The economic status of elderly divorced women. SSRN Electron J. https://doi.org/10.2139/ssrn.1090901
Hajat S, Kovats RS, Lachowycz K (2007) Heat-related and cold-related deaths in England and Wales: who is at risk? Occup Environ Med 64(2):93–100. https://doi.org/10.1136/oem.2006.029017
Hank K, Steinbach A (2018) Families and Health: A Review. In: Doblhammer G, Gumà J (eds) A demographic perspective on gender, family and health in Europe. Springer International Publishing, Cham, pp 23–39. https://doi.org/10.1007/978-3-319-72356-3_3
Hanzlíková H, Plavcová E, Kynčl J, Kříž B, Kyselý J (2015) Contrasting patterns of hot spell effects on morbidity and mortality for cardiovascular diseases in the Czech Republic, 1994–2009. Int J Biometeorol 59(11):1673–1684. https://doi.org/10.1007/s00484-015-0974-1
Hondula DM, Davis RE, Leisten MJ, Saha MV, Veazey LM, Wegner CR (2012) Fine-scale spatial variability of heat-related mortality in Philadelphia County, USA, from 1983-2008: a case-series analysis. Environ Health 11(1):16. https://doi.org/10.1186/1476-069X-11-16
Hoy A, Hänsel S, Maugeri M (2020) An endless summer: 2018 heat episodes in Europe in the context of secular temperature variability and change. Int J Climatol 40(15):6315–6336. https://doi.org/10.1002/joc.6582
Huang Z, Lin H, Liu Y, Zhou M, Liu T, Xiao J, Zeng W, Li X, Zhang Y, Ebi KL, Tong S, Ma W, Wang L (2015) Individual-level and community-level effect modifiers of the temperature–mortality relationship in 66 Chinese communities. BMJ Open 5(9):e009172. https://doi.org/10.1136/bmjopen-2015-009172
Hůnová I, Brabec M, Malý M, Knobová V, Braniš M (2017) Major heat waves of 2003 and 2006 and health outcomes in Prague. Air Qual Atmos Health 10(2):183–194. https://doi.org/10.1007/s11869-016-0419-y
IPCC (2021) Climate change 2021: The physical science basis. Contribution of working group I to the sixth assessment report of the intergovernmental panel on climate change. Cambridge University Press
Istiana N, Kurnia A, Ubaidillah A (2020) Quasi Poisson model for estimating under-five mortality rate in small area. EAI, Bogor, Indonesia. https://doi.org/10.4108/eai.2-8-2019.2290343
Jonsson AC, Lundgren L (2015) Vulnerability and adaptation to heat in cities: perspectives and perceptions of local adaptation decision-makers in Sweden. Local Environ 20(4):442–458. https://doi.org/10.1080/13549839.2014.896326
Kenney WL, Munce TA (2003) Invited review: aging and human temperature regulation. J Appl Physiol 95(6):2598–2603. https://doi.org/10.1152/japplphysiol.00202.2003
Kenny GP, Yardley J, Brown C, Sigal RJ, Jay O (2010) Heat stress in older individuals and patients with common chronic diseases. Can Med Assoc J 182(10):1053–1060. https://doi.org/10.1503/cmaj.081050
Klein Rosenthal J, Kinney PL, Metzger KB (2014) Intra-urban vulnerability to heat-related mortality in New York City, 1997–2006. Health Place 30:45–60. https://doi.org/10.1016/j.healthplace.2014.07.014
Kottek M, Grieser J, Beck C, Rudolf B, Rubel F (2006) World Map of the Köppen-Geiger climate classification updated. Metz 15(3):259–263. https://doi.org/10.1127/0941-2948/2006/0130
Kyselý J (2004) Mortality and displaced mortality during heat waves in the Czech Republic. Int J Biometeorol 49(2):91–97. https://doi.org/10.1007/s00484-004-0218-2
Kyselý J, Kříž B (2008) Decreased impacts of the 2003 heat waves on mortality in the Czech Republic: an improved response? Int J Biometeorol 52(8):733–745. https://doi.org/10.1007/s00484-008-0166-3
Kyselý J, Plavcová E (2012) Declining impacts of hot spells on mortality in the Czech Republic, 1986–2009: adaptation to climate change? Clim Chang 113(2):437–453. https://doi.org/10.1007/s10584-011-0358-4
Kyselý J, Plavcová E, Hanzlíková H, Kyncl J (2011) Comparison of hot and cold spell effects on cardiovascular mortality in individual population groups in the Czech Republic. Clim Res 49:113–129. https://doi.org/10.3354/cr01014
Lago S, Cantarero D, Rivera B, Pascual M, Blázquez-Fernández C, Casal B, Reyes F (2018) Socioeconomic status, health inequalities and non-communicable diseases: a systematic review. J Public Health 26(1):1–14. https://doi.org/10.1007/s10389-017-0850-z
Lawlor DA, Sterne JAC (2007) Socioeconomic inequalities in health. BMJ 334(7601):963–964. https://doi.org/10.1136/bmj.39203.661829.BE
Lhotka O, Kyselý J (2022) European heat waves of summer 2021 in the context of past major heat waves. EGU Gen Assy 2022. https://doi.org/10.5194/egusphere-egu22-3666
Lhotka O, Kyselý J, Farda A (2018) Climate change scenarios of heat waves in Central Europe and their uncertainties. Theor Appl Climatol 131(3–4):1043–1054. https://doi.org/10.1007/s00704-016-2031-3
Lorenz FO, Wickrama KAS, Conger RD, GHE Jr (2006) The short-term and decade-long effects of divorce on women’s midlife health. J Health Soc Behav 47(2):111–125. https://doi.org/10.1177/002214650604700202
Marí-Dell’Olmo M, Tobías A, Gómez-Gutiérrez A, Rodríguez-Sanz M, García de Olalla P, Camprubí E, Gasparrini A, Borrell C (2019) Social inequalities in the association between temperature and mortality in a South European context. Int J Public Health 64(1):27–37. https://doi.org/10.1007/s00038-018-1094-6
McGregor GR, Bessemoulin P, Ebi K, Menne B (2015) Heatwaves and health: guidance on warning-system development. WMO No. 1142. https://library.wmo.int/doc_num.php?explnum_id=3371. Accessed 22 May 2023
McMaughan DJ, Oloruntoba O, Smith ML (2020) Socioeconomic status and access to healthcare: interrelated drivers for healthy aging. Front Public Health 8:231. https://doi.org/10.3389/fpubh.2020.00231
O’Neill MS, Zanobetti A, Schwartz J (2003) Modifiers of the temperature and mortality association in seven US cities. Am J Epidemiol 157(12):1074–1082. https://doi.org/10.1093/aje/kwg096
Oksuzyan A, Brønnum-Hansen H, Jeune B (2010) Gender gap in health expectancy. Eur J Ageing 7(4):213–218. https://doi.org/10.1007/s10433-010-0170-4
Oksuzyan A, Petersen I, Stovring H, Bingley P, Vaupel JW, Christensen K (2009) The male–female health–survival paradox: a survey and register study of the impact of sex-specific selection and information bias. Ann Epidemiol 19(7):504–511. https://doi.org/10.1016/j.annepidem.2009.03.014
Otto IM, Reckien D, Reyer CPO, Marcus R, Le Masson V, Jones L, Norton A, Serdeczny O (2017) Social vulnerability to climate change: a review of concepts and evidence. Reg Environ Chang 17(6):1651–1662. https://doi.org/10.1007/s10113-017-1105-9
Palència L, De Moortel D, Artazcoz L, Salvador-Piedrafita M, Puig-Barrachina V, Hagqvist E, Pérez G, Ruiz ME, Trujillo-Alemán S, Vanroelen C, Malmusi D, Borrell C (2017) Gender policies and gender inequalities in health in Europe: results of the SOPHIE project. Int J Health Serv 47(1):61–82. https://doi.org/10.1177/0020731416662611
Petkova EP, Dimitrova LK, Sera F, Gasparrini A (2021) Mortality attributable to heat and cold among the elderly in Sofia Bulgaria. Int J Biometeorol 65(6):865–872. https://doi.org/10.1007/s00484-020-02064-y
Putnam H, Hondula DM, Urban A, Berisha V, Iñiguez P, Roach M (2018) It’s not the heat, it’s the vulnerability: attribution of the 2016 spike in heat-associated deaths in Maricopa County. Arizona Environ Res Lett 13(9):094022. https://doi.org/10.1088/1748-9326/aadb44
Romero-Ortuno R, Fouweather T, Jagger C (2014) Cross-national disparities in sex differences in life expectancy with and without frailty. Age Ageing 43(2):222–228. https://doi.org/10.1093/ageing/aft115
Sbarra DA, Whisman MA (2022) Divorce, health, and socioeconomic status: an agenda for psychological science. Curr Opin Psychol 43:75–78. https://doi.org/10.1016/j.copsyc.2021.06.007
Schwartz J (2005) Who is sensitive to extremes of temperature? A case-only analysis. Epidemiology 16(1):67–72. https://doi.org/10.1097/01.ede.0000147114.25957.71
Seebaß K (2017) Who is feeling the heat? Vulnerabilities and exposures to heat stress - individual, social, and housing explanations. Nat Cult 12(2):137–161. https://doi.org/10.3167/nc.2017.120203
Son J-Y, Liu JC, Bell ML (2019) Temperature-related mortality: a systematic review and investigation of effect modifiers. Environ Res Lett 14(7):073004. https://doi.org/10.1088/1748-9326/ab1cdb
Stafoggia M, Forastiere F, Agostini D, Biggeri A, Bisanti L, Cadum E, Caranci N, de’Donato F, De Lisio S, De Maria M, Michelozzi P, Miglio R, Pandolfi P, Picciotto S, Rognoni M, Russo A, Scarnato C, Perucci CA (2006) Vulnerability to heat-related mortality: a multicity, population-based, case-crossover analysis. Epidemiology 17(3):315–323. https://doi.org/10.1097/01.ede.0000208477.36665.34
Symoens S, Van de Velde S, Colman E, Bracke P (2014) Divorce and the multidimensionality of men and women’s mental health: the role of social-relational and socio-economic conditions. Appl Res Qual Life 9(2):197–214. https://doi.org/10.1007/s11482-013-9239-5
Székely M, Carletto L, Garami A (2015) The pathophysiology of heat exposure. Temperature (Austin) 2(4):452. https://doi.org/10.1080/23328940.2015.1051207
Tenglerová H, Huck A, Linková M (2020) Accelerating the transition to a climate prepared and resilient Europe. https://genderaction.eu/wp-content/uploads/2020/09/Mission-2-pagers_ClimateChange_FIN.pdf. Accessed 26 Sep 2022
Tobías A, Armstrong B, Gasparrini A (2017) Brief report: investigating uncertainty in the minimum mortality temperature methods and application to 52 Spanish cities. Epidemiology 28(1):72–76. https://doi.org/10.1097/EDE.0000000000000567
UN High Commissioner for Refugees (2021) Need to know guidance: working with lesbian, gay, bisexual, transgender, intersex and queer persons in forced displacement. https://www.refworld.org/docid/4e6073972.html. Accessed 26 Sep 2022
Urban A, Burkart K, Kyselý J, Schuster C, Plavcová E, Hanzlíková H, Lakes T (2016) Spatial patterns of heat-related cardiovascular mortality in the Czech Republic. Int J Environ Res Public Health 13:284. https://doi.org/10.3390/ijerph13030284
Urban A, Davídkovová H, Kyselý J (2014) Heat- and cold-stress effects on cardiovascular mortality and morbidity among urban and rural populations in the Czech Republic. Int J Biometeorol 58(6):1057–1068. https://doi.org/10.1007/s00484-013-0693-4
Urban A, Di Napoli C, Cloke HL, Kyselý J, Pappenberger F, Sera F, Schneider R, Vicedo-Cabrera AM, Acquaotta F, Ragettli MS, Íñiguez C, Tobias A, Indermitte E, Orru H, Jaakkola JJK, Ryti NRI, Pascal M, Huber V, Schneider A et al (2021) Evaluation of the ERA5 reanalysis-based universal thermal climate index on mortality data in Europe. Environ Res 198:111227. https://doi.org/10.1016/j.envres.2021.111227
Urban A, Fonseca-Rodríguez O, Di Napoli C, Plavcová E (2022) Temporal changes of heat-attributable mortality in Prague, Czech Republic, over 1982–2019. Urban Clim 44:101197. https://doi.org/10.1016/j.uclim.2022.101197
Urban A, Hanzlíková H, Kyselý J, Plavcová E (2017) Impacts of the 2015 heat waves on mortality in the Czech Republic—a comparison with previous heat waves. Int J Environ Res Public Health 14:1562. https://doi.org/10.3390/ijerph14121562
Urban A, Kyselý J (2014) Comparison of UTCI with other thermal indices in the assessment of heat and cold effects on cardiovascular mortality in the Czech Republic. IJERPH 11(1):952–967. https://doi.org/10.3390/ijerph110100952
Urban A, Kyselý J, Plavcová E, Hanzlíková H, Štěpánek P (2020) Temporal changes in years of life lost associated with heat waves in the Czech Republic. Sci Total Environ 716:137093. https://doi.org/10.1016/j.scitotenv.2020.137093
Vésier C (2022) Social inequalities in heat-related mortality. https://is.czu.cz/zp/index.pl?podrobnosti_zp=295097;zpet=;prehled=vyhledavani;vzorek_zp=chlo%C3%A9%20v%C3%A9sier;dohledat=Dohledat;kde=autor;stav_filtr=bez;typ=1;typ=2;typ=3;typ=101;typ=8;typ=7;fakulta=20;fakulta=41;fakulta=40;fakulta=71;fakulta=50;fakulta=73;fakulta=72;fakulta=10;fakulta=30;obhajoba=2022;obhajoba=2021;obhajoba=2020;jazyk=1;jazyk=3;jazyk=2;jazyk=-1;lang=en. Accessed 22 Sep 2022
Wan K, Feng Z, Hajat S, Doherty RM (2022) Temperature-related mortality and associated vulnerabilities: evidence from Scotland using extended time-series datasets. Environ Health 21(1):99. https://doi.org/10.1186/s12940-022-00912-5
Watts N, Amann M, Arnell N, Ayeb-Karlsson S, Beagley J, Belesova K, Boykoff M, Byass P, Cai W, Campbell-Lendrum D, Capstick S, Chambers J, Coleman S, Dalin C, Daly M, Dasandi N, Dasgupta S, Davies M, Di Napoli C et al (2021) The 2020 report of The Lancet Countdown on health and climate change: responding to converging crises. Lancet 397(10269):129–170. https://doi.org/10.1016/S0140-6736(20)32290-X
Watts N, Amann M, Arnell N, Ayeb-Karlsson S, Belesova K, Boykoff M, Byass P, Cai W, Campbell-Lendrum D, Capstick S, Chambers J, Dalin C, Daly M, Dasandi N, Davies M, Drummond P, Dubrow R, Ebi KL, Eckelman M et al (2019) The 2019 report of the Lancet countdown on health and climate change: ensuring that the health of a child born today is not defined by a changing climate. Lancet 394(10211):1836–1878. https://doi.org/10.1016/S0140-6736(19)32596-6
Wedderburn RWM (1974) Quasi-likelihood functions, generalized linear models, and the Gauss-Newton method. Biometrika 61(3):439. https://doi.org/10.2307/2334725
WHO (2021) Gender and health. https://www.who.int/news-room/questions-and-answers/item/gender-and-health. Accessed 26 Sep 2022
Xu P, Wang L, Liu Y, Chen W, Huang P (2020) The record-breaking heat wave of June 2019 in Central Europe. Atmos Sci Lett 21(4). https://doi.org/10.1002/asl.964
Xu Z, FitzGerald G, Guo Y, Jalaludin B, Tong S (2016) Impact of heatwave on mortality under different heatwave definitions: a systematic review and meta-analysis. Environ Int 89–90:193–203. https://doi.org/10.1016/j.envint.2016.02.007
Yanovich R, Ketko I, Charkoudian N (2020) Sex differences in human thermoregulation: relevance for 2020 and beyond. Physiology 35(3):177–184. https://doi.org/10.1152/physiol.00035.2019
Yu W, Vaneckova P, Mengersen K, Pan X, Tong S (2010) Is the association between temperature and mortality modified by age, gender and socio-economic status? Sci Total Environ 408(17):3513–3518. https://doi.org/10.1016/j.scitotenv.2010.04.058
Zueras P, Rutigliano R, Trias-Llimós S (2020) Marital status, living arrangements, and mortality in middle and older age in Europe. Int J Public Health 65(5):627–636. https://doi.org/10.1007/s00038-020-01371-w
Acknowledgements
We would like to thank all the national data providers for supplying meteorological as well as health data. Special thanks go to Bohumír Kříž (in memoriam), Jan Kynčl, National Institute of Public Health, and Hana Hanzlíková, Institute of Atmospheric Physics CAS, for preparing mortality datasets. We thank Jan Kyselý, Institute of Atmospheric Physics CAS, and Osvaldo Fonseca Rodríguez, Umeå University, for critically reviewing the manuscript.
Funding
The study was supported by the Czech Science Foundation [22-24920S].
Author information
Authors and Affiliations
Contributions
Conceptualization: Aleš Urban; Data Curation: Aleš Urban; Formal analysis: Chloé Vésier; Methodology: Aleš Urban, Chloé Vésier; Software: Chloé Vésier; Supervision: Aleš Urban; Visualization: Chloé Vésier; Writing–Original Draft: Chloé Vésier; Writing–Review and Editing: Aleš Urban.
Corresponding author
Ethics declarations
Non-financial interests
Aleš Urban is a field editor of the International Journal of Biometeorology.
Competing interests
The authors declare no competing interests.
Supplementary information
ESssM 1
(DOCX 142 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vésier, C., Urban, A. Gender inequalities in heat-related mortality in the Czech Republic. Int J Biometeorol 67, 1373–1385 (2023). https://doi.org/10.1007/s00484-023-02507-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-023-02507-2