
Abstract
Introduction
Breast cancer (BC) is the most common cancer among women, and half of those diagnosed are of working age. Positive encounters regarding work from healthcare professionals have been shown to promote return to work among sickness absentees in general. However, the knowledge about encounters possible associations with sickness absence (SA) in women with BC is scarce.
Aim
To explore if women had experienced encounters regarding work from healthcare professionals during the first year after BC surgery and if this was associated with SA during the second year after surgery, controlled for treatment and sociodemographic effects.
Methods
A prospective cohort study of 690 Swedish women with primary BC, aged 24–63 years included after surgery. Descriptive statistics and adjusted logistic regression (age, birth country, education, self-rated health, treatment) with 95% confidence intervals (CI) were used.
Results
Eighty percent of the women had experienced encounters regarding work. Women who got advice and support regarding work (adjusted odds ratio (OR) 0.5; 0.3–0.9) or were encouraged to work (adjusted OR 0.6; 0.3–0.9) had less SA. A larger proportion of those encouraged to work had less advanced cancer, surgery, hormone, or radiotherapy. Consistently, women encouraged to be on SA had more SA, but this was partly explained by disease or treatment factors (crude OR 1.6; 1.1–2.4, adjusted OR 1.2 (0.8–1.9) since a larger proportion of those with more advanced cancer, surgery, or chemotherapy had more SA.
Conclusion
Most women experienced encounters regarding work, and the nature of these encounters were associated with SA 2 years after BC surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Breast cancer (BC) is the most common cancer among women, with a 5-year survival of 90% [1, 2]. In Sweden, 50% of women diagnosed with BC are of working age [2], and in previous studies, most women with BC state that paid work is an important aspect of their lives [3, 4] and for recovery [5, 6]. With the high, rising incidence and survival rates, it is expected that more women with BC will be of working age, but there is still a knowledge gap regarding why some of them do not return-to-work (RTW) as expected according to clinical recommendations after the BC surgery [7, 8].
The long-term probability for RTW between 1 and 5 years after the BC surgery varies largely internationally, from 43 to 93% [9,10,11,12,13]. A nationwide Swedish study revealed that during the first year after BC diagnosis, 71% of the women were on sickness absence (SA), and 5 years after the diagnosis, a higher proportion of women with BC had SA and disability pension (DP) compared to women of the same ages without BC [14]. Treatment-related side-effects are assumed to influence SA during the first year after surgery [8], observed to be most pronounced in women undergoing mastectomy or chemotherapy and hormonal treatment [15]. Healthcare professionals may have an important role in the women’s SA during this period, and it has been shown that women with BC expect their assistance in prioritizing work and work continuation during treatment [16]. Several studies of sickness absentees with various diagnoses have shown that supportive and encouraging encounters regarding work with healthcare professionals promotes RTW [17,18,19,20,21,22,23,24,25,26]. In the very few studies conducted in this field, the types of encounters that have been shown to promote RTW among women with BC are giving adequate information and guiding the women with BC in work-related issues [10, 27] and healthcare professionals’ attitudes regarding RTW [28]. Although previous research has indicated that encounters regarding work may influence RTW and SA among women with BC, these studies have not controlled for treatment or sociodemographic effects.
The aim of this study was to explore if women had experienced encounters regarding work from healthcare professionals during the first year after BC surgery and if this was associated with SA during the second year after surgery, controlled for treatment and sociodemographic effects.
Material and methods
This is a prospective cohort study with a 2 year follow-up using data from questionnaires, medical files, and registers. In total, 970 women who had undergone BC surgery were eligible. The women were screened for eligibility between June 2007 and November 2009 consecutively after BC surgery, at their first oncology clinic visit for discussion of further treatment. Eligibility criteria were the following: aged ≤ 63 years, living in Stockholm, Sweden, literate in Swedish, with a first BC diagnosis not in-situ, and without known metastases or neoadjuvant treatment. Due to administrative oversight, 48 women were missed, resulting in 922 women informed about the study. Of these, 173 chose not to participate, and 749 (77.2%) women accepted to participate. As the outcome was SA or DP, we excluded those on DP for at least 50% of full-time working hours during the 2 years before the surgery (n = 37), and those on SA more than 50% 2 years’ prior (n = 4). Given some women may have been on SA due to an acute response related to BC during the period of examination before the formal BC diagnosis and surgery, all with SA the year before surgery were included. We also excluded those who during follow-up reached the age for retirement in Sweden, 65 years (n = 13) or died (n = 5), resulting in 690 women included in the study sample.
Data
In this study, questionnaire and register data were used. Questionnaire data on sociodemographic characteristics, self-rated health, and encounters regarding work with healthcare professionals within 8 months from the date of surgery, were collected through a comprehensive questionnaire. The questionnaires have been tested and are described in detail elsewhere [29, 30]. The baseline questionnaire was handed out to the women at the first visit at the clinic, about 4 weeks after the BC surgery, and follow-up questionnaires were sent to participants by post 4 and 8 months after surgery. For analysis, age was categorized from a continuous variable into “< 35,” “35–44,” “45–54,” “55–63” years. Education was dichotomized as “primary/secondary school” (≤ 12 years) and “college/university” (> 12 years), and country of birth as “born in Sweden” or “born outside of Sweden”. Health was measured by the question “How is your health in general?” at 4 weeks (baseline) and 4 and 8 months respectively after surgery. The five response alternatives were dichotomized so that “excellent,” “very good,” and “good” were included in “good” and “fair” and “poor” in “not good” when analyzed. Encounters regarding work were measured by three questions: “In relation to your BC, have you been from healthcare professionals, (1) received useful advice and support related to work?, (2) been encouraged to be on SA?, and (3) been encouraged to work?” with four response options dichotomized so that “always” and “often” were included in “always/often” and “seldom” and “never” in “seldom/never” for the analyses. Further, measurement points baseline, 4, and 8 months were combined into having experienced the encounters at any of these time points.
From the Swedish nationwide clinical register for BC, data were obtained on cancer stage, type of surgery, and death. Pathological tumor-node (TN) classification [31] was dichotomized from T0N0, stage 0 and 1 to “stage group 1,” and stages 2 and 3 to “stage group 2.” Breast surgery was dichotomized as less advanced “breast conserving” or more advanced “mastectomy including subcutaneous mastectomy,” and axillary surgery was dichotomized as less advanced “sentinel lymph node biopsy” or more advanced “axillary lymph node dissection including sampling.” From medical files, data were extracted regarding adjuvant treatment (yes/no), completed chemotherapy, radiotherapy and targeted therapy, and having hormone therapy, respectively, direct reconstruction (yes/no), and relapse within 2.5 years after surgery date (yes/no).
Data on SA and DP days were obtained from the Swedish Social Insurance Agency. In Sweden, all individuals from 16 years of age with income from work or unemployment- or parental benefits can be granted SA benefits if having reduced work capacity due to injury or disease. For most employed, the SA benefits are covered by the Social Insurance from day 15 of a SA spell; the first 14 days are covered by the employers. SA can be granted for full or part-time: 25%, 50%, or 75% of ordinary working hours. All people living in Sweden aged 19–64 can be granted DP if having long-term or permanent work incapacity due to disease or injury. In analyses of SA, we used net days in spells longer than 14 days (net days were calculated so that two half-days equals one whole day, and then summed to total days per year). SA and DP days were calculated for four different time windows: (1) the 2 years before BC surgery, year minus 2 (year−2); (2) 1 year before BC surgery, year minus 1 (year−1); (3) 1 year after BC surgery, (year1) and; (4) 2 years after BC surgery (year2). For the analysis, SA was either used as a continuous variable or categorized to “zero days,” “90 days or less,” and “more than 90 days.” DP was used as a continuous variable.
Data analysis
Descriptive statistics were calculated for the characteristics of the study sample, including SA and DP days both separately and summed together, and for encounters regarding work with healthcare professionals. Furthermore, associations between background variables and having experienced encounters regarding work were calculated. Since very few women (5.1%) had DP at year2, multivariable analyses were only conducted using SA as an outcome. In the multivariable analyses, the women who died (n = 6) or had a relapse (n = 38) during follow-up were excluded, as were women with any DP. This in order to ensure that encounters regarding work were not affected by the fact that these women already had a work disability in the form of DP at the surgery. To reveal associations between experiences of encounters regarding work year1 and SA year2 after the first BC surgery, odds ratios (OR) with 95% confidence intervals (CI) were calculated, using logistic regression. Both crude and adjusted OR were calculated, adjusting for age, education, country of birth, self-rated health at baseline, type of surgery, and chemotherapy in the multivariable analyses. Since there is a dependency between staging and treatment [8], only treatment variables and not TN classification were included. Analyses were conducted with the software SPSS 24 [32].
Results
The women were aged 24–63 years (mean 50.8 years), most of them were born in Sweden (84.5%), and more than half had college or university education (57.2%). At baseline, 60.4% of the women rated their health as excellent or very good. Four months after surgery, 38% rated their health as excellent or very good, and at 8 months after surgery, the proportion was 42.5%. According to the TN classification, two thirds of the women had cancer stages 0–1 (66.2%) and one third stages 2–3 (33.6%). Most of the women had had breast conserving surgery (66.8%) compared to mastectomy (33.2%). More than half had had sentinel lymph node biopsy (55.5%) compared to having had an axillary lymph node dissection (43.2%). A small proportion of the women had had a direct reconstruction (15.4%). The majority received adjuvant treatment during the follow-up; radiotherapy (81.7%), chemotherapy (49.0%), and targeted therapy (12.9%), and also had started hormone therapy (81.2%). Within the period of 2.5 years, 5.1% had had a relapse (Table 1).
Occurrence of SA and DP
About one third (39.6%) of the cohort had had at least some SA > 14 days in the 3 months before the BC surgery (total mean 5.6; median 0.0 days) and few were on DP at the date of surgery (4.8%). A third of the women (36.2%) had at least some SA > 14 days year2 from the surgery, among those with SA the mean number of days were 102.4 (Table 2). With regard to age, a slightly larger proportion of those who were aged < 35 and 55–63 years had SA 90 days or less year2 from BC surgery compared to women aged both 35–44 and 45–54 years (< 35, 66.7%; 35–44, 57.1%; 45–54, 61.1%; 55–63, 64.6%). Also, of the women aged 35–44 and 45–54 years, a larger proportion had more than 90 and up to 180 SA days than women aged < 35 and 55–63 years (< 35, 11.1%; 35–44, 22.2%; 45–54, 20.4%; 55–63, 12.3%), while among women of all age groups, similar proportions had more than 180 days during the year2 from the BC surgery (not shown in tables). Regarding DP, 5.1% had any DP in year2 from surgery, with a mean number of 143.4 DP days during that year. In total, the mean number of SA/DP days in year2 from the BC surgery was 111.8 among those with any SA or DP (Table 2).
Experienced encounters
A majority (80.4%) reported that they had experienced the encounter “advice and support related to work,” at least once within the first 8 months after surgery. About half of the women (50.6%) had experienced the encounter “encouraged to be on SA,” while 66.2% had experienced “encouraged to work” at least once (Table 3). In relation to sociodemographic characteristics and self-rated health, mostly similar proportions of women had experienced these three different encounters (Table 4). Regarding TN classification, a slightly larger proportion of the women with cancer stages 3–4 had been “encouraged to be on SA” (57.8%), while a larger proportion with stages 1–2 had been “encouraged to work” (70%). Concerning type of surgery, of those women who had mastectomy or axillary lymph node dissection, a slightly larger proportion had been “encouraged to be on SA” (mastectomy 55.9%; sentinel lymph node dissection 59.6%), while more of those with a sentinel lymph node biopsy were “encouraged to work” (71.4%). Of those who received chemotherapy, a higher proportion had experienced to be “encouraged to be on SA” (63.9%) and a higher proportion of those with hormone therapy or radiotherapy often/always were “encouraged to work” (67.0%; 66.3%) (Table 4).
Associations with SA
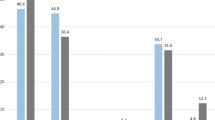
Those who always/often had experienced the encounter “advice and support regarding work”, had fewer SA days during year2 compared to women who had seldom/never experienced such encounters (mean: always/often 35.2; seldom/never 44.9 mean days) (Table 4). Those women who always/often had been “encouraged to work” had fewer SA days year2, compared to those who had seldom/never experienced such encounters (mean: yes 31.5; no 48.1).
In multivariable analyses of associations between encounters and days of SA, significant associations were found (Table 5). An association was found between having had “advice and support regarding work” and being SA more than 90 days, compared to being SA 0–14 days, when adjusting for sociodemographic, type of surgery, and chemotherapy (OR 0.5; 95% CI 0.3–0.9). Those who had been “encouraged to be on SA” had higher odds for being SA 15–90 days, when adjusting for age group, country of birth, educational level (OR 1.7; 95% CI 1.1–2.5), as well as when including baseline self-rated health (OR 1.7; 1.2–2.6). The association were attenuated when further adjusting for type of surgery and chemotherapy. Women with BC who often/always had been “encouraged to work” had lower odds for being SA 91–365 days, compared to those being SA 0 days, when adjusting for age group, country of birth, educational level (OR 0.4; 95% CI 0.3–0.7), and baseline self-rated health (OR 0.4; 95% CI 0.3–0.7). The associations also remained after adjusting for type of surgery, and chemotherapy (OR 0.6; 95% CI 0.3–0.9).
Discussion
This prospective cohort study showed that a majority of the women with BC had experienced different types of encounters regarding work from healthcare professionals. Women who had experienced “advice and support regarding work” and “encouraged to work” had fewer SA days year2, while those “encouraged to be on SA” had more SA days. The association between “encouraged to be on SA” and SA was partly explained by treatment. Those with less advanced cancer stage and/or surgery, receiving hormone or radiotherapy were more likely to have experienced the encounter “encouraged to work,” while those with more advanced cancer stage and/or surgery and those receiving chemotherapy were more likely to have had the encounter “encouraged to be on SA.” Thus, encounters regarding work were associated with future SA 2 years after surgery.
Women included in this study were of working age, and considering their general health and state of disease, most would be expected to RTW after treatment according to Swedish recommendations for SA after BC surgery [8]. One third of the women had been on SA some time during the 3 months before the surgery, which may be related to a crisis response at the time for diagnosis. During year2 from surgery, also one third of the women had been on SA. This could of course be associated with treatment, as shown in the multivariable analysis, but the question is, why are these factors associated with SA for some but not for all women when adjuvant treatments, except for hormone therapy, would be expected to have finished [8]? Persisting symptoms are one potential explanation, as women with BC have reported symptoms from treatment 10 years after treatment cessation [33]. SA after the first year could also be associated with unmeasured factors, such as work conditions [34] or concerns about future life conditions [35, 36].
We found that a majority of the women had experienced some type of encounter regarding work. This may be contrasted to Braybrooke et al. [10], despite contextual differences, where a minority of women with BC who had undergone chemotherapy were found to have received information and encouragement regarding RTW. In a study by Ganem et al. [16], it was also shown that women with BC wish that healthcare professionals would raise issues related to work and discuss possibilities to continue to work during treatment, which in the present study many women had experienced. It has also been shown in previous studies, that by support and encouragement [37] or guidance and giving adequate information [10, 27], healthcare professionals can promote RTW among sickness absentees. Similarly, we have previously found that during the first year after BC surgery, a larger proportion of those who had been encouraged to work or had been encouraged to be on SA, had followed the encouragement [38]. In the present study, women with BC who had experienced encounters regarding work had fewer SA days. It is also possible that the encounters were targeted to the “right” individuals since those with less severe disease and less advanced treatment had been encouraged to work, and those with more severe disease and advanced treatment had instead been encouraged to be on SA. This is consistent with studies showing that women who had undergone mastectomy or who had chemotherapy were more likely to be on SA [9, 13, 15], especially during year1 after surgery [14, 27]. Based on this assumption, we included both surgery and chemotherapy in the multivariable analyses and found that those factors to a large extent was associated with SA also during year2 after surgery. There are also some other possible explanations for the differences in SA. It may be that women with BC followed what healthcare professionals encouraged them to do (to be on SA or not) regardless of disease status or general health, as shown in previous studies of the same cohort [4, 28]. Therefore, it would have been interesting to have information on healthcare professionals’ actual encounters and attitudes concerning SA and work, since the encounters should be based on the patients work capacity in relation to work demands rather than attitudes [4, 28]. It is important to note that 60% of women had no SA year2 and additionally, not all women experienced any type of encounter regarding work.
Strengths and limitations
Strengths include the relatively large sample size, a great variety of variables, and collected data at several time points during the 2-year follow-up period giving a wide range of experiences over time among women with BC. Further, the response rate for the whole study population was almost 80%. The detailed information regarding different variables gave us the possibility to exclude individuals without comparable risk for SA during follow-up, i.e., those with metastasis or relapse, since they can be assumed to have more SA. Also, we excluded those who would probably not receive encounters regarding work either due to their age, or due to already having other reasons for SA: those with retirement within follow-up, on > 50% DP year−2 and year−1, or having had > 50% SA year−2 from diagnosis.
Other strengths were that the questionnaire was based on questions that have been used in earlier studies [30]. The combination of the large sample size and background data including high quality information from registers and from medical files enabled sub-group analyses with adjustment for important factors known to be associated with SA/DP among women with BC. A limitation was that even though we had information regarding start of hormone therapy, we did not know about compliance and therefore were unable to control for that in the multivariable analyses.
Another strength is that the study is conducted in Sweden, with a high employment rate among women, including women in higher ages [39]. This means that the healthy selection effect of women in the work force is not as strong as in other countries.
To have self-reported data such as experiences of encounters regarding work may be seen as a strength since it presents experiences rated by the women themselves. The baseline question about experiencing certain encounters might also affect the experience of future encounters; therefore, we combined the questions from the three first time points, giving us the information about whether the women with BC had experienced the encounters at any time within the first year after surgery, i.e., during the period when treatment was ongoing.
A limitation of the study may be that even though we had high-quality register data on SA and DP for year−2 to year2 from the date of BC surgery, we did not have information on SA in spells ≤ 14 days giving a possible underestimation of SA days. This may also be seen as a strength since only the more severe SA were included; e.g., not colds and migraines.
Conclusion
The majority of the women with BC had experienced encounters regarding work during the year1 after their surgery and most had no SA during year2 after surgery. Women having had more advanced surgery and/or had received chemotherapy were to a larger proportion on SA year2. Encounters regarding work were associated with level of SA, and this association may be partly explained by type of surgery and chemotherapy but also by healthcare professionals’ encounters regarding work. A greater awareness of the influence of encounters regarding work among healthcare professionals is needed in order to promote RTW.
References
GLOBOCAN 2012 (2017) International Agency for Research on Cancer WHO. Available via Lyon, France, GLOBOCAN (IARC) Section of cancer information. http://globocan.iarc.fr/Default.aspx
Cancerincidens i Sverige (2014) Cancer incidence in Sweden 2014 [ in Swedish].. Socialstyrelsen, Stockholm
Petersson LM, Nilsson MI, Alexanderson K, Olsson M, Wennman-Larsen A (2013) How do women value work shortly after breast cancer surgery and are their valuations associated with being on sick leave? J Occup Rehabil 23(3):391–399. https://doi.org/10.1007/s10926-012-9402-0
Nilsson MI, Olsson M, Wennman-Larsen A, Petersson LM, Alexanderson K (2013) Women’s reflections and actions regarding working after breast cancer surgery - a focus group study. Psycho-Oncology 22(7):1639–1644. https://doi.org/10.1002/pon.3192
Lilliehorn S, Hamberg K, Kero A, Salander P (2013) Meaning of work and the returning process after breast cancer: a longitudinal study of 56 women. Scand J Caring Sci 27(2):267–274. https://doi.org/10.1111/j.1471-6712.2012.01026.x
Tamminga SJ, de Boer AG, Verbeek JH, Taskila T, Frings-Dresen MH (2010) Enhancing return-to-work in cancer patients, development of an intervention and design of a randomised controlled trial. BMC Cancer 10(1):345. https://doi.org/10.1186/1471-2407-10-345
National Board of Health and Welfare (2011) Insurance medicine desicion support. Försäkringsmedicinskt beslutsstöd; bröstcancer (in Swedish). https://roi.socialstyrelsen.se/fmb/brostcancer/411. Accessed 11 Apr 2018
Senkus E, Kyriakides S, Ohno S, Penault-Llorca F, Poortmans P, Rutgers E, Zackrisson S, Cardoso F (2015) Primary breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 26(suppl_5):v8–v30. https://doi.org/10.1093/annonc/mdv298
Islam T, Dahlui M, Majid H, Nahar A, Mohd Taib N, Su T, My BCCsg (2014) Factors associated with return to work of breast cancer survivors: a systematic review. BMC Public Health 14(Suppl 3):S8. https://doi.org/10.1186/1471-2458-14-S3-S8
Braybrooke JP, Mimoun S, Zarca D, Elia D, Pinder B, Lloyd AJ, Breheny K, Lomazzi M, Borisch B (2015) Patients’ experiences following breast cancer treatment: an exploratory survey of personal and work experiences of breast cancer patients from three European countries. Eur J Cancer Care 24(5):650–661. https://doi.org/10.1111/ecc.12222
Noeres D, Park-Simon TW, Grabow J, Sperlich S, Koch-Giesselmann H, Jaunzeme J, Geyer S (2013) Return to work after treatment for primary breast cancer over a 6-year period: results from a prospective study comparing patients with the general population. Support Care Cancer 21(7):1901–1909. https://doi.org/10.1007/s00520-013-1739-1
Villaverde RM, Batlle JF, Yllan AV, Gordo AMJ, Sanchez AR, Valiente BSJ, Baron MG (2008) Employment in a cohort of breast cancer patients. Occup Med (Lond) 58(7):509–511. https://doi.org/10.1093/occmed/kqn092
Fantoni SQ, Peugniez C, Duhamel A, Skrzypczak J, Frimat P, Leroyer A (2010) Factors related to return to work by women with breast cancer in northern France. J Occup Rehabil 20(1):49–58. https://doi.org/10.1007/s10926-009-9215-y
Kvillemo P, Mittendorfer-Rutz E, Bränström R, Nilsson K, Alexanderson K (2017) Sickness absence and disability pension after breast cancer diagnosis: a 5-year nationwide cohort study. J Clin Oncol 35(18):2044–2052. https://doi.org/10.1200/jco.2015.66.0613
Eaker S, Wigertz A, Lambert PC, Bergkvist L, Ahlgren J, Lambe M, on behalf of the Uppsala/Örebro Breast Cancer G (2011) Breast cancer, sickness absence, income and marital status. A study on life situation 1 year prior diagnosis compared to 3 and 5 years after diagnosis. PloS One 6(3):e18040. https://doi.org/10.1371/journal.pone.0018040
Ganem G, Antoine EC, Touboul C, Naman H, Dohollou N, Facchini T, Coscas Y, Lortholary A, Catala S, Jacquot S, Lhomel C, Eisinger F (2016) Maintaining professional activity during breast cancer treatment. Eur J Cancer Care 25(3):458–465. https://doi.org/10.1111/ecc.12460
Nordgren L, Söderlund A (2016) Associations between socio-demographic factors, encounters with healthcare professionals and perceived ability to return to work in people sick-listed due to heart failure in Sweden: a cross-sectional study. Disabil Rehabil 38(2):168–173. https://doi.org/10.3109/09638288.2015.1031289
Nordgren L, Söderlund A (2016) Heart failure clients’ encounters with professionals and self-rated ability to return to work. Scand J Occup Ther 23(2):115–126. https://doi.org/10.3109/11038128.2015.1078840
Östlund GM, Borg KE, Wide P, Hensing GKE, Alexanderson KAE (2003) Clients’ perceptions of contact with professionals within healthcare and social insurance offices. Scand J Soc Med 31(4):275–282. https://doi.org/10.1080/14034940210165037
Lynoe N, Wessel M, Olsson D, Alexanderson K, Helgesson G (2011) Respectful encounters and return to work: empirical study of long-term sick-listed patients’ experiences of Swedish healthcare. BMJ Open 1(2):e000246. https://doi.org/10.1136/bmjopen-2011-000246
Sturesson M, Edlund C, Falkdal AH, Bernspang B (2014) Healthcare encounters and return to work: a qualitative study on sick-listed patients’ experiences. Prim Health Care Res Dev 15(4):464–475. https://doi.org/10.1017/S1463423614000255
Haugli L, Maeland S, Magnussen LH (2011) What facilitates return to work? Patients experiences 3 years after occupational rehabilitation. J Occup Rehabil 21(4):573–581. https://doi.org/10.1007/s10926-011-9304-6
Klanghed U, Svensson T, Alexanderson K (2004) Positive encounters with rehabilitation professionals reported by persons with experience of sickness absence. Work 22(3):247–254
Olsson D, Alexanderson K, Bottai M (2015) What positive encounters with healthcare and social insurance staff promotes ability to return to work of long-term sickness absentees? Scand J Soc Med 44(1):91–97. https://doi.org/10.1177/1403494815608098
Upmark M, Borg K, Alexanderson K (2007) Gender differences in experiencing negative encounters with healthcare: a study of long-term sickness absentees. Scand J Public Health 35(6):577–584. https://doi.org/10.1080/14034940701362194
Mussener U, Svensson T, Soderberg E, Alexanderson K (2008) Encouraging encounters: sick-listed persons’ experiences of interactions with rehabilitation professionals. Soc Work Health Care 46(2):71–87
Arfi A, Baffert S, Soilly AL, Huchon C, Reyal F, Asselain B, Neffati S, Rouzier R, Hequet D (2018) Determinants of return at work of breast cancer patients: results from the OPTISOINS01 French prospective study. BMJ Open 8(5):e020276. https://doi.org/10.1136/bmjopen-2017-020276
Nilsson M, Olsson M, Wennman-Larsen A, Petersson LM, Alexanderson K (2011) Return to work after breast cancer: women’s experiences of encounters with different stakeholders. Eur J Oncol Nurs 15(3):267–274. https://doi.org/10.1016/j.ejon.2011.03.005
Johnsson A, Fornander T, Rutqvist L-E, Vaez M, Alexanderson K, Olsson M (2009) Predictors of return to work ten months after primary breast cancer surgery. Acta Oncol 48(1):93–48. https://doi.org/10.1080/02841860802477899
Petersson LM, Wennman-Larsen A, Nilsson M, Olsson M, Alexanderson K (2011) Work situation and sickness absence in the initial period after breast cancer surgery. Acta Oncol 50(2):282–288. https://doi.org/10.3109/0284186x.2010.533191
Amin MB, Edge SB, Greene FL, et al (eds) (2017) AJCC Cancer staging manual, 8th edn. Springer, New York
IBM Corp (Released 2016) IBM SPSS statistics for windows. Version 22.0. Edn. IBM Corp., Armonk, NY
Harrington CB, Hansen JA, Moskowitz M, Todd BL, Feuerstein M (2010) It’s not over when it’s over: long-term symptoms in cancer survivors—a systematic review. Int J Psychiatry Med 40(2):163–181. https://doi.org/10.2190/PM.40.2.c
Blinder V, Patil S, Eberle C, Griggs J, Maly RC (2013) Early predictors of not returning to work in low-income breast cancer survivors: a 5-year longitudinal study. Breast Cancer Res Treat 140(2):407–416. https://doi.org/10.1007/s10549-013-2625-8
Drageset S, Lindstrøm TC, Underlid K (2016) “I just have to move on”: Women’s coping experiences and reflections following their first year after primary breast cancer surgery. Eur J Oncol Nurs 21(Supplement C):205–211. https://doi.org/10.1016/j.ejon.2015.10.005
Kyriakides S (2015) Survivorship care after early breast cancer. Breast 24:S163–S164. https://doi.org/10.1016/j.breast.2015.07.038
Mussener U, Festin K, Upmark M, Alexanderson K (2008) Positive experiences of encounters with healthcare and social insurance professionals among people on long-term sick leave. J Rehabil Med 40(10):805–811. https://doi.org/10.2340/16501977-0259
Bondesson T, Petersson LM, Wennman-Larsen A, Alexanderson K, Kjeldgard L, Nilsson MI (2016) A study to examine the influence of health professionals’ advice and support on work capacity and sick leave after breast cancer surgery. Support Care Cancer 24(10):4141–4148. https://doi.org/10.1007/s00520-016-3239-6
Statistic Sweden (2018) http://www.scb.se/en/finding-statistics/statistics-by-subject-area/labour-market/labour-force-surveys/labour-force-surveys-lfs/. Accessed 12.03. 2018
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The project was approved by the Regional Ethical Review Board in Stockholm, Sweden, Dnr: 2007/612–31/4, 2009/1623–32, 2013/713–32, 2014/1874–32.
Conflict of interest
The authors declare they have no competing interests. The data cannot be made publically available according to Swedish regulations and laws. Readers may contact professor Kristina Alexanderson (kristina.alexanderson@ki.se).
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Söderman, M., Friberg, E., Alexanderson, K. et al. Women’s experiences of encounters with healthcare professionals’ regarding work after breast-cancer surgery and associations with sickness absence: a 2-year follow-up cohort study. Support Care Cancer 27, 1197–1206 (2019). https://doi.org/10.1007/s00520-018-4453-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-018-4453-1