
Abstract
Background
Meta-analyses on the comparison between fusion and prosthesis in the treatment of cervical radiculopathy mainly analyse studies including mixed patient populations: patients with radiculopathy with and without myelopathy. The outcome for patients with myelopathy is different compared to those without. Furthermore, apart from decompression of the spinal cord, restriction of motion is one of the cornerstones of the surgical treatment of spondylotic myelopathy. From this point of view, the results for arthroplasty might be suboptimal for this category of patients. Comparing clinical outcome in patients exclusively suffering from radiculopathy is therefore a more valid method to compare the true clinical effect of the prosthesis to that of fusion surgery.
Aim
The objective of this study was to compare clinical outcome of cervical arthroplasty (ACDA) to the clinical outcome of fusion (ACDF) after anterior cervical discectomy in patients exclusively suffering from radiculopathy, and to evaluate differences with mixed patient populations.
Methods
A literature search was completed in PubMed, EMBASE, Web of Science, COCHRANE, CENTRAL and CINAHL using a sensitive search strategy. Studies were selected by predefined selection criteria (i.a.) patients exclusively suffering from cervical radiculopathy), and risk of bias was assessed using a validated Cochrane Checklist adjusted for this purpose. An additional overview of results was added from articles considering a mix of patients suffering from myelopathy with or without radiculopathy.
Results
Eight studies were included that exclusively compared intervertebral devices in radiculopathy patients. Additionally, 29 articles concerning patients with myelopathy with or without radiculopathy were studied in a separate results table. All articles showed intermediate to high risk of bias. There was neither a difference in decrease in mean NDI score between the prosthesis (20.6 points) and the fusion (20.3 points) group, nor was there a clinically important difference in neck pain (VAS). Comparing these data to the mixed population data demonstrated comparable mean values, except for the 2-year follow-up NDI values in the prosthesis group: mixed group patients that received a prosthesis reported a mean NDI score of 15.6, indicating better clinical outcome than the radiculopathy patients that received a prosthesis though not reaching clinical importance.
Conclusions
ACDF and ACDA are comparably effective in treating cervical radiculopathy due to a herniated disc in radiculopathy patients. Comparing the 8 radiculopathy with the 29 mixed population studies demonstrated that no clinically relevant differences were present in clinical outcome between the two types of patients.
Graphic abstract
These slides can be retrieved under Electronic Supplementary Material.

Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Anterior cervical discectomy with fusion (ACDF) is considered the standard surgical treatment for cervical radiculopathy. Decompressing the nerve root aims to diminish radicular complaints and adding a cage to the intervertebral space aims to maintain foraminal height and cervical alignment [1,2,3]. In the past three decades, the use of a disc prosthesis (ACDA) is being investigated as an alternative treatment for patients with symptomatic cervical radiculopathy caused by cervical disc herniation. The rationale for the use of a prosthesis is to avoid loss of motion at the target level, which is a consequence of treating radiculopathy with ACDF. It is hypothesized that loss of motion causes neck disability and increased mechanical stress at the adjacent levels, possibly causing acceleration of degeneration at these adjacent segments (adjacent segment degeneration; ASD) [4, 5].
Comparing the results of ACDF and ACDA has been done before in systematic reviews and meta-analyses. An overview of Bartels et al. (2017) considered 21 meta-analyses in which the included studies tended to conclude that ACDA gave a better outcome, but differences were small and not clinically relevant [6]. However, it appeared that the meta-analyses considered mainly randomized controlled trials (RCTs) that were performed on mixed patient populations: patients suffering from primarily radiculopathy and patients suffering from primarily myelopathy.
Myelopathy is presumed to be generally occurring in another type of patient, namely the patient with the more degenerated spine. Implanting a prosthesis in these patients may not lead to the optimal effect that is aimed for by implanting a prosthesis. Comparing the outcome of fusion versus prosthesis in patients that primarily suffer form myelopathy may therefore have a different outcome than evaluation of outcome in patients that suffer primarily from radiculopathy.
In this review, only studies that discuss clinical findings in patients with primary complaints of radiculopathy, excluding those suffering primarily from myelopathy, are evaluated. Additionally, outcome of these findings will be compared to clinical outcome reported in the articles considered in the meta-analyses that evaluate mixed patient populations.
Materials and methods
Literature search strategy
The initial literature search strategy was performed in PubMed, EMBASE, Web of Science, COCHRANE, CENTRAL and CINAHL on 2 August 2016, and all English- and Chinese-language publications on the comparison of ACDF and ACDA were retrieved. Two of the authors separately evaluated the articles by title, abstract or full text, when necessary, to select the studies that met the predefined selection criteria. One author translated two relevant articles from Chinese to English. The search strategies used in the different databases were based on the search string as shown in Fig. 1.

Search strategy. Search strategy that was used to perform the literature search 2 August 2016
Article selection was based upon the following criteria:
-
The study compares ACDF to ACDA in one-level anterior discectomy.
-
The study includes at least twenty patients in each treatment arm.
-
The study provides follow-up data for at least 2 years.
-
The study measures primary or secondary outcome in either the Neck Disability Index (NDI) or Visual Analogue Scale neck pain (VAS neck pain).
-
The study only includes patients suffering from radiculopathy, excluding patients suffering from myelopathy.
-
The article is not a meeting abstract.
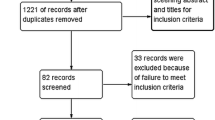
Any discrepancy in selection between the reviewers was resolved in open discussion, and, if needed, a third reviewer was asked to make a final decision. Reference screening and citation tracking were performed on the identified articles (Fig. 2).

Flow chart of article selection process radiculopathy articles. Flow chart describing the search process for the articles exclusively including patients suffering from cervical radiculopathy
When the literature search was repeated in August 2017, a meta-analysis by Bartels et al. was found [6].
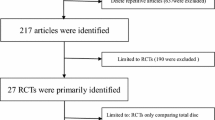
In this study, 21 meta-analyses were evaluated that focused on the outcomes of one-level arthroplasty. The included meta-analyses primarily described studies that allowed inclusion of patients suffering from cervical myelopathy. In order to be complete in our overview, the studies described in the meta-analyses were evaluated additionally in separate mixed group tables. This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA Statement [7] (Fig. 3).

Flow chart of article selection process mixed group articles. Flow chart describing the search process for the articles including patients suffering from cervical myelopathy with or without radiculopathy
Quality assessment
The methodological quality of all studies (including those from the RCTs describing mixed populations) was assessed by three independent reviewers (XY, TJ, CG), using an adjusted version of the checklist for cohort studies of the Dutch Cochrane Center [8]. If there was no consensus about the assessment, a fourth reviewer (CVL) was consulted.
Studies could be maximally awarded 9 points. Studies were then divided into low (7–9 points), intermediate (5–6 points) or high (4 or less points) risk of bias.
Outcome measures
For matters of comparison, the most frequently used outcome parameters were extracted in this systematic review: the Neck Disability Index (NDI) and the Visual Analogue Scale (VAS) for neck pain. In addition, data on reoperations and complications were collected.
The NDI is a ten-item scaled questionnaire on three different aspects of neck complaints: pain intensity, daily-work-related and non-work-related activities. Each item is scored from 0 to 5, and the raw total score ranges from 0 (best score) to 50 (worst score) [10]. Several studies indicate a MCID for NDI of 20 points on a 100-point scale [11, 12].
As many authors choose to present NDI scores on a 100-point scale, the outcome scores in this article were converted to that scale.
The Visual Analogue Scale (VAS) is the most commonly used tool to assess pain intensity. 0 mm indicates ‘no pain’ and 100 mm indicates the ‘worst pain imaginable’. According to the literature, the minimal clinical important difference (MCID) is approximately 20 mm, or 2.0 on a ten-point scale [9]. As most articles presented the VAS scores ranging from 0 to 10, we chose to convert all VAS scores to that scale in order to properly analyse and compare the data. If articles reported the NRS scores for neck pain instead of the VAS, articles were nevertheless considered eligible for inclusion because the two scales are very similar.
After performing the systematic literature review, it will be evaluated whether data can be pooled and if heterogeneity (using I2) can be calculated.
Level of evidence
The quality of evidence for all outcome parameters was evaluated using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach according to Atkins [13] and adapted from Furlan [14].
Results
Search results and study selection of studies describing radiculopathy patients
A total of 603 articles were identified, of which 357 original articles remained after removing duplicates. Titles and abstracts were screened, resulting in 42 eligible articles. These articles were read full-text, and 14 studies met all inclusion criteria. Six articles were additionally excluded after meticulously investigating the literature. The article from Burkus et al. [15] had to be excluded because it also contained patients suffering from myelopathy. The article reports on the 7-year results of a study comparing ACDF versus prosthesis. The study population seemed to consist of patients with only radiculopathy. However, while searching for earlier follow-up results from this study, the article describing the 2-year follow-up results of this population was found [16]. From that particular article, it was clear that the study population was a mixed one, also including patients with myelopathy and therefore Burkus’ article was excluded.
Five of the remaining 12 studies concerned the same RCT comparing Prodisc-C versus ACDF (autograft bone and plate). Therefore, the four studies with shorter follow-up time were excluded (one with 2-year, one with 4-year, one with 5-year and one with 7-year follow-up results) [17,18,19,20]. We decided to only include the article describing the 7-year results (the longest follow-up period) without the continued access group [21].
Additionally, one more study was excluded since it described the 1-year follow-up results [22], while the 3-year follow-up results [23] were also available; eight studies remained that fulfilled all inclusion criteria.
Two RCTs described results on the Mobi-C prosthesis in comparison with ACDF methods using autograft alone [24] and securing with a plate [25]. Additionally, there was one retrospective study (Mobi-C vs PEEK cage without plate) [26] and one prospective cohort study comparing different types of prostheses (Prestige ST, Bryan, Prodisc-C) [27] versus ACDF (PEEK cage without plate). Two other RCTs compared the Prodisc-C prosthesis to ACDF with plate fixation [21, 23], and one RCT compared the Bryan prosthesis or Kineflex|C to ACDF with plate [28]. Lastly, one article described the comparison between the Discover prosthesis and a PEEK cage without plate [29].
The mean number of patients per group in the 8 included trials was 48. The mean age of the patients was 44.7 (ACDA) and 45.4 (ACDF) years, and the percentage of male patients was 46.1% (ACDA) and 49.0% (ACDF) (Table 1).
Search results and study selection of studies describing mixed patient groups
From the 21 meta-analyses retrieved from Bartels’ article, 172 articles were found eligible for screening and after duplicates were removed 46 remained for full-text assessment. One article was selected for analysis in the radiculopathy group, as it described a population of patients from which myelopathy patients were excluded. Ten other articles were excluded because they did not report on the relevant clinical outcome measures or solely on radiological outcome parameters. Lastly, from the 35 articles that matched all inclusion criteria six articles had to be removed because they reported on the same RCTs, in which case we chose to include the article describing the longest follow-up period. Finally, 29 articles were found eligible for the mixed group overview, all reporting on the comparison between ACDA and ACDF in patients suffering from myelopathy with or without radiculopathy [15, 30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57].
In the 29 included articles, the mean follow-up period was 3 years, mean number of patients per group was 90 (ACDA) and 78 (ACDF), and the mean age 45 (ACDA) and 46 (ACDF) years. Study characteristics for each individual study can be found in Table 2.
Quality assessment
Quality assessment in radiculopathy studies
Only one article scored 7 out of 9 points, illustrating a low risk of bias [29], four articles scored five points [21, 24, 27, 28] and one scored 4 points [23] all indicating an intermediate risk of bias. The two remaining articles scored three points illustrating a high risk of bias [25, 26] (Table 3).
Quality assessment in mixed studies
From the 29 studies, there were two with a low risk of bias [36, 41], 21 with an intermediate risk of bias [15, 30, 31, 33,34,35, 38,39,40, 42,43,44,45,46,47,48,49,50, 54, 55, 57] and six with a high risk of bias [32, 37, 51,52,53, 56] (Table 4).
Clinical outcome
Neck Disability Index (NDI)
Disability in articles describing exclusively radiculopathy patients
Six articles use the NDI as a scale to report on functionality [21, 24,25,26, 28, 29] (Table 5). All articles show a significant improvement in post-operative functionality compared to baseline, for both treatment groups. However, only one article shows a significant difference in NDI between the two treatment groups after 2 years. Though the reported statistically significant difference in that article is not clinically relevant, it shows a more favourable outcome for fusion, as compared to the prosthesis [29].
Level of evidence
The level of evidence is lowered by two levels, since most studies have an intermediate to high risk of bias. Furthermore, the findings are inconsistent as only one article presented a significant difference between the two groups, while the 5 other articles did not. Additionally, only one article succeeded in precisely stating the standard deviation (SD), but only for the baseline NDI estimate [21]. Three other articles provided information from which the SD could be calculated [24, 25, 29], while the remaining four did not [23, 26,27,28]. Therefore, the level of evidence that there is no difference in NDI improvement after 2-year follow-up in radiculopathy patients is low.
Functionality in articles describing mixed patient populations
Twenty-six articles use the NDI as an outcome parameter at baseline, and after 2 years, three articles do not [31, 35, 42]. Five articles report a statistical significant difference between ACDF and ACDA 2 years after surgery in favour of the prosthesis, and the difference is, however, never exceeding the MCID of 20. In contrast to the vast majority of articles, three studies show a small difference in favour of fusion, though not statistically significant [44, 55, 56].
Level of evidence
The level of evidence is lowered by 3 levels. Findings are inconsistent, risk of bias is intermediate to high, and data are not reported sufficiently precise. Additionally, the vast majority of studies received industry sponsoring and authors reported extensive disclosures, which enlarges the probability of reporting bias. Therefore, the level of evidence that there is no difference in NDI improvement after 2-years follow-up in mixed population patients is very low.
Visual Analogue Scale (VAS) neck pain
VAS neck pain in articles describing exclusively radiculopathy patients
Seven of the eight articles used the VAS to grade neck pain, and one article used the NRS score [29]. All articles showed that post-operative pain improved compared to baseline (Table 5). None of the articles demonstrated a statistically significant difference between the ACDA and ACDF group after 2 years.
Level of evidence
The level of evidence is lowered by 1 level, since most studies have an intermediate to high risk of bias. Moreover, only one study reports the exact standard deviations with every estimate [23]. Therefore, the level of evidence is moderate that there is no difference in neck pain improvement after implanting a cage or a prosthesis in cervical radiculopathy patients.
VAS neck pain in articles describing mixed patient populations
Twenty-four articles out of the 29 articles use the VAS neck pain as an outcome measure. All articles showed that neck pain improved post-operatively in comparison with baseline, in both treatment groups. Four articles report a statistically significant difference between the prosthesis and fusion in favour of the prosthesis [46, 50, 51, 57] (Table 6).
Level of evidence
The level of evidence is lowered with three levels. All articles have an intermediate to high risk of bias, the vast majority of studies received industry sponsoring, and authors reported extensive disclosures, which enlarges the probability of reporting bias. Furthermore, findings are inconsistent and estimates of effect are not sufficiently precise as not all articles state the exact data. Therefore, the level of evidence that there is no difference in neck pain improvement after implanting a cage or a prosthesis in mixed population patients is very low.
Reoperations
Reoperation rate in articles describing exclusively radiculopathy patients
Seven of the eight articles reported reoperation rates, of which two articles report statistically significant differences in the rates. One study reports more reoperations in the fusion group [24], and the other higher rates in the prosthesis group [29]. Outcome reporting on the level of reoperation is rather heterogeneous and incomplete; however, the results are suggesting that reoperations are most frequent at the adjacent level for the ACDF group and at the index level for the ACDA group (Table 7).
Reoperation rate in articles describing mixed patient populations
The majority of the articles report on “subsequent surgical interventions”, which include revisions, removals and supplemental fixations. Three of the 29 studies report statistically significant differences between the groups in terms of reoperation rates, all in favour of the arthroplasty group [40, 54].
Complications
Complications in articles describing exclusively radiculopathy patients
The most common complications, apart from reoperations, included; adjacent segment disease (ASD), trauma, ongoing neck and/or arm pain, dysphagia, hoarseness, musculoskeletal pain and infections. Complications were seldom permanent. Four articles described adjacent segment disease [21, 23,24,25], of which only one article described a significantly higher incidence of ASD in ACDF patients [24]. No other statistically significant differences in complication rates were described between the treatment groups.
Complications in articles describing mixed patient populations
Three articles report statistically significant differences in the incidence of complications; the first study found a higher incidence of device-related complications in the ACDF group [48], the second study reported a higher rate of overall adverse events in the ACDA group [38], and the third article found more severe adjacent-level radiographic changes in the ACDF group [33]. Two other articles studied ASD very specifically but couldn’t find statistically significant differences between the two treatment strategies [37, 56]. However, it should be noted that in both article types, the articles that report on ASD use different diagnostic criteria for ASD. This could influence the reliability of the results and thus influence the comparability between articles that describe results on ASD.
Heterogeneity
Pooling results from the eight radiculopathy articles was considered; however, it was found that results were too heterogeneously reported for doing so. The number of studies was small, standard deviations were scarcely reported, p-values were mostly provided for the comparison between baseline and 2 years post-operatively within one treatment group instead of between the treatment group. Pooling the data would therefore require statistical imputation for the majority of the standard deviations and p-values. Articles were also clinically heterogeneous, as NDI and VAS scores were expressed on different scales and some articles reported the exact values after 2 years, while others reported the decline from baseline to 2 years or the difference between ACDA and ACDF at 2 years. Pooling results in mixed group articles has been done previously and is therefore likely not to lead to new insights [58,59,60,61]. Subsequently, this means that heterogeneity tests, such as the I2, were not performed, as data were not pooled.
Discussion
Meticulous literature research reveals that pain and disability scores were comparable in patients after 2 years and not dependent on receiving either a cage or a prosthesis, after anterior cervical discectomy for radiculopathy. Likewise, no difference in outcome scores was found between these surgical interventions in mixed patient populations. The same was true for the reoperation rates and the incidence of adjacent segment degeneration (ASD). After using the GRADE approach, the level of evidence for absence of a difference in neck pain and disability in radiculopathy patients is higher than the level of evidence in the mixed patient population; however, the overall level of evidence was low. This conclusion is in line with a meta-analysis by Bartels from 2010, which demonstrates that most studies comparing ACDF and ACDA are not blinded and that a clinical benefit for the prosthesis is not proven [58].
Several other meta-analyses comparing ACDA and ACDF have been published [59,60,61]. These meta-analyses included mainly studies that did not exclude myelopathy patients. These patients are prone to have more severely degenerated cervical spines and perform different on outcome scales. It is therefore most striking that in this systematic review the mean NDI 2 years post-operatively is lower (better) in the ACDA group with both myelopathy and radiculopathy patients than in the ACDA group with radiculopathy patients. This phenomenon might suggest the presence of bias due to industry sponsoring or lack of blinding. An alternative hypothesis could be that patients with more degenerated cervical spines are used to a certain amount of pain and therefore are more likely to report a better disability or pain score.
This review was set up as a counterweight to the 21 meta-analyses retrieved from Bartels’ article on studies comparing ACDF and ACDA concluding that outcome in prosthesis implanted patients was slightly better than in patients that underwent cervical fusion, although not statistically significant nor clinically relevant. It was hypothesized that outcome could be more convincingly favourable for the prosthesis if only radiculopathy patients would be considered. However, the opposite conclusion had to be drawn. Not only were the results in radiculopathy patients not different in ACDA and ACDF patients, but careful analysis of literature on mixed patient populations demonstrated that results were comparable in that patient population too. The suggestion that is offered by most of the existing articles, that the prosthesis is clinically superior to fusion, is therefore most likely to be too optimistic.
Another argument that is often used in favour of the prosthesis is claim of superior radiological results in terms of ASD and Range Of Motion (ROM). However, a recent systematic review shows no convincing radiological evidence for superiority of the prosthesis in ASD [62]. Additionally, the authors stress the absence of solid evidence for a correlation between the increased incidence of ASD and worse clinical outcome.
A limitation of the majority of the analysed studies is the use of a combined success score to define which treatment arm performs better. Apart from including an improvement in NDI or VAS score, most of these success scores added ‘neurological success’. This means that an evaluation conducted by the investigator for muscle strength, sensory assessments and reflex assessments was included. These investigator-conducted evaluations are prone to bias as the articles do not mention whether or not the investigator was blinded to the treatment the patient received. When these combined success scores are not taken into account, but only the plain clinical outcome measures and their statistical significance and clinical relevance, the inevitable conclusion is that ACDA is not superior to ACDF.
Based on clinical outcome measures, literature indicates that the results of ACDF and ACDA do not differ in the treatment of cervical radiculopathy. The results are not prominently different in patients suffering from myelopathy with or without radiculopathy. Further research should have more statistical power, should apply specific inclusion criteria to increase the external validity to specific groups of patients, should blind both the patients and the outcome assessor and report long-term follow-up results in order to draw definitive conclusions on the clinical relevance of the prosthesis. With the increase in power, the possibility of performing an additional subgroup analyses should be considered to identify possible subgroups that might benefit more from receiving a prosthesis.
References
Robinson RA, Smith GW (1955) Anterolateral cervical disc removal and interbody fusion for cervical disc syndrome. Bull John Hopkins Hosp. 96:223–224
Cloward RB (1958) The anterior approach for ruptured cervical discs. J Neurosurg 15:602–614
Dereymaeker A, Mulier J: [Vertebral fusion by a ventral approach in cervical intervertebral disk disorders.] Rev Neurol. (Paris) 99:597–616, 19589 (Fr)
Robertson JT, Papadopoulos SM, Traynelis VC (2005) Assessment of adjacent-segment disease in patients treated with cervical fusion or arthroplasty: a prospective 2-year study. J Neurosurg Spine 3:417–423
Eck JC, Humphreys SC, Lim TH et al (2002) Biomechanical study on the effect of cervical spine fusion on adjacent-level intradiscal pressure and segmental motion. Spine 27:2431–2434
Bartels RHMA, Donk RD, Verhagen WIM, Hosman AJF, Verbeek ALM (2017) Reporting the results of meta-analyses: a plea for incorporating clinical relevance referring to an example. Spine J 17(11):1625–1632
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097
Form for quality assessment of a randomized controlled trial (RCT). Dutch Cochrane Quality Assessment. https://netherlands.cochrane.org/sites/netherlands.cochrane.org/files/public/uploads/4.4_rct_checklist.pdf. Accessed 18 Dec 2017
Carreon LY, Glassman SD, Campbell MJ, Anderson PA (2010) Neck Disability Index, short form-36 physical component summary, and pain scales for neck and arm pain: the minimum clinically important difference and substantial clinical benefit after cervical spine fusion. The Spine Journal 10(6):469–474
Vernon H, Mior S (1991) The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther 14(7):409–415
Auffinger BM, Lall RR, Dahdaleh NS, Wong AP, Lam SK, Koski T et al (2013) Measuring surgical outcomes in cervical spondylotic myelopathy patients undergoing anterior cervical discectomy and fusion: assessment of minimum clinically important difference. PLoS ONE 8(6):e67408. https://doi.org/10.1371/journal.pone.0067408
Lauche R, Langhorst J, Dobos GJ, Cramer H (2013) Clinically meaningful differences in pain, disability and quality of life for chronic nonspecific neck pain—a reanalysis of 4 randomized controlled trials of cupping therapy. Complement Ther Med 21(4):342–347. https://doi.org/10.1016/j.ctim.2013.04.005
Atkins D, Best D, Briss P, Eccles M, Falck-Ytter Y (2004) Grading quality of evidence and strength of recommendations. BMJ 328(7454):1490
Furlan AD, Pennick V, Bombardier C, van Tulder M (2009) 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine 34(18):1929–1941
Burkus J, Traynelis V, Haid R, Mummaneni P (2014) Clinical and radiographic analysis of an artificial cervical disc: 7-year follow-up from the Prestige prospective randomized controlled clinical trial. J Neurosurg Spine 21(4):516–528
Burkus JK, Haid RW, Traynelis VC, Mummaneni PV (2010) Long-term clinical and radiographic outcomes of cervical disc replacement with the Prestige disc: results from a prospective randomized controlled clinical trial. J Neurosurg Spine 13:308–318
Delamarter R, Murrey D, Janssen M, Goldstein J, Zigler J, Tay B et al (2010) Results at 24 months from the prospective, randomized, multicenter Investigational Device Exemption trial of ProDisc-C versus anterior cervical discectomy and fusion with 4-year follow-up and continued access patients. SAS J 4(4):122–128
Murrey D, Janssen M, Delamarter R, Goldstein J, Zigler J, Tay B et al (2009) Results of the prospective, randomized, controlled multicenter Food and Drug Administration investigational device exemption study of the ProDisc-C total disc replacement versus anterior discectomy and fusion for the treatment of 1-level symptomatic cervical disc disease. Spine J 9(4):275–286
Zigler J, Delamarter R, Murrey D, Spivak J, Janssen M (2013) ProDisc-C and anterior cervical discectomy and fusion as surgical treatment for single-level cervical symptomatic degenerative disc disease. Spine 38(3):203–209
Loumeau T, Darden B, Kesman T, Odum S, Van Doren B, Laxer EB, Murrey D (2016) A RCT comparing 7-year clinical outcomes of one level symptomatic cervical disc disease (SCDD) following ProDisc-C total disc arthroplasty (TDA) versus anterior cervical discectomy and fusion (ACDF). Eur Spine J 25(7):2263–2270
Janssen M, Zigler J, Spivak J, Delamarter R, Darden B, Kopjar B (2015) ProDisc-C total disc replacement versus anterior cervical discectomy and fusion for single-level symptomatic cervical disc disease. J Bone Joint Surg 97(21):1738–1747
Nabhan A, Ahlhelm F, Shariat K, Pitzen T, Steimer O, Steudel W et al (2007) The ProDisc-C prothesis: clinical and radiological experience 1 year after surgery. Spine 32(18):1935–1941
Nabhan A, Steudel W, Pape D, Ishak B (2007) Segmental kinematics and adjacent level degeneration following disc replacement versus fusion: RCT with three years of follow-up. J Long Term Eff Med Implants 17(3):229–236
Hou Y, Nie L, Pan X, Si M, Han Y, Li J et al (2016) Effectiveness and safety of Mobi-C for treatment of single-level cervical disc spondylosis: a randomised control trial with a minimum of five years of follow-up. Bone Joint J 98B(6):829–833
Zhang H, Shao Y, Chen Y, Hou Y, Cheng L, Si M et al (2014) A prospective, randomised, controlled multicentre study comparing cervical disc replacement with anterior cervical decompression and fusion. Int Orthop 38(12):2533–2541
Park J, Roh K, Cho J, Ra Y, Rhim S, Noh S (2008) Comparative analysis of cervical arthroplasty using mobi-c® and anterior cervical discectomy and fusion using the solis® -cage. J Korean Neurosurg Soc 44(4):217–221
Sala V, Lisi C, Di Natali G, Zanellato S, Dall’Angelo A, Tinelli C et al (2015) Functional and quality of life evaluation after single level cervical discectomy and fusion or cervical disc replacement. G Ital Med Lav 37(4):239–244
Coric D, Kim PK, Clemente JD, Boltes MO, Nussbaum M, James S (2013) Prospective randomized study of cervical arthroplasty and anterior cervical discectomy and fusion with long-term follow-up: results in 74 patients from a single site. J Neurosurg Spine 18(1):36–42
Sundseth J, Fredriksli O, Kolstad F, Johnsen L, Pripp A, Andresen H et al (2017) The Norwegian Cervical Arthroplasty Trial (NORCAT): 2-year clinical outcome after single-level cervical arthroplasty versus fusion—a prospective, single-blinded, randomized, controlled multicenter study. Eur Spine J 26:1225–1235
Cheng L, Nie L, Li M, Huo Y, Pan X (2011) Superiority of the bryan® disc prosthesis for cervical myelopathy: a randomized study with 3-year followup. Clin Orthop Relat Res 469(12):3408–3414
Coric D, Finger F, Boltes P (2006) Prospective randomized controlled study of the Bryan Cervical Disc: early clinical results from a single investigational site. J Neurosurg Spine 4(1):31–35
Coric D, Cassis J, Carew J, Boltes M (2010) Prospective study of cervical arthroplasty in 98 patients involved in 1 of 3 separate investigational device exemption studies from a single investigational site with a minimum 2-year follow-up. J Neurosurg Spine 13(6):715–721
Coric D, Nunley P, Guyer R, Musante D, Carmody C, Gordon C et al (2011) Prospective, randomized, multicenter study of cervical arthroplasty: 269 patients from the Kineflex|C artificial disc investigational device exemption study with a minimum 2-year follow-up. J Neurosurg Spine 15(4):348–358
Davis RJ, Nunley PD, Kim KD et al (2015) Two-level total disc replacement with Mobi-C cervical artificial disc versus anterior discectomy and fusion: a prospective, randomized, controlled multicenter clinical trial with 4-year follow-up results. J Neurosurg Spine 22:15–25
Ding C, Liu H, Hu T et al (2012) Clinical outcomes of Prestige LP cervical disc replacement a prospective controlled single site trail with 24-month follow up. Chin J Orthop 32:32–38
Fay LY, Huang WC, Tsai TY et al (2014) Differences between arthroplasty and anterior cervical fusion in two-level cervical degenerative disc disease. Eur Spine J 23:627–634
Garrido B, Taha T, Sasso R (2010) Clinical outcomes of bryan cervical disc arthroplasty a prospective, randomized, controlled, single site trial with 48-month follow-up. J Spinal Disord Tech 23(6):367–371
Gornet M, Burkus J, Shaffrey M, Nian H, Harrell F (2016) Cervical disc arthroplasty with prestige LP disc versus anterior cervical discectomy and fusion: seven-year outcomes. Int J Spine Surg 10:24
Grasso G (2015) Clinical and radiological features of hybrid surgery in multilevel cervical degenerative disc disease. Eur Spine J 24(Suppl 7):842–848
Hisey M, Zigler J, Jackson R, Nunley P, Bae H, Kim K et al (2016) Prospective, randomized comparison of one-level Mobi-C cervical total disc replacement vs anterior cervical discectomy and fusion: results at 5-year follow-up. Int J Spine Surg 10:10
Hou Y, Liu Y, Yuan W et al (2014) Cervical kinematics and radiological changes after discover artificial disc replacement versus fusion. Spine J 14:867–877
Hacker RJ (2005) Cervical disc arthroplasty: a controlled randomized prospective study with intermediate follow-up results. J Neurosurg Spine 3(6):424–428
Jawahar A, Cavanaugh DA, Kerr EJ, Birdsong EM, Nunley PD (2010) Total disc arthroplasty does not affect the incidence of adjacent segment degeneration in cervical spine: results of 93 patients in three prospective randomized clinical trials. Spine J 10:1043–1048
Kim SW, Limson MA, Kim SB et al (2009) Comparison of radiographic changes after ACDF versus Bryan disc arthroplasty in single and bi-level cases. Eur Spine J 18(2):218–231
Li Z, Yu S, Zhao Y, Hou S, Fu Q, Li F et al (2014) Clinical and radiologic comparison of dynamic cervical implant arthroplasty versus anterior cervical discectomy and fusion for the treatment of cervical degenerative disc disease. J Clin Neurosci 21(6):942–948
Phillips F, Geisler F, Gilder K, Reah C, Howell K, McAfee P (2015) Long-term outcomes of the US FDA IDE prospective, randomized controlled clinical trial comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion. Spine 40(10):674–683
Porchet F, Metcalf NH (2004) Clinical outcomes with the Prestige II cervical disc: preliminary results from a prospective randomized clinical trial. Neurosurg Focus 17:E6
Riew KD, Buchowski JM, Sasso R, Zdeblick T, Metcalf NH, Anderson PA (2008) Cervical disc arthroplasty compared with arthrodesis for the treatment of myelopathy. J Bone Joint Surg Am 90(11):2354–2364
Riina J, Patel A, Dietz JW, Hoskins JS, Trammell TR et al (2008) Comparison of single-level cervical fusion and a metal-on-metal cervical disc replacement device. Am J Orthop (Belle Mead NJ). 37:E71–E77
Rožanković M, Marasanov SM, Vukić M (2017) Cervical disk replacement with discover versus fusion in a single-level cervical disk disease: a prospective single-center randomized trial with a minimum 2-year follow-up. Clin Spine Surg 30(5):515–522
Sasso R, Smucker J, Hacker R, Heller J (2007) Clinical outcomes of BRYAN cervical disc arthroplasty: a prospective, randomized, controlled, multicenter trial with 24-month follow-up. J Spinal Disord Tech 20(7):481–491
Sasso RC, Anderson PA, Riew KD, Heller JG (2011) Results of cervical arthroplasty compared with anterior discectomy and fusion: four-year clinical outcomes in a prospective, randomized controlled trial. J Bone Joint Surg Am 93(18):1684–1692
Steinmetz M, Patel R, Traynelis V, Resnick D, Anderson P (2008) Cervical disc arthroplasty compared with fusion in a workers’ compensation population. Neurosurgery 63(4):741–747
Vaccaro A, Beutler W, Peppelman W, Marzluff J, Highsmith J, Mugglin A et al (2013) Clinical outcomes with selectively constrained SECURE-C cervical disc arthroplasty. Spine 38(26):2227–2239
Wang Y, Cai B, Zhang XS et al (2008) Clinical outcomes of single level Bryan cervical disc arthroplasty: a prospective controlled study. Zhonghua Wai Ke Za Zhi 46:328–332
Yan S, Di J, Shen Y (2017) Adjacent segment degeneration following anterior cervical discectomy and fusion versus the bryan cervical disc arthroplasty. Med Sci Monit 23:2692–2700
Zhang X, Zhang X, Chen C, Zhang Y, Wang Z, Wang B et al (2012) Randomized, controlled, multicenter, clinical trial comparing BRYAN cervical disc arthroplasty with anterior cervical decompression and fusion in China. Spine 37(6):433–438
Bartels R, Donk R, Verbeek A (2010) No justification for cervical disc prostheses in clinical practice. Neurosurgery 66(6):1153–1160
Gao F, Mao T, Sun W, Guo W, Wang Y, Li Z et al (2015) An updated meta-analysis comparing artificial cervical disc arthroplasty (CDA) versus anterior cervical discectomy and fusion (ACDF) for the treatment of cervical degenerative disc disease (CDDD). Spine 40(23):1816–1823
Wu A, Xu H, Mullinix K, Jin H, Huang Z, Lv Q et al (2015) Minimum 4-year outcomes of cervical total disc arthroplasty versus fusion; a meta-analysis based on prospective randomized controlled trials. Medicine 94(15):e665
Zhang Y, Liang C, Tao Y, Zhou X, Li H, Li F et al (2015) Cervical total disc replacement is superior to anterior cervical decompression and fusion: a meta-analysis of prospective randomized controlled trials. PLoS ONE 10(3):e0117826
Yang X, Janssen T, Arts MP, Peul WC, Vleggeert-Lankamp CLA (2018) Radiological follow-up after implanting cervical disc prosthesis in anterior discectomy: a systematic review. Spine J. 18(9):1678–1693. https://doi.org/10.1016/j.spinee.2018.04.021
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict on interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Goedmakers, C.M.W., Janssen, T., Yang, X. et al. Cervical radiculopathy: is a prosthesis preferred over fusion surgery? A systematic review. Eur Spine J 29, 2640–2654 (2020). https://doi.org/10.1007/s00586-019-06175-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-019-06175-y