
Abstract
Purpose
The aim of this study was to validate the use of the Short Musculoskeletal Function Assessment (SMFA) questionnaire in patients with a spine fracture.
Methods
Cross-sectional cohort of individuals that had sustained a spine fracture (C1-L5) one year earlier. Patients were asked to fill out SMFA, Oswestry Disability Index (ODI), EQ-5D-3L and EQ-VAS. Spearman’s rank correlation coefficient (rho) was used to assess convergent validity for each patient-reported outcome measure (PROM). Bland–Altman plots were used to assess PROM agreement.
Results
82 patients completed all questionnaires. The correlations between SMFA Dysfunction and Bother indices and ODI were 0.89 and 0.86, with EQ-5D-3L index 0.89 and 0.80, and with EQ-VAS 0.80 and 0.73, respectively. The correlation for separate categories of the SMFA dysfunction index (daily activities, emotional status, arm and hand function, mobility) ranged between 0.71–0.87 for ODI, 0.72–0.84 for EQ-5D-3L index, and 0.67–0.77 for EQ-VAS. A selection of the ten items of SMFA that had the highest correlations with ODI resulted in a correlation of 0.91. The agreements between SMFA indices and ODI in Bland–Altman plots were good with small differential biases and minimal proportional biases, but worse for SMFA and EQ-5D-3L index and EQ-VAS.
Conclusion
The SMFA indices are highly correlated with ODI in patients with a spine fracture. The Dysfunction index and Bother index, or selected SMFA items, may be used to assess outcome in patients with spine fractures as an alternative to ODI.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Patient-reported outcome measures (PROMs) that accurately measure the impact of spinal injury are important tools to determine optimal treatment and cost-effectiveness [1]. One of the most commonly used condition-specific PROMs for spinal disorders is the Oswestry Disability Index (ODI) [2, 3]. Although developed to measure disability in individuals with degenerative low back pain, ODI has been extensively used in the context of spinal trauma [2, 3].
The Short Musculoskeletal Function Assessment Questionnaire (SMFA) is a self-administered questionnaire developed to measure functional outcome for a wide variety of musculoskeletal disorders [4]. SMFA has been translated to several languages and has been shown to be a reliable and validated PROM in the context of different types of musculoskeletal disorders [5, 6] Although being a condition-specific PROM, SMFA has the advantage, similarly to generic PROMs, of being able to compare outcomes between different types of disorders and treatments within the musculoskeletal system, while still being sensitive for changes that generic PROMs may fail to detect [4, 5, 7]. Although patients with spine disorders have been included in previous studies of SMFA [4, 8], a comparison has never been made with ODI.
The aim of this study was to validate the use of SMFA in patients with spine fracture.
Methods
Study design and setting
This is a prospective, observational cohort study on data collected from consecutive patients.
Study population, data collection and follow-up
Inpatients with a spine fracture from the first cervical vertebra (C1) to the fifth lumbar vertebra (L5) admitted to the Karolinska University Hospital in Huddinge between January 1st 2016 and October 31st 2017 were eligible for inclusion. Patients were treated with either operative or non-operative treatment.
One year after the spine fracture, according to the routines of the Swedish Fracture Register, all patients were sent questionnaires by regular mail. The flow chart of the study is shown in Fig. 1. For this report, 82 patients with complete data for the planned analyses were included.

Flow chart of the study
Patient-reported outcome measures (PROMs)
Short musculoskeletal function assessment (SMFA)
SMFA is a condition-specific questionnaire developed to assess outcome for a wide range of musculoskeletal disorders [4]. It consists of 46 items divided into two parts, corresponding to the patient’s dysfunction and bother. The ‘dysfunction’ part consists of 34 questions related to difficulties performing different types of activities of daily life. The dysfunction items are divided into four categories–daily activities, emotional status, arm and hand function and mobility. The ‘bother’ part consists of 12 questions where the patient grades how bothered they are during certain activities. Each item is graded from 1–5 with 1 being good function and 5 being poor. The final scores of the dysfunction and bother parts are then converted into their respective indices, the ‘Dysfunction index’ and ‘Bother index’, ranging from 0–100 with the formula \(\left[ {{{\left( {{\text{actual }}\;{\text{score}} {-}{\text{ lowest }}\;{\text{possible }}\;{\text{score}}} \right)} \mathord{\left/ {\vphantom {{\left( {{\text{actual }}\;{\text{score}} {-}{\text{ lowest }}\;{\text{possible }}\;{\text{score}}} \right)} {{\text{possible}}\;{\text{ range }}\;{\text{of }}\;{\text{score}}}}} \right. \kern-0pt} {{\text{possible}}\;{\text{ range }}\;{\text{of }}\;{\text{score}}}}} \right] \times 100\) with higher score indicating poorer outcome [4].
EQ-5D-3L
The EQ-5D-3L is a generic health-related quality of life questionnaire developed by the EuroQol Group [9]. EQ-5D-3L has five items relating to five dimensions of health – mobility, self-care, usual activities, pain/discomfort and anxiety/depression that are graded in three levels (no problems, moderate problems or severe problems). The EQ-5D-3L index reflects the societal perspective of health and ranges from approximately 1 (best) to 0 (worst) in the Swedish experience-based value set using the time-trade-off method [10]. EQ-5D-3L is also accompanied by a visual analogue scale (EQ-VAS), where the patient rates his or her health on a scale from 0 to 100, where 0 equals worst and 100 equals the best possible health.
Oswestry disability index (ODI)
ODI is a condition-specific questionnaire specifically developed to assess outcome in patients with low back pain [2]. Each of the ten ODI items has six answers and is graded 0–5, with 0 corresponding to no disability and 5 to highest disability. The items are converted into an index by the formula \(\left( {{{{\text{total}}\;{\text{score}}} \mathord{\left/ {\vphantom {{{\text{total}}\;{\text{score}}} {{\text{total}}\;{\text{possible}}\;{\text{score}}}}} \right. \kern-0pt} {{\text{total}}\;{\text{possible}}\;{\text{score}}}}} \right) \times 100\) giving a range from 0–100 with higher score indicating poorer outcome [11].
Missing data
Both ODI and SMFA have strategies for handling missing data. If only one item was missing for the ODI the index formula was adjusted so the total score equaled 45 instead of 50 [11], and patients with two or more missing items were excluded [12]. If more than one value was answered for an item, the highest score was counted [11]. Missing values for the Dysfunction index of SMFA was replaced by substituting with the mean value for that category if the missing data for that category was less than 50% [4]. If more than 50% of a single category in the Dysfunction index was missing the patient was excluded. For the Bother index substitution is not possible, since each question represents a unique situation and patients with any missing item on the Bother index were excluded. Patients with any missing data on the five dimensions of EQ-5D-3L were excluded from the study. Patients with unanswered EQ-VAS were included in the study (n = 6).
Statistics
Histograms were used to visually inspect for normality of data. Continuous data are presented descriptively with means, medians, quantiles, minimum, maximum and standard deviations. Categorical data are presented as numbers and percentages.
Ceiling and floor effects were considered present if more than 15% of the patients achieved the best and worst score respectively for each PROM [13]. Spearman’s rank correlation coefficient was used to determine convergent validity between PROMs. Spearman’s rho of 0–0.29 was considered as negligible, 0.30–0.49 as low, 0.50–0.69 as moderate, 0.70–0.89 as high and 0.90–1.0 as very high [14]. Confidence intervals for the Spearman correlations were calculated using Fisher Z-transformation [15]. Bland–Altman plots (means plotted against mean difference) including the limits of agreement defined as the range expected to include 95% of the differences between instruments (± 1.96 × standard deviation of difference) were used to visually determine the agreement between PROMs [16].
We investigated whether a subset of the SMFA items could be used as substitute for ODI. To test this a correlation matrix was made for all individual items of SMFA and ODI, using Spearman’s correlations. The ten individual items of SMFA with the highest correlation with the individual items of ODI were chosen and an index was generated, by us named the SMFA Modified index, ranging from 0–100 was calculated similarly to the Dysfunction and Bother index using the formula: \(\left[ {{{\left( {{\text{actual }}\;{\text{score}} {-}{\text{ lowest }}\;{\text{possible }}\;{\text{score}}} \right)} \mathord{\left/ {\vphantom {{\left( {{\text{actual }}\;{\text{score}} {-}{\text{ lowest }}\;{\text{possible }}\;{\text{score}}} \right)} {{\text{possible}}\;{\text{ range }}\;{\text{of }}\;{\text{score}}}}} \right. \kern-0pt} {{\text{possible}}\;{\text{ range }}\;{\text{of }}\;{\text{score}}}}} \right] \times 100\).
To ease comparisons with SMFA and ODI in plots and tables the EQ-5D-3L index was inverted and multiplied by 100, and EQ-VAS inverted.
All statistical analyses were performed using RStudio software version 4.1.0 for Windows (R Foundation for Statistical Computing). Significance was set to p < 0.05.
Ethics
The study was conducted in accordance with the ethical principles of the Helsinki Declaration and was approved by the Regional Ethical Review Board in Stockholm, Sweden (Dnr 2016/897–31/1).
Results
Patients and descriptive data
Characteristics of the cohort are summarized in Table 1. The results of the PROMs at follow-up are shown in Table 2. All PROMs followed a similar pattern with indices skewed towards full health. Ceiling effects was seen for the ODI, EQ-5D-3L and some of the separate categories in the SMFA. For the SMFA Dysfunction, Bother and Modified index no ceiling effect were present.
SMFA-ODI crosswalk
The Spearman correlations between all individual items of SMFA and ODI was summarized in a matrix. The 10 items of SMFA that had the highest correlation with the 10 ODI items were collected to generate the SMFA Modified index (Appendix 1). Item 9 and 10 of ODI both had the highest correlation with item 25 of SMFA, so the item with the second highest correlation (item 21 of SMFA) was chosen as the corresponding item for item 9 of ODI. Both item 1 and 6 of ODI had the highest correlation with item 36 of SMFA. Item 36 of SMFA was chosen as the corresponding item of item 1 of ODI and the item with the second highest correlation, item 23 of SMFA, was chosen as the corresponding item of item 6 of ODI.
Convergent validity
Correlations between PROMs are summarized in Table 3. All correlations were moderate to high. All SMFA indices, including the indices for each separate category (daily activities, emotional status, arm and hand function, mobility) were highly correlated with ODI (Spearman’s rho 0.71–0.91). All SMFA indices had moderate to high correlations with both the EQ-5D-3L index and EQ-VAS (rho 0.72–0.89 and 0.67–0.82 respectively).
The Spearman correlations for patients with a cervical spine fracture only were moderate to high when comparing the SMFA indices and ODI, EQ-5D-3L and EQ-VAS (rho 0.60–0.88) (Table 3). The Spearman correlations for patients with a thoracic or lumbar fracture only were high between all PROMs (rho 0.79–0.93) with the strongest correlations seen between ODI and the SMFA Modified index (rho = 0.93) (Table 3).
The SMFA indices are plotted against ODI in Fig. 2. All SMFA indices follow a pattern similar to ODI.

Scatter plots of the Short Musculoskeletal Function Assessment (SMFA) Dysfunction index, SMFA Bother index and the SMFA Modified index versus Oswestry Disability Index (ODI) stratified according to sex
Agreement
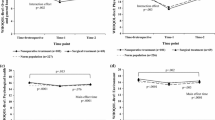
The Bland–Altman plot for the SMFA Modified Index and ODI is shown in Fig. 3. Similar patterns were seen for all other SMFA indices and ODI (data not shown). There were small negative differential biases for all SMFA indices indicating that the ODI tends to score slightly lower compared to SMFA indices. There was a small proportional bias indicating larger differences between SMFA and ODI in patients with larger scores.

Bland–Altman plot comparing the Short Musculoskeletal Function Assessment (SMFA) Modified index and the Oswestry Disability Index (ODI). The y-axis represents the difference between scores and the x-axis represents the mean of both scores. The solid horizontal line represents the mean difference, and the dashed horizontal lines represents the 95% limits of agreement
The SMFA indices and the EQ-5D-3L index showed large negative differential biases as well as a significant proportional bias in the Bland–Altman plots (data not shown). The SMFA indices and the EQ-VAS showed good agreement, with a slight positive differential bias, minimal proportional biases, but with wider limits of agreement compared to SMFA indices and ODI (data not shown).
Discussion
SMFA indices are highly associated with ODI and EQ-5D-3L in patients who have sustained a spine fracture. Both the Dysfunction index and the Bother index, as well as our suggested Modified index of SMFA had high correlations with ODI and good agreement visualized on the Bland–Altman plots. The relationship became slightly higher when only analyzing patients with a thoracic or lumbar fracture. SMFA scores follow ODI scores closely and seem sensitive enough to detect the disabilities associated with a spine fracture, irrespective of fracture site, similarly to ODI.
In our study we found small differential biases indicating that SMFA on average yields higher scores compared to ODI. This may in part be explained by the sheer number of items in SMFA, (46 vs 10), some of which are related, and the number of steps for each item being fewer for SMFA (1–5 for SMFA and 0–5 for ODI). SMFA also contains more items that could be influenced by other musculoskeletal conditions and may therefore give a higher range of scores. There was a small proportional bias between the SMFA indices and ODI, which was most prominent for the Modified index. Although the differential and proportional biases were small, the limits of agreements were wide, so it may not be advisable to use these instruments interchangeably for individual patients, as the scores may differ significantly.
The SMFA indices and the adjusted EQ-5D-3L index did not display a normal distribution of the differences and showed a significant proportional bias, with larger differences for worse health related quality of outcomes in the Bland–Altman plots. This may be explained by the adjusted EQ-5D-3L index not being equal in range of values and not being responsive enough to detect the smaller differences in disability compared to SMFA and ODI. EQ-VAS had a small positive differential bias, but the limits of agreement were very wide, so it may not be advisable to use interchangeably with SMFA for individual patients.
Compared with ODI the SMFA Dysfunction, Bother and Modified index didn’t display a ceiling effect [13, 17]. This shows that SMFA may be better at differentiating more minor disability in patients than ODI. Previous studies have shown that ODI is most effective in patients with more severe symptoms [11]. Future studies comparing SMFA with ODI in patients with spinal disorders should aim to also include patients with severe symptoms.
This study is important in the context of national quality registries in Sweden, since data collection of spine fractures has been transitioned from the Swedish Spine Registry (Swespine) to the Swedish Fracture Register [18]. With the transition, the data collection expanded to also include non-operatively treated patients, whereas before only operatively treated were collected. Swespine uses ODI as the condition-specific instrument, but the Swedish Fracture Register uses SMFA. Unlike ODI, the SMFA can compare outcome in patients with multiple musculoskeletal injuries, and could be used to compare outcome in patients with different types of musculoskeletal diseases [4, 7]. However SMFA has not been used in spine disease related studies before and, prior to this study, no comparison between SMFA and ODI have been made.
There are some limitations that should be acknowledged. Our data collection was limited to one center, only included the outcome for previous inpatients and only reflects one follow-up timepoint. Patients from multiple centers and repeated measurements, both in close proximity for measuring reliability and at different timepoints to detect change over time, as well as a wider range of health utilities would have increased the strength of our study.
The response rate was 54%, although only 80% of the returned questionnaires were complete (43% of total). A reason for the low response rate could be that patients were part of routine care and no reminders were sent. The interest for filling in questionnaires may therefore be low. However, when compared to the response rate in the Swedish Fracture Register overall, the response rate in this study is higher [19, 20]. It is reasonable to believe that our patients that had been treated as inpatients at a referral center may have more severe injuries than the average patient with a spine fracture. Whether this affects the response rate is unknown. Nevertheless, investigating a relationship between different questionnaires may not be affected by the response rate [19, 21].
In this study we did not use the modified version of ODI designed for neck-pain, Neck Disability Index (NDI) [22], in patients with a cervical fracture. Despite this, the correlations were strong which is to be expected, since there is an overlap in the items in ODI and NDI. A previous study by Spiegel et al. [23] found that the correlation (rho) between NDI and ODI in patients with neck pain was 0.755.
Conclusion
The SMFA indices are highly associated with ODI in patients with a spine fracture. The Dysfunction index and Bother index, or selected SMFA items, may be used to assess outcome in patients with a spine fracture as an alternative to ODI. SMFA may be better at differentiating outcomes in patients with less severe symptoms compared to ODI. The SMFA also has the advantage over ODI of being able to compare outcomes between individuals with multiple musculoskeletal injuries, as well as comparing interventions of spine injuries to that of other types of musculoskeletal injuries.
.
Data avalibility
The data used for creating the analyses in this manuscript is available as an Appendix 1.
References
Buijs GS, de Gendt EEA, Sadiqi S, Post MW, Muijs SPJ, Oner FC (2022) Long-Term Reliability and Validity of the AO Spine PROST (Patient-Reported Outcome Spine Trauma). Spine (Phila Pa 1976) 47:562–569. https://doi.org/10.1097/brs.0000000000004379
Fairbank JC, Couper J, Davies JB, O’Brien JP (1980) The Oswestry low back pain disability questionnaire. Physiotherapy 66:271–273
Cutler HS, Guzman JZ, Connolly J, Al Maaieh M, Skovrlj B, Cho SK (2016) Outcome Instruments in spinal trauma surgery: a bibliometric analysis. Global Spine J 6:804–811. https://doi.org/10.1055/s-0036-1579745
Swiontkowski MF, Engelberg R, Martin DP, Agel J (1999) Short musculoskeletal function assessment questionnaire: validity, reliability, and responsiveness. J Bone Joint Surg Am 81:1245–1260. https://doi.org/10.2106/00004623-199909000-00006
Ponzer S, Skoog A, Bergström G (2003) The short musculoskeletal function assessment questionnaire (SMFA): cross-cultural adaptation, validity, reliability and responsiveness of the Swedish SMFA (SMFA-Swe). Acta Orthop Scand 74:756–763. https://doi.org/10.1080/00016470310018324
Wang Y, He Z, Lei L, Lin D, Li Y, Wang G, Zhai H, Xu J, Zhang G, Lin M (2015) Reliability and validity of the Chinese version of the short Musculoskeletal function assessment questionnaire in patients with skeletal muscle injury of the upper or lower extremities. BMC Musculoskelet Disord 16:161. https://doi.org/10.1186/s12891-015-0617-z
Wollmerstedt N, Kirschner S, Faller H, König A (2006) Reliability, validity and responsiveness of the German short Musculoskeletal function assessment questionnaire in patients undergoing surgical or conservative inpatient treatment. Qual Life Res 15:1233–1241. https://doi.org/10.1007/s11136-006-0066-0
Guevara CJ, Cook C, Pietrobon R, Rodríguez G, Nunley J 2nd, Higgins LD, Olson SA, Vail TP (2006) Validation of a Spanish version of the short Musculoskeletal function assessment questionnaire (SMFA). J Orthop Trauma 20:623–629. https://doi.org/10.1097/01.bot.0000246417.07498.4b
Group TE (1990) EuroQol a new facility for the measurement of health-related quality of life. Health Policy 16:199–208. https://doi.org/10.1016/0168-8510(90)90421-9
Burström K, Sun S, Gerdtham UG, Henriksson M, Johannesson M, Levin L, Zethraeus N (2014) Swedish experience-based value sets for EQ-5D health states. Qual Life Res 23:431–442. https://doi.org/10.1007/s11136-013-0496-4
Roland M, Fairbank J (2000) The Roland–morris disability questionnaire and the oswestry disability questionnaire. Spine (Phila Pa 1976) 25:3115–3124. https://doi.org/10.1097/00007632-200012150-00006
Fairbank JC, Pynsent PB (2000) The oswestry disability index. Spine (Phila Pa 1976) 25:2940–2952. https://doi.org/10.1097/00007632-200011150-00017
McHorney CA, Tarlov AR (1995) Individual-patient monitoring in clinical practice: are available health status surveys adequate? Qual Life Res 4:293–307. https://doi.org/10.1007/bf01593882
Mukaka MM (2012) Statistics corner: a guide to appropriate use of correlation coefficient in medical research. Malawi Med J 24:69–71
Bonett D, Wright T (2000) Sample size requirements for estimating pearson, kendall and spearman correlations. Psychometrika 65:23–28. https://doi.org/10.1007/BF02294183
Giavarina D (2015) Understanding bland altman analysis. Biochem Med (Zagreb) 25:141–151. https://doi.org/10.11613/bm.2015.015
Lim CR, Harris K, Dawson J, Beard DJ, Fitzpatrick R, Price AJ (2015) Floor and ceiling effects in the OHS: an analysis of the NHS PROMs data set. BMJ Open 5:e007765. https://doi.org/10.1136/bmjopen-2015-007765
Wennergren D, Ekholm C, Sandelin A, Möller M (2015) The Swedish fracture register: 103,000 fractures registered. BMC Musculoskelet Disord 16:338. https://doi.org/10.1186/s12891-015-0795-8
Juto H, Gärtner Nilsson M, Möller M, Wennergren D, Morberg P (2017) Evaluating non-responders of a survey in the Swedish fracture register: no indication of different functional result. BMC Musculoskelet Disord 18:278. https://doi.org/10.1186/s12891-017-1634-x
Wennergren D, Möller M (2018) Implementation of the Swedish Fracture Register. Unfallchirurg 121:949–955. https://doi.org/10.1007/s00113-018-0538-z
Lindman I, Olsson H, Öhlin A, Hamrin Senorski E, Stålman A, Ayeni OR, Sansone M (2020) Loss to follow-up: initial non-responders do not differ from responders in terms of 2-year outcome in a hip arthroscopy registry. J Hip Preserv Surg 7:281–287. https://doi.org/10.1093/jhps/hnaa028
Vernon H, Mior S (1991) The neck disability index: a study of reliability and validity. J Manipulative Physiol Ther 14:409–415
Spiegel MA, Lafage R, Lafage V, Ryan D, Marascalchi B, Trimba Y, Ames C, Harris B, Tanzi E, Oren J, Vira S, Errico T, Schwab F, Protopsaltis TS (2016) Developing the total disability index based on an analysis of the interrelationships and limitations of oswestry and neck disability index. Spine (Phila Pa 1976) 41:74–81. https://doi.org/10.1097/brs.0000000000001159
Acknowledgements
We acknowledge all physicians and patients contributing data, and Christina Hell for the help with questionnaire distribution.
Funding
Open access funding provided by Karolinska Institute. The work for this study was funded by a grant from CIMED/Karolinska Institutet and the Swedish Research Council (number 2020–00493). Paul Gerdhem was supported by Uppsala University and Region Stockholm. The funding sources had no influence on this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of Interest
None of the authors have any conflicts of interest to declare. None of the authors had any financial or proprietary interests in any material discussed in this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Appendix 1. Items of SMFA with the highest Spearman correlations with ODI generating the Modified index.
Appendix 1. Items of SMFA with the highest Spearman correlations with ODI generating the Modified index.
See Table 4
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Blixt, S., Mukka, S., Försth, P. et al. Validity of the short musculoskeletal function assessment questionnaire in patients with a spine fracture. Eur Spine J 32, 1471–1479 (2023). https://doi.org/10.1007/s00586-023-07581-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07581-z