
Abstract
Purpose
The aim of the study was to determine the effect of trauma etiology on the management, functional outcomes and psychiatric characteristics of suicide jumpers and patients who accidentally fall from height.
Methods
89 patients (48 accidental falls and 41 suicidal jumpers) who had undergone spinal surgery were included in the study. The patients were evaluated clinically and radiologically. Visual Analog Scale (VAS), Roland Morris Disability Questionnaire (RMDQ) and McGill Pain Questionnaire (MPQ) were performed for functional evaluation. BECK hopelessness scale (BHS), BECK depression inventory (BDI), and SF-36 scales were used for the psychiatric evaluation. All outcomes were compared between suicidal jumpers and accidental falls.
Results
The RMDQ and ODI questionnaires stated a higher disability in the suicide jump group (p = 0.001 and p = 0.029, respectively). However, the VAS and MPQ questionnaires did not differ in significance between groups (p = 0.182 and p = 0.306, respectively). The SF-36 scale showed that physical function, role emotional, vitality and mental health subdomains were worse in the suicide jump group (p = 0.001, p = 0.029, p = 0.014 and p = 0.030, respectively). BDI scores were significantly higher in the suicide jump group while no difference was observed between the groups in terms of BSH (p = 0.017 and p = 0.940, respectively).
Conclusion
Psychiatric disorders are more common in patients in the suicidal jumpers. The presence of underlying psychiatric problems adversely affects the postoperative functional outcomes of patients with surgically treated spinal fractures. A multidisciplinary approach together with raising awareness in this way can improve the clinical outcomes after orthopedic treatment, even if there is physical disability.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fall from height occurs as a result of suicide, accident or criminal events [1]. Traumatic spinal injuries are usually caused by high-energy injuries, and one of the most common causes is falling from a height [2]. Depression and psychotic disorders are frequent in patients with spinal injuries due to suicide attempts and require special attention from mental health teams after the rehabilitation period [3]. In patients with mental illness, the risk of complications after falling from height is 1.5 times higher than in patients without it and mental health status can be an important indicator in the prognosis of morbidity [4]. Psychiatric treatments may affect the clinical outcome of orthopedic treatment, especially in suicidal jumpers with spinal injury [5]. The importance of identifying patients at high risk for suicide attempts in case of jumping from height has been previously mentioned in terms of patient management, as they cause more serious injuries and worse outcomes than those who accidentally fall from height [6].
Several studies have compared demographic characteristics, injury patterns, skeletal and blunt trauma exposures of accidental falls and suicidal jumpers [7, 8]. Previous studies examine the demographic characteristics, surgical treatments, combined injuries and psychological histories of spinal fractures that occur as a result of jumping from a height in suicides [9, 10]. In addition, psychiatric disorders have been reported in suicidal jumpers, whether or not they have been diagnosed before [11, 12]. The present study aims to determine the effect of trauma etiology on these parameters by comparing the demographic characteristics, surgical management, clinical results and psychiatric characteristics of suicidal jumpers and patients who accidentally fall from height. Our hypothesis is that suicide intention may adversely affect functional outcomes and mental health status in patients who underwent surgery due to spinal fracture as a result of falling from a height.
Materials and methods
Patients who admitted due to fall from a height between January 2015 and December 2020 were retrospectively examined after local ethics committee approval (IRB decision number: 2022/02 – protocol code: 2022-01-11). A total of 89 patients (48 accidental falls and 41 suicidal jumpers) who had undergone spinal surgery were included in the study. Spinal fractures caused by mechanisms other than falling from height, presence of previous spinal disease, patients who had previous spinal surgery for reasons other than spinal fracture, those with missing medical documents, those under 18 years of age, patients with dementia and cognitive dysfunction, and patients with inadequate follow-up (less than 12 months) were excluded from the study. The patients were evaluated clinically and radiologically. In the clinical evaluation, systemic examination was performed in terms of accompanying injuries in addition to detailed musculoskeletal and neurological examination. Two-planned spinal radiography, computed tomography and magnetic resonance imaging were used in the radiological evaluation.
According to international standards and previous literature, patients with a minimum fall height of 3 m (10 feet, 1 floor) or more were considered as falling from height, and their records were examined in the present study [13]. Suicidal attempt was defined by interviewing the patients and their relatives. Official investigations of the accident scene, eyewitness testimonies, surveillance footage, presence of a suicide note, previous suicide attempts gave us some additional information on the cause of the injury. Psychiatric consultations were requested, and the mental health status of the patients was evaluated through face-to-face interviews. Previous medical records of the patients were checked and the history of mental illness was also evaluated. Both orthopedic and psychiatric retrospective analysis were performed.
In the orthopedic data evaluation, the patients were examined in terms of parameters such as demographic characteristics, trauma and fracture characteristics, accompanying injuries, surgical time, instrumentation level, follow-up period (months), amount of bleeding and complications. In the radiological evaluation, preoperative and final thoracic kyphosis angle (TKA), lumbar lordosis angle (LLA) and final sagittal balance were measured. LLA was calculated by measuring between the lumbar lordosis to thoracic kyphosis inflection point and the S1 upper end-plate as described by Roussouly [14]. TKA was measured between the T4 upper end-plate and T12 lower end-plate as described in the literature due to the superposition of the humeral heads and the poor quality of normal radiographs [15]. Sagittal balance was defined as the horizontal distance between the C7 plumb line and the posterior-superior S1 corner [16]. Visual Analog Scale (VAS), Roland Morris Disability Questionnaire (RMDQ), Oswestry Disability Index (ODI) and McGill Pain Questionnaire (MPQ), which have Turkish validity and reliability studies, were used in functional evaluation [17,18,19,20].
In the psychiatric data evaluation, the patients were investigated for the presence of known/unknown psychiatric disease by 2 senior psychiatrist. The patients were classified as previously diagnosed or newly diagnosed at admission. BECK hopelessness scale (BHS), BECK depression inventory (BDI), and SF-36 scales with Turkish validity and reliability studies were performed [21,22,23]. Psychiatric scale outcomes were compared between suicidal jumpers and accidental falls. All patients were operated under general anesthesia in the prone position and under the guidance of fluoroscopy with a standard posterior approach. Posterior instrumentation and fusion (if necessary) were performed. The patients were followed up monthly for the first 6 months and then every 6 months.
Statistical analysis
NCSS (Number Cruncher Statistical System) program was used for statistical analysis. Descriptive statistical methods (mean, standard deviation, median, frequency, percentage, minimum, maximum) were used for evaluation of the study data. The conformity of the quantitative data to the normal distribution was tested with the Shapiro–Wilk test and graphical examinations. Student t test was used for comparisons between two groups of normally distributed quantitative variables, and Mann–Whitney U test was used for comparisons between two groups of non-normally distributed quantitative variables. Dependent groups t test was used for within-group comparisons of normally distributed quantitative variables. Pearson chi-square test and Fisher–Freeman–Halton test were used to compare qualitative data. Statistical significance was accepted as p < 0.05.
Results
The descriptive characteristics of the patients are presented in Table 1. The lower mean age and the higher female sex rate compared to the falling from height group were noteworthy in the suicide jump group (p = 0.001 and p = 0.019, respectively). Accompanying trauma and presence of psychiatric illness was statistically more frequent in the suicide jump group (p = 0.021 and p = 0.001, respectively). Compression fractures were frequent in patients who fell from height while burst and especially chance fractures were more common in suicide patients (p = 0.001). It was observed that the patients in the suicide jump group had a significantly higher need for blood transfusion in the perioperative period (p = 0.018).
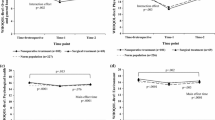
No difference was found between the groups in terms of the preoperative TKA and LLA (p = 0.954 and p = 0.940, respectively). Although the postoperative TKA and LLA improved significantly in both group, the alterations of TKA and LLA were statistically significant only in the fall from height group (p = 0.001). However, no difference was observed between the groups in terms of final sagittal balance (Table 2).
The RMDQ and ODI questionnaires stated a higher disability in the suicide jump group (p = 0.001 and p = 0.029, respectively). However, the VAS and MPQ questionnaires did not differ in significance between groups (p = 0.182 and p = 0.306, respectively). Although there was no difference between the groups in terms of pain scores, it was noteworthy that the disability was higher in the suicide jump group. The SF-36 scale showed that physical function, role emotional, vitality and mental health subdomains were worse in the suicide jump group (p = 0.001, p = 0.029, p = 0.014 and p = 0.030, respectively). BDI scores were significantly higher in the suicide jump group while no difference was observed between the groups in terms of BSH (p = 0.017 and p = 0.940, respectively) (Table 3).
Discussion
The most important finding of our study is that although the pain scores of suicidal jumpers and patients who accidentally fell from height did not differ and their radiological results improved significantly, disability was significantly higher in suicidal jumpers. Another important finding is that depression scores were significantly higher in the suicide group. Recent studies comparing the injury patterns of accidental falls and suicidal jumpers indicate a high incidence of spinal fractures [7, 8, 24,25,26,27]. In addition, there are some studies that examine only suicidal spinal fractures and especially compare suicidal spinal fractures with spinal fractures caused by other trauma mechanisms [9, 10]. The differences between intentionally and unintentionally fall in patients who underwent surgery for spinal fractures as a result of falling from a height were investigated in the present study. demographic characteristics, radiological and functional outcomes, and psychiatric/mental health conditions.
An autopsy study that retrospectively analyzed cases of suicidal jump and accidental falls has stated that victims of suicide were younger, had more serious injuries (thorax, abdomen, pelvis, upper and lower extremities) and had psychiatric histories in most of them [24]. Several studies reported that suicidal jumpers are younger than accidental falls, and female gender predominates, head, chest, abdomen and extremity injuries are more common in suicidal jumpers, and they have higher trauma severity scores than those who accidentally fall from a height [6, 7, 25, 27]. In our study, similar to the literature, the average age of suicidal jumpers was young and the female sex ratio was high. In addition, the presence of concomitant trauma and psychiatric illness was statistically more common in suicidal jumpers. The higher frequency of concomitant injuries in suicidal jumpers may be related to their higher jumping heights. However, due to the retrospective nature of our study, it was not possible to document exactly how high the patients jumped. In the present study, mental problems such as psychosis and depression, as well as bipolar disease, domestic violence or asperger’s/epilepsy were observed more frequently in suicidal jumpers. Therefore, assessment of the functional recovery of patients with mental illness could be difficult. In the present study, psychiatric evaluations were evaluated by 2 senior psychiatrists. As mentioned in the material and method section of our study, patients with "cognitive dysfunction", which was among the exclusion criteria, were excluded from the study. In other words, patients with psychiatrically complete cognitive function (stable mental abilities, including memory, language and rational thinking) were included to obtain the accurate outcomes.
Nielsen et al. stated that the majority of survivors of suicide attempts by jumping were diagnosed with psychotic illness [11]. A study comparing suicidal jumpers and accidentally falls from a height showed that female suicidal jumpers had a low average age (high number of adolescents) and the majority of them had psychiatric disorders [12]. Those literature data also support our study results. Cervical spine lesions are less common in fall survivors, while thoracic and lumbar spine and especially thoracolumbar junction injuries predominate [10, 26]. The occurrence of a burst fracture of the spine has been reported to be an important feature of suicidal jumping [9]. In the present study, compression fractures were more common in patients who accidentally fell from a height. Burst and especially chance fracture were prominent in suicidal jumpers. Although there was a significant difference between the two groups in terms of fracture morphology, no difference was observed between fracture region (thoracic, lumbar, and thoracolumbar).
Suicide jumpers may not be able to give objective and accurate answers. The minimum follow-up period for patients who have undergone surgery was 24 months. It was stated that the follow-up was monthly in the first 6 months and then, every 6 months. Psychiatric diseases have periods of exacerbation and remission. Patients whose minimum follow-up has exceeded 24 months and whose follow-up has not been interrupted are likely to be in psychiatric remission. The most commonly used scales for functional outcomes after spinal fracture treatment are SF-36, RMDQ, and ODI, and VAS is reported as most frequently used scale for the evaluation of the back pain [28]. A prospective cohort study by Siebenga et al. emphasizes that the RMDQ and VAS scales have a strong positive correlation with each other in measuring disability in a group of patients with back pain, whether or not operated for a thoracolumbar spine fracture [29]. Similarly, the VAS and MPQ questionnaires did not significantly differ between the groups in the present study. Although there was no difference between the groups in terms of pain scores, disability was higher in the suicide group according to the RMDQ and ODI questionnaires. Physical pain can be affected by a variety of factors and can be distorted by patients with mental illness and affect the interpretation of physical symptoms [30]. This perception of pain is different even in psychiatric subdisease groups (schizophrenia/bipolar) [31]. In addition, how to measure the functionality and disability of psychiatric patients are an issue that is gaining importance in the world of psychiatry. Instead of discussing symptoms with patients with mental illness, mental health doctors focus on what they cannot do because these symptoms interfere with daily activities. Psychotherapists and psychiatrists provide guidance to patients and other clinicians about the content and process of functional assessment [32]. Similarly, pain and functional evaluation along with psychiatric evaluation were evaluated with the help of 2 experienced psychiatrists in the current study. The risk of major depression after spinal fracture due to chronic pain and limitation of activities of daily living can be reduced by early surgical interventions and medications [33]. In our study, depression scores were significantly higher in the suicide group, and no difference was observed between the groups in terms of hopelessness.
In a previous study, differences were found in clinical and radiological results after various clinical and radiological evaluations such as VAS, ODI, sagittal index and local kyphosis angle in thoracolumbar fractures. This has been attributed to the lack of standardized clinical and radiological criteria [34]. Bouyer et al. reported that although deformity correction was optimal in the postoperative radiological evaluation of patients with thoracic or lumbar fractures, the SF-36 criteria showed deterioration compared to the general population scores [35]. Radiological outcome measures may not always correlate with clinical outcomes [36, 37]. Verlan et al. stated that no technique could restore and protect the fractured segment at the physiological level in the surgically treated thoracic and lumbar spine regardless of the severity of the injury, but the results appeared better than expected in terms of pain and return to work [38]. Posterior instrumentation and fusion (if necessary) were performed to the patients in our study. Postoperative TKA and LLA improved significantly in both groups. No difference was observed between the groups in terms of pain scores. In the present study, although the postoperative radiological measurements and pain scores of the patients were similar, the disability scores were worse in the suicide group. In addition, the outcomes of the physical function, role emotional, vitality and mental health subdomains of the SF-36 scale were worse in suicidal jumpers. BHS results were similar in both groups, while BDI scores were higher in the suicide group. We think that disability itself may be due to depression rather than a physical context.
The outcomes of the present study are not surprising. On the other hand, those results lead to further study questions that need to be answered. The strength of the present study is its remarkable study question and straight forward methodology. The limitations of the study are the rather small sample size, the retrospective study design, and lack of randomization. In addition, the lack of standardization of patients with psychiatric diseases in the suicidal jumper group in the evaluation of pain and functional scores is another situation that limits the study. Another limitation is that due to the retrospective design of our study, the data regarding the heights from which the patients fell could not be clearly documented.
Conclusion
Psychiatric disorders are more common in patients in the suicidal jumpers. Therefore, orthopedic surgeons should question the suicide attempt in patients with spinal fractures admitted as a result of falling from a height, and their psychiatric history or mental problems should be taken into account. The presence of underlying psychiatric problems adversely affects the postoperative functional outcomes of patients with surgically treated spinal fractures. We think that a multidisciplinary approach together with raising awareness in this way can improve the clinical outcomes after orthopedic treatment, even if there is physical disability.
References
Greenberg MI (1978) Falls from heights. J Am Coll Emerg Physicians 7(8):300–301. https://doi.org/10.1016/S0361-1124(78)80192-0
Taşoğlu Ö, Koyuncu E, Daylak R, İnce Z, Yenigün D, Özgirgin N (2018) Demographic and clinical characteristics of persons with spinal cord injury in Turkey: one-year experience of a primary referral rehabilitation center. J Spinal Cord Med 41(2):157–164. https://doi.org/10.1080/10790268.2016.1224215
CastañoMonsalve B, Benito Penalva J, Vidal Samsó J (2019) Spinal cord injury due to suicide attempt, psychiatric profile and functional disability. Rev Neurol 68(07):290. https://doi.org/10.33588/rn.6807.2018210
Clous EA, Ponsen KJ, van Hensbroek PB, Luitse JSK, Olff M, Goslings JC (2015) Falling from a height: psychiatric comorbidity and complications. Ned Tijdschr Geneeskd 159:A7729
Yoo JI, Cha Y, Kim JT, Park CH, Choy W, Koo KH (2022) Orthopedic patients with mental disorder: literature review on preoperative and postoperative precautions. Clin Orthop Surg 14(2):155. https://doi.org/10.4055/cios21156
Piazzalunga D, Rubertà F, Fugazzola P, Allievi N, Ceresoli M, Magnone S, Ansaloni L (2020) Suicidal fall from heights trauma: difficult management and poor results. Eur J Trauma Emerg Surg 46(2):383–388. https://doi.org/10.1007/s00068-019-01110-8
Kang BH, Jung K, Huh Y (2021) Suicidal intent as a risk factor for mortality in high-level falls: a comparative study of suicidal and accidental falls. Clin Exp Emerg Med 8(1):16–20. https://doi.org/10.15441/ceem.20.019
Terayama T, Toda H, Tanaka Y, Saitoh D, Yoshino A (2022) Differences in trauma ınjury patterns and severity between ıntentional and accidental falls from a height: a japanese nationwide trauma database study. Cureus. https://doi.org/10.7759/cureus.25861
Kim DY, Choi HJ, Park JY, Kim KH, Kuh SU, Chin DK, Kim KS, Jin BH (2014) Burst fractures as a result of attempted suicide by jumping. Korean J Neurotrauma 10(2):70. https://doi.org/10.13004/kjnt.2014.10.2.70
Kano H, Matsuo Y, Kubo N, Fujimi S, Nishii T (2019) Spinal injuries in suicidal jumpers. Spine 44(1):13–18. https://doi.org/10.1097/BRS.0000000000002757
Nielssen O, Glozier N, Babidge N, Reutens S, Andrews D, Gerard A, Large MM (2010) Suicide attempts by jumping and psychotic illness. Aust N Z J Psychiatry 44(6):568–573. https://doi.org/10.3109/00048671003606086
Faggiani M, Aragno E, Aprato A, Rosso G, Conforti LG, Maina G, Massè A (2020) Falls from height: orthopaedic and psychiatric evaluation. Acta Biomed 91(4-S):79–84. https://doi.org/10.23750/abm.v91i4-S.9366
Nau C, Leiblein M, Verboket RD, Hörauf JA, Sturm R, Marzi I, Störmann P (2021) Falls from great heights: risk to sustain severe thoracic and pelvic injuries increases with height of the fall. J Clin Med 10(11):2307. https://doi.org/10.3390/jcm10112307
Roussouly P, Pinheiro-Franco JL (2011) Sagittal parameters of the spine: biomechanical approach. Eur Spine J 20(S5):578–585. https://doi.org/10.1007/s00586-011-1924-1
Dubousset J, Charpak G, Skalli W, de Guise J, Kalifa G, Wicart P (2008) Modélisation vertébrale et squelettique par le système EOS. Arch Pediatr 15(5):665–666. https://doi.org/10.1016/S0929-693X(08)71868-2
Gelb DE, Lenke LG, Bridwell KH, Blanke K, McEnery KW (1995) An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 20(12):1351–1358
Yaray O, Akesen B, Ocaklioğlu G, Aydinli U (2011) Validation of the Turkish version of the visual analog scale spine score in patients with spinal fractures. Acta Orthop Traumatol Turc 45(5):353–358. https://doi.org/10.3944/AOTT.2011.2528
Küçükdeveci AA, Tennant A, Elhan AH, Niyazoglu H (2001) Validation of the Turkish version of the roland-morris disability questionnaire for use in low back pain. Spine 26(24):2738–2743. https://doi.org/10.1097/00007632-200112150-00024
Yakut E, Düger T, Öksüz Ç, Yörükan S, Üreten K, Turan D, Güler Ç (2004) Validation of the turkish version of the oswestry disability ındex for patients with low back pain. Spine 29(5):581–585. https://doi.org/10.1097/01.brs.0000113869.13209.03
GungorTavsanli N, Ozcelik H, Karadakovan A (2013) Examine of quality of life of elderly indivudals suffering pain. Ağrı J Turk Soc Algolog 25(3):93–110. https://doi.org/10.5505/agri.2013.20082
Seber G, Dilbaz N, Kaptanoğlu C, Tekin D (1993) Umutsuzluk ölçeği: geçerlilik ve güvenirliği. Kriz Derg. 1(3):139–142. https://doi.org/10.1501/Kriz_0000000045
Hisli N (1988) Beck depresyon envanterinin gecerliligi uzerine bir calisma (a study on the validity of beck depression inventory). J Psychol 6:118–122
Koçyiğit H, Aydemir Ö, Ölmez N, Memiş A (1999) Kısa form-36 (KF36)’nın Türkçe versiyonunun güvenirliliği ve geçerliliği. İlaç Tedavi Dergisi 12(2):102–106
Tsellou M, Dona A, Antoniou A, Goutas N, Skliros E, Papadopoulos IN, Papadodima SA (2022) A comparative autopsy study of the injury distribution and severity between suicidal and accidental high falls. Forensic Sci Med Pathol 18(4):407–414. https://doi.org/10.1007/s12024-022-00496-z
Rocos B, Acharya M, Chesser TJS (2015) The pattern of injury and workload associated with managing patients after suicide attempt by jumping from a height. Open Orthop J 9(1):395–398. https://doi.org/10.2174/1874325001509010395
Richter D, Hahn MP, Ostermann PAW, Ekkernkamp A, Muhr G (1996) Vertical deceleration injuries: a comparative study of the injury patterns of 101 patients after accidental and intentional high falls. Injury 27(9):655–659. https://doi.org/10.1016/S0020-1383(96)00083-6
Papadakis SA, Pallis D, Galanakos S, Georgiou DF, Kateros K, Macheras G, Sapkas G (2020) Falls from height due to accident and suicide attempt in Greece. A comparison of the injury patterns. Injury 51(2):230–234. https://doi.org/10.1016/j.injury.2019.12.029
Schoenfeld AJ, Bono CM (2011) Measuring spine fracture outcomes: common scales and checklists. Injury 42(3):265–270. https://doi.org/10.1016/j.injury.2010.11.040
Siebenga J, Leferink VJM, Segers MJM, Elzinga MJ, Bakker FC, Ten DH, Patka P (2008) A prospective cohort study comparing the VAS spine score and Roland-Morris disability questionnaire in patients with a type A traumatic thoracolumbar spinal fracture. Eur Spine J 17(8):1096–1100. https://doi.org/10.1007/s00586-008-0705-y
Kim DJ, Mirmina J, Narine S, Wachtel J, Carbajal JM, Fox H, Cáceda R (2022) Altered physical pain processing in different psychiatric conditions. Neurosci Biobehav Rev 33:104510. https://doi.org/10.1016/j.neubiorev.2021.12.033
Atik L, Konuk N, Akay O, Ozturk D, Erdogan A (2007) Pain perception in patients with bipolar disorder and schizophrenia. Acta Neuropsychiatr 19(5):284–290. https://doi.org/10.1111/j.1601-5215.2007.00193.x
Rogers JC, Holm MB (2016) Functional assessment in mental health: lessons from occupational therapy. Dialogues Clin Neurosci 18(2):145–154. https://doi.org/10.31887/DCNS.2016.18.2/jrogers
Chang CY, Chen WL, Hsieh PY, Ho SY, Huang CC, Lee TH, Lin YR (2020) Clinical treatment and medication in decreasing the development of major depression caused by spinal fracture. J Int Med 48(11):030006052097288. https://doi.org/10.1177/0300060520972885
Acar E, Dinçer D (2019) Evaluation of postoperative clinical and radiological outcomes of thoracolumbar vertebral fractures. Eurasian J Emerg 18(1):9–16. https://doi.org/10.4274/eajem.galenos.2017.66375
Bouyer B, Vassal M, Zairi F, Dhenin A, Grelat M, Dubory A, Lonjon N (2015) Surgery in vertebral fracture: epidemiology and functional and radiological results in a prospective series of 518 patients at 1 year’s follow-up. Orthop Traumatol Surg Res 101(1):11–15. https://doi.org/10.1016/j.otsr.2014.11.012
Knop C, Fabian HF, Bastian L, Blauth M (2001) Late results of thoracolumbar fractures after posterior ınstrumentation and transpedicular bone grafting. Spine 26(1):88–99. https://doi.org/10.1097/00007632-200101010-00016
Andress HJ, Braun H, Helmberger T, Schürmann M, Hertlein H, Hartl WH (2002) Long-term results after posterior fixation of thoraco-lumbar burst fractures. Injury 33(4):357–365. https://doi.org/10.1016/S0020-1383(02)00030-X
Verlaan JJ, Diekerhof CH, Buskens E, Van der Tweel I, Verbout AJ, Dhert WJA, Oner FC (2004) Surgical treatment of traumatic fractures of the thoracic and lumbar spine: a systematic review of the literature on techniques, complications, and outcome. Spine 29(7):803–814. https://doi.org/10.1097/01.brs.0000116990.31984.A9
Funding
Open access funding provided by the Scientific and Technological Research Council of Türkiye (TÜBİTAK).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Çakmur, B.B., Duramaz, A., Çakmur, K.N. et al. Do the management and functional outcomes of the surgically treated spinal fractures change in suicidal jumpers?. Eur Spine J (2024). https://doi.org/10.1007/s00586-024-08259-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00586-024-08259-w