
Abstract
Background
Focused ultrasound (FUS) shows promise for enhancing drug delivery to the brain by temporarily opening the blood–brain barrier (BBB), and it is increasingly used in the clinical setting to treat brain tumours. It remains however unclear whether FUS is being introduced in an ethically and methodologically sound manner. The IDEAL-D framework for the introduction of surgical innovations and the SYRCLE and ROBINS-I tools for assessing the risk of bias in animal studies and non-randomized trials, respectively, provide a comprehensive evaluation for this.
Objectives and methods
A comprehensive literature review on FUS in neuro-oncology was conducted. Subsequently, the included studies were evaluated using the IDEAL-D framework, SYRCLE, and ROBINS-I tools.
Results
In total, 19 published studies and 12 registered trials were identified. FUS demonstrated successful BBB disruption, increased drug delivery, and improved survival rates. However, the SYRCLE analysis revealed a high risk of bias in animal studies, while the ROBINS-I analysis found that most human studies had a high risk of bias due to a lack of blinding and heterogeneous samples. Of the 15 pre-clinical stage 0 studies, only six had formal ethical approval, and only five followed animal care policies. Both stage 1 studies and stage 1/2a studies failed to provide information on patient data confidentiality. Overall, no animal or human study reached the IDEAL-D stage endpoint.
Conclusion
FUS holds promise for enhancing drug delivery to the brain, but its development and implementation must adhere to rigorous safety standards using the established ethical and methodological frameworks. The complementary use of IDEAL-D, SYRCLE, and ROBINS-I tools indicates a high risk of bias and ethical limitations in both animal and human studies, highlighting the need for further improvements in study design for a safe implementation of FUS in neuro-oncology.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
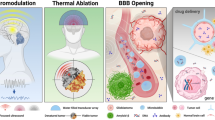
Focused ultrasound (FUS) is a non-invasive technology that utilizes high or low-intensity ultrasound waves to treat (mainly) neurological disorders such as Parkinson’s disease and essential tremors but has recently found promising use in neuro-oncology [19, 26]. The first significant in vivo application of FUS in animals was conducted by Lynn et al. at Columbia University in 1943 [22]. The use of low-intensity ultrasound (LIFUS) with active scalp cooling [8], and pre-procedural imaging to plan the ultrasonic trajectory has greatly improved the efficacy of FUS since then. Ultimately the relentless scientific efforts led to the first major application of FUS in Neurosurgery dates in 1956 by Ballantine et al. at Massachusetts General Hospital [8, 13].
In the field of glioblastoma (GBM) research, among the most aggressive brain tumors, developments of new neuro-oncological treatment strategies have progressed slowly, since Stupp et al. [39] showed that neurosurgical patients receiving chemoradiation with temozolomide have a median survival of mere 14.6 months. To improve the efficacy of novel drugs, researchers have developed a technique that combines low-intensity focused ultrasound (LIFUS) with intravenously injected gas-encapsulated microbubbles (MBs) to extend the duration of the BBB opening [5]. In addition to enhancing drug delivery, FUS has also been found by pre-clinical studies to enhance neuro-oncological immunotherapy and act as a radiosensitiser [18]. Although most clinical studies have been in vitro, FUS is already being used in neurosurgical neuro-oncology, and clinical trials assessing its clinical effect are ongoing [31]. Given that FUS is a relatively novel neurosurgical technology, the question arises whether FUS has been sufficiently scrutinized and undergone evaluation before being used in clinical trials involving humans.
Given the high stakes and narrow margins for error in neurosurgery, particularly for high-risk patients, the evaluation and implementation of surgical devices necessitate strict and meticulous examination. The IDEAL-D framework (Idea, Development, Exploration, Assessment, Long-term study—Devices) has been developed and widely advocated for this purpose. Created by an expert consensus group, the IDEAL-D framework provides a structured approach to the development, evaluation, and implementation of surgical innovations to improve patient outcomes and safety, from first use through clinical practice [10]. However, the adoption of IDEAL(-D) in neurosurgery remains limited [33], likely due to a combination of lack of awareness, insufficient due diligence, and perceptions of the framework as impractical. Nevertheless, to ensure the safety of neurosurgical patients, knowledge of and adherence to the framework are crucial.
Building upon the underpinnings of the IDEAL-D framework and its significance in neurosurgery, the combined application of the SYstematic Review Centre for Laboratory animal Experimentation (SYRCLE) tool and Risk Of Bias In Non-randomized Studies—of Interventions (ROBINS-I) tool emerges as an effective strategy for bolstering the methodological evaluation and uncovering potential biases in various stages of surgical innovation. Using SYRCLE and ROBINS-I together with the IDEAL-D framework allows for a more robust evaluation of the methodological quality and potential biases in studies at various stages of surgical innovation development. SYRCLE is a tool designed to assess the risk of bias in animal studies, while ROBINS-I aims to identify potential biases in non-randomized studies of interventions. Therefore, this article aims to assess whether the IDEAL-D framework has been followed for the introduction of FUS in neuro-oncology, as well as evaluate the methodological quality and risk of bias in studies using SYRCLE and ROBINS-I tools.
Methodology
A comprehensive narrative literature search was performed searching for all published clinical and preclinical studies, as well as registered trials, on the use of focused ultrasound in neuro-oncology. The search terms used can be found in Supplementary Digital Content Table 1, and the PRISMA flowchart can be found in Supplementary Digital Content Table 2. The search was done using the following databases: “Embase,” “Medline,” “PubMed,” and “ClinicalTrials.gov.” No date limiters were applied. The final search date was December 31, 2022. Inclusion criteria were original studies examining the use of FUS in the context of BBB disruption and enhanced drug delivery in the treatment of brain tumors, clinically or pre-clinically, written in the English language. Reviews were excluded. Data on the various parameters were extracted as per IDEAL framework recommendations on their website idealcollaboration.com [36], a detailed list of the extracted parameters can be found in Supplementary Digital Content Table 3.
To complement the IDEAL-D framework, the SYRCLE and ROBINS-I tools were also employed in our methodology. The SYRCLE tool is specifically designed to assess the risk of bias in animal studies, while the ROBINS-I tool is used for evaluating the risk of bias in non-randomized trials.
Data extraction was conducted using Microsoft Excel, and graphs were created using the R software (version 4.0.4) [35]. In addition, articles were critically appraised, and the risk of bias was determined against all the domains of the SYRCLE and ROBINS-I tool by two independent reviewers (SGT and JK), and a consensus was reached by discussion.
Results
The literature search yielded 19 original published studies (15 pre-clinical stage 0 studies, two clinical stage 1 studies, and two stage 1/2a) [1, 3, 4, 7, 12, 14, 17, 20, 21, 23, 25, 27,28,29,30, 34, 40, 42, 43], and 12 registered trials [16, 37].
Study and therapy characteristics
The geographical distribution of the studies is illustrated in Fig. 1, with most studies having been conducted in the USA (n = 8). The study characteristics of the original publications are summarised in Table 1 and Fig. 2. The most frequently studied disease types were glioma (not otherwise specified), GBM, and recurrent GBM (Fig. 2A). Rodents were the most commonly used model (Fig. 2B). The most frequently used drugs were Cisplatin (n = 3) and Methotrexate (n = 4). The ExAblate low-frequency ultrasound system (n = 4) and Optison (n = 3) were the most used FUS platforms. Registered trials are all in-human, stage 1, or stage 1/2a studies (Table 2). Seven of these trials are marked as “active and recruiting” (Table 2).

A world map showing the country of origin of the published original studies (n = 19) [1, 3, 4, 7, 12, 14, 17, 20, 21, 23, 25, 27,28,29,30, 34, 40, 42, 43] on therapeutic FUS for BBB modulation. The legend at the bottom denotes the number of studies published per respective country as separate colour. The corresponding author’s country of affiliation was chosen to represent the origin of the study itself

Two bar plots summarise the findings on disease type (A) and sample type (B) examined by the included published original studies on therapeutic FUS for BBB modulation (n = 19) [1, 3, 4, 7, 12, 14, 17, 20, 21, 23, 25, 27,28,29,30, 34, 40, 42, 43]. In the second row, two bar plots summarise the findings on disease type (C) and trial stage and sample size (D) examined by the included registered, but not published, clinical trials on therapeutic FUS for BBB modulation (n = 12) [37].
Outcomes and complications
The primary outcomes of all included studies were focused on investigating the efficacy and safety of BBB disruption using FUS. However, we observed a high degree of heterogeneity among the specific outcome measures used across the studies (Table 3). Of the included studies, five investigated the survival and safety of FUS in BBB disruption, while 11 studies examined the effect of BBB on macromolecular transfer, including medication transfer across the BBB (Table 3). Most animal studies (n = 10) do not report functional outcomes, as they were generally sacrificed after the procedure for histological examination. Interestingly, most published clinical and pre-clinical studies (n = 12) did not report complications, while only five studies reported no complications (Table 3). Nonetheless, most included animal and human studies reported largely positive outcomes in terms of their respective primary and secondary outcomes (n = 17). None of the in-human studies reported direct side effects or complications of FUS therapy. Overall, BBB disruption was reported to be associated with successful disruption of the BBB, increased drug delivery, improved survival rates, and good safety (Table 3).
Stage 0 studies
IDEAL-D analysis
IDEAL-D stage 0 studies involve the preclinical stage of surgical innovation development, focusing on laboratory and animal research, and aim to establish the feasibility, safety, and proof-of-concept for the new technique or device before transitioning to clinical testing (Fig. 3) [10].

A A stacked pie chart summarised the findings of the IDEAL-D analysis of published stage 0 studies (n = 15) [1, 4, 7, 12, 17, 20, 21, 25, 27,28,29,30, 40, 42, 43]. Each ring is denoted with an alphabetical letter and the corresponding categorical variable is denoted in the legend at the bottom of the graph. A) Were all predictable risks to patients investigated before human studies began? B) Were guidelines on best scientific practice and ethics specific to the types of study followed where available? C) Was a minimum dataset describing technical consistency made public before first-in-human testing? D) Did the outcome description address relevant parameters (i.e. Whether intended goal of procedure is accomplished? Level of difficulty of performing procedure or using device as compared to standard of care? Safety risks? Desirability of intervention?) E) Was stage endpoint reached? (Any studies that could avoid predictable risks of failure or harm to the first human should have been conducted.) The colour of the rings correlate to the legend at the right side of the graph and denote whether the categorical variables were fully addressed (“Yes”), incompletely addressed (“Partially”), or not at all addressed (“No”). B Risk of bias summary plot for non-randomized studies with a bar chart of the distribution of risk-of-bias judgments for all included stage 0 studies (n = 15) [1, 4, 7, 12, 17, 20, 21, 25, 27,28,29,30, 40, 42, 43] across the domains of the SYRCLE tool, shown in percentages (%), is shown. At the bottom, an overall risk of bias, which represents the collated risk-of-bias judgements for all domains, is depicted
Of the 15 studies [1, 4, 7, 12, 17, 20, 21, 25, 27,28,29,30, 40, 42, 43] included in the analysis only 4 studies [1, 21, 27, 43] investigated the predictable risks in animal models, while the remaining studies did not address these risks adequately. Most of the studies were scored negatively regarding the exploration of the majority of predictable risks to patients due to the lack of investigation of complex neurological sequelae in the animals, including testing of neurological higher functioning. Among the included studies, Alonso et al. [42] (2013) stood out for following guidelines on best scientific practises and ethics specific to animal studies [11, 32]. None of the other studies, reported on the use of randomization nor participant and investigator blinding. However, all studies made a minimum dataset describing technical consistency before first-in-human testing and addressed relevant parameters as outlined in the methodology section (n = 15/15). Overall, none of the studies fully reached the stage endpoint due to poor methodology, and only six studies partially reached it (Fig. 4A). All scores are also presented in Supplementary Digital Content Table 4.

A stacked pie chart summarised the findings of the IDEAL-D analysis of published stage 1 (excluding stage 1/2a) studies (n = 2) [14, 23]. Each ring is denoted with an alphabetical letter and the corresponding categorical variable is denoted in the legend at the bottom of the graph. A) Were full details of patient selection, technique, and outcomes and patients not selected during the time frame, and why provided? B) Were standard well-defined measures for reporting outcome and patient characteristics used? C) Was a structured reporting system used? D) Was the above information made available to peers regardless of outcome? E) Was stage endpoint reached? (Outcomes will determine whether to proceed to stage 2a.) The colour of the rings correlate to the legend at the right side of the graph and denote whether the categorical variables were fully addressed (“Yes”), incompletely addressed (“Partially”), or not at all addressed (“No”). B Risk of bias summary plot for non-randomized studies with a bar chart of the distribution of risk-of-bias judgments for all included stage 1 studies (n = 2) [3, 34] across the domains of the ROBINS-I tool, shown in percentages (%) is shown. At the bottom, an overall risk of bias, which represents the collated risk-of-bias judgements for all domains, is depicted
Fifteen animal studies were evaluated for their adherence to animal welfare and ethics guidelines. Of the 15 studies, six had formal approval from an animal committee [4, 17, 25, 28, 42, 43], five did not have formal approval but followed appropriate animal care policies [7, 12, 20, 30, 40], and four had no information regarding approval or animal care [1, 21, 27, 29]. Regarding euthanization and anesthesia methods, all studies except one [42] reported appropriate methods. There was a lack of information provided on the level of animal care in most studies. All studies were transparent regarding any conflicts of interest including received grants.
SYRCLE analysis
SYRCLE analysis of 15 studies, presented in Fig. 5 and Supplementary Digital Content Table 5, showed varying degrees of bias across different parameters. Only three studies [7, 28, 43] exhibited a low risk of bias in sequence generation by properly randomizing samples, while the remaining 12 [1, 4, 12, 17, 20, 21, 25, 27, 29, 30, 40, 42] showed concerns or unclear risk, mainly due to lack of randomization. One study [29] notably scored high risk for not employing controls. For baseline characteristics, most studies (12/15) scored low risk of bias; two showed some concerns due to insufficient animal data. Allocation concealment was a concern in most studies (n = 13/15), with two scoring high risk. All studies scored “some concerns” for random housing, with the majority (12/15) not addressing the blinding of caregivers. Only Alonso et al. [42] implemented a low-risk, double-blinding methodology. Random outcome assessment was unclear in most (n = 13/15) studies, with two scoring high risk. Outcome assessor blinding was generally unaddressed (n = 10/15), except for two studies [1, 28]. Incomplete outcome data had low risk in most cases (n = 13/15), with one high-risk exception. All studies scored low risk for selective outcome reporting. Overall, the studies varied in bias risk: four high, seven unclear, and four low. An in-depth explanation of scoring parameters and rationale is provided in Supplementary Digital Content Table 5.

A A stacked pie chart summarised the findings of the IDEAL-D analysis of published stage 1/2a studies (n = 2) [3, 34]. Each ring is denoted with an alphabetical letter and the corresponding categorical variable is denoted in the legend at the bottom of the graph. A) Was a study protocol made available? B) Were standard well-defined measures for reporting outcome and patient characteristics used? C) Were all exclusions reported and explained? D) Were all cases reported sequentially with annotation and explanation of when and why changes to indication or procedure took place? E) Was stage endpoint reached? (Display main outcomes graphically to illustrate the above.) The colour of the rings correlate to the legend at the right side of the graph and denote whether the categorical variables were fully addressed (“Yes”), incompletely addressed (“Partially”), or not at all addressed (“No”). B Risk of bias summary plot for non-randomized studies with a bar chart of the distribution of risk-of-bias judgments for all included stage 1/2a studies (n = 2) [3, 34] across the domains of the ROBINS-I tool, shown in percentages (%) is shown. At the bottom, an overall risk of bias, which represents the collated risk-of-bias judgements for all domains, is depicted
Stage 1 studies
IDEAL-D analysis
Under the IDEAL-D framework [3, 34], stage 1 studies mark the initial foray into human clinical testing, aiming to assess the safety and feasibility of the innovation within a confined patient cohort.
Two studies were included in the analysis (Fig. 4A) [14, 23], both of which had well-defined measures for reporting outcomes and patient characteristics, a structured reporting system, and disclosed all information regardless of outcomes. They partially reached the stage endpoint due to methodological shortcomings, particularly the lack of blinding and randomization. Ethical standards were maintained with formal board approval and informed patient consent, but patient confidentiality procedures were not explicitly described. Both studies fully disclosed any potential conflicts of interest. All scores are also presented in Supplementary Digital Content Table 6.
ROBINS-I analysis
ROBINS-I analysis, summarised in Fig. 4B and Supplementary Digital Content Table 7, of the same two studies, showed a low risk of bias for participant selection, deviations from intended interventions, and selection of the reported result. However, they scored high risk due to confounding factors: heterogenous medication regime for Mainprize et al. [23] and a varied patient sample for Idbaih A et al. [14]. Mainprize et al. [23] also had a moderate risk for classification of intervention and high risk for missing data due to a high dropout rate and missing tumor samples. Both studies had a high risk of bias in outcome measurement due to a lack of blinding. Overall, Mainprize et al [23]. was assessed as having a high risk of bias, while Idbaih A et al. [14] was seen as a moderate risk.
Stage 1/2a studies
IDEAL-D analysis
IDEAL-D stage 1/2a studies [3, 34] are situated a transitional stage between early clinical safety evaluations and the exploration of the novel surgical technique or device in a larger patient cohort. These studies involve refining the technique, determining optimal parameters, and expanding evaluations to multiple centers for more robust safety and efficacy data. Two studies were included in the analysis (Fig. 5A). All scores are also presented in Supplementary Digital Content Table 8.
The analysis revealed that both studies scored positively for making their study protocol available, explaining all exclusions, and reporting all cases sequentially with annotation and explanation of when and why changes to indication or procedure took place. However, the studies were only partially able to reach the stage endpoint of the IDEAL-D framework due to poor outcome reporting methodology. Both stage 1/2a studies obtained formal approval from their respective ethics boards and respected patient autonomy by providing information about the study and gaining informed consent. The studies both ensured patient safety and disclosed any potential conflicts of interest. However, no information regarding the confidentiality of patient data was available.
ROBINS-I analysis
In Fig. 5B and Supplementary Digital Content Table 9, the results of the ROBINS-I analysis are shown (n = 2). The studies [3, 34] demonstrated a low risk of bias in several categories, such as confounding, participant selection, intervention classification, deviations from intended interventions, and missing data. However, they scored highly for bias in outcome measurement due to insufficient description of how neurological outcomes were measured, and moderate risk of other bias due to a lack of blinding. Overall, both studies were classified as having a moderate risk of bias.
Discussion
This methodological analysis of the 15 pre-clinical studies revealed that none fully and only six partially reached the IDEAL stage endpoint for stage 0 studies. Both IDEAL-D stage 1 studies only partially reached the stage endpoint due to poor methodology of blinding and randomization. Of the two stage 1/2a studies, poor outcome reporting meant that the stage endpoint was only partially reached. However, all stage 1 and 1/2a studies stated that they obtained formal approval from their respective ethics boards, respected patient autonomy, and ensured patient safety. Overall, the SYRCLE analysis scored four pre-clinical studies as high, seven studies as unclear, and four studies as low risk of bias. The ROBINS-I analysis for clinical studies showed that the stage 1 studies were scored as moderate (n = 1) and high risk of bias (n = 1), and both stage 1/2a studies were classified as having a moderate risk of bias. Given our methodological findings, the efficacy and safety of BBB disruption using FUS, as summarized in our review, are likely subject to overestimation and lack of generalizability.
The results of the IDEAL-D and SYRCLE analyses suggest that most stage 0 studies investigating FUS in animal models are conducted with poor methodology and a high risk of bias. Specifically, most studies failed to use appropriate animal models, follow guidelines on best scientific practice and ethics specific to animal studies, or adequately address predictable risks to patients, including complex neurological sequelae and testing of neurological higher functioning. The SYRCLE analysis revealed that sequence generation parameters, including baseline characteristics, allocation concealment, random housing, and blinding of caregivers and outcome assessors, were not addressed. The absence of formal animal committee approval in several studies demonstrates a lack of awareness of ethical guidelines by researchers. This is cause for concern as unnecessary animal suffering may jeopardize scientific research efforts and undermine study credibility. Although most studies reported appropriate detail regarding euthanization and methods for anesthesia, information about animal living conditions was frequently omitted. These findings highlight the need for more rigorous methodological standards and adherence to best scientific practice and ethics in stage 0 studies of FUS in animal models.
Our findings suggest that the animal studies have not yet reached the IDEAL-D stage endpoint, indicating that more high-quality non-human studies are necessary to ensure the safety of FUS before translation into humans [24]. However, many human clinical trials have already been registered, and the feasibility of halting them is limited. Thus, increased methodological scrutiny of human studies to ensure the safety and efficacy of FUS is required. Several studies explore the complex neurological side-effects of FUS; however, the lack of bias and randomization in stage 1 and stage 1/2a undermine the reliability and validity of the findings [6]. The current study serves as an important stimulus for employing appropriate measures to ensure the high validity of findings, such as pre-specified endpoints, blinding, and randomization. This would lead to improved reliability of study results and increase the safety of FUS technology for human subjects.
Overall, our results demonstrate a concerning lack of adherence to methodological and ethical frameworks such as IDEAL-D, SYRCLE, and ROBINS-I in studies related to FUS in neurosurgery, with none of the studies fully reaching the IDEAL end stage [11]. One possible explanation for the lack of adherence to methodological and ethical frameworks is a lack of awareness among researchers [8]. While IDEAL-D was developed in the UK, our analysis found that most included studies on FUS were from the USA. This suggests that there may be a need to increase awareness of these frameworks outside of Europe and to encourage researchers to incorporate them into their study protocols [41]. Most studies report positive outcomes of FUS accompanied by few or no complications associated with the technology; however, the lack of adherence to ethical and methodological frameworks, as noted in the analysis, places the reliability and validity of the results obtained into question. Therefore, the efficacy and safety of BBB disruption using FUS, which our study also summarised, may lack accuracy and generalizability and could be a misleading overestimation. Therefore, further research that adheres to ethical and methodological frameworks, such as SYRCLE, ROBINS-I, and IDEAL-D, is needed to confirm the efficacy and safety of FUS for brain tumors and to guide clinical practice.
The present study’s findings may be limited by several factors. While the study used three different appraisal tools, they all have limitations, such as the ROBINS-I tools’ inability to capture all sources of bias [38] and the IDEAL-D tools’ subjective nature [24]. The retrospective application of the IDEAL-D framework in this study may be challenging due to its inherent limitations. The IDEAL-D framework is designed to guide the planning, conduct, and reporting of surgical innovation studies, and applying it retrospectively may present challenges in accurately assessing the study’s methodology and results—it is similar to trying “to put the genie back inside the bottle”. Furthermore, the limited availability of data in some studies may have hindered the ability to assess certain outcomes or biases [9], and the relatively small sample size of studies included may limit the generalizability of the findings [2]. Moreover, publication bias may have affected the study’s results, as studies with positive outcomes may be more likely to be published than those with negative outcomes [15]. Despite these limitations, the present study provides important insights into the use of FUS and highlights areas where further research is needed.
Conclusion
In conclusion, our narrative analysis of FUS studies in the field of neuro-oncology has uncovered important concerns about the ethical and methodological foundations of this emerging technology. Our detailed evaluation reveals a potential for bias and a concerning degree of methodological inconsistency, issues which have the potential to significantly compromise the validity of reported safety and efficacy outcomes. Particularly concerning is the noted deficit in compliance with recognized methodological and ethical standards, including the IDEAL-D, SYRCLE, and ROBINS-I frameworks. Animal studies were particularly found wanting in this regard, necessitating a renewed commitment to ethical and methodological rigor to ensure robust results that can effectively inform subsequent clinical trials. Given the considerable number of registered human clinical trials, the urgent requirement for improvements in study quality cannot be overstated. Further, the noted geographical disparity in adherence to frameworks like IDEAL-D makes a compelling case for a global initiative to standardize research methodologies. Future research in this field must work assiduously to address these shortcomings, uphold stringent ethical norms, and refine trial methodologies. This is crucial to ensure that the implementation of FUS in neuro-oncology practice is both safe and effective.
Data availability
Provided in the supplementary file.
Code availability
Available on request.
Abbreviations
- BBB:
-
Blood-brain barrier
- FUS:
-
Focused ultrasound
- IDEAL:
-
Idea, Development, Exploration, Assessment, Long-term follow-up
- IDEAL-D:
-
IDEAL Description, an expanded version of IDEAL
- ROBINS-I:
-
Risk Of Bias In Non-randomized Studies—of Interventions
- SYRCLE:
-
Systematic Review Centre for Laboratory animal Experimentation
- UK:
-
United Kingdom
- US:
-
United States
- WHO:
-
World Health Organization
References
Alonso A, Reinz E, Leuchs B et al (2013) Focal delivery of AAV2/1-transgenes into the rat brain by localized ultrasound-induced BBB opening. Mol Ther Nucleic Acids 2:e73. https://doi.org/10.1038/MTNA.2012.64
Bottigliengo D, Baldi I, Lanera C et al (2021) Oversampling and replacement strategies in propensity score matching: a critical review focused on small sample size in clinical settings. BMC Med Res Methodol 21(1). https://doi.org/10.1186/s12874-021-01454-z
Carpentier A, Canney M, Vignot A et al (2016) Clinical trial of blood-brain barrier disruption by pulsed ultrasound. Sci Transl Med 8(343). https://doi.org/10.1126/SCITRANSLMED.AAF6086/SUPPL_FILE/8-343RE2_SM.PDF
Chen PY, Hsieh HY, Huang CY, Lin CY, Wei KC, Liu HL (2015) Focused ultrasound-induced blood-brain barrier opening to enhance interleukin-12 delivery for brain tumor immunotherapy: a preclinical feasibility study. J Transl Med 13(1):1–12. https://doi.org/10.1186/S12967-015-0451-Y/TABLES/1
Conti A, Kamimura HAS, Novell A, Duggento A, Toschi N (2020) Magnetic resonance methods for focused ultrasound-induced blood-brain barrier opening. Front Phys 8. https://doi.org/10.3389/fphy.2020.547674
Elias WJ, Lipsman N, Ondo WG et al (2016) A randomized trial of focused ultrasound thalamotomy for essential tremor. N Engl J Med 375(8):730–739. https://doi.org/10.1056/NEJMOA1600159
Fan CH, Ting CY, Chang YC, Wei KC, Liu HL, Yeh CK (2015) Drug-loaded bubbles with matched focused ultrasound excitation for concurrent blood–brain barrier opening and brain-tumor drug delivery. Acta Biomater 15:89–101. https://doi.org/10.1016/J.ACTBIO.2014.12.026
Harary M, Segar DJ, Huang KT, Tafel IJ, Valdes PA, Cosgrove GR (2018) Focused ultrasound in neurosurgery: a historical perspective. Neurosurg Focus 44(2):E2. https://doi.org/10.3171/2017.11.FOCUS17586
Higgins JPT, Thomas J, Chandler J, et al (2019) Cochrane Handbook for Systematic Reviews of Interventions. https://doi.org/10.1002/9781119536604
Hirst A, Philippou Y, Blazeby J et al (2019) No surgical innovation without evaluation: evolution and further development of the IDEAL framework and recommendations. Ann Surg 269(2):211–220. https://doi.org/10.1097/SLA.0000000000002794
Hooijmans CR, Rovers MM, De Vries RBM, Leenaars M, Ritskes-Hoitinga M, Langendam MW (2014) SYRCLE’s risk of bias tool for animal studies. BMC Med Res Methodol 14(1):43. https://doi.org/10.1186/1471-2288-14-43
Hsu PH, Wei KC, Huang CY et al (2013) Noninvasive and targeted gene delivery into the brain using microbubble-facilitated focused ultrasound. PLoS One 8(2):e57682. https://doi.org/10.1371/JOURNAL.PONE.0057682
Hynynen K, Clement GT, McDannold N et al (2004) 500-Element ultrasound phased array system for noninvasive focal surgery of the brain: a preliminary rabbit study with ex vivo human skulls. Magn Reson Med 52(1):100–107. https://doi.org/10.1002/MRM.20118
Idbaih A, Canney M, Belin L et al (2019) Safety and feasibility of repeated and transient blood-brain barrier disruption by pulsed ultrasound in patients with recurrent glioblastoma. Clin Cancer Res 25(13):3793–3801. https://doi.org/10.1158/1078-0432.CCR-18-3643/74166/AM/SAFETY-AND-FEASIBILITY-OF-REPEATED-AND-TRANSIENT
Ioannidis JPA (2018) Why most published research findings are false. In: Getting to Good: Research Integrity in the Biomedical Sciences. https://doi.org/10.1371/journal.pmed.0020124
Karmur BS, Philteos J, Abbasian A et al (2020) Blood-brain barrier disruption in neuro-oncology: strategies, failures, and challenges to overcome. Front Oncol 10:1811. https://doi.org/10.3389/FONC.2020.563840/BIBTEX
Kinoshita M, McDannold N, Jolesz FA, Hynynen K (2006) Noninvasive localized delivery of Herceptin to the mouse brain by MRI-guided focused ultrasound-induced blood-brain barrier disruption. Proc Natl Acad Sci U S A 103(31):11719–11723. https://doi.org/10.1073/PNAS.0604318103/SUPPL_FILE/04318FIG4.PDF
Kovacsa ZI, Kima S, Jikariaa N et al (2017) Disrupting the blood-brain barrier by focused ultrasound induces sterile inflammation. Proc Natl Acad Sci U S A 114(1):E75–E84. https://doi.org/10.1073/PNAS.1614777114/SUPPL_FILE/PNAS.201614777SI.PDF
Lipsman N, Meng Y, Bethune AJ et al (2018) Blood–brain barrier opening in Alzheimer’s disease using MR-guided focused ultrasound. Nat Commun 9(1):2336. https://doi.org/10.1038/s41467-018-04529-6
Liu HL, Hua MY, Yang HW et al (2010) Magnetic resonance monitoring of focused ultrasound/magnetic nanoparticle targeting delivery of therapeutic agents to the brain. Proc Natl Acad Sci U S A 107(34):15205–15210. https://doi.org/10.1073/PNAS.1003388107/SUPPL_FILE/PNAS.201003388SI.PDF
Liu HL, Hua MY, Chen PY et al (2010) Blood-brain barrier disruption with focused ultrasound enhances delivery of chemotherapeutic drugs for glioblastoma treatment. Radiology 255(2):415–425. https://doi.org/10.1148/RADIOL.10090699/ASSET/IMAGES/LARGE/10090699FIG08F.JPEG
Lynn JG, Putnam TJ (1944) Histology of cerebral lesions produced by focused ultrasound. Am J Pathol. 20(3):637. Accessed May 21, 2023. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2033152/
Mainprize T, Lipsman N, Huang Y et al (2019) Blood-brain barrier opening in primary brain tumors with non-invasive MR-guided focused ultrasound: a clinical safety and feasibility study. Sci Rep 9(1):1–7. https://doi.org/10.1038/s41598-018-36340-0
McCulloch P, Altman DG, Campbell WB et al (2009) No surgical innovation without evaluation: the IDEAL recommendations. Lancet 374(9695):1105–1112. https://doi.org/10.1016/S0140-6736(09)61116-8
McDannold N, Vykhodtseva N, Hynynen K (2006) Targeted disruption of the blood–brain barrier with focused ultrasound: association with cavitation activity. Phys Med Biol 51(4):793. https://doi.org/10.1088/0031-9155/51/4/003
McDannold N, Clement GT, Black P, Jolesz F, Hynynen K (2010) Transcranial magnetic resonance imaging- guided focused ultrasound surgery of brain tumors: initial findings in 3 patients. Neurosurgery 66(2):323–332. https://doi.org/10.1227/01.NEU.0000360379.95800.2F
McDannold N, Arvanitis CD, Vykhodtseva N, Livingstone MS (2012) Temporary disruption of the blood-brain barrier by use of ultrasound and microbubbles: safety and efficacy evaluation in rhesus macaques. Cancer Res 72(14):3652–3663. https://doi.org/10.1158/0008-5472.CAN-12-0128/650292/AM/TEMPORARY-DISRUPTION-OF-THE-BLOOD-BRAIN-BARRIER-BY
McDannold N, Zhang Y, Supko JG et al (2019) Acoustic feedback enables safe and reliable carboplatin delivery across the blood-brain barrier with a clinical focused ultrasound system and improves survival in a rat glioma model. Theranostics 9(21):6284. https://doi.org/10.7150/THNO.35892
Mehier-Humbert S, Bettinger T, Yan F, Guy RH (2005) Plasma membrane poration induced by ultrasound exposure: implication for drug delivery. J Control Release 104(1):213–222. https://doi.org/10.1016/J.JCONREL.2005.01.007
Mei J, Cheng Y, Song Y et al (2009) Experimental study on targeted methotrexate delivery to the rabbit brain via magnetic resonance imaging–guided focused ultrasound. J Ultrasound Med 28(7):871–880. https://doi.org/10.7863/JUM.2009.28.7.871
Meng Y, Pople CB, Budiansky D, Li D, Suppiah S, Lim-Fat MJ, Perry J, Sahgal A, Lipsman N (2022) Current state of therapeutic focused ultrasound applications in neuro-oncology. J Neurooncol 156(1):49–59. https://doi.org/10.1007/s11060-021-03861-0
Muhlhausler BS, Bloomfield FH, Gillman MW (2013) Whole animal experiments should be more like human randomized controlled trials. PLoS Biol 11(2). https://doi.org/10.1371/JOURNAL.PBIO.1001481
Ota HCU, Smith BG, Alamri A et al (2020) The IDEAL framework in neurosurgery: a bibliometric analysis. Acta Neurochir (Wien) 162(12):2939–2947. https://doi.org/10.1007/S00701-020-04477-5/TABLES/2
Park SH, Kim MJ, Jung HH et al (2020) Safety and feasibility of multiple blood-brain barrier disruptions for the treatment of glioblastoma in patients undergoing standard adjuvant chemotherapy. J Neurosurg 134(2):475–483. https://doi.org/10.3171/2019.10.JNS192206
R Core Team (n.d.) R: a language and environment for statistical. R Foundation for statistical Computing, Vienna, Austria
Recommendations - Ideal. Accessed May 21, 2023. https://www.ideal-collaboration.net/the-ideal-framework/recommendations/
Search of: focused ultrasound | Brain Cancer - List Results - ClinicalTrials.gov. Accessed May 23, 2023. https://clinicaltrials.gov/ct2/results?cond=Brain+Cancer&term=focused+ultrasound&cntry=&state=&city=&dist=
Sterne JA, Hernán MA, Reeves BC et al (2016) ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ (Online) 355. https://doi.org/10.1136/bmj.i4919
Stupp R, Mason WP, van den Bent MJ et al (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352(10):987–996. https://doi.org/10.1056/NEJMOA043330/SUPPL_FILE/987SA1.PDF
Treat LH, McDannold N, Vykhodtseva N, Zhang Y, Tam K, Hynynen K (2007) Targeted delivery of doxorubicin to the rat brain at therapeutic levels using MRI-guided focused ultrasound. Int J Cancer 121(4):901–907. https://doi.org/10.1002/IJC.22732
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP (2014) The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg 12(12):1495–1499. https://doi.org/10.1016/j.ijsu.2014.07.013
Wei KC, Chu PC, Wang HYJ et al (2013) Focused ultrasound-induced blood–brain barrier opening to enhance temozolomide delivery for glioblastoma treatment: a preclinical study. PLoS One 8(3):e58995. https://doi.org/10.1371/JOURNAL.PONE.0058995
Ziadloo A, Burks SR, Gold EM et al (2012) Enhanced homing permeability and retention of bone marrow stromal cells by noninvasive pulsed focused ultrasound. Stem Cells 30(6):1216–1227. https://doi.org/10.1002/STEM.1099
Author information
Authors and Affiliations
Contributions
S.G.T. was involved in conceptualisation, methodology, supervision, visualisation, and writing—original draft and writing—revised draft. M.L.D.B. was involved in conceptualisation, methodology, supervision, writing—original draft and writing—revised draft. All other authors were involved in writing—original draft and writing—revised draft.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Comments
The process of developing new therapies and medical devices is a critical component of advancing healthcare and improving patient outcomes and identifying new strategies for the treatment of malignant gliomas is paramount. Although the ethical issues raised by the authors are extremely important, in recent years, concerns have been raised about the impact of excessive regulations on the pace of innovation and the development of new therapies in the clinical and preclinical trial stages. While regulations are undoubtedly important to ensure patient safety and scientific validity of results, my opinion is that an overly burdensome regulatory environment can inadvertently stifle innovation and hinder the progress of novel therapies.
Clinical and preclinical trials serve as the cornerstone of the drug and medical device development process. These trials are designed to rigorously test the safety, efficacy, and potential risks of new treatments before they are approved for widespread use. Regulations are put in place to ensure that these trials are conducted with the utmost ethical standards and scientific rigor, protecting patients from potential harm and preventing unproven treatments from entering the market. However, an excess of regulations can lead to unintended consequences. The lengthy and intricate regulatory processes can substantially prolong the timeline for bringing new therapies to market, resulting in increased development costs and delayed patient access to innovative treatments. High regulatory burdens can also discourage investment in research and development, particularly among smaller biotech companies and startups that may lack the resources to navigate complex regulatory pathways.
Excessive regulations can also stifle the development of treatments for rare and orphan diseases, such as gliomas. As a result, potential treatments for these conditions may face unnecessary hurdles, delaying their availability to patients who have limited options and are in desperate search for care. Furthermore, the risk-averse nature induced by excessive regulations can discourage researchers from exploring high-risk, high-reward therapeutic avenues. Innovation often thrives when researchers are encouraged to take calculated risks and pursue unconventional approaches. Overregulation can hinder this process, favoring more conservative and incremental advancements over potentially groundbreaking ones.
Thus, it must be underscored that the way is finding the right balance between safety and innovation to ensure that patients have timely access to safe and effective treatments while fostering an environment conducive to scientific progress. To this purpose, regulatory agencies, industry stakeholders, and the research community must collaborate to streamline regulatory processes without compromising patient safety. Also, implementing measures such as adaptive trial designs, real-world evidence integration, and improved communication between regulatory agencies and researchers can expedite the evaluation process without compromising rigor. Ultimately, the goal should be to create an environment where groundbreaking therapies can flourish without compromising patient well-being.
Alfredo Conti
Bologna
Italy
This article is part of the Topical Collection on Brain tumors
Previous presentation
None.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
{kind=link}
{kind=link}
Cite this article
Thavarajasingam, S.G., Kilgallon, J.L., Ramsay, D.S.C. et al. Methodological and ethical challenges in the use of focused ultrasound for blood–brain barrier disruption in neuro-oncology. Acta Neurochir 165, 4259–4277 (2023). https://doi.org/10.1007/s00701-023-05782-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-023-05782-5