
Abstract
Purpose
To compare the failure rates and the prevalence of technical complications between full-coverage tooth-supported monolithic zirconia (MZ) and porcelain-veneered zirconia (PVZ) fixed dental prosthesis, based on a systematic literature review.
Methods
An electronic search was performed in three databases, supplemented by hand searching. Several statistical methods were used.
Results
Seventy-four publications reported 6370 restorations (4264 PVZ; 2106 MZ; 8200 abutment teeth; 3549 patients), followed up until 152 months. A total of 216 prostheses failed, and survival was statistically significant different between groups. PVZ had higher occurrence of complications than MZ; the difference was especially greater for either minor or major chipping. The difference in prevalence of either minor or major chipping was statistically significant for PVZ prostheses between cementation with glass ionomer and adhesive resin cement (higher), adhesive resin and resin-modified glass ionomer cement (RMGIC, higher), and between RMGIC (higher) and glass ionomer cement. For MZ the difference was significant only for minor chipping between RMGIC (higher) and adhesive resin cement. Abutment teeth to PVZ prostheses more often lost vitality. Decementation was not observed with RMGIC. Air abrasion did not seem to clinically decrease the decementation risk. The 5-year difference in the occurrence of minor or major chipping between MZ and PVZ prostheses was statistically significant, but nor for catastrophic fracture.
Conclusion
Tooth-supported PVZ prostheses present higher failure and complication rates than MZ prosthesis. The difference in complications is striking when it comes to chipping.
Clinical relevance
Awareness of the outcome differences between different types of zirconia prostheses is important for clinical practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The development of yttria-stabilized tetragonal zirconia polycrystalline (Y-TZP) for dental purposes has resulted in a range of different products. The main advantages of Y-TZP include exceptional mechanical properties, biocompatibility, and resistance to corrosion [1, 2]. One of the greatest disadvantages of the Y-TZP, at least when it comes to dental restorations, is the less than desirable translucency of the material. Translucency is important, as a certain degree of translucency of the dental ceramic is needed to let the natural background color shine throughout the translucent material, so the dental restoration can present a more natural appearance [3].
There are today two main categories of dental prostheses made of Y-TZP: monolithic zirconia (MZ), in which the bulk of the restorations is made of zirconia and external stains are painted in order to better copy the natural colors of teeth, and porcelain-veneered zirconia (PVZ), in which a framework of zirconia is fabricated, upon which veneering porcelain is applied [4]. Prostheses made of MZ are stronger, but present a compromised aesthetic aspect, while PVZ prostheses, with a core of Y-TZP and an outer layer of ceramic (also called as bilayer structure), better resemble natural teeth, although are vulnerable to chipping and delamination [2]. This may predispose PVZ to a higher prevalence of clinical technical complications.
Questions have been raised concerning the effect of cement type on the clinical outcomes, although a recent review failed to find evidence of difference in the complication patterns between adhesive and conventional cementation for zirconia and lithium disilicate tooth-supported crowns [5].
Therefore, the purpose of the present systematic review of the literature was to test the null hypothesis of no difference in the failure rates and the prevalence of technical complications between full-coverage tooth-supported MZ and PVZ fixed dental prosthesis (FDP). The review presented an additional focus on the effect of the type of cement used on the occurrence of complications.
Materials and methods
This study followed the PRISMA Statement guidelines [6]. Registration in PROSPERO was undertaken (registration number CRD42022342097).
Objective
The focused question was elaborated according to the PICO format (participants, interventions, comparisons, outcomes): In patients being rehabilitated with dental prosthetic restorations, is there a difference in the failure rate and in the prevalence of technical complications between monolithic zirconia and porcelain-veneered zirconia prostheses?
Search strategies
An electronic search without time restrictions was undertaken in October 2021, with a complementary updated search in June 2023, in the following databases: PubMed/Medline, Web of Science, and Science Direct. The following terms were used in the search strategies: (tooth OR teeth OR tooth-supported) AND (dental prosthesis OR dental restoration) AND (monolithic zirconia OR porcelain-veneered zirconia OR porcelain fused to zirconia OR pressed on zirconia ceramics).
Due to the initial large number of search entries in Science Direct, the options “research articles” and “review articles” were selected in the filter “Article type.”
A manual search of all related prosthodontic and specialist dental and oral journals was performed. The reference list of the identified studies and the relevant reviews on the subject were also checked for possible additional studies. Gray literature was not searched.
Inclusion and exclusion criteria
Eligibility criteria included clinical human studies, either randomized or not, providing information on the clinical outcomes of full-coverage tooth-supported MZ and/or PVZ FDPs. The minimum of follow-up was set to 6 months. Only publications written in English were considered for inclusion.
Combined tooth-implant-supported FDP cases were excluded, as well as zirconia copings to be used with removable partial dentures. Inlay-retained FDP cases were excluded, as they do not present the same quality of support as a conventional FDP. Cases of zirconia restorations aimed to be cemented on abutment teeth for partial removable dental prosthesis were excluded, as these are subjected to additional forces on the occlusal rest seat and from retentive clasps. Cases of partial crowns and endocrowns were excluded. Additional exclusion criteria were case reports, technical reports, animal studies, in vitro studies, and reviews papers.
Study selection
Two reviewers independently screened the titles and abstracts of the entries (publications) resulted from the searches conducted in the three databases. The full text of a publication was obtained when this appeared to meet the inclusion criteria, or for when there were insufficient data in the title and abstract to make a clear decision, which was carried out independently by two reviewers. Any disagreements between the reviewers were solved by discussion.
The detection of duplicate references from different electronic databases was performed by using the RefWorks Reference Management Software (Ex Libris, Jerusalem, Israel).
Quality assessment
The Quality Assessment Tool for Case Series Studies of the National Institutes of Health [7] was used for the quality assessment of the included studies. The studies were classified as “good” (at least 7 points—the least risk of bias; results are considered to be valid), “fair” (susceptible to some bias deemed not sufficient to invalidate its results), or “poor” quality (significant risk of bias).
Definitions
Yttria-stabilized zirconia is a ceramic material, a white crystalline oxide of zirconium (ZrO2), with its crystal structure stabilized by the addition of yttrium oxide (Y2O3) or yttria [8].
Monolithic zirconia restorations were defined as those with the same chemical and physical properties throughout its thickness [9]. These are dental prostheses with a bulk of zirconia fabricated by computer-aided design and computer-aided manufacturing (CAD/CAM) and painted with external stains [4].
Porcelain-veneered zirconia restorations were defined as those with a zirconia framework enhanced with veneering porcelain [9].
Success was defined as a prothesis that had remained unchanged (no complication or intervention) over the observation period. Survival was defined as the cases in which the prothesis remained in situ, with the occurrence of any complication, while still in function. Prostheses removed or replaced were considered failed prostheses [10].
Biological complications included caries, loss of tooth vitality, periapical infection, mobility, and abutment loss. Technical complications included tooth fracture, loss of retention, framework fracture, and minor and major veneer chipping.
Chipping was defined as loss of ceramic substance, being classified as minor (managed chair-side, such as in-mouth polishing of the fracture) or major (usually sent to the dental lab for reparation or replaced by a new prosthesis) [11, 12].
Catastrophic fracture was defined as a fracture extending through the entire bulk of the restoration, namely, from the external to the inner surface.
“Unacceptable color” and “unacceptable anatomical form” of the restorations were considered neither biological nor technical complications, and therefore not considered for the present review.
Data extraction
From the studies included in the final analysis, the following data were extracted (when available): year of publication, study design and setting, number of patients, patients’ age, type of material (MZ, PVZ), number of failed and placed prosthesis, jaws receiving the prosthesis (maxilla and/or mandible), type of prosthetic rehabilitation, opposing dentition, presence of smokers or bruxers, and follow-up time. Authors of the included studies were contacted for additional information in case of need for additional data.
Analyses
Descriptive statistics were expressed in means, standard deviations (SD), and percentages; Kolmogorov–Smirnov test was used to evaluate normal distribution and Levene’s test to evaluate homoscedasticity. The comparison of continuous variables between two independent groups was done with Student’s t-test or Mann–Whitney, and Pearson’s chi-squared or Fisher’s exact test for the comparison of categorical variables. Comparison of prostheses survival between different groups was done with the log-rank (Mantel-Cox) test. Information for the period of prosthesis failure extracted from the included studies was used to calculate interval survival rate (ISR), and the cumulative survival rate (CSR) was calculated over the maximal period of follow-up reported, in a life-table survival analysis.
The estimated 5-year occurrence proportions of minor and major chipping, as well as of catastrophic fracture were calculated, by assuming constant event rates. The total exposure time of the prostheses of the studies was calculated, and from this the estimated annual rate per 100 prosthesis years and the estimated occurrence after 5 years for each of these 3 outcomes were calculated. The 95% confidence intervals for the survival proportions were calculated using the 95% confidence limits of the event rates. A meta-analysis for each group was conducted using proportions with inverse-variance weights. The value of 0.5 were added to zero frequencies. Groups were then compared using a z-test.
The degree of statistical significance was considered p < 0.05. Data were statistically analyzed using the SPSS version 28 software (SPSS Inc., Chicago, IL, USA).
Results
Literature search
The study selection process is summarized in Fig. 1. The search strategy initially resulted in 2600 papers (461 in PubMed, 557 in Web of Science, and 1582 in Science Direct). A number of 592 articles were cited in more than one research of terms (duplicates). Two reviewers independently screened the abstracts for those articles related to the focus question. Of the resulted 2008 studies, 1894 were excluded for not being related to the topic. Hand searching of selected journals did not yield additional papers. The full-text reports of the remaining 114 articles led to the exclusion of 40 articles because they did not meet the inclusion criteria: shorter follow-up report with an already published longer follow-up report with the same cohort group of patients (n = 16), not enough or no clinical outcome data available (n = 4), no separate information on clinical outcomes between tooth- and implant-supported prostheses (n = 3), endocrowns (n = 3), inlay-retained restorations (n = 3), more than one type of restoration material included in the study, but no separate data on the zirconia restorations (n = 1), restorations made of zirconia-reinforced lithium silicate (n = 1), technical complications not investigated (n = 1), restorations in abutment teeth for partial removable dentures (n = 1), 3D-printed zirconia crowns (n = 1), no follow-up (n = 1), not providing clinical information regarding the number of prosthesis, but the number of prosthetic units (n = 1), lab study (n = 1), single-retainer prostheses (n = 1), partial crowns (n = 1), and study of post-cementation occlusion with no follow-up (n = 1). Thus, 74 publications were included in the review [13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86].

Study screening process
Description of the studies
The 74 included clinical studies reported 6264 tooth-supported zirconia FDPs, supported by 8200 abutment teeth (pontics were not taken into consideration in this amount). The 3549 patients consisted of 1377 (43.1%) men and 1818 (56.9%) women, with no available information on gender for 354 patients.
Table 1 presents the summarized data of the included studies, separately between the two groups. The mean follow-up time of the group of PVZ was higher than for the group of MZ prostheses (p < 0.001; Mann–Whitney test). Women were more often than men rehabilitated with PVZ FDPs, the opposite happening with MZ FDPs (p < 0.001; Pearson’s chi-squared test). Most of the prostheses were single crowns, for both groups (67.7% of PVZ and 94.4% of MZ). Adhesive resin was most commonly used for cementation of the prostheses, and natural teeth were most often observed in the opposing arch occluding to the zirconia prostheses.
In general, PVZ FDPs had a higher occurrence of complications than MZ FDPs. The difference was, in particular, greater when either minor or major chip-offs were considered. Decementation was more commonly seen in prosthesis cemented with adhesive resin than with glass ionomer, with no occurrences with resin-modified glass ionomer.
Table 2 shows the prevalence of minor and major chipping among tooth-supported PVZ and MZ prostheses, for the different types of cementations applied. If the factor time is not considered, the difference of the prevalence of chipping was statistically significant for PVZ prostheses between cementation with glass ionomer and adhesive resin cement (for minor chipping), resin-modified glass ionomer and adhesive resin cement (for both minor and major chipping), and between resin-modified glass ionomer and glass ionomer cement (for both minor and major chipping). For MZ the difference was significant only for minor chipping between resin-modified glass ionomer and adhesive resin cement.
Table 3 shows the prevalence of decementation among tooth-supported PVZ or MZ prostheses, for the different types of cementations applied, between prostheses that had their inner surface air abraded or not. No cases of decementation were observed for prostheses cemented with resin-modified glass ionomer, regardless of whether air abraded or not. Air-abraded PVZ FDPs decemented more often when cemented with conventional glass ionomer cement.
Table 4 shows the prevalence of vitality loss among teeth supporting PVZ or MZ prostheses for the different types of cementations applied. In general, abutment teeth to PVZ prostheses more often lost vitality.
Table 5 shows the prevalence of minor or major chipping among tooth-supported PVZ or MZ prostheses, for when air abrasion prior to cementation was conducted or not. No difference was observed in the prevalence of chipping, either minor or major, when either PVZ or MZ were air abraded or not.
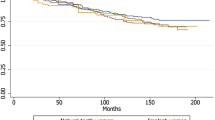
A total of 216 prostheses were considered failure, and the mean time from prosthesis cementation to failure was not statistically significant different between the groups (p = 0.935; Mann–Whitney test). There was no clear concentration of failures in any period of the follow-up, either for PVZ or MZ prostheses (Tables 6 and 7, respectively). The 5-year CSR was lower for PVZ than for MZ prostheses. The survival was statistically significant different between groups (p = 0.007; log-rank test). As the number of cases entering the longest follow-up intervals was very low for both groups, the survival between the groups was compared after the follow-up was limited to 5 years, which still resulted in a statistically significant difference between the groups (p < 0.001; log-rank test). When the data were limited to follow-up up to 5 years, the CSR was 88.7% and 93.3% for PVZ and for MZ prostheses, respectively.
The estimated 5-year occurrence of minor chipping, major chipping, and catastrophic fracture for MZ prostheses were 0.076% (95% CI 0.042, 0.111, SE 0.018), 0.080% (95% CI 0.042, 0.118, SE 0.019), and 0.301% (95% CI 0.244, 0.357, SE 0.029), respectively (Table S1, see Supplementary material). The estimated 5-year occurrence of minor chipping, major chipping, and catastrophic fracture for PVZ prostheses were 10.445% (95% CI 10.253, 10.637, SE 0.098), 1.874% (95% CI 1.803, 1.945, SE 0.036), and 0.383% (95% CI 0.349, 0.417, SE 0.017), respectively (Table S2, see Supplementary material). The difference in the 5-year occurrence of minor and major chipping between MZ and PVZ prostheses was statistically significant (p < 0.001 and p = 0.002, respectively), but nor for the occurrence of catastrophic fracture (p = 0.122).
Quality assessment
All included studies were classified as “good” (Table S3, see Supplementary material). In most cases the main issues in the publications were related to statistical methods not being well described and to the inclusion of non-consecutive patients in the studies.
Discussion
The aim of the present review was to evaluate and compare the clinical outcomes between full-coverage tooth-supported MZ and PVZ FDPs. The results showed that MZ prostheses present higher survival rates than PVZ prostheses (p = 0.007). The reason for this difference can be due to the great difference in the occurrence of some complications that led to removal and/or replacement of the prosthesis. A much higher occurrence of porcelain chipping/fracture, framework fracture, and vitality loss were observed among PVZ than among MZ restorations.
The group of PVZ restorations had a significantly higher mean follow-up time than the group of MZ restorations, namely, a mean of 48.2 and 38.4 months, respectively. This could be one of the reasons contributing to a higher rate of technical complications among PVZ in relation to the MZ ones. It is expected that the longer the mean follow-up time, the higher the risk of presenting more complications. However, it does not explain all the possible reasons for a higher occurrence of technical complications among PVZ prostheses.
PVZ prostheses are more prone to chip-off fractures than MZ prostheses—the latter do not have a veneering ceramic and are expected to have less chipping and fracture complications [87]. The greater prevalence of chipping among PVZ restorations can due to the mismatch in the thermal expansion between the porcelain and the zirconia framework, which leads to the development of residual stresses, which in turn leads to initiation of cracking and veneer chipping. During the cooling process, thermal gradients can develop in crowns and FDPs and create another source of residual stress [88,89,90,91]. In comparison to restorations made of PVZ, monolithic designs have a higher load-bearing capacity [92]. It is also important to point out that resin-based cements may increase the strength of zirconia restorations to fracture, with glass ionomer cements being usually associated with lower fracture strength [93,94,95], which is in accordance with the results of the present review—the rates of minor or major chipping, for either PVZ or MZ, were higher for when the prostheses were cemented with glass ionomer in comparison to adhesive resin cements. Another important issue is the distinction of zirconia crowns with different yttria contents (3 and 5 mol%), as 3 mol% zirconia crowns fracture at almost twice the loads of the 5 mol% zirconia crowns [93]. In this context, the authors of an in vitro study suggested that it would be wise to avoid pre-treatment of 5Y crowns with air abrasion, as this reduced the strength of these crowns, the same not happening with 3Y-crowns [93], although the authors of another in vitro study, although also showing a difference in fracture load between 3 and 5Y crowns, suggested that crowns fabricated from 5Y-Z may be particle abraded if luted with resin cements [94]. Unfortunately, it was not possible to make an analysis of either failure or complications in relation to the different yttria contents of the restorations, as detailed information about the zirconia material used was not always provided. For example, there was information in some studies that either “Lava,” or “BruxZir,” or “Prettau Zirconia” was used, but with no further detail reported. This is an issue since dental zirconia from these three brands are available as either 3Y-TZP or 5Y-TZP.
The higher prevalence of framework fracture among PVZ than in MZ prostheses (0.8% vs. 0.2%, respectively) may be related to the inherent difference in the restoration design between these two types of zirconia restorations, as PVZ restorations present a thinner core of zirconia material than MZ restorations, which in turn influences the thickness of the crown/prosthesis margins [96]. Therefore, it may be expected that PVZ prosthesis would have a higher risk of framework fracture.
Teeth supporting PVZ prostheses presented a higher rate of vitality loss than teeth supporting MZ prostheses (1.5% vs. 0.3%, respectively), which could be related to the fact that veneer restorations are thicker, meaning that more underlying tooth structure needs to be removed [2], raising the risk of overheating the pulp, which is increased as the dentin thickness decreases. The mean tooth structure removal for full-crown restorations is greater for PVZ than for MZ restorations [97]. Dentin is an efficient insulator and will dissipate heat if an adequate amount of thickness remains. As such, trauma to the pulp tissue via heat is dependent on the proximity of the heat source to the pulp [98]. Greater extent of destruction of coronal and root structure was found to be a significant predictor of root canal therapy after single-crown placement [99]. It has been suggested that leaving 2 mm of dentinal thickness is sufficient to provide the pulp with protection from most restorative procedures [100]. Tooth vitality is suggested to contribute positively to the survival of single crowns and fixed dental prostheses [101].
The rate of decementation was higher when prostheses were cemented with zinc phosphate (5.0%)—only cases of PVZ prostheses were cemented with this type of cement. The zinc phosphate cement should not be recommended due to unfavorable properties such as brittleness and water solubility [102]. When it comes to the most commonly used cements, decementation was more commonly seen among prostheses cemented with adhesive resin than with glass ionomer in the MZ group. This goes against the results of an in vitro study, in which it was observed that adhesive resin cements present higher bond strength than glass ionomer cements in the bonding between zirconia and dentin [103]. However, a study observed no difference in the clinical performance for the cementation of zirconia copings between these two types of cement after 48 months [104]. As there is still no clear consensus about the difference in performance between the use of these two cements for zirconia restorations, one can only hypothesize that the possible cause for these findings could be related to the downsides of resin cements. Adhesive bonding has the disadvantage of being technique sensitive, as multiple steps of pretreatment are required and the prepared surface can easily get contaminated [93, 105]. Moreover, zirconia does not bond to resin-based cement as strongly as a silica-based ceramic [93, 106]. These factors could possibly have influenced the results.
No cases of decementation were observed among prostheses cemented with resin-modified glass ionomer, even when the inner surfaces of the prostheses were not air abraded previously to cementation. In general, the rate of decementation for zirconia restorations cemented with either conventional glass ionomer or adhesive resin cements was higher when the inner surface of the prostheses were air abraded before cementation. However, it seems that there is still some controversy whether air abrasion alters the shear bond strength of zirconia ceramic restorations [107]. Nevertheless, sandblast damage introduced into the ceramic undersurfaces causes further reductions in strength levels, with surface abrasion treatments possibly being an important degrading factor in long-term performance of all-ceramic crowns [108].
The problem with decementation when adhesive cements are used may be due to the already aforementioned reasons, although in vitro studies showed that resin-modified glass-ionomer cement presented the same level of retentive quality or the same mean removal stress as resin luting agents [109,110,111]. Moreover, similar clinical outcomes for the cementation of zirconia restorations between these cements were observed in a clinical study [112].. However, there is no clear consensus on the subject, as other in vitro studies showed that resin-modified glass ionomer cements present lower mean bond strengths between zirconia and dentin than resin-based luting cements [103, 113]. The results were not favorable for the conventional glass ionomer cement though. Compared to conventional glass ionomer, resin-modified glass ionomer cements have been showing better clinical performance [114].
The present review is not without limitations. First of all, most of the included studies were retrospective reports, which inherently results in flaws, manifested by the gaps in information and incomplete records. The number of technical complications observed is very probably underestimated, since not all studies reported data on all types of complications. Second, several professionals were involved in the treatment of these patients, which could have had some influence on the failure and complications rate. Third, much of the research in the field is limited by small cohort sizes and short follow-up periods, which could have led to an underestimation of the actual clinical outcomes.
Conclusions
Tooth-supported PVZ FDPs present a lower survival than MZ FDPs (p = 0.007). The difference in the 5-year occurrence of minor (p < 0.001) and major chipping (p = 0.002) between MZ and PVZ prostheses was statistically significant, the same not happening with catastrophic fracture (p = 0.122). Loss of vitality happens more often with abutment teeth to PVZ prostheses. Decementation was not observed with resin-modified glass ionomer cement. Air abrasion does not seem to clinically decrease the risk of decementation.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article [and/or] its supplementary materials.
References
Denry I, Kelly JR (2008) State of the art of zirconia for dental applications. Dental Mater: official publication of the Academy of Dental Materials 24:299–307. https://doi.org/10.1016/j.dental.2007.05.007
Zhang Y, Lawn BR (2018) Novel zirconia materials in dentistry. J Dent Res 97:140–147. https://doi.org/10.1177/0022034517737483
Heffernan MJ, Aquilino SA, Diaz-Arnold AM, Haselton DR, Stanford CM, Vargas MA (2002) Relative translucency of six all-ceramic systems. Part I: core materials. J Prosthet Dent 88:4–9
Tavangar MS, Mousavipour E, Ansarifard E (2021) The effect of bleaching on the optical and physical properties of externally stained monolithic zirconia. Clin Exp Dental Res 7:861–867. https://doi.org/10.1002/cre2.433
Maroulakos G, Thompson GA, Kontogiorgos ED (2019) Effect of cement type on the clinical performance and complications of zirconia and lithium disilicate tooth-supported crowns: a systematic review. Report of the Committee on Research in Fixed Prosthodontics of the American Academy of Fixed Prosthodontics. J Prosthet Dent 121:754–765. https://doi.org/10.1016/j.prosdent.2018.10.011
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, McKenzie JE (2021) PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ (Clinical research ed) 372:n160. https://doi.org/10.1136/bmj.n160
NIH (2014) Quality assessment tool for case series studies. National Institutes of Health (NIH). https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed 25 Oct 2021
Piconi C, Maccauro G (1999) Zirconia as a ceramic biomaterial. Biomaterials 20:1–25. https://doi.org/10.1016/s0142-9612(98)00010-6
(2017) The glossary of prosthodontic terms: ninth edition. The Journal of prosthetic dentistry 117:e1-e105 https://doi.org/10.1016/j.prosdent.2016.12.001
Hawthan MA, Chrcanovic BR, Larsson C (2023) Long-term retrospective clinical study of tooth-supported fixed partial dentures: a multifactorial analysis. J Prosthodont Res 67:238–245. https://doi.org/10.2186/jpr.JPR_D_21_00222
Hawthan M, Chrcanovic BR, Larsson C (2022) Retrospective study comparing clinical outcomes of fixed dental prostheses in matched groups of bruxer and nonbruxer patients. Int J Dent 2022:6818170. https://doi.org/10.1155/2022/6818170
Hawthan M, Chrcanovic BR, Larsson C (2022) Retrospective clinical study of tooth-supported single crowns: a multifactor analysis. Euro J Oral Sci 130:e12871. https://doi.org/10.1111/eos.12871
Barile G, Capodiferro S, Muci G, Carnevale A, Albanese G, Rapone B, Corsalini M (2023) Clinical outcomes of monolithic zirconia crowns on posterior natural abutments performed by final year dental medicine students: a prospective study with a 5-year follow-up. Int J Environ Res Public Health 20:2943. https://doi.org/10.3390/ijerph20042943
Beuer F, Edelhoff D, Gernet W, Sorensen JA (2009) Three-year clinical prospective evaluation of zirconia-based posterior fixed dental prostheses (FDPs). Clin Oral Invest 13:445–451. https://doi.org/10.1007/s00784-009-0249-5
Beuer F, Stimmelmayr M, Gernet W, Edelhoff D, Güth JF, Naumann M (2010) Prospective study of zirconia-based restorations: 3-year clinical results. Quintessence Int (Berlin, Germany : 1985) 41:631–637
Burke FJ, Crisp RJ, Cowan AJ, Lamb J, Thompson O, Tulloch N (2013) Five-year clinical evaluation of zirconia-based bridges in patients in UK general dental practices. J Dent 41:992–999. https://doi.org/10.1016/j.jdent.2013.08.007
Cehreli MC, Kökat AM, Akça K (2009) CAD/CAM Zirconia vs. slip-cast glass-infiltrated alumina/zirconia all-ceramic crowns: 2-year results of a randomized controlled clinical trial. J Appl Oral Sci : revista FOB 17:49–55. https://doi.org/10.1590/s1678-77572009000100010
Chaar MS, Passia N, Kern M (2015) Ten-year clinical outcome of three-unit posterior FDPs made from a glass-infiltrated zirconia reinforced alumina ceramic (in-ceram zirconia). J Dent 43:512–517. https://doi.org/10.1016/j.jdent.2015.02.016
Christensen RP, Ploeger BJ (2010) A clinical comparison of zirconia, metal and alumina fixed-prosthesis frameworks veneered with layered or pressed ceramic: a three-year report. J Am Dental Assoc 141:1317–1329. https://doi.org/10.14219/jada.archive.2010.0076
Dhima M, Paulusova V, Carr AB, Rieck KL, Lohse C, Salinas TJ (2014) Practice-based clinical evaluation of ceramic single crowns after at least five years. J Prosthet Dent 111:124–130. https://doi.org/10.1016/j.prosdent.2013.06.015
Dogan S, Raigrodski AJ, Zhang H, Mancl LA (2017) Prospective cohort clinical study assessing the 5-year survival and success of anterior maxillary zirconia-based crowns with customized zirconia copings. J Prosthet Dent 117:226–232. https://doi.org/10.1016/j.prosdent.2016.07.019
Ferrari M, Sorrentino R, Cagidiaco C, Goracci C, Vichi A, Gherlone E, Zarone F (2015) Short-term clinical performance of zirconia single crowns with different framework designs: 3-year clinical trial. Am J Dent 28:235–240
Forrer FA, Schnider N, Brägger U, Yilmaz B, Hicklin SP (2020) Clinical performance and patient satisfaction obtained with tooth-supported ceramic crowns and fixed partial dentures. J Prosthet Dent 124:446–453. https://doi.org/10.1016/J.PROSDENT.2019.08.012
Gardell E, Larsson C, von Steyern PV (2021) Translucent zirconium dioxide and lithium disilicate: a 3-year follow-up of a prospective, practice-based randomized controlled trial on posterior monolithic crowns. Int J Prosthodont 34:163–172. https://doi.org/10.11607/ijp.6795
Gherlone E, Mandelli F, Capparè P, Pantaleo G, Traini T, Ferrini F (2014) A 3 years retrospective study of survival for zirconia-based single crowns fabricated from intraoral digital impressions. J Dent 42:1151–1155. https://doi.org/10.1016/j.jdent.2014.06.002
Grohmann P, Bindl A, Hämmerle C, Mehl A, Sailer I (2015) Three-unit posterior zirconia-ceramic fixed dental prostheses (FDPs) veneered with layered and milled (CAD-on) veneering ceramics: 1-year follow-up of a randomized controlled clinical trial. Quintessence Int (Berlin, Germany : 1985) 46:871–80. https://doi.org/10.3290/j.qi.a34701
Groten M, Huttig F (2010) The performance of zirconium dioxide crowns: a clinical follow-up. Int J Prosthodont 23:429–431
Gseibat M, Sevilla P, Lopez-Suarez C, Rodriguez V, Pelaez J and Suarez MJ (2022) Prospective clinical evaluation of posterior third-generation monolithic zirconia crowns fabricated with complete digital workflow: two-year follow-up. Materials (Basel, Switzerland) 15 https://doi.org/10.3390/ma15020672
Habibi Y, Dawid M-T, Waldecker M, Rammelsberg P, Boemicke W (2020) Three-year clinical performance of monolithic and partially veneered zirconia ceramic fixed partial dentures. J Esthet Restor Dent 32:395–402. https://doi.org/10.1111/jerd.12568
Hammoudi W, Trulsson M, Svensson P, Smedberg JI (2022) Long-term results of a randomized clinical trial of 2 types of ceramic crowns in participants with extensive tooth wear. J Prosthet Dent 127:248–257. https://doi.org/10.1016/j.prosdent.2020.08.041
Hansen TL, Schriwer C, Øilo M, Gjengedal H (2018) Monolithic zirconia crowns in the aesthetic zone in heavy grinders with severe tooth wear - an observational case-series. J Dent 72:14–20. https://doi.org/10.1016/j.jdent.2018.01.013
Heller H, Sreter D, Arieli A, Beitlitum I, Pilo R and Levartovsky S (2022) Survival and success rates of monolithic zirconia restorations supported by teeth and implants in bruxer versus non-bruxer patients: a retrospective study. Materials (Basel, Switzerland) 15 https://doi.org/10.3390/ma15030833
Håff A, Löf H, Gunne J, Sjögren G (2015) A retrospective evaluation of zirconia-fixed partial dentures in general practices: an up to 13-year study. Dent Mater 31:162–170. https://doi.org/10.1016/j.dental.2014.11.009
Ioannidis A, Bindl A (2016) Clinical prospective evaluation of zirconia-based three-unit posterior fixed dental prostheses: up-to ten-year results. J Dent 47:80–85. https://doi.org/10.1016/j.jdent.2016.01.014
Kasem AT, Ellayeh M, Özcan M, Sakrana AA (2023) Three-year clinical evaluation of zirconia and zirconia-reinforced lithium silicate crowns with minimally invasive vertical preparation technique. Clin Oral Invest 27:1577–1588. https://doi.org/10.1007/s00784-022-04779-1
Kitaoka A, Akatsuka R, Kato H, Yoda N, Sasaki K (2018) Clinical evaluation of monolithic zirconia crowns: a short-term pilot report. Int J Prosthodont 31:124–126. https://doi.org/10.11607/ijp.5444
Koenig V, Vanheusden AJ, Le Goff SO, Mainjot AK (2013) Clinical risk factors related to failures with zirconia-based restorations: an up to 9-year retrospective study. J Dent 41:1164–1174. https://doi.org/10.1016/j.jdent.2013.10.009
Koenig V, Wulfman C, Bekaert S, Dupont N, Le Goff S, Eldafrawy M, Vanheusden A, Mainjot A (2019) Clinical behavior of second-generation zirconia monolithic posterior restorations: two-year results of a prospective study with Ex vivo analyses including patients with clinical signs of bruxism. J Dent 91:103229. https://doi.org/10.1016/j.jdent.2019.103229
Kollar A, Huber S, Mericske E, Mericske-Stern R (2008) Zirconia for teeth and implants: a case series. Int J Periodontics Restor Dent 28:479–487
Konstantinidis I, Trikka D, Gasparatos S and Mitsias ME (2018) Clinical outcomes of monolithic zirconia crowns with CAD/CAM technology. A 1-year follow-up prospective clinical study of 65 patients. International journal of environmental research and public health 15 https://doi.org/10.3390/ijerph15112523
Konstantinidis IK, Jacoby S, Rädel M, Böning K (2015) Prospective evaluation of zirconia based tooth- and implant-supported fixed dental prostheses: 3-year results. J Dent 43:87–93. https://doi.org/10.1016/j.jdent.2014.10.011
Le M, Dirawi W, Papia E and Larsson C (2022) Clinical outcome of three different types of posterior all-ceramic crowns. A 3-year follow-up of a multicenter, randomized, controlled clinical trial. Int J Prosthodontics https://doi.org/10.11607/ijp.8016
Lops D, Mosca D, Casentini P, Ghisolfi M, Romeo E (2012) Prognosis of zirconia ceramic fixed partial dentures: a 7-year prospective study. Int J Prosthodont 25:21–23
Mikeli A, Walter MH, Rau SA, Raedel M, Raedel M (2022) Three-year clinical performance of posterior monolithic zirconia single crowns. J Prosthet Dent 128:1252–1257. https://doi.org/10.1016/j.prosdent.2021.03.004
Miura S, Yamauchi S, Kasahara S, Katsuda Y, Fujisawa M, Egusa H (2021) Clinical evaluation of monolithic zirconia crowns: a failure analysis of clinically obtained cases from a 3.5-year study. J Prosthodont Res 65:148–154. https://doi.org/10.2186/jpr.JPOR_2019_643
Molin MK, Karlsson SL (2008) Five-year clinical prospective evaluation of zirconia-based Denzir 3-unit FPDs. Int J Prosthodont 21:223–227
Monaco C, Caldari M, Scotti R (2013) Clinical evaluation of 1,132 zirconia-based single crowns: a retrospective cohort study from the AIOP clinical research group. Int J Prosthodont 26:435–442. https://doi.org/10.11607/ijp.3099
Monaco C, Llukacej A, Baldissara P, Arena A, Scotti R (2017) Zirconia-based versus metal-based single crowns veneered with overpressing ceramic for restoration of posterior endodontically treated teeth: 5-year results of a randomized controlled clinical study. J Dent 65:56–63. https://doi.org/10.1016/J.JDENT.2017.07.004
Naenni N, Bindl A, Sax C, Hämmerle C, Sailer I (2015) A randomized controlled clinical trial of 3-unit posterior zirconia-ceramic fixed dental prostheses (FDP) with layered or pressed veneering ceramics: 3-year results. J Dent 43:1365–1370. https://doi.org/10.1016/j.jdent.2015.07.013
Ohlmann B, Eiffler C, Rammelsberg P (2012) Clinical performance of all-ceramic cantilever fixed dental prostheses: results of a 2-year randomized pilot study. Quintessence Int (Berlin, Germany : 1985) 43:643–8
Ortorp A, Kihl ML, Carlsson GE (2012) A 5-year retrospective study of survival of zirconia single crowns fitted in a private clinical setting. J Dent 40:527–530. https://doi.org/10.1016/j.jdent.2012.02.011
Pathan MS, Kheur MG, Patankar AH, Kheur SM (2019) Assessment of antagonist enamel wear and clinical performance of full-contour monolithic zirconia crowns: one-year results of a prospective study. J Prosthodontics : official journal of the American College of Prosthodontists 28:e411–e416. https://doi.org/10.1111/jopr.12960
Peláez J, Cogolludo PG, Serrano B, Lozano JFL, Suárez MJ (2012) A prospective evaluation of zirconia posterior fixed dental prostheses: three-year clinical results. J Prosthet Dent 107:373–379. https://doi.org/10.1016/S0022-3913(12)60094-8
Pihlaja J, Näpänkangas R, Raustia A (2014) Early complications and short-term failures of zirconia single crowns and partial fixed dental prostheses. J Prosthet Dent 112:778–783. https://doi.org/10.1016/j.prosdent.2014.03.008
Pihlaja J, Näpänkangas R, Raustia A (2016) Outcome of zirconia partial fixed dental prostheses made by predoctoral dental students: a clinical retrospective study after 3 to 7 years of clinical service. J Prosthet Dent 116:40–46. https://doi.org/10.1016/j.prosdent.2015.10.026
Poggio CE, Dosoli R, Ercoli C (2012) A retrospective analysis of 102 zirconia single crowns with knife-edge margins. J Prosthet Dent 107:316–321. https://doi.org/10.1016/s0022-3913(12)60083-3
Pontevedra P, Lopez-Suarez C, Rodriguez V, Pelaez J, Suarez MJ (2022) Randomized clinical trial comparing monolithic and veneered zirconia three-unit posterior fixed partial dentures in a complete digital flow: three-year follow-up. Clin Oral Invest 26:4327–4335. https://doi.org/10.1007/s00784-022-04396-y
Raigrodski AJ, Yu A, Chiche GJ, Hochstedler JL, Mancl LA, Mohamed SE (2012) Clinical efficacy of veneered zirconium dioxide-based posterior partial fixed dental prostheses: five-year results. J Prosthet Dent 108:214–222. https://doi.org/10.1016/S0022-3913(12)60165-6
Rinke S, Gersdorff N, Lange K, Roediger M (2013) Prospective evaluation of zirconia posterior fixed partial dentures: 7-year clinical results. Int J Prosthodont 26:164–171. https://doi.org/10.11607/ijp.3229
Rinke S, Schäfer S, Lange K, Gersdorff N, Roediger M (2013) Practice-based clinical evaluation of metal-ceramic and zirconia molar crowns: 3-year results. J Oral Rehabil 40:228–237. https://doi.org/10.1111/joor.12018
Sagirkaya E, Arikan S, Sadik B, Kara C, Karasoy D, Cehreli M (2012) A randomized, prospective, open-ended clinical trial of zirconia fixed partial dentures on teeth and implants: interim results. Int J Prosthodont 25:221–231
Sailer I, Balmer M, Hüsler J, Hämmerle CHF, Känel S, Thoma DS (2018) 10-year randomized trial (RCT) of zirconia-ceramic and metal-ceramic fixed dental prostheses. J Dent 76:32–39. https://doi.org/10.1016/j.jdent.2018.05.015
Salido MP, Martinez-Rus F, del Rio F, Pradies G, Ozcan M, Suarez MJ (2012) Prospective clinical study of zirconia-based posterior four-unit fixed dental prostheses: four-year follow-up. Int J Prosthodont 25:403–409
Sax C, Hämmerle CH, Sailer I (2011) 10-year clinical outcomes of fixed dental prostheses with zirconia frameworks. Int J Comput Dent 14:183–202
Schmitt J, Goellner M, Lohbauer U, Wichmann M, Reich S (2012) Zirconia posterior fixed partial dentures: 5-year clinical results of a prospective clinical trial. Int J Prosthodont 25:585–589
Schmitt J, Wichmann M, Holst S, Reich S (2010) Restoring severely compromised anterior teeth with zirconia crowns and feather-edged margin preparations: a 3-year follow-up of a prospective clinical trial. Int J Prosthodont 23:107–109
Schmitter M, Mussotter K, Rammelsberg P, Gabbert O, Ohlmann B (2012) Clinical performance of long-span zirconia frameworks for fixed dental prostheses: 5-year results. J Oral Rehabil 39:552–557. https://doi.org/10.1111/j.1365-2842.2012.02311.x
Seidel A, Belli R, Breidebach N, Wichmann M, Matta RE (2020) The occlusal wear of ceramic fixed dental prostheses: 3-year results in a randomized controlled clinical trial with split-mouth design. J Dent 103:103500. https://doi.org/10.1016/j.jdent.2020.103500
Serra-Pastor B, Loi I, Fons-Font A, Solá-Ruíz MF, Agustín-Panadero R (2019) Periodontal and prosthetic outcomes on teeth prepared with biologically oriented preparation technique: a 4-year follow-up prospective clinical study. J Prosthodont Res 63:415–420. https://doi.org/10.1016/j.jpor.2019.03.006
Seydler B, Schmitter M (2015) Clinical performance of two different CAD/CAM-fabricated ceramic crowns: 2-year results. J Prosthet Dent 114:212–216. https://doi.org/10.1016/j.prosdent.2015.02.016
Shi J-Y, Li X, Ni J, Zhu Z-Y (2016) Clinical evaluation and patient satisfaction of single zirconia-based and high-noble alloy porcelain-fused-to-metal crowns in the esthetic area: a retrospective cohort study. J Prosthodontics : official journal of the American College of Prosthodontists 25:526–530. https://doi.org/10.1111/jopr.12344
Solá-Ruiz MF, Baixauli-López M, Roig-Vanaclocha A, Amengual-Lorenzo J, Agustín-Panadero R (2021) Prospective study of monolithic zirconia crowns: clinical behavior and survival rate at a 5-year follow-up. J Prosthodont Res 65:284–290. https://doi.org/10.2186/jpr.JPR_D_20_00034
Sola-Ruiz MF, Leon-Martine R, Labaig-Rueda C, Selva-Otalaorrouchi E, Agustin-Panadero R (2022) Clinical outcomes of veneered zirconia anterior partial fixed dental prostheses: A 12-year prospective clinical trial. J Prosthet Dent 127:846–851. https://doi.org/10.1016/j.prosdent.2020.09.046
Tanaka S, Takaba M, Ishiura Y, Kamimura E, Baba K (2015) A 3-year follow-up of ceria-stabilized zirconia/alumina nanocomposite (Ce-TZP/A) frameworks for fixed dental prostheses. J Prosthodont Res 59:55–61. https://doi.org/10.1016/j.jpor.2014.11.006
Tang Z, Zhao X, Wang H (2021) Quantitative analysis on the wear of monolithic zirconia crowns on antagonist teeth. BMC Oral Health 21:94. https://doi.org/10.1186/s12903-021-01452-z
Tang Z, Zhao X, Wang H, Liu B (2019) Clinical evaluation of monolithic zirconia crowns for posterior teeth restorations. Medicine 98:e17385. https://doi.org/10.1097/md.0000000000017385
Tanner J, Niemi H, Ojala E, Tolvanen M, Närhi T, Hjerppe J (2018) Zirconia single crowns and multiple-unit FDPs—an up to 8 -year retrospective clinical study. J Dent 79:96–101. https://doi.org/10.1016/j.jdent.2018.10.012
Tartaglia GM, Sidoti E, Sforza C (2015) Seven-year prospective clinical study on zirconia-based single crowns and fixed dental prostheses. Clin Oral Invest 19:1137–1145. https://doi.org/10.1007/s00784-014-1330-2
Teichmann M, Wienert AL, Rückbeil M, Weber V, Wolfart S, Edelhoff D (2018) Ten-year survival and chipping rates and clinical quality grading of zirconia-based fixed dental prostheses. Clin Oral Invest 22:2905–2915. https://doi.org/10.1007/s00784-018-2378-1
Tinschert J, Schulze KA, Natt G, Latzke P, Heussen N, Spiekermann H (2008) Clinical behavior of zirconia-based fixed partial dentures made of DC-Zirkon: 3-year results. Int J Prosthodont 21:217–222
Tsumita M, Kokubo Y, Ohkubo C, Sakurai S, Fukushima S (2010) Clinical evaluation of posterior all-ceramic FPDs (Cercon): a prospective clinical pilot study. J Prosthodont Res 54:102–105. https://doi.org/10.1016/j.jpor.2010.01.001
Valenti M, Valenti A, Schmitz JH, Cortellini D, Canale A (2023) Survival analysis up to 7 years of 621 zirconia monolithic single crowns with feather-edge margins fabricated with a cast-free workflow starting from intraoral scans: a multicentric retrospective study. J Prosthet Dent 129:76–82. https://doi.org/10.1016/j.prosdent.2022.05.029
Vigolo P, Mutinelli S (2012) Evaluation of zirconium-oxide-based ceramic single-unit posterior fixed dental prostheses (FDPs) generated with two CAD/CAM systems compared to porcelain-fused-to-metal single-unit posterior FDPs: a 5-year clinical prospective study. J Prosthodontics : official journal of the American College of Prosthodontists 21:265–269. https://doi.org/10.1111/j.1532-849X.2011.00825.x
Vult von Steyern P, Carlson P, Nilner K (2005) All-ceramic fixed partial dentures designed according to the DC-Zirkon technique. A 2-year clinical study. J Oral Rehabil 32:180–187. https://doi.org/10.1111/j.1365-2842.2004.01437.x
Waldecker M, Behnisch R, Rammelsberg P, Bömicke W (2022) Five-year clinical performance of monolithic and partially veneered zirconia single crowns-a prospective observational study. J Prosthodont Res 66:339–345. https://doi.org/10.2186/jpr.JPR_D_21_00024
Worni A, Katsoulis J, Kolgeci L, Worni M, Mericske-Stern R (2017) Monolithic zirconia reconstructions supported by teeth and implants: 1- to 3-year results of a case series. Quintessence Int (Berlin, Germany : 1985) 48:459–467. https://doi.org/10.3290/j.qi.a38138
Lameira DP, Buarque e Silva WA, Andrade e Silva F, De Souza GM (2015) Fracture strength of aged monolithic and bilayer zirconia-based crowns. BioMed Res Int 2015:418641. https://doi.org/10.1155/2015/418641
Aboushelib MN, Kleverlaan CJ, Feilzer AJ (2006) Microtensile bond strength of different components of core veneered all-ceramic restorations. Part II: zirconia veneering ceramics. Dental Mater : official publication of the Academy of Dental Materials 22:857–863. https://doi.org/10.1016/j.dental.2005.11.014
Fischer J, Stawarzcyk B, Trottmann A, Hämmerle CH (2009) Impact of thermal misfit on shear strength of veneering ceramic/zirconia composites. Dental Mater : official publication of the Academy of Dental Materials 25:419–423. https://doi.org/10.1016/j.dental.2008.09.003
Guazzato M, Proos K, Quach L, Swain MV (2004) Strength, reliability and mode of fracture of bilayered porcelain/zirconia (Y-TZP) dental ceramics. Biomaterials 25:5045–5052. https://doi.org/10.1016/j.biomaterials.2004.02.036
Swain MV (2009) Unstable cracking (chipping) of veneering porcelain on all-ceramic dental crowns and fixed partial dentures. Acta Biomater 5:1668–1677. https://doi.org/10.1016/j.actbio.2008.12.016
Beuer F, Stimmelmayr M, Gueth JF, Edelhoff D, Naumann M (2012) In vitro performance of full-contour zirconia single crowns. Dental Mater : official publication of the Academy of Dental Materials 28:449–456. https://doi.org/10.1016/j.dental.2011.11.024
Indergård JA, Skjold A, Schriwer C, Øilo M (2021) Effect of cementation techniques on fracture load of monolithic zirconia crowns. Biomater Inv Dent 8:160–169. https://doi.org/10.1080/26415275.2021.1990764
Lawson NC, Jurado CA, Huang CT, Morris GP, Burgess JO, Liu PR, Kinderknecht KE, Lin CP, Givan DA (2019) Effect of surface treatment and cement on fracture load of traditional zirconia (3Y), translucent zirconia (5Y), and lithium disilicate crowns. J Prosthodontics : official journal of the American College of Prosthodontists 28:659–665. https://doi.org/10.1111/jopr.13088
Tsuyuki Y, Sato T, Nomoto S, Yotsuya M, Koshihara T, Takemoto S, Yoshinari M (2018) Effect of occlusal groove on abutment, crown thickness, and cement-type on fracture load of monolithic zirconia crowns. Dent Mater J 37:843–850. https://doi.org/10.4012/dmj.2017-350
Skjold A, Schriwer C, Gjerdet NR, Øilo M (2022) Fractographic analysis of 35 clinically fractured bi-layered and monolithic zirconia crowns. J Dent 125:104271. https://doi.org/10.1016/j.jdent.2022.104271
Schwindling FS, Waldecker M, Rammelsberg P, Rues S, Bömicke W (2019) Tooth substance removal for ceramic single crown materials-an in vitro comparison. Clin Oral Invest 23:3359–3366. https://doi.org/10.1007/s00784-018-2753-y
Nyborg H, Brännström M (1968) Pulp reaction to heat. J Prosthet Dent 19:605–612. https://doi.org/10.1016/0022-3913(68)90262-x
Kirakozova A, Caplan DJ (2006) Predictors of root canal treatment in teeth with full coverage restorations. J Endodontics 32:727–730. https://doi.org/10.1016/j.joen.2005.11.001
Ettinger RL, Qian F (2004) Postprocedural problems in an overdenture population: a longitudinal study. J Endodontics 30:310–314. https://doi.org/10.1097/00004770-200405000-00003
Hawthan M, Larsson C, Chrcanovic BR (2023) Survival of fixed prosthetic restorations on vital and nonvital teeth: a systematic review. J Prosthodontics : official journal of the American College of Prosthodontists. https://doi.org/10.1111/jopr.13735
Dupuis V, Laviole O, Potin-Gautier M, Castetbon A, Moya F (1992) Solubility and disintegration of zinc phosphate cement. Biomaterials 13:467–470. https://doi.org/10.1016/0142-9612(92)90168-n
Vivek VJ, Venugopal P, Divakar N, Bharath S, Sarin K, Mohammed N (2022) Comparison of zirconia to dentin bonding using resin-based luting cements and resin-modified glass-ionomer cement: in vitro. J Pharm Bioallied Sci 14:S460-s463. https://doi.org/10.4103/jpbs.jpbs_779_21
Torres C, Ávila D, Gonçalves LL, Meirelles L, Mailart MC, Di Nicoló R, Borges AB (2021) Glass ionomer versus self-adhesive cement and the clinical performance of zirconia coping/press-on porcelain crowns. Oper Dent 46:362–373. https://doi.org/10.2341/20-229-c
Mutlu Ö (2013) Luting cements for dental applications. In: Vallittu P (ed) Non-metallic biomaterials for tooth repair and replacement. Woodhead Publishing, Cambridge, pp 375–394
Dérand P, Dérand T (2000) Bond strength of luting cements to zirconium oxide ceramics. Int J Prosthodont 13:131–135
Kern M (2015) Bonding to oxide ceramics—laboratory testing versus clinical outcome. Dental Mater : official publication of the Academy of Dental Materials 31:8–14. https://doi.org/10.1016/j.dental.2014.06.007
Zhang Y, Lawn BR, Rekow ED, Thompson VP (2004) Effect of sandblasting on the long-term performance of dental ceramics. J Biomed Mater Res B Appl Biomater 71:381–386. https://doi.org/10.1002/jbm.b.30097
Capa N, Ozkurt Z, Canpolat C, Kazazoglu E (2009) Shear bond strength of luting agents to fixed prosthodontic restorative core materials. Aust Dent J 54:334–340. https://doi.org/10.1111/j.1834-7819.2009.01159.x
Ernst CP, Cohnen U, Stender E, Willershausen B (2005) In vitro retentive strength of zirconium oxide ceramic crowns using different luting agents. J Prosthet Dent 93:551–558. https://doi.org/10.1016/j.prosdent.2005.04.011
Palacios RP, Johnson GH, Phillips KM, Raigrodski AJ (2006) Retention of zirconium oxide ceramic crowns with three types of cement. J Prosthet Dent 96:104–114. https://doi.org/10.1016/j.prosdent.2006.06.001
Pyo SW, Park K, Daher R, Kwon HB, Han JS, Lee JH (2023) Comparison of the clinical outcomes of resin-modified glass ionomer and self-adhesive resin cementations for full-coverage zirconia restorations. J Dent 135:104558. https://doi.org/10.1016/j.jdent.2023.104558
Sabatini C, Patel M, D’Silva E (2013) In vitro shear bond strength of three self-adhesive resin cements and a resin-modified glass ionomer cement to various prosthodontic substrates. Oper Dent 38:186–196. https://doi.org/10.2341/11-317-l
Hübel S, Mejàre I (2003) Conventional versus resin-modified glass-ionomer cement for class II restorations in primary molars. A 3-year clinical study. Int J Pediatr Dent 13:2–8. https://doi.org/10.1046/j.1365-263x.2003.00416.x
Acknowledgements
We would like to thank the following authors who provided us additional information about their studies (in alphabetical order of the surname): Wolfgang Bömicke, Shifra Levartovsky, Michael Moscovitch, Chiarella Sforza, and Moritz Waldecker.
Funding
Open access funding provided by Malmö University.
Author information
Authors and Affiliations
Contributions
Shahed Shihabi: definition of the methodology, literature search, drafting of the manuscript, and critical revision of the article. Bruno Ramos Chrcanovic: conception of the study, definition of the methodology, literature search, statistical analysis, drafting of the manuscript, critical revision of the article, visualization, and supervision. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
Not applicable. This is a systematic review of the literature.
Consent to participate
Not applicable. This is a systematic review of the literature.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shihabi, S., Chrcanovic, B.R. Clinical outcomes of tooth-supported monolithic zirconia vs. porcelain-veneered zirconia fixed dental prosthesis, with an additional focus on the cement type: a systematic review and meta-analysis. Clin Oral Invest 27, 5755–5769 (2023). https://doi.org/10.1007/s00784-023-05219-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-023-05219-4