
Abstract
Patients with rheumatoid arthritis (RA) have an increased risk of developing cardiovascular disease (CVD). Identification of at-risk patients is paramount to initiate preventive care and tailor treatments accordingly. Despite international guidelines recommending all patients with RA undergo CVD risk assessment, rates remain suboptimal. The objectives of this review were to map the strategies used to conduct CVD risk assessments in patients with RA in routine care, determine who delivers CVD risk assessments, and identify what composite measures are used. The Joanna Briggs Institute methodological guidelines were used. A literature search was conducted in electronic and grey literature databases, trial registries, medical clearing houses, and professional rheumatology organisations. Findings were synthesised narratively. A total of 12 studies were included. Strategies reported in this review used various system-based interventions to support delivery of CVD risk assessments in patients with RA, operationalised in different ways, adopting two approaches: (a) multidisciplinary collaboration, and (b) education. Various composite measures were cited in use, with and without adjustment for RA. Results from this review demonstrate that although several strategies to support CVD risk assessments in patients with RA are cited in the literature, there is limited evidence to suggest a standardised model has been applied to routine care. Furthermore, extensive evidence to map how health care professionals conduct CVD risk assessments in practice is lacking. Research needs to be undertaken to establish the extent to which healthcare professionals are CVD risk assessing their patients with RA in routine care.
Key Points • A limited number of system-based interventions are in use to support the delivery of CVD risk assessments in patients with RA. • Multidisciplinary team collaboration, and education are used to operationalise interventions to support Health Care Professionals in conducting CVD risk assessments in practice. • The extent to which Health Care Professionals are CVD risk assessing their patients with RA needs to be established. |
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Rheumatoid Arthritis (RA) is a chronic, destructive, musculoskeletal disorder of unknown aetiology, characterised by symmetric polyarthritis and erosive synovitis [1]. RA age-standardised prevalence rates are rising globally [2], with current rates ranging from 0.24 to 1% of the general population [3]. Despite significant advancements in treatments over the past 20 years, RA still causes substantial mortality due to comorbidities such as cardiovascular disease (CVD) [4]. Studies have demonstrated 45 to 60% increased mortality in RA patient groups due to CVD compared to the general adult population [5,6,7]. This can be attributed to a high prevalence of traditional risk factors which, when combined with chronic inflammation, result in accelerated atherosclerosis [8, 9]. CVD as an umbrella term represents four separate disease entities: ischemic heart disease, cerebrovascular disease, peripheral arterial disease, and aortic atherosclerosis [10]. Ischemic heart disease and cerebrovascular disease are the top two causes of death globally, with eight out of 10 events being preventable [11].
Due to the increased global prevalence of RA and associated costs to healthcare, particularly in the presence of concomitant CVD, preventative care is vital [12, 13]. In patients with RA, CVD risk screening can be undertaken by any healthcare professional (HCP) involved in patient care including physicians, nurses, and allied health professionals working in a variety of disciplines including but not limited to rheumatology, cardiology, vascular medicine, neurology, and general medicine. CVD risk screening is undertaken to detect the presence or absence of traditional CVD risk factors such as smoking, hyperlipidaemia, or hypertension. CVD risk assessment, however, is the next step in identifying those patients who are deemed ‘at-risk’ of developing a cardiovascular event and stratifies that risk into low, medium, high, or very high, so interventions can be tailored accordingly [14]. CVD risk assessment, therefore, involves the application of an instrument as a composite measure of risk factor variables, and the recording of a score to assess risk beyond the initial screening for traditional risk factors [15]. European guidelines recommend that in patients with RA, a CVD risk assessment using a composite measure of risk factor variables should be performed at least once every five years and following a major change in anti-rheumatic medication [16].
The use of a validated composite measure as part of a standardised approach to CVD risk assessment in patients with RA enables an accurate risk prediction for individual patients [16]. This allows HCPs to inform patients about their prognosis and permits personalised treatment decisions for CVD prevention [17]. Numerous CVD risk assessment measures exist, from general population measures with and without adaptation for RA, to RA disease specific tools, examples of which can be seen in Online Resource 1. EULAR (European Alliance of Associations for Rheumatology, formally the European League Against Rheumatism) published recommendations on CVD risk management in patients with RA [16]. These recommendations suggest all patients with RA should be CVD risk assessed using a CVD risk assessment measure, recommended by either national or international guidelines. Furthermore, EULAR recommends all risk prediction algorithms not including RA as an independent variable should be adjusted by a 1.5 multiplication factor to enable more accurate risk prediction estimates in this patient cohort [16].
The delivery of CVD risk assessments, beyond the use of a composite measure has not been well defined. Supportive strategies may be in use to assist HCPs in delivering CVD risk assessments in practice. Therefore, the aim of this review was to identify the scope of literature available regarding CVD risk assessments undertaken by HCPs as part of routine care in patients with RA.
The objectives of this review were to:
-
I.
Map the strategies HCPs use to deliver CVD risk assessment in patients with RA.
-
II.
Determine how and who conducts a CVD risk assessment in patients with RA.
-
III.
Identify what composite measures are used in practice when assessing patients with RA for CVD risk.
Methods
This scoping review applied the Joanna Briggs Institute Methodological Guidelines [18]. A protocol for this review was registered with the Open Science Framework (https://osf.io/f68vu). The Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) checklist [19] was used to guide the reporting of this review and is available in Online Resource 2.
Eligibility criteria
The population, concept, and context (PCC) framework was used to determine the review eligibility criteria [18]. These were as follows: Population: Any HCP involved in the care of patients with RA; Concept: CVD risk assessment, including risk assessment using a risk prediction instrument as a composite measure of risk factors, as part of a risk management strategy, or risk prediction study; Context: Patients aged 18 years and older with RA cared for in any setting. We sought to include experimental and epidemiological studies including randomised and non-randomised controlled trials, quasi-experimental studies, prospective and retrospective cohort studies, case reports, cross-sectional studies, qualitative research, and grey literature such as policy statements, and government reports that yield data relating to CVD risk assessment in patients with RA as part of routine care. In this review, routine care was defined as an established way of working at the time a study or report was undertaken [20], as opposed to experimental systems introduced as part of an intervention for the study period only. Routine care encompasses patient centred centre, and is focused on individual patients, conducted by HCPs, in real-world settings, rather than investigative studies that tend to be focused on populations, involving researchers and research subjects, conducted under experimental conditions [21]. We included interventional studies where the intervention delivered CVD risk assessments in a routine care setting or where CVD risk assessment was part of routine care and the intervention aimed to enhance risk assessment rates or improve patient outcomes.
Studies involving patients with other forms of inflammatory joint disease where RA data couldn’t be isolated were excluded. Studies that focused on single risk factor prediction models or individual risk factor correlation/ incidence/ prevalence studies were also excluded. Studies where CVD risk assessment scoring was researcher led and conducted as part of the study intervention, rather than clinician led as part of routine care were excluded. Data relating to participants younger than 18 years of age were also excluded.
Information sources
Searches for peer-reviewed publications were conducted in six electronic databases (MEDLINE and CINAHL via EBSCO, the Cochrane Database of Systematic Reviews, Scopus, Web of Science and Academic Search Complete). Three trial registries (ClinicalTrials.gov, EU Clinical Trial Register, and the International Clinical Trials Registry Platform) were also searched to capture any relevant information.
Three grey literature databases (Base, OAIster, and Trip Pro) were searched for information relating to standard methods of CVD risk assessment in patients with RA internationally. Databases of relevant major medical clearing houses (Lenus, the National Guidelines Clearing House, and the Guidelines International Network) were also searched for information relating to policy documents or recommendations. Of note, grey literature searching was conducted with a focus on countries that score high on the human development index (HDI) and that possess similar healthcare development rankings such as life expectancy, education, and gross income per capita [22]. These countries include Ireland, the United Kingdom (UK), Denmark, Sweden, the Netherlands, the United States of America (USA), Canada, Australia, and New Zealand [23].
Considering the target population (i.e., patients with RA), further grey literature specific to the discipline of rheumatology was sought from the International League of Associations for Rheumatology website. This helped identify relevant information from regional partner organisations including EULAR, the American College of Rheumatology, the African League of Associations for Rheumatology, the Asia Pacific League of Associations for Rheumatology, and the Pan American League of Associations for Rheumatology.
Search strategy
Relevant keywords and subject headings were identified for CVD, risk assessment, and RA (Online Resource 3). Searches were last conducted in December 2023. The search strategy for each database is available in Online Resource 4. Searches were customised to all peer-reviewed electronic databases and limited to the English language. No date or setting limitations were applied to maximise retrieval. The reference lists of all sources deemed eligible and included in the review were searched for additional relevant studies.
Selection of sources of evidence
The web-based software tool Covidence was used to screen and select relevant studies from all information sources [24]. Duplicates were deleted automatically in Covidence. Title, abstract, and full text screenings were conducted independently by two authors (LM and either PC, MMS, or NC) and conflicts were resolved by a third.
Charting the data
A data extraction tool adapted from the Joanna Briggs Institute [18] was utilised to extract key information about the sources of evidence regarding the author(s), year of publication, country, aims, design, sample size and target population, CVD assessment delivery including any strategy used, who the assessment was conducted by and in what location, composite measure(s) used (including modifications), frequency of assessment, and study findings. Data extraction was completed by LM and checked for accuracy by PC, MMS, and NC.
Synthesis of results
A narrative synthesis was conducted from the extracted data using a priori determined headings guided by the objectives of this review and included: strategies used to CVD risk assess patients with RA, HCPs who conduct CVD risk assessments in patients with RA, the setting where CVD risk assessments took place, the composite measure used, if adjusted for RA, and frequency of measure application.
Results
Selection of sources of evidence
The initial search following deduplication yielded 3,243 results. After title and abstract screening, 207 records were included for full text review. Of those, 12 records were deemed eligible for inclusion in the review. All records were identified from electronic database searching. No records were included from trial registries or the grey literature search. Further details on study selection can be found in the PRISMA flowchart (Fig. 1).

PRISMA flow chart
Results of individual sources of evidence
Findings from the included studies, including study characteristics are available in the data extraction table (Table 1).
Characteristics of sources of evidence
Of the 12 studies included, three originated from Norway [30, 31, 35], two from the UK [27, 28], two from the Netherlands [34, 36] and one from: Ireland [26], France [29], Malta [33], Canada [32], and the USA [25]. Studies were published between 2009 [26] and 2023 [34]. The designs of included studies were quasi-experimental [25], pre-post intervention audit [26], survey [27], prospective observational [28, 29], service audits [30, 33], observational implementational [31], retrospective cohort and survey [32], cross-sectional observational [34, 35], and prospective cross-sectional [36]. Sample sizes ranged from 22 [29] to 4,483 [31] participants. The combined target populations of included studies were patients with RA (n = 8,420), rheumatology consultants (n = 119), and General Practitioners (GPs)/Family Physicians (n = 207).
Strategies
Strategies to support the delivery of CVD risk assessments in patients with RA in routine care were reported in eight studies [25, 26, 29,30,31, 34,35,36], three of which reported 100% CVD risk assessment rates in routine care (n = 125) [34], (n = 201) [35], (n = 720) [36]. Each strategy adopted various system-based interventions with two approaches to support delivery: (a) multidisciplinary team (MDT) collaboration [25, 30, 31, 35, 36] and (b) education [25, 26, 31].
System-based interventions involved the use of an electronic medical record reminder with a decision support tool [25], a shared care booklet [26], a standardised CVD risk assessment form [29], a purposively designed CVD risk assessment clinic [30], an electronic data collection and display system [31], structured scheduling of CVD risk assessment [34], a purposively designed CVD prevention clinic [35], and a guideline implementation project [36]. Electronic systems were used by two studies as strategies to support delivery of CVD risk assessments in practice. Akenroye et al.’s [25] electronic medical record reminder was deemed unsuccessful by the authors as CVD risk assessments were not performed in 93% (n = 104) of patients. Ikdahl et al. [31] also reported the use of an electronic support system to support delivery of CVD risk assessments and cite an assessment rate of 44.7% (n = 2,004) in practice which, in their opinion, was deemed successful. Ambrose et al. [26] used a shared care booklet to improve rates of CVD risk factor screening and assessment in practice and found, after re-auditing their service, improved rates of risk factor screening (necessary to conduct CVD risk assessments) from 60–85% for blood pressure, 58–75% for lipid profiles, and from 55–80% for weight assessment. Ikdahl et al. [30] reported the use of a purposively designed clinic for CVD risk factor measurement and assessment yielding a 52.1% (n = 276) assessment rate. Raadsen et al. [34] also reported the use of a similar system-based approach with scheduling of CVD risk assessment clinic visits and reported a 100% (n = 125) CVD risk assessment rate. Semb et al. [35] used additional vascular imaging as part of their CVD risk assessment strategy. In their observational study 42% (n = 85) were found to have improved CVD risk stratification as a direct result of identifying carotid plaque on ultrasound compared to using a composite measure alone. Van den Oever et al. [36] designed the I-CaRe project to implement Dutch cardiovascular risk management recommendations [37]. As a result, van den Oever et al. [36] report a 100% (n = 720) CVD risk assessment rate in practice.
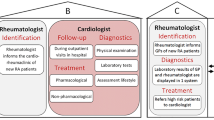
Of the studies that reported successful system-based interventions [30, 31, 34,35,36], four adopted an MTD approach to support delivery [30, 31, 35, 36]. Ikdahl et al. [30] developed a structured MDT clinic with defined roles for rheumatology doctors, nurses, and secretaries to implement European recommendations at that time [38]. They reported an increase of CVD risk assessment rates from 5.1% (n = 31) to 52.1% (n = 276) when patients were seen in the structured MDT clinic [OR = 20.97 (95% CI = 14.0; 31.3)]. Ikdahl et al. [31] presented results after implementation of a nation-wide quality assurance project involving a purposively designed CVD risk assessment programme. They also assigned duties to members of the rheumatology MDT and attribute its success primarily to this MDT approach. Semb et al. [35] reported the improvement of CVD risk stratification in their RA patient cohort because of specialised vascular imaging made possible by their cross disciplinary cardiology- rheumatology clinic. Van den Oever et al. [36] reported research nurses and rheumatology doctors undertake CVD risk assessments on all patients with RA as part of their Cardiovascular Risk Management in Rheumatoid Arthritis (I-Ca-Re) strategy, citing a 100% (n = 720) CVD risk assessment rate in routine care. Akenroye et al. [25] reported rheumatology consultants and GPs conducted CVD risk assessments collaboratively in their patients with RA, however despite implementing their electronic reminder, their intervention was deemed unsuccessful as assessment rates were only 7% (n = 8) in practice.
Education as a component of system-based interventions to support CVD risk assessment delivery was seen in three studies. Akenroye et al. [25] described the need for information sessions for participating rheumatologists. HCP and patient education was used in Ambrose et al.’s [26] shared care intervention to support CVD risk assessment delivery. The type, structure or content of this education was not described by the authors; however, a service audit eight months later demonstrated an improvement in measurement rates of CVD risk factors. Ikdahl et al. [31] reported the use of a CVD module and brief intervention training on smoking cessation and dietary advice for HCPs as part of their nationwide CVD risk assessment project.
Type of HCP conducting CVD risk assessments in patients with RA and the setting in which CVD risk assessments are carried out
Rheumatology doctors undertook CVD risk assessments on their own in four studies [26, 29, 32, 36], GPs undertook assessments in primary care in two studies [27, 28], and one study reported nurse led CVD risk assessment in routine care [34]. Another study reported that rheumatology consultants and GPs conducted CVD risk assessments on shared patients independently [25], and two studies reported involving a combination of rheumatology consultants, nurses, and secretaries in CVD risk assessment delivery [30, 31]. Information on who conducted CVD risk assessment was not reported in two papers [33, 35]. CVD risk assessments took place in the hospital setting [25, 26, 29,30,31,32,33,34,35,36], in primary care [25, 27, 28], in private practice [29], and in a rehabilitation centre [36].
CVD risk assessment (instrumentation)
Composite CVD risk assessment measures in use and frequency of application
A variety of general population CVD risk assessment measures were used: the Systemic Coronary Risk Evaluation (SCORE) calculator [30, 31, 33,34,35,36]; the Framingham Risk Score (FRS) [25, 26, 28, 29, 32]; the Q Research Cardiovascular Risk (Q Risk) calculator [27, 28]; the Joint British Societies (JBS) score [28]; and the American College of Cardiology/American Heart Association (ACC/AHA) calculator [35]. Two studies stated the use of more than one composite measure of CVD risk in routine care [28, 35]. Only four studies reported on the frequency of CVD risk reassessment, which was conducted on a yearly basis [30, 31, 33, 36].
Of the 12 studies, four acknowledged the increased risk of CVD due to systemic inflammation related to RA [30, 31, 33, 36] and three acknowledged the impact of both, RA disease-specific and RA treatment-specific factors that result in increased CVD risk [27, 29, 32]. Interpretation of CVD risk assessment in terms of the impact of RA was discussed in three studies [29, 34, 36], where it was acknowledged that higher RA disease activity results in an increased CVD risk and therefore timing of the CVD assessment, for patients with RA, should be completed when disease is quiescent.
Adjustment of CVD risk assessment measure for RA
Of the six studies that reported using the SCORE tool [30, 31, 33,34,35,36], five stated the results were adjusted for RA [30, 31, 33,34,35] with varying methods including application of the 1.5 coefficient [33,34,35], using the high-risk country chart [31], or adding 15 years to the patients age [36]. Four of the five studies that reported using the FRS did not state if it was adjusted for RA [25, 26, 28, 32]. Gossec et al. [29] who also reported using the FRS reminded rheumatology consultants to apply the 1.5 multiplication factor to the FRS score as part of their study requirements; however, they acknowledged they were unable to ascertain if the consultants complied. Authors that cited the JBS and the Q RISK 2 as being in use in routine care [27, 28] did not need to adjust results to account for RA as both calculators include RA as an independent variable. The Q RISK 2 was used by the GP samples in both Bell and Rowe’s [27] survey and Emanuel et al.’s [28] observational study. The JBS calculator cited by Emanual et al. [28] also includes RA as an independent variable. The ACC/AHA calculator reported in Semb et al.’s [35] study does not have RA as a variable in its algorithm nor does the study indicate the results were adjusted to account for RA related CVD risk.
Discussion
Results from this review demonstrated that although there is evidence that some strategies are used to support CVD risk assessment in patients with RA, extensive evidence establishing how HCPs conduct CVD risk assessments in practice is lacking. It was anticipated that a scoping review of the literature would yield the breadth of evidence necessary to map the strategies used in routine care. Many of the included studies focused on interventions to enhance current practices or reported CVD risk assessment as a by-product of an intervention to implement guidelines. Evidence such as retrospective chart reviews and standard operating protocols or procedures from professional rheumatology organisations might have allowed for more of a robust review of the current practice landscape.
From the studies included in this review, there is evidence to suggest that some strategies are used to support the delivery of CVD risk assessments in patients with RA [25, 26, 29,30,31, 34,35,36] with associated improved [29,30,31] or optimum [34,35,36] rates of assessment. Other evidence has been published that supports system-based programmes in the identification and measurement of CVD risk factors in patients with RA [39, 40], and system-based clinical decision supports for CVD risk assessment in the general population [41,42,43]. Tong et al. [44] suggests tools to assist HCPs in engaging in the CVD risk assessment conversation should also be developed with follow-up systems to facilitate CVD risk assessment and management. Of the 12 studies included in this review, four did not reference using any supportive strategy to deliver risk assessments in practice [27, 28, 32, 33]. Each of these four studies reported either low assessment rate levels [27, 28], inadequate management of CVD risk in general by the HCP [32], or low levels of CVD risk factor measurement [33]. Low CVD risk assessment rates in patients with RA results in missed opportunities for identification of CVD risk factors [45] and inhibits communication of individualised risk to the patient [46,47,48].
According to Gosh-Swaby et al. [49] patients who have the highest risk of developing CVD report the lowest awareness. Therefore, maximising assessment rates in practice is vital to ensure patients are aware of their individual risk, so treatments can be tailored accordingly. The supportive strategies identified in this review, albeit limited in numbers, reported improved or maximised rates of CVD assessment in routine care. By maximising rates of CVD risk assessment through supportive strategies and appropriate communication of CVD risk, more patients can become aware of their individual risk factors and can work with HCPs in initiating preventative therapy [49, 50].
Four of the five studies that used a system-based approach with MDT collaboration to support delivery of CVD risk assessments reported rates of between 44.7% -100% in practice [30, 31, 35, 36]. Despite adopting a cross disciplinary collaboration between rheumatologists and GPs to deliver CVD risk assessments in patients with RA, Akenroye et al. [25] reported assessment rates remained suboptimal at only 7% (n = 8). They suggest a possible reason for this was due to rheumatologists’ low awareness of RA related CVD risk. In contrast the broader literature has demonstrated that rheumatology consultants are aware of this risk but feel it’s the responsibility of the GPs to undertake CVD risk assessment in primary care [39, 46], demonstrating a lack of physician ownership in practice [51,52,53]. Three of these four studies involved nursing in their MDT collaboration [30, 31, 36]. One study cited independent nurse-led CVD risk assessment as part of routine care [34], without MTD collaboration but reported 100% CVD risk assessment rates. Studies exploring the impact of nurse-led care in patients with other chronic conditions have demonstrated improved outcomes compared to usual care [54,55,56,57]. Evidence has also been published to suggest nurses adopt a holistic and tailored approach to CVD risk assessment across a number of chronic conditions [58] with nurse-led CVD risk assessment programmes proving successful in the general population [59] primary care [60] and are well established in other chronic disease models of care [61,62,63]. Effective nurse-led CVD risk factor management programmes for patients with inflammatory disease have also been reported in the literature [64, 65]. According to European recommendations for the role of the nurse in inflammatory arthritis [66] rheumatology nurses should participate in comprehensive disease management and undertake extended roles to improve patient outcomes. Therefore, implementing nurse-led CVD risk assessment for patients with RA may prove effective in increasing rates and standardising delivery.
Strategies that used system-based interventions with an educational approach to support delivery of CVD risk assessments involved information sessions on CVD risk factor definitions and treatment goals [25], dual doctor and patient education interventions which were identified but not described in the text [26] and educating HCPs on health promotion advice [31]. Only one of these studies reported having satisfactory CVD risk assessment rates in practice of 44.7% (n = 2,004) [31]. Education highlighting the awareness of RA as an independent CVD risk factor was not seen in any of the included studies. Perhaps because the included studies were undertaken largely in hospital settings with rheumatology consultants who, according to Nguyen-Oghalai et al. [46], are aware of RA related CVD risk, therefore education of HCPs as a component of a CVD risk assessment framework might not be deemed necessary. Bell and Rowe’s [27] survey highlighted the importance of GP education where it was noted that GPs who had received education about RA, or who identified RA as a risk factor were significantly more likely to undertake a CVD risk assessment on patients with RA (p < 0.0001). Patient education was only seen in combination with HCP education in one study [26]. Protocols defining integrated roles for both rheumatology teams and GPs when CVD risk assessing patients with RA is essential but should also include patient education to compliment clinical discussions [67]. Only two studies reported incorporating both MDT collaboration and HCP education [25, 31] with varying results.
A number of CVD risk assessment measures were reported in use. Six of the European studies [30, 31, 33,34,35,36] reported using the SCORE calculator which was initially validated for use across 12 European cohorts [68]. Both the USA and Canadian studies [25, 32] cited the use of the FRS, mirroring the American validation cohort [69]. Both UK based studies [27, 28] reported using the Q RISK measure, aligning with the initial British derivation and validation cohort [70]. It appears, from this review, HCPs favour CVD risk assessment measures developed in cohorts similar to their patient populations. Measurements developed for and validated in specific countries may not be suitable for use in other countries unless adequate testing and validation has occurred, as differences in the prevalence of traditional risk factors across countries can affect risk scores, resulting in inaccurate risk predictions [71].
The most frequently cited assessment measure was the SCORE calculator [30, 31, 33,34,35,36] with five studies reporting score adjustment to account for RA [31, 33,34,35,36]. The FRS was also cited in use [25, 26, 28, 29, 32] but without reference to adjustment for RA. The FRS algorithm significantly underestimates CVD risk in RA patients, particularly older patients with positive serology and patients with persistently elevated inflammatory markers [72, 73]. Therefore, it is essential when using a general population calculator such as the FRS to adjust scores to account for RA related CVD risk [16].
This review found no RA disease specific CVD risk assessment measures in use in routine care. Disease specific calculators have been developed that include traditional CVD risk factors in their algorithm with the addition of disease specific variables such as clinical activity, corticosteroid use, and elements of functional ability (see in Online Resource 1) which have notable effects on CVD risk [74]. However, despite this, RA specific CVD risk calculators are not superior to general population CVD risk calculators in estimating future CVD risk in patients with RA [75, 76] and as a result are not recommended for use in patients with RA over modified general population risk calculators [16].
Of the five composite measures mentioned in the included studies, two include RA disease as an independent variable (Q RISK and JBS), [27, 28], recognizing the impact of inflammatory disease on CVD risk. None of the measures incorporated C-Reactive Protein, an inflammatory mediator, which rises in states of inflammation including flaring RA disease [77, 78]. Only one measure (Q RISK) captured corticosteroid use, recognizing the impact of medication on CVD risk. Of note, composite measures included in our review did not make a distinction between the role of inflammation from RA disease and the role of RA treatment (e.g., corticosteroids) in increased CVD risk.
Strengths and limitations
The search strategy for this review was not limited to a specific period to help retrieval and avoid reporting bias. The search field was broadened by using a number of platforms to search for sources of evidence including electronic databases, trial registries, and the grey literature. The double screening process helped ensure that relevant studies were not missed. As for limitations it is possible that studies reporting CVD risk screening practices might have also conducted CVD risk assessments as part of routine care but did not report it as a separate/discrete element.
Conclusions
Findings of this scoping review identified a variety of system-based interventions to support the delivery of CVD risk assessments in patients with RA, operationalised in different ways using one, or a combination of, two approaches: (a) MDT collaboration, and (b) education. Various HCPs deliver CVD risk assessments in different settings including the hospital, private practice, rehabilitation units and primary care. A number of general population CVD risk assessment measurements were cited in use by studies in this review, with and without adjustment for RA. This review demonstrates that although several strategies to support the delivery of CVD risk assessments in patients with RA are cited in use in the literature, there is limited evidence to suggest a standardised model has been applied in practice. This review has identified a gap in the literature of robust evidence detailing the CVD risk assessment practices of HCPs in the routine care of patients with RA. Research needs to be undertaken to establish the extent to which HCPs are CVD risk assessing their patients with RA as part of routine care.
Data Availability
The author confirms that all data generated or analysed during this study are available in supplementary information files 1–4.
References:
Cush JJ (2022) Rheumatoid arthritis: early diagnosis and treatment. Rheum Dis Clin North Am 48(2):537–547. https://doi.org/10.1016/j.rdc.2022.02.010
Safiri S, Kolahi AA, Hoy D, Smith E, Bettampadi D, Mansournia MA, Almasi-Hashiani A, Ashrafi-Asgarabad A, Moradi-Lakeh M, Qorbani M, Collins G, Woolf AD, March L, Cross M (2019) Global, regional and national burden of rheumatoid arthritis 1990–2017: a systematic analysis of the Global Burden of Disease study 2017. Ann Rheum Dis 78(11):1463–1471. https://doi.org/10.1136/annrheumdis-2019-215920
Almoallim H, Al Saleh J, Badsha H, Ahmed HM, Habjoka S, Menassa JA, El-Garf A (2020) A Review of the Prevalence and Unmet Needs in the Management of Rheumatoid Arthritis in Africa and the Middle East. Rheumatol Ther 8(1):1–16. https://doi.org/10.1007/s40744-020-00252-1
Rezuș E, Macovei LA, Burlui AM, Cardoneanu A, Rezuș C (2021) Ischemic heart disease and rheumatoid arthritis-two conditions, the same background. Life (Basel) 11(10):1042. https://doi.org/10.3390/life11101042
Aviña-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D (2008) Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum 59(12):1690–7. https://doi.org/10.1002/art.24092
Meune C, Touzé E, Trinquart L, Allanore Y (2009) Trends in cardiovascular mortality in patients with rheumatoid arthritis over 50 years: a systematic review and meta-analysis of cohort studies. Rheumatology (Oxford) 48(10):1309–13. https://doi.org/10.1093/rheumatology/kep252
Sparks JA, Chang SC, Liao KP, Lu B, Fine AR, Solomon DH, Costenbader KH, Karlson EW (2016) Rheumatoid Arthritis and Mortality Among Women During 36 Years of Prospective Follow-Up: Results From the Nurses’ Health Study. Arthritis Care Res (Hoboken) 68(6):753–62. https://doi.org/10.1002/acr.22752
Michaud K, Wolfe F (2007) Comorbidities in rheumatoid arthritis. Best Pract Res Clin Rheumatol 21(5):885–906. https://doi.org/10.1016/j.berh.2007.06.002
Jagpal A, Navarro-Millán I (2018) Cardiovascular co-morbidity in patients with rheumatoid arthritis: a narrative review of risk factors, cardiovascular risk assessment and treatment. BMC Rheumatol 2:10. https://doi.org/10.1186/s41927-018-0014-y
Olvera Lopez E, Ballard BD, Jan A (2023) Cardiovascular Disease. In: StatPearls [Internet]. StatPearls Publishing, Treasure Island
World Health Organisation (2022) The Top 10 causes of death—WHO | World Health Organization. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death. Accessed 8th Dec 2022
Joyce AT, Smith P, Khandker R, Melin JM, Singh A (2009) Hidden cost of rheumatoid arthritis (RA): estimating cost of comorbid cardiovascular disease and depression among patients with RA. J Rheumatol 36(4):743–52. https://doi.org/10.3899/jrheum.080670
Hollan I, Dessein PH, Ronda N, Wasko MC, Svenungsson E, Agewall S, Cohen-Tervaert JW, Maki-Petaja K, Grundtvig M, Karpouzas GA, Meroni PL (2015) Prevention of cardiovascular disease in rheumatoid arthritis. Autoimmun Rev 14(10):952–69. https://doi.org/10.1016/j.autrev.2015.06.004
Lloyd-Jones DM, Braun LT, Ndumele CE, Smith SC, Sperling LS, Virani SS, Blumenthal RS (2019) Use of risk assessment tools to guide decision-making in the primary prevention of atherosclerotic cardiovascular disease: a special report from the american heart association and American college of cardiology. Circle 139:e1162–e1177. https://doi.org/10.1161/CIR.0000000000000638
Cooney MT, Dudina AL, Graham IM (2009) Value and limitations of existing scores for the assessment of cardiovascular risk: a review for clinicians. J Am Coll Cardiol 54(14):1209–27. https://doi.org/10.1016/j.jacc.2009.07.020
Agca R, Heslinga SC, Rollefstad S, Heslinga M, McInnes IB, Peters MJ, Kvien TK, Dougados M, Radner H, Atzeni F, Primdahl J, Södergren A, Wallberg Jonsson S, van Rompay J, Zabalan C, Pedersen TR, Jacobsson L, de Vlam K, Gonzalez-Gay MA, Semb AG, Kitas GD, Smulders YM, Szekanecz Z, Sattar N, Symmons DP, Nurmohamed MT (2017) EULAR recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders: 2015/2016 update. Ann Rheum Dis 76(1):17–28. https://doi.org/10.1136/annrheumdis-2016-209775
de Vries TI, Visseren FLJ (2020) Cardiovascular risk prediction tools made relevant for GPs and patients. Heart heartjnl-2019-316377. https://doi.org/10.1136/heartjnl-2019-316377
Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, McInerney P, Godfrey CM, Khalil H (2021) Updated methodological guidance for the conduct of scoping reviews. JBI Evid Implement 19(1):3–10. https://doi.org/10.1097/XEB.0000000000000277
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, Moher D, Peters MDJ, Horsley T, Weeks L, Hempel S, Akl EA, Chang C, McGowan J, Stewart L, Hartling L, Aldcroft A, Wilson MG, Garritty C, Lewin S, Godfrey CM, Macdonald MT, Langlois EV, Soares-Weiser K, Moriarty J, Clifford T, Tunçalp Ö, Straus SE (2018) PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 169(7):467–473. https://doi.org/10.7326/M18-0850
Etzelmueller A, Vis C, Karyotaki E, Baumeister H, Titov N, Berking M, Cuijpers P, Riper H, Ebert DD (2020) Effects of internet-based cognitive behavioral therapy in routine care for adults in treatment for depression and anxiety: systematic review and meta-analysis. J Med Internet Res 22(8):e18100. https://doi.org/10.2196/18100
Sacristán JA (2015) Clinical research and medical care: towards effective and complete integration. BMC Med Res Methodol 15:4. https://doi.org/10.1186/1471-2288-15-4
United Nations Development Programme (2021) https://hdr.undp.org/data-center/human-development-index#/indicies/HDI Accessed 19th Dec 2022
Hegarty J, Flaherty SJ, Saab MM, Goodwin J, Walshe N, Wills T, McCarthy VJC, Murphy S, Cutliffe A, Meehan E, Landers C, Lehane E, Lane A, Landers M, Kilty C, Madden D, Tumelty M, Naughton C (2021) An international perspective on definitions and terminology used to describe serious reportable patient safety incidents: a systematic review. J Patient Saf 17(8):e1247–e1254. https://doi.org/10.1097/PTS.0000000000000700
Covidence systematic review software (2023) Veritas health innovation, Melbourne, Australia. Available at www.covidence.org. Accessed 11 Dec 2023
Akenroye AT, Kumthekar AA, Alevizos MK, Mowrey WB, Broder A (2017) Implementing an electronic medical record-based reminder for cardiovascular risk screening in rheumatoid arthritis. Arthritis Care Res (Hoboken) 69(5):625–632. https://doi.org/10.1002/acr.22966
Ambrose NL, O’Connell P, Kearns G (2009) Limiting cardiovascular risk in Irish rheumatoid arthritis patients. Ir J Med Sci 178(1):53–5. https://doi.org/10.1007/s11845-008-0252-x
Bell C, Rowe IF (2011) The recognition and assessment of cardiovascular risk in people with rheumatoid arthritis in primary care: a questionnaire-based study of general practitioners. Musculoskeletal Care 9(2):69–74. https://doi.org/10.1002/msc.196
Emanuel G, Charlton J, Ashworth M, Gulliford MC, Dregan A (2016) Cardiovascular risk assessment and treatment in chronic inflammatory disorders in primary care. Heart 102(24):1957–1962. https://doi.org/10.1136/heartjnl-2016-310111
Gossec L, Salejan F, Nataf H, Nguyen M, Gaud-Listrat V, Hudry C, Breuillard P, Dernis E, Boumier P, Durandin-Truffinet M, Fannius J, Fechtenbaum J, Izou-Fouillot MA, Labatide-Alanore S, Lebrun A, LeDevic P, LeGoux P, Sacchi A, Salliot C, Sparsa L, d’André FL, Dougados M, Rheumatology Network RHEVER (2013) Challenges of cardiovascular risk assessment in the routine rheumatology outpatient setting: an observational study of 110 rheumatoid arthritis patients. Arthritis Care Res (Hoboken) 65(5):712–7. https://doi.org/10.1002/acr.21935
Ikdahl E, Rollefstad S, Olsen IC, Kvien TK, Hansen IJ, Soldal DM, Haugeberg G, Semb AG (2015) EULAR task force recommendations on annual cardiovascular risk assessment for patients with rheumatoid arthritis: an audit of the success of implementation in a rheumatology outpatient clinic. Biomed Res Int 2015:515280. https://doi.org/10.1155/2015/515280
Ikdahl E, Rollefstad S, Wibetoe G, Salberg A, Krøll F, Bergsmark K, Kvien TK, Olsen IC, Soldal DM, Bakland G, Lexberg Å, Gjesdal CG, Gulseth C, Haugeberg G, Semb AG (2018) Feasibility of cardiovascular disease risk assessments in rheumatology outpatient clinics: experiences from the nationwide NOCAR project. RMD Open 4(2):e000737. https://doi.org/10.1136/rmdopen-2018-000737
Ladak K, Hashim J, Clifford-Rashotte M, Tandon V, Matsos M, Patel A (2018) Cardiovascular risk management in rheumatoid arthritis: A large gap to close. Musculoskeletal Care 16(1):152–157. https://doi.org/10.1002/msc.1196
Magro R, Buhagiar M, Taliana N, Borg AA (2014) Cardiovascular risk assessment and management in rheumatoid arthritis: are guidelines being followed? Malta Med J 26(1):49–54. https://www.um.edu.mt/library/oar/bitstream/123456789/1625/1/2014.Vol26.Issue1.A9.pdf. Accessed 11 Dec 2023
Raadsen R, Hansildaar R, van Kuijk AWR, Nurmohamed MT (2023) Male rheumatoid arthritis patients at substantially higher risk for cardiovascular mortality in comparison to women. Semin Arthritis Rheum 62:152233. https://doi.org/10.1016/j.semarthrit.2023.152233
Semb AG, Ikdahl E, Hisdal J, Olsen IC, Rollefstad S (2016) Exploring cardiovascular disease risk evaluation in patients with inflammatory joint diseases. Int J Cardiol 223:331–336. https://doi.org/10.1016/j.ijcard.2016.08.129
van den Oever IAM, Heslinga M, Griep EN, Griep-Wentink HRM, Schotsman R, Cambach W, Dijkmans BAC, Smulders YM, Lems WF, Boers M, Voskuyl AE, Peters MJL, van Schaardenburg D, Nurmohamed MT (2017) Cardiovascular risk management in rheumatoid arthritis patients still suboptimal: the implementation of cardiovascular risk management in rheumatoid arthritis project. Rheumatology (Oxford) 56(9):1472–1478. https://doi.org/10.1093/rheumatology/kew497
Wiersma T, Smulders YM, Stehouwer CD, Konings KT, Lanphen J (2012) Samenvatting van de multidisciplinaire richtlijn 'Cardiovasculair risicomanagement' (herziening 2011) [Summary of the multidisciplinary guideline on cardiovascular risk management (revision 2011)] (in Dutch). Ned Tijdschr Geneeskd 156(36):A5104. Dutch
Peters MJ, Symmons DP, McCarey D, Dijkmans BA, Nicola P, Kvien TK, McInnes IB, Haentzschel H, Gonzalez-Gay MA, Provan S, Semb A, Sidiropoulos P, Kitas G, Smulders YM, Soubrier M, Szekanecz Z, Sattar N, Nurmohamed MT (2010) EULAR evidence-based recommendations for cardiovascular risk management in patients with rheumatoid arthritis and other forms of inflammatory arthritis. Ann Rheum Dis 69(2):325–31. https://doi.org/10.1136/ard.2009.113696
Bartels CM, Roberts TJ, Hansen KE, Jacobs EA, Gilmore A, Maxcy C, Bowers BJ (2016) Rheumatologist and primary care management of cardiovascular disease risk in rheumatoid arthritis: patient and provider perspectives. Arthritis Care Res (Hoboken) 68(4):415–23. https://doi.org/10.1002/acr.22689
Primdahl J, Clausen J, Hørslev-Petersen K (2013) Results from systematic screening for cardiovascular risk in outpatients with rheumatoid arthritis in accordance with the EULAR recommendations. Ann Rheum Dis 72(11)
Njie GJ, Proia KK, Thota AB, Finnie RKC, Hopkins DP, Banks SM, Callahan DB, Pronk NP, Rask KJ, Lackland DT, Kottke TE; Community Preventive Services Task Force (2015) Clinical decision support systems and prevention: a community guide cardiovascular disease systematic review. Am J Prev Med 49(5):784–795. https://doi.org/10.1016/j.amepre.2015.04.006
Holt TA, Thorogood M, Griffiths F, Munday S, Friede T, Stables D (2010) Automated electronic reminders to facilitate primary cardiovascular disease prevention: randomised controlled trial. Br J Gen Pract 60(573):e137-43. https://doi.org/10.3399/bjgp10X483904
Yunda J, Pacheco D, Millan J (2015) A web-based fuzzy inference system based tool for cardiovascular disease risk assessment. NOVA 13(24):7–16. https://doi.org/10.22490/24629448.1712
Tong M, Gilmore-Bykovskyi A, Block L, Ramly E, White DW, Messina ML, Bartels CM (2022) Rheumatology clinic staff needs: barriers and strategies to addressing high blood pressure and smoking risk. J Clin Rheumatol 28(7):354–361. https://doi.org/10.1097/RHU.0000000000001868
Barber CE, Esdaile JM, Martin LO, Faris P, Barnabe C, Guo S, Lopatina E, Marshall DA (2016) Gaps in addressing cardiovascular risk in rheumatoid arthritis: assessing performance using cardiovascular quality indicators. J Rheumatol 43(11):1965–1973. https://doi.org/10.3899/jrheum.160241
Nguyen-Oghalai TU, Hunnicutt SE, Smith ST, Maganti R, McNearney TA (2007) Factors that impact decision making among rheumatologists in the initiation of treatment for hypertension in rheumatoid arthritis. J Clin Rheumatol 13(6):307–12. https://doi.org/10.1097/RHU.0b013e318156bcc2
Barber CE, Smith A, Esdaile JM, Barnabe C, Martin LO, Faris P, Hazlewood G, Noormohamed R, Alvarez N, Mancini GB, Lacaille D, Keeling S, Aviña-Zubieta JA, Marshall D (2015) Best practices for cardiovascular disease prevention in rheumatoid arthritis: a systematic review of guideline recommendations and quality indicators. Arthritis Care Res (Hoboken) 67(2):169–79. https://doi.org/10.1002/acr.22419
Schmidt TJ, Aviña-Zubieta JA, Sayre EC, Abrahamowicz M, Esdaile JM, Lacaille D (2018) Quality of care for cardiovascular disease prevention in rheumatoid arthritis: compliance with hyperlipidemia screening guidelines. Rheumatology (Oxford) 57(10):1789–1794. https://doi.org/10.1093/rheumatology/key164
Ghosh-Swaby OR, Kuriya B (2019) Awareness and perceived risk of cardiovascular disease among individuals living with rheumatoid arthritis is low: results of a systematic literature review. Arthritis Res Ther 21(1):33. https://doi.org/10.1186/s13075-019-1817-y
Teoh BC, Syed Sulaiman SA, Tan BE (2020) Knowledge of cardiovascular disease risk in rheumatoid arthritis patients before and after educational intervention from a Southeast Asia country: Malaysia. Arch Rheumatol 36(1):63–71. https://doi.org/10.46497/ArchRheumatol.2021.7726
Navarro-Millán I, Cornelius-Schecter A, O’Beirne RJ, Morris MS, Lui GE, Goodman SM, Cherrington AL, Fraenkel L, Curtis JR, Safford MM (2020) Views of primary care physicians and rheumatologists regarding screening and treatment of hyperlipidemia among patients with rheumatoid arthritis. BMC Rheumatol 4:14. https://doi.org/10.1186/s41927-020-0112-5
Navarro-Millán I, Young SR, Shurbaji S, McDavid C, Cornelius-Schecter A, Johnson B, Cherrington AL, Fraenkel L, Goodman SM, Curtis JR, Venkatachalam S, Safford MM (2020) Barriers and facilitators for screening and treatment of hyperlipidemia among patients with inflammatory arthritis. BMC Rheumatol 4:26. https://doi.org/10.1186/s41927-020-00123-w
Semb AG, Ikdahl E, Wibetoe G, Crowson C, Rollefstad S (2020) Atherosclerotic cardiovascular disease prevention in rheumatoid arthritis. Nat Rev Rheumatol 16(7):361–379. https://doi.org/10.1038/s41584-020-0428-y
Chan RJ, Marx W, Bradford N, Gordon L, Bonner A, Douglas C, Schmalkuche D, Yates P (2018) Clinical and economic outcomes of nurse-led services in the ambulatory care setting: A systematic review. Int J Nurs Stud 81:61–80. https://doi.org/10.1016/j.ijnurstu.2018.02.002
Murfet GO, Allen P, Hingston TJ (2014) Maternal and neonatal health outcomes following the implementation of an innovative model of nurse practitioner-led care for diabetes in pregnancy. J Adv Nurs 70(5):1150–1163. https://doi.org/10.1111/jan.12277
Xu H, Mou L, Cai Z (2017) A nurse-coordinated model of care versus usual care for chronic kidney disease: meta-analysis. J Clin Nurs 26(11–12):1639–1649. https://doi.org/10.1111/jocn.13533
Hendriks JM, de Wit R, Crijns HJ, Vrijhoef HJ, Prins MH, Pisters R, Pison LA, Blaauw Y, Tieleman RG (2012) Nurse-led care vs. usual care for patients with atrial fibrillation: results of a randomized trial of integrated chronic care vs. routine clinical care in ambulatory patients with atrial fibrillation. Eur Heart J 33(21):2692–9. https://doi.org/10.1093/eurheartj/ehs071. Erratum in: Eur Heart J. 2013 Feb;34(6):408
Primdahl J, Ferreira RJ, Garcia-Diaz S, Ndosi M, Palmer D, van Eijk-Hustings Y (2016) Nurses’ role in cardiovascular risk assessment and management in people with inflammatory arthritis: a European perspective. Musculoskelet Care 14(3):133–51. https://doi.org/10.1002/msc.1121
Kavita, Thakur JS, Vijayvergiya R, Ghai S (2020) Task shifting of cardiovascular risk assessment and communication by nurses for primary and secondary prevention of cardiovascular diseases in a tertiary health care setting of Northern India. BMC Health Serv Res 20(1):10. https://doi.org/10.1186/s12913-019-4864-9
Tiessen AH, Smit AJ, Broer J, Groenier KH, Meer KVD (2012) Randomized controlled trial on cardiovascular risk management by practice nurses supported by self monitoring in primary care. BMC Fam Pract 3:90. https://doi.org/10.1186/1471-2296-13-90
Woodward A, Wallymahmed M, Wilding J, Gill G (2006) Successful cardiovascular risk reduction in type 2 diabetes by nurse-led care using an open clinical algorithm. Diabet Med 23(7):780–7. https://doi.org/10.1111/j.1464-5491.2006.01889.x
McLoughney CR, Khan ASA, Ahmed AB (2007) Effectiveness of a specialist nurse-led intervention clinic in the management of cardiovascular risk factors in diabetes. Eur Diab Nursing 4:100–105. https://doi.org/10.1002/edn.89
Zhang J, Zheng X, Ma D, Liu C, Ding Y (2022) Nurse-led care versus usual care on cardiovascular risk factors for patients with type 2 diabetes: a systematic review and meta-analysis. BMJ Open 12(3):e058533. https://doi.org/10.1136/bmjopen-2021-058533
Bartels CM, Ramly E, Johnson HM, Lauver DR, Panyard DJ, Li Z, Sampene E, Lewicki K, McBride PE (2019) Connecting rheumatology patients to primary care for high blood pressure: specialty clinic protocol improves follow-up and population blood pressures. Arthritis Care Res (Hoboken) 71(4):461–470. https://doi.org/10.1002/acr.23612
Bartels CM, Johnson L, Ramly E, Panyard DJ, Gilmore-Bykovskyi A, Johnson HM, McBride P, Li Z, Sampene E, Lauver DR, Lewicki K, Piper ME (2022) Impact of a rheumatology clinic protocol on tobacco cessation quit line referrals. Arthritis Care Res (Hoboken) 74(9):1421–1429. https://doi.org/10.1002/acr.24589
Bech B, Primdahl J, van Tubergen A, Voshaar M, Zangi HA, Barbosa L, Boström C, Boteva B, Carubbi F, Fayet F, Ferreira RJO, Hoeper K, Kocher A, Kukkurainen ML, Lion V, Minnock P, Moretti A, Ndosi M, Pavic Nikolic M, Schirmer M, Smucrova H, de la Torre-Aboki J, Waite-Jones J, van Eijk-Hustings Y (2020) 2018 update of the EULAR recommendations for the role of the nurse in the management of chronic inflammatory arthritis. Ann Rheum Dis 79(1):61–68. https://doi.org/10.1136/annrheumdis-2019-215458
John H, Hale ED, Treharne GJ, Korontzis K, Obrenovic K, Carroll D, Kitas GD (2011) Patient evaluation of a novel patient education leaflet about heart disease risk among people with rheumatoid arthritis. Musculoskeletal Care 9(4):194–9. https://doi.org/10.1002/msc.207
Conroy RM, Pyörälä K, Fitzgerald AP, Sans S, Menotti A, De Backer G, De Bacquer D, Ducimetière P, Jousilahti P, Keil U, Njølstad I, Oganov RG, Thomsen T, Tunstall-Pedoe H, Tverdal A, Wedel H, Whincup P, Wilhelmsen L, Graham IM, SCORE project group (2003) Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J 24(11):987–1003. https://doi.org/10.1016/s0195-668x(03)00114-3
Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB (1998) Prediction of coronary heart disease using risk factor categories. Circ 97(18):1837–47. https://doi.org/10.1161/01.cir.97.18.1837
Hippisley-Cox J, Coupland C, Vinogradova Y, Robson J, May M, Brindle P (2007) Derivation and validation of QRISK, a new cardiovascular disease risk score for the United Kingdom: prospective open cohort study. BMJ 335(7611):136. https://doi.org/10.1136/bmj.39261.471806.55
Hermansson J, Kahan T (2018) Systematic review of validity assessments of Framingham risk score results in health economic modelling of lipid-modifying therapies in Europe. Pharmacoeconomics 36(2):205–213. https://doi.org/10.1007/s40273-017-0578-1
Crowson CS, Matteson EL, Roger VL, Therneau TM, Gabriel SE (2012) Usefulness of risk scores to estimate the risk of cardiovascular disease in patients with rheumatoid arthritis. Am J Cardiol 110(3):420–4. https://doi.org/10.1016/j.amjcard.2012.03.044
Arts EE, Popa C, Den Broeder AA, Semb AG, Toms T, Kitas GD, van Riel PL, Fransen J (2015) Performance of four current risk algorithms in predicting cardiovascular events in patients with early rheumatoid arthritis. Ann Rheum Dis 74(4):668–74. https://doi.org/10.1136/annrheumdis-2013-204024
Bonek K, Głuszko P (2016) Cardiovascular risk assessment in rheumatoid arthritis - controversies and the new approach. Reumatologia 54(3):128–35. https://doi.org/10.5114/reum.2016.61214
Crowson CS, Gabriel SE, Semb AG, van Riel PLCM, Karpouzas G, Dessein PH, Hitchon C, Pascual-Ramos V, Kitas GD: Trans-Atlantic Cardiovascular Consortium for Rheumatoid Arthritis (2017) Rheumatoid arthritis-specific cardiovascular risk scores are not superior to general risk scores: a validation analysis of patients from seven countries. Rheumatol (Oxford) 56(7):1102–1110. https://doi.org/10.1093/rheumatology/kex038
Solomon DH, Greenberg J, Curtis JR, Liu M, Farkouh ME, Tsao P, Kremer JM, Etzel CJ (2015) Derivation and internal validation of an expanded cardiovascular risk prediction score for rheumatoid arthritis: a consortium of rheumatology researchers of North America registry study. Arthritis Rheumatol 67(8):1995–2003. https://doi.org/10.1002/art.39195Erratum.In:ArthritisRheumatol.2016Feb;68(2):515
Bechman K, Tweehuysen L, Garrood T, Scott DL, Cope AP, Galloway JB, Ma MHY (2018) Flares in rheumatoid arthritis patients with low disease activity: predictability and association with worse clinical outcomes. J Rheumatol 45(11):1515–1521. https://doi.org/10.3899/jrheum.171375
Sproston NR, Ashworth JJ (2018) Role of C-reactive protein at sites of inflammation and infection. Front Immunol 13(9):754. https://doi.org/10.3389/fimmu.2018.00754
Funding
Open Access funding provided by the IReL Consortium. This research was undertaken as part of a PhD programme of study supported by an employment-based scholarship funded by the College of Medicine and Health, University College Cork.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Murphy, L., Saab, M.M., Cornally, N. et al. Cardiovascular disease risk assessment in patients with rheumatoid arthritis: A scoping review. Clin Rheumatol 43, 2187–2202 (2024). https://doi.org/10.1007/s10067-024-06996-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-024-06996-3