
Abstract
Background
The issue of sex differences in stroke has gained concern in the past few years. However, multicenter studies are still required in this field. This study explores sex variation in a large number of patients and compares stroke characteristics among women in different age groups and across different countries.
Methods
This multicenter retrospective cross-sectional study aimed to compare sexes regarding risk factors, stroke severity, quality of services, and stroke outcome. Moreover, conventional risk factors in women according to age groups and among different countries were studied.
Results
Eighteen thousand six hundred fifty-nine patients from 9 countries spanning 4 continents were studied. The number of women was significantly lower than men, with older age, more prevalence of AF, hypertension, and dyslipidemia. Ischemic stroke was more severe in women, with worse outcomes among women (p: < 0.0001), although the time to treatment was shorter. Bridging that was more frequent in women (p:0.002). Analyzing only women: ischemic stroke was more frequent among the older, while hemorrhage and TIA prevailed in the younger and stroke of undetermined etiology. Comparison between countries showed differences in age, risk factors, type of stroke, and management.
Conclusion
We observed sex differences in risk factors, stroke severity, and outcome in our population. However, access to revascularization was in favor of women.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The incidence of ischemic stroke is increasing with age, especially among women. It ranges from 41.5–70.5/100 thousand in western countries to 131–151.5/100 thousand in eastern countries [1].
Since 2001, the Institute of Medicine has highlighted the importance of studying sex differences in diseases and its impact on outcome [2].
Exploring such differences can promote more precise management protocols in acute and chronic stroke settings. Furthermore, data about sex variability concerning the delay of onset to door and door to treatment times still need unravelling, as this information can impact equity of stroke services and, consequently, stroke outcome [3].
And despite that several articles have demonstrated a minimal sex difference in revascularization therapy yet, this might still negatively influence disease outcomes in women [4, 5].
Moreover, even fewer studies have touched on the issue of stroke in women in the context of an epidemiological study among different geographical regions [6].
Furthermore, the variance in ethnicity, culture, nutrition, and health habits among populations can influence sex-related health services. Thus, stroke risk factors in women need to be investigated in various regions of the world.
Accordingly, the current study was conducted to compare sex differences relevant to stroke risk factors, quality of management, and outcome of acute ischemic stroke (AIS). In addition, we were also interested in exploring these sex differences among various countries.
Methods
This is a multicentric, observational, cross-sectional, retrospective study done by analyzing stroke units’ databases of participating countries.
Representatives of stroke units/centers who previously participated and co-authored an earlier study [7] were contacted through email and invited to share their stroke units’ data for analysis. Time period was specified in the study protocol sent to all participating centers as “The past 5 years from January 2017 till January 2022.”
A total of 9 centers, representing 9 different countries and 4 continents, participated, including Egypt, Iran, Oman, Poland, Romania, Spain, the USA, Turkey, and Paraguay. All types of stroke were studied (acute ischemic stroke (AIS), hemorrhagic, transient ischemic attack (TIA), and subarachnoid hemorrhage). The study population was evaluated for risk factors, stroke subtypes, stroke severity according to the National Institutes of Health Stroke Scale (NIHSS), and acute stroke management based on current international guidelines: intravenous thrombolysis (IVT), thrombectomy (MT), or bridging between men and women. The outcome was measured by the modified Rankin scale (mRS), defining favorable outcome as mRS < 2.
Women were further divided into the childbearing period (CB) (18–45 years), premenopausal (PM) (46–60 years), and menopausal (M) (> 60 years). A comparison was made between different age categories regarding types of stroke, TOAST classification of ischemic stroke, management, and outcome on discharge and at 3 months follow-up.
Finally, a comparison among countries was made for age, risk factors, type of stroke, and management.
Statistics
Statistical analysis was done using SPSS version 19th (SPSS Inc., Chicago). To test for normality of continuous data distribution, the Shapiro-Wilks test was used. Mean and standard deviation were used for normally distributed data, while median and interquartile range (IQR) were used for shewed data. Categorical data were presented as frequencies. The Mann–Whitney test or Kruskal–Wallis test was used to compare not normally distributed continuous variables with nominal independent variables. The chi-square test was used for comparison of nominal data.
Results
Demographic data and clinical characteristics for both groups: (Table 1)
Risk factors
A total of 18,659 patients were studied most of whom (68%) were in the age group > 60 years. Women constituted 44.1% and had a significantly higher age than men (p < 0.0001). The number of women was significantly lower than men in premenopausal age group, and higher in menopausal age group (p < 0.0001).
Regarding risk factors, women had more atrial fibrillation (AF), hypertension, and dyslipidemia (p < 0.0001). At the same time, they were significantly lower in smoking (p < 0.0001) and other vascular diseases (p = 0.02).
Type of stroke
Ischemic strokes were more frequent in men than in women (p = 0.03), while TIA was more in women (p < 0.000). There was no difference in hemorrhagic between both sexes.
Stroke severity and management
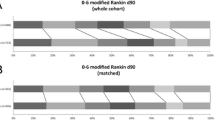
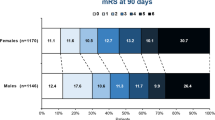
NIHSS was significantly higher in women on admission. Moreover, the outcome, as measured by mRS, was less favorable in women at discharge and after 3 months (p < 0.0001). On the other hand, the type of acute management whether conservative or revascularization was similar, except for bridging therapy that was more frequently performed in women (p = 0.002).
Onset to door time (OTD) was significantly lower in women (p < 0.0001), while door to needle (DTN) and hospital stay showed no difference between the sexes.
Comparison of stroke characteristics among women: (Table 2)
Women tend to be significantly older (p < 0.0001). Ischemic stroke was significantly higher among the older age group (post hoc analysis: menopausal group significantly more than the two younger age groups). On the contrary, hemorrhagic stroke, subarachnoid hemorrhage, and TIA were significantly higher in younger groups (post hoc analysis: the non-significant difference between CB and PM, and significant difference between both groups and M group).
According to TOAST classification, small vessel stroke and large vessel stroke were higher in the PM group (post hoc analysis: significantly higher incidence in PM compared to the other two groups and higher in M compared to CB group). Cardio-embolic stroke was significantly higher in M group as compared to the 2 other younger groups, while there was no difference between CB and PM groups. Stroke of undetermined etiology was higher in younger age (CB) (post hoc analysis: significantly less in M compared to the other two groups). Stroke of other determined etiology was significantly more in CB age group as compared to the other two groups.
Onset to needle and door to needle times showed no disparity among age groups. There was a marginal difference in favor of CB and PM groups compared to M group for conservative management (p = 0.03), marginal difference in favor of M group compared with the two younger groups for MT (p = 0.04, 0.03), and no difference regarding IVT.
And NIHSS on admission was significantly higher in M group (p < 0.001), whereas favorable outcome on discharge and at 3 months was more frequently reported in younger age groups, being more significantly in CB compared to both PM and M and in PM compared to M (p < 0.0001).
Risk Factors according to sex among participating countries: (Table 3)
The median age in women was lower in both Egypt and Oman as compared to all other countries, and this comes in the context of a younger age of men, as well. It is also notable that the frequency of patients in the 2 younger age groups was higher in these 2 countries (37.2% and 50% respectively) compared to less than 30% in other countries.
AF was significantly more reported among women in Egypt, Iran, Poland, Spain, and Turkey. Hypertension was more reported in women in Egypt, Iran, Spain, and Turkey, and more in men in Poland.
Diabetes was more frequent in women in Iran and Turkey, and more in men in the USA. Dyslipidemia was significantly more frequent in women in Iran only. Smoking was more frequent in men in Egypt, Iran, Spain, USA, Turkey, and Paraguay.
Previous stroke and congestive heart failure showed non-significant difference among both sexes in all countries. And other vascular diseases were more in men only in Egypt.
Comparison of stroke severity, type, intervention, and outcome among the participating countries: (Tables 4 and 5)
Severity
NIHSS was higher in women in all countries except Poland, where men had a severer stroke. Egypt, Iran, the USA, and Paraguay had significantly more severe strokes in women than in other countries.
Type of stroke
Incidence of ischemic stroke was significantly more in women in Oman and Poland, while it was more in men in the USA. Hemorrhagic stroke was significantly more in men in Oman and Poland.
TIA was more in women in Iran. Moreover, in Egypt and Oman, subarachnoid hemorrhage was similar in both sexes, while other countries did not report it.
As for acute management, in Egypt, only bridging therapy was significantly more often in women; in Oman IVT and MT were more in women, while conservative therapy was more in men so was bridging therapy. Poland reported IVT and bridging more in women, while conservative therapy was more frequently given to men.
Outcome was worse among women in all countries except Poland. This sex difference was significant in Egypt, Iran, USA, and Turkey.
Discussion
The study of sex differences is an emerging field of stroke epidemiology and care. This study explored sex differences related to various aspects of stroke etiology and management.
Comparison between sexes in the whole sample
Among the studied cohort of 18,659 patients, stroke incidence was higher among men with a ratio of 1.27:1. And despite that the ratio might vary among studies, yet the incidence is consistently higher among men. Generally speaking, women reportedly have a lower risk of developing stroke than men, though the magnitude of this difference decreases after menopause [8]. In line with this, most of the participating countries reported that age-related difference was reversed for those aged above 60.
Similar to previously published studies, the mean age at stroke presentation was higher among women [9, 10]. On average, women were about 4 years older than men, which is concordant with other research that has also demonstrated that women were older at the time of their first stroke [11, 12].
Regarding the mean age of the whole patients (males and females), we noticed that Egyptian stroke patients were younger than stroke patients in other countries. It is noticeable in most studies from Egypt that the age of stroke patients is younger than other countries. This is possibly either due to multiple risk factors or is genetically determined. The mean age is around 62 in several of our previous research [13, 14].
Regarding risk factor profile according to sex, our findings coincide with other studies [15,16,17,18]. Most important to mention is AF that is consistently relevant to sex so female sex has been incorporated as a risk factor in the CHADS2VASc2 score for decision-making about anticoagulation [19].
There was a disparity between our findings and other studies reporting higher prevalence of dyslipidaemia in women [20]. The prevalence of dyslipidaemia was reportedly associated with higher socioeconomic development and is attributable to western diet and high caloric intake [21].
Thus, this low prevalence of dyslipidaemia in our sample could be due to racial differences or dietary habits, given the preponderance of eastern population reaching 61% among our cohort.
On comparison of stroke subtypes, although we found variable patterns between both sexes, yet others reported that with the exception of SAH, there is little evidence of sex difference in stroke subtypes [4, 20, 22].
Regarding stroke severity and outcome, we found that women had a severer stroke on admission and worse outcome which could be attributed to their older age at the time of stroke incidence. However even after adjusting for age, still female sex per se was found to be a determinant for negative outcome [23, 24]. In addition, the poor outcome in women has been ascribed to lower pre-stroke functional status, body mass index, AF, and hypertension [25].
But despite this sex difference in outcome, our results illustrated that the type of management was similar for sexes except for bridging therapy that was more frequently administered in women. Pre-hospital delay was significantly lower among women, while other in-hospital time factors showed no difference. Many previous western studies reported that OTD is longer in women. We suppose that this trend might have changed in the past few years, that is why the title of our article is “Do stroke services still show sex differences? A multicentre study.” We have 2 comments here. First that the bigger number of patients in our study (11,295) is from eastern countries versus (7364) from western countries. Thus, the results might be colored by the eastern culture where elderly women are usually living with caregivers from the family, and any health issue is promptly attended to by family members. This cultural notion was highlighted in a recent reference stating “women are less likely to receive IVT compared to men in the US and most European countries, but not in Asia and Germany.” [26] Second, the trends might be changing due to public awareness of stroke and urgency of early treatment; thus, the gap between sexes is diminishing. This has been mentioned in the same study as the one cited below where they stated “Subgroup analyses including only patients deemed eligible for IVT however did not show any significant sex difference in IVT treatment anymore.” [26].
The sex difference in revascularization therapy varied among various studies. It was previously observed in European and US-based studies but not in studies from Asia and Germany [24, 27].
Comparison between age groups among women
Concerning stroke subtype, similar to other studies, the presence of cardio-embolic stroke in older patients is explained by higher prevalence of AF [28]. On the other hand, the absence of conventional risk factors explains why younger age group presented with stroke of undetermined/other determined etiology [29, 30].
When it comes to severity and outcome, the presence of comorbidities and premorbid state related to aging, in addition to the higher incidence of cardio-embolic stroke, could explain severer stroke in advanced age [31].
Comparison of stroke characteristics across participating countries
The median age of women in both Egypt and Oman was younger as compared to all other countries, and this comes in the context of a younger age of stroke for the whole population [23].
The younger age of stroke patients in Egypt and Oman compared to other countries, and on the contrary the very few young patients in Poland, both need further verification by future research.
Also, Poland was the only country to have less stroke severity and better outcome among women, possibly because women had significantly less prevalence of hypertension and less hemorrhagic strokes than men. Moreover, women who had an ischemic stroke were more prone to receive IVT and bridging therapy.
Similar to a previous study [15], there was a trend towards administering interventional management to women that reached a significantly higher level than men in some countries. The shorter onset to door reported for women could be a contributing factor for the type of management.
We can conclude that globally, stroke services provided to women are no more inferior to those provided to men, thanks to previous work that drew attention to this sex disparity. Despite that, still female sex remains an unmodifiable risk factor for severer stroke and worse outcome. Thus, future studies are warranted to explore modifiable female-related risk factors including pregnancy, postpartum, and hormonal changes [8].
Study limitations
In the current study, all patients were recruited from specialized stroke units where the best acute stroke services are supposedly offered. So, the results do not reflect the state of services in general hospitals in the participating countries.
References
Ding Q, Liu S, Yao Y, Liu H, Cai T, Han L (2022) Global, regional, and national burden of ischemic stroke, 1990’2019. Neurology 98(3):E279–E290. https://doi.org/10.1212/WNL.0000000000013115
The Lancet Neurology (2019) A spotlight on sex differences in neurological disorders. Lancet Neurol 18(4):319. https://doi.org/10.1016/S1474-4422(19)30001-8
Weber R, Krogias C, Eyding J et al (2019) Age and sex differences in ischemic stroke treatment in a nationwide analysis of 1.11 million hospitalized cases. Stroke 50(12):3494–3502. https://doi.org/10.1161/STROKEAHA.119.026723
Ayala C, Croft JB, Greenlund KJ et al (2002) Sex differences in US mortality rates for stroke and stroke subtypes by race/ethnicity and age, 1995–1998. Stroke 33(5):1197–1201. https://doi.org/10.1161/01.STR.0000015028.52771.D1
Women’s Health (1985) Report of the public health service task force on women’s health issues. Publ Health Rep 100(1):73–106
Jaberinezhad M, Farhoudi M, Nejadghaderi SA et al (2022) The burden of stroke and its attributable risk factors in the Middle East and North Africa region, 1990–2019. Sci Rep 12(1):1–11. https://doi.org/10.1038/s41598-022-06418-x
Nogueira RG, Qureshi MM, Abdalkader M et al (2021) Global impact of COVID-19 on stroke care and IV thrombolysis. Neurology 96(23):e2824–e2838. https://doi.org/10.1212/WNL.0000000000011885
Kremer C, Gdovinova Z, Bejot Y et al (2022) European Stroke Organisation guidelines on stroke in women: management of menopause, pregnancy and postpartum. Eur Stroke J 7(2):I-XIX. https://doi.org/10.1177/23969873221078696
McCullough LD, Alkayed NJ, Traystman RJ, Williams MJ, Hurn PD (2001) Postischemic estrogen reduces hypoperfusion and secondary ischemia after experimental stroke. Stroke 32(3):796–802. https://doi.org/10.1161/01.STR.32.3.796
Murphy SJ, McCullough LD, Smith JM (2004) Stroke in the female: role of biological sex and estrogen. ILAR J 45(2):147–159. https://doi.org/10.1093/ilar.45.2.147
Danesi MA, Okubadejo NU, Ojini FI, Ojo OO (2013) Incidence and 30-day case fatality rate of first-ever stroke in urban Nigeria: the prospective community based Epidemiology of Stroke in Lagos (EPISIL) phase II results. J Neurol Sci 331(1–2):43–47. https://doi.org/10.1016/j.jns.2013.04.026
Appelros P, Stegmayr B, Terént A (2009) Sex differences in stroke epidemiology. Stroke 40(4):1082–1090. https://doi.org/10.1161/strokeaha.108.540781
Farag S, Kenawy FF, Shokri HM et al (2021) The clinical characteristics of patients with pre-existing leukoaraiosis compared to those without leukoaraiosis in acute ischemic stroke. J Stroke Cerebrovasc Dis 30(9):105956. https://doi.org/10.1016/j.jstrokecerebrovasdis.2021.105956
El Nahas NM, Shokri HM, Roushdy TM et al (2019) Urban versus rural Egypt: stroke risk factors and clinical profile: cross-sectional observational study. J Stroke Cerebrovasc Dis 28(11):104316. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.104316
Madsen TE, Khoury JC, Leppert M et al. Temporal trends in stroke incidence over time by sex and age in the GCNKSS. Stroke. Published online 2020:1070–1076. https://doi.org/10.1161/STROKEAHA.120.028910
Rexrode KM, Madsen TE, Yu AYX, Carcel C, Lichtman JH, Miller EC (2022) The impact of sex and gender on stroke. Circ Res 130(4):512–528. https://doi.org/10.1161/CIRCRESAHA.121.319915
Peters SAE, Carcel C, Millett ERC, Woodward M (2020) Sex differences in the association between major risk factors and the risk of stroke in the UK Biobank cohort study. Neurology 95(20):E2715–E2726. https://doi.org/10.1212/WNL.0000000000010982
Peters SAE, Huxley RR, Woodward M (2013) Comparison of the sex-specific associations between systolic blood pressure and the risk of cardiovascular disease: a systematic review and meta-analysis of 124 cohort studies, including 1.2 million individuals. Stroke 44(9):2394–2401. https://doi.org/10.1161/STROKEAHA.113.001624
Madsen TE, Howard G, Kleindorfer DO et al (2019) Sex differences in hypertension and stroke risk in the REGARDS study: a longitudinal cohort study. Hypertension 74(4):749–755. https://doi.org/10.1161/HYPERTENSIONAHA.119.12729
Madsen TE, Howard VJ, Jiménez M et al (2018) Impact of conventional stroke risk factors on stroke in women an update. Stroke 49(3):536–542. https://doi.org/10.1161/STROKEAHA.117.018418
Pirillo A, Casula M, Olmastroni E, Norata GD, Catapano AL (2021) Global epidemiology of dyslipidaemias. Nat Rev Cardiol 18(10):689–700. https://doi.org/10.1038/s41569-021-00541-4
Kapral MK, Fang J, Hill MD et al (2005) Sex differences in stroke care and outcomes: results from the Registry of the Canadian Stroke Network. Stroke 36(4):809–814. https://doi.org/10.1161/01.STR.0000157662.09551.e5
Reeves MJ, Bushnell CD, Howard G et al (2008) Sex differences in stroke: epidemiology, clinical presentation, medical care, and outcomes. Lancet Neurol 7(10):915–926. https://doi.org/10.1016/S1474-4422(08)70193-5
Cai B, De LS, Li H, Liu ZQ, Peng B (2020) Sex differences of acute stroke treatment and in hospital outcomes after intravenous thrombolysis in patients with ischemic stroke. Front Neurol 11(October):1–6. https://doi.org/10.3389/fneur.2020.545860
Bonkhoff AK, Karch A, Weber R, Wellmann J, Berger K (2021) Female stroke: sex differences in acute treatment and early outcomes of acute ischemic stroke. Stroke (February):406–415. https://doi.org/10.1161/STROKEAHA.120.032850
Ospel J, Singh N, Ganesh A, Goyal M (2023) Sex and gender differences in stroke and their practical implications in acute care. J Stroke 25(1):16–25. https://doi.org/10.5853/jos.2022.04077
Phan HT, Blizzard CL, Reeves MJ et al (2017) Sex differences in long-term mortality after stroke in INSTRUCT (INternational STRoke oUtComes sTudy). Circ Cardiovasc Qual Outcomes 10(2):1–10. https://doi.org/10.1161/CIRCOUTCOMES.116.003436
Strong B, Lisabeth LD, Reeves M (2020) Sex differences in IV thrombolysis treatment for acute ischemic stroke: a systematic review and meta-analysis. Neurology 95(1):11–22. https://doi.org/10.1212/WNL.0000000000009733
Heidenreich PA, Trogdon JG, Khavjou OA et al (2011) Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation 123(8):933–944. https://doi.org/10.1161/CIR.0b013e31820a55f5
Smajlović D (2015) Strokes in young adults: epidemiology and prevention. Vasc Health Risk Manag 11:157–164. https://doi.org/10.2147/VHRM.S53203
Si Y, Xiang S, Zhang Y et al (2020) Clinical profile of aetiological and risk factors of young adults with ischemic stroke in West China. Clin Neurol Neurosurg 193(August 2019):105753. https://doi.org/10.1016/j.clineuro.2020.105753
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
Each group of authors from each center receives IRB from their local ethical committee.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
What is already known on this topic
• The burden of stroke is increasing worldwide.
• A poor understanding of sex differences leads to misconceptions and biases in the management of male and female stroke patients.
What this study adds
• Explore sex difference in stroke services in different countries.
How this study might affect research, practice, or policy.
• Improve the quality of stroke services provided to patients.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nahas, N.E., Shokri, H., Roushdy, T. et al. Do stroke services still show sex differences? A multicenter study. Neurol Sci 45, 1097–1108 (2024). https://doi.org/10.1007/s10072-023-07026-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-023-07026-x