
Abstract
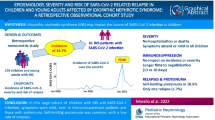
The features of IgA nephropathy (IgAN) after SARS-CoV-2 infection have not been well characterized. In this study, we compared the clinical and pathological characteristics of patients with IgAN who had experienced SARS-CoV-2 infection to those who had not. We conducted a retrospective study that enrolled 38 patients with biopsy-proven IgAN following SARS-CoV-2 infection with 4 months (post-SARS-CoV-2 infection group) and 1154 patients with IgAN prior to the pandemic (pre-SARS-CoV-2 infection group). Among the SARS-CoV-2 group cases, 61% were females. The average duration from SARS-CoV-2 infection to renal biopsy was 78.6 days. Prior to SARS-CoV-2 infection, the patients had different presentations of nephropathy. One patient had isolated hematuria, two had isolated proteinuria, twenty presented with both hematuria and proteinuria, and one patient had elevated serum creatinine. Additionally, there were eight cases with uncertain nephropathy history, and six cases did not have a history of nephropathy. Following SARS-CoV-2 infection, five patients experienced gross hematuria, one case exhibited creatinine elevation, and five cases showed an increase in proteinuria. The group of patients infected with SARS-CoV-2 after the COVID-19 pandemic exhibited older age, higher hypertension ratio and lower eGFR values compared to the pre-SARS-CoV-2 infection group. As for pathological parameters, a higher proportion of patients in the post-SARS-CoV-2 infection group exhibited a higher percentage of sclerotic glomeruli and glomerular ischemic sclerosis. There were no significant differences observed between the two groups in terms of therapy involving steroids, immunosuppressants, or RAS inhibitors. IgA nephropathy patients who were infected with SARS-CoV-2 were generally older and experienced more severe kidney damage compared to those without SARS-CoV-2 infection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The COVID-19 pandemic has had a profound impact on global health, with the emergence of new variants of the SARS-CoV-2 virus posing ongoing challenges. While severe respiratory infections have been the prominent clinical manifestation of COVID-19, it is now evident that the virus can affect other organs beyond the respiratory system [1].
Increasing evidence suggests that SARS-CoV-2 virus can cause kidney damage and gastrointestinal symptoms in infected individuals. Kidney damage, including acute kidney injury and proteinuria, has been observed and has been associated with higher mortality rates in severe cases [2]. To date, several types of glomerular diseases have been identified in association with COVID-19, including collapsing glomerulopathy, lupus nephritis, IgA nephropathy (IgAN), and acute kidney failure [3]. IgAN is a common primary glomerular disease worldwide and has been previously associated with respiratory or intestinal infections [4]. However, it is still unclear whether the manifestation of IgAN is influenced by SARS-CoV-2 infection. The specific impact of SARS-CoV-2 on the development, severity or progression of IgAN is not well understood. Currently, there is limited available information regarding the clinical and pathological characteristics of patients with IgAN who have also contracted SARS-CoV-2. Given the limited number of case reports and studies investigating the relationship between SARS-CoV-2 infection and IgAN, further research is needed to determine any potential association and understand the underlying mechanisms.
The aim of this study was to assess the clinical and pathological characteristics of IgAN patients who with a history of SARS-CoV-2 infection. By conducting this study, the researchers sought to gather information and insights into how the presence of SARS-CoV-2 infection may influence the features of IgAN.
Methods
Study design and population
This retrospective study involved a group of patients with IgAN at Tianjin Medical University General Hospital. A total of 1154 patients diagnosed with IgAN through renal biopsy, which included at least 8 glomeruli in our cohorts between July 2011 and December 2020, were analyzed. Patients with secondary IgAN, such as those with systemic lupus erythematosus and Henoch Schonlein purpura, were excluded from the study. Additionally, patients with IgAN accompanied by minimal change disease, membranous nephropathy or diabetic nephropathy were also excluded (Fig. 1).

Flowchart of the recruitment process
From December 8, 2022, to April 6, 2023, a total of 48 patients were diagnosed IgAN in our hospital. These patients represented approximately 22.5% of the total number of patients who underwent renal biopsies during the specified time frame. Among them, five patients were found to be free of SARS-CoV-2 infection. Additionally, one patient had a concurrent diagnosis of diabetic nephropathy, one patient had a concurrent diagnosis of membranoproliferative glomerulonephritis, and three patients with less than eight glomeruli observed during renal biopsy were excluded from the study (Fig. 1).
This study was approved by the institutional ethics committee of Tianjin Medical University General Hospital, and all patients provided written informed consent.
Clinical data collection
Demographic characteristics and clinical data including age, gender, hypertension ratio, diabetic ratio, systolic blood pressure (SBP), hemoglobin (Hb), erythrocyte sedimentation rate (ESR), blood platelet (PLT), prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen (FIB), D-dimer, serum albumin (Alb), serum globulin (GLO), serum creatinine (Scr), estimated glomerular filtration rate (eGFR), serum uric acid (UA), proteinuria, Complement C3, Complement C4, urinary red blood cell, total cholesterol (TC), triglyceride (TG), low density lipoprotein (LDL), serum immunoglobulin A (IgA) and serum immunoglobuling G (IgG) were collected at the time of renal biopsy.
Definitions
Individuals with a blood pressure of ≥ 140/90 mmHg are considered hypertension [5].
The eGFR was calculated using the Chronic Kidney Epidemiology Collaboration (CKD-EPI) equation, which is a tool commonly used to assess kidney function in patients with CKD [6]. The histological lesions were categorized based on the Oxford classification scores (MEST-C, M: mesangial hypercellularity; E: endocapillary hypercellularity; S: segmental glomerulosclerosis; T: tubular atrophy/interstitial fibrosis, and C: crescent) [7]. The presence of more than 50% crescent in the glomerular cystic cavity was considered a larger crescent.
A renin-angiotensin system inhibitor (RASI) refers to the use of drugs such as angiotensin-converting enzyme inhibitors (ACEIs) and/or angiotensin receptor blockers (ARBs) after a biopsy. Immunosuppressive therapy was defined as treatment with cyclophosphamide, cyclosporine, or mycophenolate mofetil, following a kidney biopsy.
Statistical analysis
Normally distributed continuous variables were compared using Student’s t test and expressed as mean ± standard deviation (SD). Non-normally distributed continuous data were compared using the Mann–Whitney U test and presented as medians and interquartile ranges. Dichotomous data were presented as both numerical values and percentages, and statistical comparison was performed using the χ2 test. The statistical analysis, conducted using SPSS 25.0 software, showed P < 0.05 (two-tailed) was considered significant.
Results
Baseline characteristics of IgAN patients following COVID-19 infection
A total of 38 patients who had contracted COVID-19 were included in this study.
Table 1 provides an overview of the demographic and clinical characteristics of these patients. The mean age of patients in the post-SARS-CoV-2 infection group was 45.89 years and the mean SBP was 135 mmHg. Among the COVID-19 cases included in the study, the majority (61%, n = 23) were female. Regarding the timing of renal biopsy, the mean duration from SARS-CoV-2 infection to the biopsy procedure was 78.6 days. Prior to SARS-CoV-2 infection, the patients had different presentations of nephropathy. One patient had isolated hematuria, two had isolated proteinuria, twenty presented with both hematuria and proteinuria, and one patient had elevated serum creatinine. Additionally, there were eight cases with uncertain nephropathy history, and six cases did not have a history of nephropathy. Following COVID-19 infection, five patients experienced gross hematuria, one case exhibited creatinine elevation, and five cases showed an increase in proteinuria (Table 1).
Clinical and pathological characteristics of IgAN patients in the post-COVID-19 and pre-COVID-19 infection groups
We compared the clinical and pathological characteristics of IgAN patients who had contracted COVID-19 to those who had not. As shown in Table 2, the group of patients infected with SARS-CoV-2 after the COVID-19 pandemic exhibited older age (45.89 ± 14.98 vs. 38.17 ± 12.53 years, P < 0.001), higher hypertension ratio (65.8% vs. 41.9%, P = 0.03) and lower eGFR values (77.36 ± 25.2 ml/min vs. 92.58 ± 31.31 ml/min, P = 0.03) than those in the pre-SARS-CoV-2 infection group. Although there was no statistically significant difference in the incidence of diabetes between the two groups, the post-SARS-CoV-2 infection group had a higher prevalence of diabetes (13.2% vs. 5.7%, P = 0.057). Based on the pathological parameters, the post-SARS-CoV-2 infection group showed a higher proportion of sclerotic glomeruli [13.2% (14.94%, 57.54%) vs. 11.54% (0.0, 28%), P < 0.001] and glomerular ischemic sclerosis [18.61% (6.67%, 31.41%) vs. 5.26% (0.0, 14.29%), P < 0.001] compared to the pre-SARS-CoV-2 infection group. Though there was no statistically significant difference in the tubular atrophy/interstitial fibrosis (T1/2), the post-COVID-19 infection group had a higher proportion of T1/2 lesions (73.7% vs. 60.6%, P = 0.057) compared to the pre-SARS-CoV-2 infection group (Table 3). There was no significant difference in gender, SBP, ESR, PLT, PT, APTT, FIB, D-Dimer, ALB, GLO, urinary protein, serum creatinine, uric acid, urinary red blood cell count, IgA, IgG, complement C3, C4, TC, TG, LDL between the two groups (Table 2). There were no differences observed between the two groups in terms of other pathological parameters, including the percentage of M1, E1, S1, C1/C2, sclerotic glomeruli, glomerular globally sclerotic, glomerular segmental sclerosis, crescents, large crescents, and fibrinoid necrosis (Table 3). No significant differences were observed between the two groups in terms of therapy involving steroids, immunosuppressants, or RAS inhibitors (Table 3).
Discussion
The COVID-19 pandemic, caused by SARS-CoV-2, has had a significant impact on the global economy and public health [8]. Apart from the expected pulmonary involvement in SARS-CoV-2, other organ impacts have also been reported, including kidney involvement in patients with COVID-19 [9, 10]. SARS-CoV-2 infection may lead to various types of kidney damage [11, 12]. Although IgAN has been reported in association with SARS-CoV-2, these reports are limited to individual cases [13, 14]. To the best of our knowledge, this is the first study to compare clinical and pathological characteristics of IgAN between post-SARS-CoV-2 infection group and pre-SARS-CoV-2 infection group.
Starting from December 7, 2022, the relaxation of control measures in China, including the lifting of regional mass testing restrictions and the implementation of home isolation or quarantine, contributed to an unprecedented surge of the Omicron variant. As a result, there was a significant increase in the prevalence rate of COVID-19 [15]. A total of 48 patients were diagnosed IgAN from December 8, 2022 to April 6, 2023 in our hospital. These patients constituted approximately 22.5% of the total patients who underwent renal biopsy during that time. We analyzed the incidence rate of IgAN during the same time period before the COVID-19 outbreak and it ranged between 21.2 and 38.0% in recent three years in our center. Ten patients were excluded from the study due to their ineligibility for inclusion. Among the 38 patients who contracted SARS-CoV-2, 24 had a documented history of nephropathy, 8 had an uncertain nephropathy history, and 6 did not have any prior history of nephropathy before being infected with COVID-19. After SARS-CoV-2 infection, 13.2% of the patients (5/38) presented with gross hematuria. It is well known that many viral and bacterial pathogens have the ability to trigger gross-hematuria and increased proteinuria. Therefore, we can conclude that, as expected, COVID-19 share with other pathogens the ability to exacerbate the clinical features of IgAN. In recent years, there have been several reports of patients with preexisting or newly diagnosed IgAN who are susceptible to gross hematuria after receiving the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccine [16]. We also observed that 13.2% of the patients (5/38) experienced an increase in proteinuria after contracting SARS-CoV-2. These findings suggest that SARS-CoV-2 infection may lead to gross hematuria or an exacerbation of proteinuria in a subset of patients with IgAN. It is important to monitor and assess proteinuria levels in individuals with IgAN who have been infected with SARS-CoV-2 to ensure appropriate management and treatment of kidney-related complications.
It is not yet clear whether the occurrence of COVID-19 affects the presentation of the IgAN. One case reports have described five cases of IgAN with gross hematuria that were confirmed by biopsy after SARS-CoV-2 infection [14]. In one case among the reported cases, the individual experienced gross hematuria within two days after the onset of fever. The hematuria lasted for a duration ranging from 1 to 6 days. Additionally, it is worth noting that during the episode of gross hematuria, one patient developed acute kidney injury (AKI). In our study, we found that the cohort of patients infected with SARS-CoV-2 exhibited advanced age, a higher prevalence of hypertension and lower levels of eGFR compared to those in the pre-SARS-CoV-2 infection group. Although there was no statistically significant difference in diabetes incidence between the two groups, the post-COVID-19 infection group had a higher prevalence of diabetes. As for pathological characters, the post-COVID-19 infection group exhibited a higher proportion of sclerotic glomeruli and glomerular ischemic sclerosis compared to the pre-COVID-19 infection group. Even though there was no statistically significant difference in the tubular atrophy/interstitial fibrosis (T1/2), the post-COVID-19 infection group had a higher proportion of T1/2 lesions. This finding suggested the older age in patients with SARS-Cov-2 is consistent with the evidence in the literature and alone can explain the clinical and histological characteristics found in the cohort of patients with covid-19 infection. Indeed, multiple studies have consistently reported the elderly population is known to be more vulnerable to severe illness and complications associated with COVID-19 [13]. Advanced age is recognized as a significant risk factor for developing severe symptoms, experiencing higher rates of hospitalization, requiring intensive care, and facing an increased risk of mortality from COVID-19. Regular monitoring of renal function and appropriate medical care are crucial for identifying and managing any declines in eGFR or related renal complications in elderly individuals who contract COVID-19. As for treatment decision, we found the treatment approach remained consistent regardless of the presence of COVID-19.
So far, the pathogenic mechanism underlying COVID-19-associated kidney damage remains incompletely understood. It has been suggested that elevated levels of a circulating form of abnormal glycosylation (Gd-IgA1) may contribute to the pathogenesis of IgAN [17, 18]. COVID-19 virus primarily affects the respiratory tract, leading to the stimulation of excessive production of IgA1, including Gd-IgA1 [16]. Gd-IgA1 has the potential to recognize specific structures on certain microorganisms and form circulating complexes with them, thereby facilitating antigenic recognition. Previous studies have demonstrated that potential underlying mechanisms of kidney involvement in COVID-19 may include direct kidney infection through ACE-2 receptors expressed in tubular cells and podocytes [19]. Additionally, an indirect mechanism may involve cytokine release syndrome observed in COVID-19 patients [20]. The cytokines released during COVID-19 infection, including IL-1, IL-6, and TNF, have the potential to stimulate the proliferation and maturation of IgA1-producing B cells, thereby contributing to the development and severity of IgAN [21, 22]. In this study, we found no evidence of an increased incidence rate of IgAN during COVID-19 infection. However, we did observe that SARS-CoV-2 infection might be associated with severe kidney damage in these patients. The high prevalence of glomerular sclerosis among our post-COVID-19 infection group suggests a chronic disease trajectory in this population. While a higher proportion of T1/2 lesions suggests that COVID-19 infection may induce tubulointerstitial lesions in the kidney in IgAN, further research is needed to establish a clear causal relationship between COVID-19 and tubulointerstitial damage in this context. In this study, we observed that while Covid-19 infection can exacerbate IgAN, it does not contribute to an increased incidence of IgAN. This suggests that the virus is not a causal factor in the development of the disease.
The present study has several limitations that should be acknowledged. Firstly, it was a retrospective cohort study, which may introduce inherent biases and limit the generalizability of the findings. The small sample sizes in the post-COVID-19 infection group further impact the statistical power and reliability of the results. Secondly, the underlying mechanisms linking COVID-19 infection and the onset as well as clinical manifestations of IgAN remain unclear, and further research is warranted to elucidate these mechanisms.
Conclusion
IgA nephropathy patients who were infected with SARS-CoV-2 were generally older and experienced more severe kidney damage compared to those without SARS-CoV-2 infection. This indicates that the presence of the virus may exacerbate the underlying glomerular disease, leading to more pronounced renal abnormalities, particularly in elderly patients. Further research is necessary to better understand the mechanisms underlying the relationship between SARS-CoV-2 infection and IgAN.
Availability of data and materials
Raw data used during the current study are available from the corresponding author on reasonable request for non-commercial use.
References
Suso AS, Mon C, Oñate Alonso I et al. IgA vasculitis with nephritis (Henoch-Schönlein Purpura) in a COVID-19 patient. Kidney international reports, Kidney Int Rep, 2020;5(11).
Cheng Y, Luo R, Wang K, et al. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020;97(5):829–38.
Shimmel A, Shaikhouni S, Mariani L. Current understanding of clinical manifestations of COVID-19 in glomerular disease. Glomerular Dis. 2021;1(4):250–64.
Ma Y, Xu G. New-onset IgA nephropathy following COVID-19 vaccination. QJM Int J Med 2023;116(1):26–39.
Zhang X, Shi S, Ouyang Y et al., A validation study of crescents in predicting ESRD in patients with IgA nephropathy.J Transl Med, 2018;16(1).
Wang J, Xie P, Huang JM, et al. The new Asian modified CKD-EPI equation leads to more accurate GFR estimation in Chinese patients with CKD. Int Urol Nephrol. 2016;48(12):2077–81.
Trimarchi H, Barratt J, Cattran DC, et al. Oxford classification of IgA nephropathy 2016: an update from the IgA nephropathy classification working group. Kidney Int. 2017;91(5):1014–21.
Maeda K, Higashi-Kuwata N, Kinoshita N, et al. Neutralization of SARS-CoV-2 with IgG from COVID-19-convalescent plasma. Sci Rep. 2021;11(1):5563.
Walsh EE, Frenck RW Jr, Falsey AR, et al. Safety and immunogenicity of two RNA-based covid-19 vaccine candidates. N Engl J Med. 2020;383(25):2439–50.
Pérez A, Torregrosa I, D’Marco L, et al. IgA-Dominant infection-associated glomerulonephritis following SARS-CoV-2 infection. Viruses. 2021;13(4):587.
Dadson P, Tetteh CD, Rebelos E, et al. Underlying kidney diseases and complications for COVID-19: a review. Front Med. 2020;7: 600144.
Becker RC. COVID-19-associated vasculitis and vasculopathy. J Thromb Thrombolysis. 2020;50(3):499–511.
Huang Y, Li XJ, Li YQ et al. Clinical and pathological findings of SARS-CoV-2 infection and concurrent IgA nephropathy: a case report. BMC Nephrol 2020;21(1).
Ueda H, Okabe M, Shimizu A et al., Gross Hematuria following SARS-CoV-2 infection in IgA nephropathy: a report of 5 cases. Kidney Med 2023;5(6).
Bai Y, Shao Z, Zhang X, et al. Reproduction number of SARS-CoV-2 Omicron variants, China, December 2022–January 2023. J Travel Med 2023;taad049.
Farooq H, Aemaz Ur Rehman M, Asmar A, et al. The pathogenesis of COVID-19-induced IgA nephropathy and IgA vasculitis: a systematic review. J Taibah Univ Med Sci 2022;17(1): 1–13.
My W, Cs C, Gt Y et al., The emerging role of pathogenesis of IgA nephropathy. J Clin Med 2018;7(8).
Tanaka M, Seki G, Someya T, et al. Aberrantly glycosylated IgA1 as a factor in the pathogenesis of IgA nephropathy. Clin Dev Immunol. 2011;2011: 470803.
Varga Z, Flammer AJ, Steiger P, et al. Endothelial cell infection and endotheliitis in COVID-19[J]. Lancet (London, England). 2020;395(10234):1417–8.
Soleimani M. Acute kidney injury in SARS-CoV-2 infection: direct effect of virus on kidney proximal tubule cells. Int J Mol Sc. 2020;21:3275.
van den Wall BAW, Daha MR, Haaijman JJ, et al. Elevated production of polymeric and monomeric IgA1 by the bone marrow in IgA nephropathy[J]. Kidney Int. 1989;35(6):1400–4.
Sugino H, Sawada Y, Nakamura M. IgA vasculitis: etiology, treatment, biomarkers and epigenetic changes. Int J Mol Sci. 2021;22(14):7538.
Acknowledgements
The authors thank all the study subjects for their participation.
Funding
This study is supported by Tianjin Health Science and Technology Project (TJWJ2022MS005), Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-071C), Kidney Medical development research Fund (SO.20220718TJ), and the National Key Research and Development Program of China (2019YFF0216502).
Author information
Authors and Affiliations
Contributions
HL, ZL, ZW, FW and YX collected samples. HL and ZW prepared data. HL and ZL analyzed the data. HL drafted the manuscript. YL and JJ revised the manuscript. YL and TY conceived the overall study. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethics approval and consent to participate
All subjects provided written informed consents. The study protocol was approved by the Institutional Ethical Committee of Tianjin medical university general hospital.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, H., Li, Z., Wu, Z. et al. Clinical and pathological findings of IgA nephropathy following SARS-CoV-2 infection. Clin Exp Med 24, 43 (2024). https://doi.org/10.1007/s10238-023-01271-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10238-023-01271-2