
Summary
Introduction
Non-specific low back pain (NLBP) is a common and clinically significant condition with substantial socioeconomic implications. Whole-body vibration therapy (WBVT) has shown effectiveness in improving pain and sensorimotor function (e.g., in osteoporosis) in previous studies. However, studies had heterogeneous settings. The aim of this study was to assess the effects of WBVT on pain, function, proprioception, and postural stability in patients with subacute and chronic NLBP.
Methods
A systematic literature search was conducted in the scientific databases PubMed, EMBASE, and PEDro (from inception until 17.05.2023). Only prospective controlled and uncontrolled studies were included. Outcome measures assessed were pain intensity, function (activities of daily living and physical function), proprioception, and postural stability.
Results
A total of 12 original articles (n = 821) were included in the analysis. Ten of the studies were randomized controlled trials, one study had a crossover design, and one study had a one-group pre–post study design. The studies compared WBVT vs. no intervention, WBVT vs. basic physical therapy, WBVT vs. core stabilization exercises with and without respiratory resistance, WBVT vs. lumbar extension exercises, and WBVT vs. whole body electromyostimulation training. The treatment approaches varied in terms of duration (2–18 weeks), frequency (2–3 times per week, two applications with a 2-week break), vibration frequency (5–30 Hz), type of exercises (WBVT with or without static or dynamic exercises), and vibration direction (horizontal and vertical). Significant pain reduction was observed in all 10 studies that investigated pain levels. Significant improvement in daily activity function was reported in five of the six studies that investigated daily function, while improvement in physical function was observed in all four studies that investigated physical function. Improvement in proprioception was reported in all three studies that investigated proprioception, and significant improvement in postural stability was observed in four out of six studies that investigated postural stability. No adverse events or side effects related to WBVT were reported.
Conclusion
The majority of the included studies demonstrated significant pain reduction, improvement in physical and daily functioning, and enhanced proprioception. Improvement in postural stability was less consistent. WBVT appears to be a safe and effective treatment modality for subacute and chronic NLBP when used within a multimodal approach. Future research should focus on standardized settings including assessment methods, treatment regimens, frequencies, and intensities.
Zusammenfassung
Hintergrund
Der primäre unspezifische untere Rückenschmerz (NLBP) ist eine häufig auftretende und klinisch bedeutende Erkrankung mit erheblichen sozioökonomischen Auswirkungen. Die Ganzkörper-Vibrationstherapie (WBVT) hat sich bei unterschiedlichen Indikationen zur Verbesserung von Schmerz und Sensomotorik (z. B. Osteoporose) in bis dato sehr heterogenen Studiensettings als wirksam erwiesen. Das Ziel dieser Studie war es, die Auswirkungen der WBVT auf Schmerz, Funktion, Propriozeption und posturale Stabilität bei Patienten mit subakutem und chronischem unspezifischem unterem Rückenschmerz zu bewerten.
Methoden
Es wurde eine systematische Literatursuche in den wissenschaftlichen Datenbanken PubMed, EMBASE und PEDro (von Gründung bis 17.05.2023) durchgeführt. Es wurden nur prospektive kontrollierte und unkontrollierte Studien eingeschlossen. Zielparameter waren Schmerzintensität, Funktion, Propriozeption und posturale Stabilität.
Ergebnisse
In die Analyse wurden insgesamt 12 Originalarbeiten (n = 821) eingeschlossen. Davon waren 10 randomisierte kontrollierte Studien, eine Cross-over-Studie und eine Prä-post-Studie ohne Kontrollgruppe. In den Studien erfolgte der Vergleich von WBVT vs. keine Maßnahme, WBVT vs. Bewegungstherapie mit allgemeinen körperlichen Übungen, WBVT vs. rumpfstabilisierende Übungen mit und ohne Atemwegswiderstand, WBVT vs. lumbale Extensionsübungen und WBVT vs. Ganzkörper-Elektromyostimulation. Die Behandlungsansätze variierten in Bezug auf die Dauer (2–18 Wochen), Häufigkeit (2- bis 3‑mal/Woche, 2 Anwendungen mit einer 2‑wöchigen Pause), Vibrationsfrequenz (5–30 Hz), Art der Übungen (WBVT mit oder ohne statische oder dynamische Übungen), und Vibrationsrichtung (horizontal und vertikal). In allen 10 Studien, die die Schmerzintensität untersuchten, wurde eine signifikante Schmerzreduktion festgestellt. In 5 von 6 Studien, die die tägliche Funktion untersuchten, wurde über eine signifikante Verbesserung der täglichen Aktivitäten berichtet, während in allen 4 Studien, die die körperliche Funktion untersuchten, eine signifikante Verbesserung festgestellt wurde. In allen 3 Studien, die die Propriozeption untersuchten, wurde über eine signifikante Verbesserung berichtet. In 4 von 6 Studien, die die posturale Stabilität untersuchten, wurde eine Verbesserung festgestellt. Es wurden keine Nebenwirkungen oder unerwünschten Ereignisse im Zusammenhang mit der WBVT berichtet.
Schlussfolgerung
Die Mehrheit der eingeschlossenen Studien ergab eine signifikante Schmerzreduktion, Verbesserung der körperlichen Funktion sowie eine verbesserte Propriozeption. Die Verbesserung der posturalen Stabilität war weniger konsistent. Daher scheint die Ganzkörper-Vibrationstherapie in Verbindung mit einem multimodalen Ansatz eine sichere und wirksame Behandlung zu sein.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The lifetime prevalence of low back pain (LBP) is estimated to reach up to 84% and the prevalence of chronic low back pain (CLBP) is approximately 23%, with a notable 11–12% of the population experiencing disability due to LBP [3]. After an initial episode of LBP, 44–78% of individuals experience recurrence of pain and 26–37% experience a recurrence of work disability [3].
Non-specific low back pain (NLPB) is a prevalent musculoskeletal condition that has emerged as a significant global public health concern. NLBP does not have a known anatomical, pathological, or neurological origin, and it is typically diagnosed when other potential causes have been ruled out. It is characterized by pain that typically emanates from the lowest rib and extends to the gluteal fold, with the possibility of radiating somatic referred pain into the thigh, extending above the knee [1].
The majority of episodes of NLBP are not associated with significant underlying pathology [2]. However, approximately 10–15% of patients with acute NLBP progress to develop CLPB [2].
Chronic pain, particularly in the context of the healthcare system, poses significant challenges. The chronic condition typically does not improve and consumes a substantial amount of resources [3].
There are numerous potential non-pharmacological therapies for NLBP. Whole-body vibration therapy (WBVT) is usually used for treatment of various musculoskeletal disorders like osteoporosis, osteoarthritis, fibromyalgia, and NLBP [4,5,6,7]. The therapeutic effect of WBVT is explained through the tonic vibration reflex [8]. Vibration stimulates the extrafusal muscle fibers, which in turn elicits a stretch reflex of the muscles, representing a general stimulus [9]. This stimulus induced by WBVT is used as a therapeutic effect. The general stimulus of the tonic vibration reflex at 20 Hz during WBVT can lead to relaxation of existing muscle cramps [9]. Additionally, the stretch reflex can also strengthen weak core muscles in this regard [9]. This set of muscles comprises the collection of core muscles encircling the spine and abdominal organs which extend from the diaphragm to the pelvic floor muscles. These muscles collaborate harmoniously to furnish stability to the spinal region [10]. Using an oscillating platform, dynamic and static exercises can be performed in standing, sitting, and lying positions. Different frequencies and amplitudes (0–45 Hz, 0–12 mm) can be adjusted accordingly [11].
A systematic review by Wang et al. (2020) concluded that there is limited evidence suggesting that WBVT is beneficial for NLBP when compared with other forms [7]. However, there is still a lack of standardized protocols for assessments and interventions, as well as a limited number of systematic reviews conducted in the last few years.
Therefore, our study aims to address this gap by summarizing the existing evidence and evaluating the efficacy of WBVT for NLBP. The hypothesis is that therapeutic WBVT is an effective intervention for individuals with NLBP.
Methods
Identification and selection of studies
A systematic review was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [12].
The search was conducted in the electronic databases PubMed, EMBASE, and PEDro. Studies using the keywords “back pain” or “low back pain” and “whole body vibration” or “WBV” were extracted and considered for inclusion in the study. No filters were applied. The systematic literature search and the assessment of bias risk was independently performed by two researchers, and discrepancies in study selection were resolved through discussion. The search results were screened based on title and abstract. The eligible articles underwent a full-text analysis. Inclusion criteria for the present systematic review comprised studies conducted within primary care settings, specifically emphasizing randomized controlled trials, as guided by the PICOS (population, intervention, comparison, outcomes, and study design) framework [13, 14]. Crossover studies and pre–post studies were also considered for a better review of physiotherapeutic interventions.
Inclusion and exclusion criteria
Inclusion criteria for the studies were men and women of all ages with subacute and chronic NLBP for at least 6 weeks. Studies were considered suitable for this systematic review if at least one intervention group received WBVT therapy for a minimum duration of 2 weeks with a frequency ranging from one to three sessions per week.
Any quantitative study type of primary and peer-reviewed research that included WBVT as an intervention for NLBP was considered for inclusion. The inclusion criteria were as follows:
-
Participants: patients of all ages with NLBP for at least 6 weeks;
-
Intervention: WBVT therapy for a minimum duration of 2 weeks;
-
Control groups: no WBVT, basic physical therapy, no control group;
-
Outcomes: effects on pain, activities of daily living and physical activity, lumbar proprioception, and postural stability;
-
Study design: prospective, controlled, and uncontrolled studies, crossover design;
-
Language limitations: published in English or German.
Retrospective trials, case reports, reviews, letters, editorials, commentaries, and conference papers were excluded.
Studies examining patients with work-related vibration, such as truck drivers, were excluded. Likewise, studies analyzing subjects without LBP who received WBVT therapy were excluded.
Data collection and analysis
The following data were collected: author, publication year, country, study design, sample size, dropout rate, and authors’ conclusions. Patient characteristics included mean age and gender. Intervention characteristics encompassed the use of the vibration device, settings such as hertz and amplitude, type of exercises (static or dynamic) on the vibration device, treatment duration, and follow-up period. We also recorded the treatment provided to the control group. The primary outcome measures of this review were pain assessed using the visual analog scale (VAS) and the numerical rating scale (NRS), the Roland Morris Disability Scale (RMQ), and the Oswestry Disability Index (ODI). Secondary outcomes examined included lumbar proprioception and postural stability.
The outcome data were reported as median value with standard deviation. The significance level between study groups and the significance level in the study group before and after therapy were indicated using the p-value. A few studies provided the effect size according to Cohen and a between-group difference with a 95% confidence interval.
The assessment of bias risk for randomized studies was conducted using the PEDro criterion.
Results
Literature search
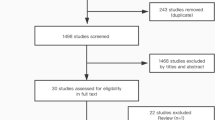
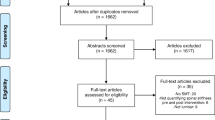
A total of 309 studies published until May 17, 2023 were identified and screened for eligibility based on their titles and abstracts as depicted in Fig. 1. After removing duplicates, 254 studies were rejected as non-eligible; 21 studies were selected for full-text analysis and 12 studies met the inclusion criteria [15,16,17,18,19,20,21,22,23,24,25,26]. Among these, there were 10 randomized controlled trials [15, 16, 18,19,20,21,22,23,24, 26], one crossover study [25], and one single-group pre- and post-test design [17].

Identification of studies
The risk of bias analysis is summarized in Table 1. The PEDro scale ranged from 4–9 points, showing that the articles were of fair to good methodological quality. Nine studies demonstrated good quality, while two studies had fair quality (Table 1).
The included studies were heterogeneous, both in terms of treatment protocols and in terms of outcome parameters. Pooling of data for meta-analysis was not possible. Therefore, we were limited to describing the included studies.
Study characteristics
The key characteristics of the studies are summarized in Table 2.
Participants
A total of 821 study participants were included. The average age of the subjects ranged from 21.6 to 61.6 years. Among them, 658 participants had CLBP, 48 participants had subacute LBP, 65 participants had chronic back pain (CBP), and 50 participants had no back pain. 21 participants with CBP dropped out before receiving vibration therapy, and all 50 patients with no back pain did not receive any intervention.
Intervention
Of the 381 participants receiving WBVT, 317 received WBVT as a standalone therapy [15,16,17,18,19, 22,23,24,25], 20 participants received WBVT in combination with lumbar stabilization training with biofeedback [21], 16 participants with subacute LBP received WBVT with respiratory resistance therapy and stabilizing exercises (SERW) [26], and 28 participants received WBVT along with home exercises [20].
The implementation of WBVT differed among the studies. Some studies only included dynamic exercises [16, 19], while others combined dynamic and static movement exercises [15, 23]. On the other hand, some studies focused on holding static postural exercises in various positions [20, 22, 26], or only adopted a basic position with slight knee flexion [17, 18, 21, 24, 25].
The control groups received different treatment approaches like no treatment [17], basic physical exercises [15, 23], trunk-stabilizing exercises with [21] and without biofeedback [16], trunk-stabilizing exercises along with home exercises [20], exercises solely at home [20], stabilizing exercises with respiratory resistance (SER) and without respiratory resistance (SE) [26], whole-body electromyostimulation (WB EMS) therapy with trunk-specific exercises [23], and isodynamic lumbar extension exercises [19].
Not all studies compared WBVT with non-WBVT. One crossover study compared low-frequency WBVT (LF) at 30 Hz with high-frequency WBVT (HF) at 50 Hz [25]. Another study investigated differences between horizontal and vertical WBVT [23]. A one-group pre-test and post-test study examined the impact of WBVT in a single group [22].
Different vibration platforms were utilized: BodyGreen® [B.Green Technology Co., Ltd., Xiushui Township, Changhua County, Taiwan (R.O.C.)], [15, 22]. Galileo® [16,17,18,19, 21], Power Plate® [20, 25], Wellengang platform® [23], and sW–VH11 platform® [26].
Different frequencies of WBVT were applied in the included studies. Two studies had increasing frequencies over the course of the study, ranging from 5 to 20 Hz [16] and from 10 to 30 Hz [17]. Frequencies of 9 Hz [15, 22], 10 Hz [23], 18 Hz [19, 21], 20 Hz [18], 25 Hz [20], and 30 Hz [26] were examined.
Different studies with varying treatment durations were included in this review, ranging from 2 weeks to 18 weeks.
Three studies examined follow-up periods after completion of therapy, with durations of 6 months [19], 3 months [20], and 1 month [24].
Outcome
Primary evaluated outcomes: pain intensity, impact on activities of daily living and physical function
The primary outcomes in this systematic review involve evaluation of the effects of WBVT, with a focus on examining the changes in pain intensity and functional impairment. Overall, ten out of the 12 studies assessed pain intensity before and after the intervention using the visual analog scale (VAS), the numeric rating scale (NRS), or the categorical quantitative VAS (QVAS) [15, 18,19,20,21,22,23,24,25,26]. The impact of back pain on activities of daily living was assessed using the Oswestry Disability Index (ODI) in six studies [15,16,17,18, 21, 24]. To assess physical function impairment due to back pain, four out of the 12 studies investigated the Roland Morris Disability Score (RMQ; Table 3).
Secondarily evaluated outcomes: trunk proprioception, postural stability
Three studies included in this review examined trunk proprioception, investigating joint position sense in flexion and extension using the Con-Trex Multi Joint system® [15, 22]. The repositioning error at 0%, 30%, and 60% of the maximum range of motion using an electrogoniometer for both low-frequency (LF) and high-frequency (HF) vibration therapy was examined [25].
Five out of the 12 studies investigated postural stability. [16,17,18, 21, 24]. One study used the MFT S3 Checks that determine the stability index (STI), sensorimotor index (SMI), and symmetry index (SI) in both standing and sitting positions [16]. Another study measured the fall index (FI) over time using posturography (Tetrax®) [21]. One study examined postural control using the Leonardo Mechanograph®, assessing standard deviations in the anterior–posterior and medio–lateral directions [17]. Two studies also investigated postural stability using the anterior–posterior stability index (PSTAntPost/AP) and medial–lateral stability index (PSTMedLat/ML) with the Biodex balance system™ [18, 24]. One study measured static balance ability using a Wii and calculated the center of pressure (CoP), velocity, length, and area ([26]; Table 4).
Primary outcome: effect of WBVT on pain intensity
In the study by Pozo-Cruz et al. [18], a significant improvement in VAS scores was observed between the intervention group receiving WBVT and the control group receiving no therapy.
Similarly, Wang et al. [15] found a significant improvement in VAS scores between the intervention group receiving WBVT and the control group receiving general exercises. A significant improvement in the global perceived effect of change on the VAS was also analyzed between the groups [15].
Yang et al. [21] showed a significant improvement in VAS scores both between and within the groups. The intervention group received WBVT, while the control group received exercises for lumbar stability.
Karacay et al. [20] revealed a significant improvement in VAS scores both between and within the groups. The intervention group received WBVT, control group 1 received core stabilization exercises (CSG), and control group 2 (CG) received home exercises.
The study by Park et al. [26] also demonstrated a significant reduction in QVAS scores in all three groups (SERW, SER; SE). The SERW and SER groups showed a significant difference in QVAS improvement compared to the SE group.
Rittweger et al. [19] showed a significant reduction in VAS scores within both the intervention and control groups, but no significant difference was found between the intervention and control groups. The intervention group received WBVT, while the control group received lumbar extension exercises.
Micke et al. [23] observed a significant decrease in VAS scores in all groups (WBV, EMS, circuit training) before and after therapy, but there was no significant difference in pain reduction between the three groups.
Zheng et al. [22] observed a significant improvement during therapy in the single group using WBV.
Two studies compared different WBVT settings [24, 25]. In the study by Kim et al. [24], a significant improvement in VAS scores was found after both horizontal and vertical vibrations, but no significant difference was observed between the two groups.
The same result was observed in the crossover study by Sajadi et al. [25], where a significant improvement was seen within both low-frequency (LF) and high-frequency (HF) WBVT groups, but no significant difference was found between the groups.
Primary outcome: effect of WBVT on activities of daily living
A significant improvement in daily activity measured with the ODI was observed between the intervention group and control group in the studies by Kaeding et al. [17] and Pozo-Cruz et al. [18]. The intervention group received WBV, while the control group did not receive any treatment. Similarly, Wang et al. [15] reported a significant improvement in ODI scores in the intervention group compared to the control group, which received general exercises. A significant improvement in the global perceived effect of change on the ODI was also found between the groups.
However, Yang et al. [21] did not observe a significant improvement in ODI scores between the groups. Both the control group, which performed exercises for lumbar stability, and the intervention group with WBVT showed a significant improvement in the follow-up assessment.
Furthermore, a significant improvement was observed after WBVT with horizontal and vertical vibration in the study by Kim et al. [24]. However, no significant difference was found between the two groups.
In the study by Wegener et al. [16], no significant improvement in activities of daily living was observed in either the intervention group with WBVT or the control group with exercises using TheraBand® or weights.
Primary outcome: effect of WBVT on physical function
A significant improvement in physical function, as measured by the RMQ, was observed between the intervention and control groups in the studies by Pozo-Cruz et al. [18] and Kaeding et al. [17], where WBVT was compared to no therapy.
Similarly, in the comparison among the three groups in the study by Park et al. [26], both SERW and SER demonstrated a significant increase, surpassing the SE group.
In the study by Karacay et al. [20], significant improvement was observed in the groups receiving WBVT and core stabilization exercises with the therapists establishing and controlling the neutral position of the pelvis, but not in the group performing only home exercises. A significant improvement in RMQ scores between the groups was not determined.
Secondary outcome: effect of WBV on trunk proprioception
In the study by Wang et al. [15], the intervention group exhibited additional positive outcomes in terms of lumbar flexion joint position sense and lumbar extension joint position sense compared to the control group. Both groups received a general physical training program, with WBVT (intervention group) and without WBVT (control group).
Similarly, in the study by Zheng et al. [22], a significant reduction in lumbar flexion and extension angle deviation was observed following WBV.
In the study by Sajadi et al. [25], a significant improvement in reposition error (RE) was found in the low-frequency (LF) group at 0° lumbar flexion, 30° lumbar flexion, and 60° lumbar flexion, while in the high-frequency (HF) group, a significant improvement was observed only at 0° lumbar flexion. A significant difference between the two groups was observed only at 0° [25]. Based on the findings, it was observed that the variation in lumbar flexion RE was influenced by the frequency of WBVT rather than the angle of flexion [25]. The low-frequency WBV, as implemented in the proposed protocol, resulted in greater improvement in RE [25].
Secondary outcome: effect of WBVT on postural stability
Wegener et al. [16] examined postural stability using the MFT-S3 Check in patients with no back pain and NCBP before the intervention. Only patients with NCBP received an intervention, after which the MFT S3 Check was repeated. There was no difference in postural stability between the no back pain and NCBP groups in sitting or in standing positions before the intervention. After therapy, the control group, which performed trunk stability exercises using TheraBand® and weights, showed a significant improvement in the stability index (STI) in both standing and sitting positions, as well as in the sensorimotor index (SMI) in the standing position. The WBVT group did not show a significant improvement in postural stability, and there was also no significant difference between the groups.
The assessment of postural control in the study of Kaeding et al. [17], comparing participants in the intervention group receiving WBVT and participants without therapy, showed no significant difference between the groups before the WBVT therapy and even 3 months after its completion.
The fall index (FI) in the study by Yang et al. [21] showed a significant improvement in the vibration group compared to the group performing only lumbar stability exercises.
In the study by Pozo-Cruz et al. [18], a significant improvement in postural stability was observed in the intervention group receiving WBVT compared to the control group without therapy, as measured by the PSTAntPost.
Both groups in the crossover study by Kim et al. [24] showed a significant improvement in standing balance control scores with both horizontal and vertical vibration. However, there was no significant difference between the groups.
In the study by Park et al. [26] a significant improvement in balance ability was observed in the SERW group, while the SER and SE groups did not show a significant improvement.
Discussion
Whole-body vibration therapy is a measure which is frequently used in the clinical setting. It seems to have several advantages for both patients as well as physicians. For example, it offers effective exercises that require minimal space and do not necessitate additional equipment. Additionally, the incidence of adverse events associated with WBVT therapy is rare, as none of the 12 examined studies reported any such occurrences. Moreover, this approach is not only beneficial for individuals who are unable to participate in traditional exercise therapy due to musculoskeletal constraints, but also for those who experience fears or anxieties related to conventional exercise therapy.
The term “kinesiophobia” is frequently encountered in the literature when discussing patients suffering from CLBP [27]. These patients avoid physical activity due to fear of experiencing painful movements or reinjury. They assume a position of avoidance and endure their pain through physical inactivity [24, 28].
However, literature has demonstrated that regular physical activity is superior to no treatment or usual care in managing CLBP [29].
Patients with CLBP experience significant limitations in their daily functioning and physical activity due to the persistent and ongoing pain, which affects their abilities in both professional and personal life [30]. An improvement in these limitations during the course of therapy may be attributed to a mere reduction in pain [19]. Effective pain reduction is the crucial initial step in the treatment of CLBP patients, leading to subsequent positive outcomes.
The findings from the present systematic review reveal an improvement in the pain condition among patients who underwent WBVT [15, 18,19,20,21,22,23,24,25,26]. Five out of the 10 studies demonstrated a significant superiority of the WBVT compared to the control group. Additionally, five studies showed a significant improvement in pain symptoms within the intervention group during the observation period.
The improvement in pain status and positive response to physical activity resulting from WBVT can lead to a reduction in kinesiophobia [27]. This is reflected in the results of our systematic review. Three out of the six studies demonstrated a significant improvement in pain symptoms between the intervention and the control group [15, 17, 18]. Two of the six studies showed a significant improvement within the intervention group during the observation period [20, 23].
Likewise, there was an improvement in physical function after WBVT. One study showed a significant improvement within the intervention group [20]. A significant improvement between the groups was detected in three of the four studies that examined physical function [17, 18, 20, 26].
The pathology of CLBP is difficult to understand due to its complex heterogeneity. Peripheral causes of CLBP can involve degeneration of the bony and ligamentous, fibrous, and muscular components of the lumbar spine. Nociceptors contained within these components can be sensitized through inflammatory processes, lowering their threshold for activation. Additionally, these processes can trigger pathological nerve growth, resulting in neuropathic pain [31]. However, central mechanisms are also described. This involves an alteration in the processing of stimuli in the brain, particularly with faulty descending pain pathways [31]. Structural differences in the musculature have also been identified in CLBP. Atrophy of the multifidus muscles and an abnormality in the fiber type of the paraspinal muscles have been reported in CLBP [32].
It is hypothesized that CLBP patients exhibit divergences in trunk muscle activity and kinematics, and the spinal stability may either be increased or decreased in this patient population [33]. A “tight control” can lead to high spinal loading with sustained spinal activity, while “loose control” can result in increased tensile loading [33]. Tailored treatments should be directed at these phenotypes based on the condition of spinal stability [33]. Our review investigates the impact of WBVT on proprioception and postural stability in patients with subacute and CLBP, taking into account the altered spinal kinematics observed in these individuals.
Two of the two studies that examined proprioception showed significant improvement in proprioception in patients with CLBP [15, 22].
It was observed that a low frequency of 30 Hz resulted in a more significant improvement in proprioception compared to a high frequency of 50 Hz [25].
The results regarding the effects of WBVT on postural stability in patients with subacute and CLBP are inconclusive in this systematic review. In three studies WBVT showed significant improvements compared to the control group [15, 18, 23], and one study showed significant improvements within the intervention group [21]. Nevertheless, there are two references that showed no significant improvement after WBVT [16, 17].
Overall, the results support the efficacy of WBVT in patients with subacute and CLBP with a particular focus on pain reduction and improvement in physical and daily activity. The contradictory results regarding postural control/stability reinforce the hypothesis that patients with CBP may exhibit either “tight control” or “loose control” of the spine, requiring specific therapies based on their condition. Further studies should classify patients into different groups based on the underlying etiology to determine significant differences in the effectiveness of WBV.
Of the 12 studies, one specifically focused on patients with subacute NLBP [26]. The results of these patients were found to be comparable to those of patients with CLBP. These findings suggest that WBVT may be beneficial even in the subacute phase of low back pain. Consequently, it can be inferred that WBVT has the potential to be applied early in the management of subacute NLBP.
Interestingly, many publications in the literature address work-related WBVT in relation to LBP. LBP particularly occurs during seated activities such as driving in vehicles [34,35,36].
A systematic review of Burström et al. [37] establishes a link between occupational vibration and LBP, identifying a spinal resonance frequency for the seated operator between 4 and 8 Hz.
However, the reason why WBVT is still offered as a treatment for LBP despite this association is a crucial difference in the duration and the therapeutic framework of the applied vibration [7].
In this systematic review, evidence suggests that WBVT represents a promising approach with potential benefits for the management of subacute and CLBP. It is essential to acknowledge the multifactorial nature of back pain etiology, thus requiring a multimodal treatment approach. Certain psychological factors such as fear-avoidance beliefs, self-efficacy, pain-coping mechanisms, catastrophizing tendencies, and even the presence of depressed mood have been shown to be important predictors of a person’s disability status [38]. Consequently, WBVT should be considered as a complementary therapy in clinical practice. Additionally, it is crucial to incorporate psychoeducation alongside therapeutic interventions.
There are several limitations to this systematic review. The comparability of the studies is restricted due to variations in study protocols, such as observation periods, frequency, and administration of WBVT. In future studies, it will be necessary to improve the methodological quality through minimizing the methodological limitations (for example, missing control group, low sampling rate, or no standardized clinical outcome). Furthermore, more high-quality studies are urgently needed to find the best WBVT for subacute and CLBP.
Conclusion
Therapeutic whole-body vibration appears to be a viable and secure treatment modality for individuals experiencing subacute and CLBP. The use of WBVT as an adjunctive component within a multimodal treatment framework for subacute and CLBP, with an emphasis on pain reduction and enhancement of activities of daily living and physical functions, as well as improvements in postural stability and proprioception, has demonstrated beneficial effects. However, further investigation is necessary, with standardized assessments and interventions to explore optimal protocols, long-term effects, and the potential mechanisms underlying the observed positive outcomes associated with WBVT.
References
Walker BF. The prevalence of low back pain: a systematic review of the literature from 1966 to 1998. J Spinal Disord. 2000;13:205–17.
Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389:736–47.
Krismer M, van Tulder M. Strategies for prevention and management of musculoskeletal conditions. Low back pain (non-specific). Best Pract Res Clin Rheumatol. 2007;21:77–91.
Bouchard C. Prevention of falls, prevention of osteoporosis, or both: what is the best strategy for preventing fractures in older women? Menopause.20(10):995–6. https://doi.org/10.1097/GME.0b013e3182a49d90.
Salmon JR, Roper JA, Tillman MD. Does acute whole-body vibration training improve the physical performance of people with knee osteoarthritis? J Strength Cond Res. 2012;26:2983–9.
Collado-Mateo D, Adsuar JC, Olivares PR, Del Pozo-Cruz B, Parraca JA, Del Pozo-Cruz J, et al. Effects of whole-body vibration therapy in patients with Fibromyalgia: a systematic literature review. Evid Based Complement Alternat Med. 2015;2015:719082.
Wang W, Wang S, Lin W, Li X, Andersen LL, Wang Y. Efficacy of whole body vibration therapy on pain and functional ability in people with non-specific low back pain: a systematic review. BMC Complement Med Ther. 2020;20:158.
Zaidell LN, Mileva KN, Sumners DP, Bowtell JL. Experimental evidence of the tonic vibration reflex during whole-body vibration of the loaded and unloaded leg. Plos One. 2013;8:e85247.
Rittweger J, Mutschelknauss M, Felsenberg D. Acute changes in neuromuscular excitability after exhaustive whole body vibration exercise as compared to exhaustion by squatting exercise. Clin Physiol Funct Imaging. 2003;23:81–6.
Akuthota V, Ferreiro A, Moore T, Fredericson M. Core stability exercise principles. Curr Sports Med Rep. 2008;7:39–44.
Wheeler AA, Jacobson BH. Effect of whole-body vibration on delayed onset muscular soreness, flexibility, and power. J Strength Cond Res. 2013;27:2527–32.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Eriksen MB, Frandsen TF. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J Med Libr Assoc. 2018;106:420–31.
Amir-Behghadami M, Janati A. Population, Intervention, Comparison, Outcomes and Study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg Med J Engl. 2020;p:387.
Wang X‑Q, Gu W, Chen B‑L, Wang X, Hu H‑Y, Zheng Y‑L, et al. Effects of whole-body vibration exercise for non-specific chronic low back pain: an assessor-blind, randomized controlled trial. Clin Rehabil. 2019;33:1445–57.
Wegener V, Rarack S, Tiffe T, Grill E, Melcher C, Birkenmaier C, et al. Effects of whole body vibration therapy and classic physiotherapy on postural stability in people with back pain: a randomized trial. Clin Spine Surg. 2019;32:E214–E20.
Kaeding TS, Karch A, Schwarz R, Flor T, Wittke T‑C, Kück M, et al. Whole-body vibration training as a workplace-based sports activity for employees with chronic low-back pain. Scand J Med Sci Sports. 2017;27:2027–39.
del Pozo-Cruz B, Hernández Mocholí MA, Adsuar JC, Parraca JA, Muro I, Gusi N. Effects of whole body vibration therapy on main outcome measures for chronic non-specific low back pain: a single-blind randomized controlled trial. J Rehabil Med. 2011;43:689–94.
Rittweger J, Just K, Kautzsch K, Reeg P, Felsenberg D. Treatment of chronic lower back pain with lumbar extension and whole-body vibration exercise: a randomized controlled trial. Spine (Phila Pa 1976). 2002;27:1829–34.
Karacay CB, Sahbaz T, Gurtekin B, Yildiz S, Ozcan E. Effectiveness of whole-body vibration exercise and core stabilization exercise in chronic non-specific low back pain: a randomized-controlled study. Turkish J Phys Med Rehabil. 2022;68:184–94.
Yang J, Seo D. The effects of whole body vibration on static balance, spinal curvature, pain, and disability of patients with low back pain. J Phys Ther Sci. 2015;27:805–8.
Zheng Y‑L, Wang X‑F, Chen B‑L, Gu W, Wang X, Xu B, et al. Effect of 12-Week Whole-Body Vibration Exercise on Lumbopelvic Proprioception and Pain Control in Young Adults with Nonspecific Low Back Pain. Med Sci Monit Int Med J Exp Clin Res. 2019;25:443–52.
Micke F, Weissenfels A, Wirtz N, von Stengel S, Dörmann U, Kohl M, et al. Similar pain intensity reductions and trunk strength improvements following whole-body electromyostimulation vs. whole-body vibration vs. conventional back-strengthening training in chronic non-specific low back pain patients: a three-armed randomized control trial. Front Physiol. 2021;12:664991.
Kim H, Kwon BS, Park J‑W, Lee H, Nam K, Park T, et al. Effect of whole body horizontal vibration exercise in chronic low back pain patients: vertical versus horizontal vibration exercise. Ann Rehabil Med. 2018;42:804–13.
Sajadi N, Bagheri R, Amiri A, Maroufi N, Shadmehr A, Pourahmadi M. Effects of different frequencies of whole body vibration on repositioning error in patients with chronic low back pain in different angles of lumbar flexion. J Manipulative Physiol Ther. 2019;42:227–36.
Park S‑H, Oh Y‑J, Seo J‑H, Lee M‑M. Effect of stabilization exercise combined with respiratory resistance and whole body vibration on patients with lumbar instability: A randomized controlled trial. Medicine (Baltimore). 2022;101:e31843.
Ishak NA, Zahari Z, Justine M. Kinesiophobia, pain, muscle functions, and functional performances among older persons with low back pain. Pain Res Treat. 2017;2017:3489617.
Clauw DJ, Williams D, Lauerman W, Dahlman M, Aslami A, Nachemson AL, et al. Pain sensitivity as a correlate of clinical status in individuals with chronic low back pain. Spine (Phila Pa 1976). 1999;24:2035–41.
Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Exercise therapy for chronic low back pain. Cochrane Database Syst Rev. 2021;9:CD9790.
McGorry RW, Webster BS, Snook SH, Hsiang SM. The relation between pain intensity, disability, and the episodic nature of chronic and recurrent low back pain. Spine (Phila Pa 1976). 2000;25:834–41.
Li W, Gong Y, Liu J, Guo Y, Tang H, Qin S, et al. Peripheral and central pathological mechanisms of chronic low back pain: a narrative review. J Pain Res. 2021;14:1483–94.
Goubert D, Van Oosterwijck J, Meeus M, Danneels L. Structural changes of lumbar muscles in non-specific low back pain: a systematic review. Pain Physician. 2016;19:E985–1000.
van Dieën JH, Reeves NP, Kawchuk G, van Dillen LR, Hodges PW. Motor control changes in low back pain: divergence in presentations and mechanisms. J Orthop Sports Phys Ther. 2019;49:370–9.
Bovenzi M, Schust M, Mauro M. An overview of low back pain and occupational exposures to whole-body vibration and mechanical shocks. Med Lav. 2017;108:419–33.
Barrero LH, Cifuentes M, Rodríguez AC, Rey-Becerra E, Johnson PW, Marin LS, et al. Whole-body vibration and back pain-related work absence among heavy equipment vehicle mining operators. Occup Environ Med. 2019;76:554–9.
Tiemessen IJH, Hulshof CTJ, Frings-Dresen MHW. Low back pain in drivers exposed to whole body vibration: analysis of a dose-response pattern. Occup Environ Med. 2008;65:667–75.
Burström L, Nilsson T, Wahlström J. Whole-body vibration and the risk of low back pain and sciatica: a systematic review and meta-analysis. Int Arch Occup Environ Health. 2015;88:403–18.
Puri BK, Theodoratou M. The efficacy of psychoeducation in managing low back pain: A systematic review. Psychiatrike. 2022;34(3):231–42. https://doi.org/10.22365/jpsych.2022.104.
Funding
Open access funding provided by Medical University of Vienna.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
F. Remer, M. Keilani, P. Kull and R. Crevenna declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Remer, F., Keilani, M., Kull, P. et al. Effects of whole-body vibration therapy on pain, functionality, postural stability, and proprioception in patients with subacute and chronic non-specific low back pain: a systematic review. Wien Med Wochenschr (2023). https://doi.org/10.1007/s10354-023-01026-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10354-023-01026-4