
Abstract
Aim
Resiliency and satisfaction with life are identified as factors related to health behavior in the general population. However, little is known about health behavior and its predictors in public nursing home residents. The purpose of the study was to establish the nature of the relationship between resiliency, satisfaction with life, and health behavior in institutionalized older adults in Poland.
Subject and methods
A cross-sectional study with purposive sampling was performed in public nursing homes in Poland. A total of 161 male and female senior residents aged 60 to 99 (Mean = 76.65, SD = 9.23) were examined. Mediation analysis was performed with the Hayes’ PROCESS macro.
Results
This study revealed that resiliency, satisfaction with life, and health behavior are positively associated with each other in older persons. Satisfaction with life plays a mediating role in the relationship between resiliency and health behavior in residents of long-term care institutions.
Conclusion
Our findings underscore the important role played by personal resources in strengthening interventions and supporting the efforts of nursing home residents to engage in health behavior.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Health behavior is the activity that people undertake for the purpose of maintaining or enhancing their health, body image, and preventing health problems (Cockerham 2014). In old age is an important determinant of health outcomes and long life — a way of preventing chronic diseases, maintaining body performance, slowing the progression of functional curtailments, and improving the general quality of life (Hrobonova et al. 2011; Selivanova and Cramm 2014; Swindell et al. 2010). The period of late adulthood can, therefore, be experienced as ‘healthy aging’ for which health-related behavior is necessary (Peel et al. 2005).
However, little is known about the specificity and determinants of health-related behavior in long-term care institutions. The existing studies usually focus on a specific behavior in this group, particularly on physical activity (Resnick and Boltz 2016; Chad et al. 2005; Csapo et al. 2009; Salguero et al. 2011). Many studies, however, examine various physical and mental health aspects (Dobrzyn-Matusiak et al. 2014; Harris and Castle 2019) and quality of life in institutionalized older people (Appelhof et al. 2017; Borowiak and Kostka 2004), indirectly indicating the importance of proper health-related behavior.
According to McCabe et al. (1997), health-related behavior in long-term care facilities may include making healthy food choices, engaging in physical activity, seeking information about health and treatment, practicing relaxation and positive attitudes to life, and keeping emotionally supportive relationships. A typical day in nursing homes has many unscheduled hours for residents to undertake many types of health-favorable activities. Unfortunately, only a few studies have examined health behavior in nursing home settings in such a complex way (Kim et al. 2006; McCabe et al. 2005; Zadworna-Cieślak 2019). There are also some studies from Poland focused on the comparison between institutionalized and non-institutionalized older adults. Their results indicate that the general level of health-promoting behavior was lower in institutional participants (Cybulski et al. 2015), and quality of life generally decreased, with a growing level of dependence and institutionalization (Kostka, and Jachimowicz 2010).
Nevertheless, the increasing number of nursing homes can facilitate strengthening older residents’ quality of life and a healthy lifestyle (Chisholm et al. 2018). Research examining the topic of nursing home residents’ health behavior is therefore extremely important for practice.
Health-related behavior is determined by various factors, notably by psychosocial ones (Gochman 2013; Ogińska-Bulik et al. 2015; Palank 1991; Zadworna-Cieślak and Ogińska-Bulik 2018). Personal resources seem to be particularly important among them. One of the psychosocial resource, referred to as a ‘meta-resource’, is resiliency. It represents the personality characteristics allowing individuals to effectively cope with stress, promoting flexibility, persistent adaptation, tolerance of failures, motivation, and remedial action in difficult situations. People characterized by a high level of resilience are more positively adapted to life; they have higher self-esteem and self-efficacy (Ogińska-Bulik and Juczyński 2008). Nevertheless, it must be noted that while resiliency refers to a trait of personality or a relatively permanent individual resource, resilience is defined as the process of successfully overcoming negative life events (Richardson 2002). There is ample empirical evidence attesting to the importance of both resilience and resiliency for optimal human functioning in the late-life period (Holmes et al. 2018; MacLeod et al. 2016; Resnick et al. 2018). Resiliency has been found to be a determinant of late-life satisfaction and physical health (Beutel, et al. 2010; Fullen et al. 2018; Zadworna-Cieślak and Ogińska-Bulik 2019), as well as perceived life quality, reduced anxiety, and reduced depression in older adults (Gerino et al. 2017). However, studies focused on the relationship between resiliency and health-related behavior in older adults are still scarce (Ogińska-Bulik et al. 2015; Perna et al. 2012).
Looking for the mechanisms of the impact of resiliency on health behavior and health outcomes, one might refer to Fredrikson’s (2001) broaden-and-build theory of positive emotions. The theory highlights the significance of positive emotions for well-being, both physical and psychological. As resiliency is associated with the occurrence of positive emotions, it can strengthen health and well-being. One of the possible ways to better health outcomes is health-promoting behavior. Therefore, resiliency, well-being, and health behavior seem to be associated.
Subjective well-being can be described as the level at which individuals evaluate or appraise their own lives. Such evaluations can either manifest themselves as cognitive reflections, representing reflective appraisals of life, or as affective feelings. Life satisfaction can be considered to be the cognitive component of this broader construct, and can be defined as the process of making a global cognitive assessment of one’s past life (Diener et al. 1985; Diener et al. 2018; Pavot and Diener 2009). People satisfied with their life often practice healthier behavior; this mediational pathway may be a major reason for their better state of health and longevity (Diener et al. 2017). However, only a few studies to date have been focused on older adults, especially institutionalized ones. Their findings indicate that well-being and life satisfaction predict physical activity level, more preventive behavior, as well as lower rates of obesity, smoking, and heavy alcohol drinking in older nursing home residents (Kim et al. 2016; Kim et al. 2014; Strine et al. 2008).
In recent years, substantial scientific evidence has linked positive emotional health to lower cardiovascular morbidity and mortality independently of negative emotions. Some potential mechanisms have been assumed to explain these relationships, including enhanced health behavior, direct physiological effects, and enhanced resistance to stress in persons with high versus low positive emotional resources (Davis 2009). However, the positive adaptation abilities of older adults can be compromised by institutionalization (Callegari et al. 2016). The role of resiliency and life satisfaction in the functioning of people’s health has not been fully understood. There is also no research answering the question about the significance of the above-mentioned factors for seniors’ health behavior in the nursing home setting.
Thus, the aim of the present study was to determine whether satisfaction with life acts as a mediator in the relationship between the resiliency and health-related behavior of residents of long-term care institutions. The study was exploratory, with no directional hypotheses formulated; however, the following research questions were proposed:
-
Is the level of health-related behavior associated with sociodemographic factors (age, sex, education, as well as marital, parental, and financial status)?
-
What is the nature of the relationship between the variables (resiliency, satisfaction with life, health-related behavior)?
-
Does satisfaction with life act as a mediator in the relationship between resiliency and health-related behavior?
Method
Study design
A cross-sectional design with purposive sampling was chosen for the study, which involved male and female residents of five public nursing homes in central Poland. The functioning roles of these homes and the types of services they provide are regulated by the Social Welfare Act of 12 March 2004 (consolidated text Polish Official Journal of 2019 text 1508). Therefore, they can be considered to be representative of all public nursing homes in Poland.
Inclusion/exclusion criteria
The main inclusion criteria were as follows: being a nursing home resident, age over 60, and proper intellectual functions that enabled the understanding of the instruction and measure items. The exclusion criterion was dementia and serious mental disabilities, as well as a lack of informed consent. Each resident who met the eligibility criteria was asked to complete a set of self-assessment questionnaires (paper versions).
Ethical consideration
The research procedure was performed in accordance with the Helsinki Declaration of Human Rights (World Medical Association/WMA 2013). The study protocol was approved by the Research Ethics Board at the University of Lodz. We obtained consent from the head of each institution where the study was to be conducted. The participants were informed that the results of the study would only be used for scientific purposes, that participation was anonymous and completely voluntary, and that they could withdraw at any time without penalty.
Procedure
The psychologists employed in the institutions helped us recruit respondents for the study sample. In the case of those residents who may have had limited sight or who were at an advanced age, a research team member decided about the need for individual support in completing tests, such as providing additional explanations or reading questions. According to Isaksson et al. (2007), this type of individual help can help to obtain reliable data when working with elderly respondents.
Data collection
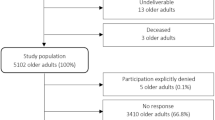
The data was collected between November 2017 and September 2018. Initially, a total of 237 residents living in five public nursing homes were considered for participation in the study: of these, 47 were rejected at the recruitment stage due to failure to meet the inclusion criteria. Of the remaining 190 volunteers who met the inclusion criteria, 29 withdrew from participation when the study was already in progress. Finally, the results from 161 residents who met the eligibility criteria and returned completed sets of questionnaires were included in the analyses. The overall response rate was 68%.
Measures
Sociodemographic characteristics
Sociodemographic characteristics were assessed by means of a questionnaire developed for the purpose of the current study, which collected information about the participants’ sex, age, education level, marital status, having children, and subjectively perceived financial status.
Health behavior (outcome variable)
Health behavior was assessed using the Health-Related Behavior Questionnaire for Seniors (Kwestionariusz Zachowań Zdrowotnych dla Seniorów, KZZ-S; Zadworna-Cieślak 2017). The KZZ-S measures the health behaviors of older people (above 60 years old). It consists of 24 items, and yields the overall health behavior score as well as separate scores for five behavioral categories. There are: (1) positive attitude towards life, (2) behavior associated with physical health, (3) attention to mental health, (4) behavior related to prevention and treatment, and (5) environmental behavior. Answers are given on a 5-point Likert scale (ranging from 1 = false about me to 5 = true about me). A higher score indicates a higher level of behavior beneficial to health. The psychometric properties of KZZ-S are satisfactory (Cronbach’s α was .87 for the whole test, and ranged from .63 to .79 for its subscales). In the current sample, Cronbach’s alpha for the total score was .89.
Resiliency
Resiliency was assessed by means of the Resiliency Measurement Scale (Skala Pomiaru Prężności, SPP-25; Ogińska-Bulik and Juczyński 2008). The tool measures the overall level of resiliency, understood as a personal trait, and its five components: (1) determination and persistence in action, (2) openness to new experiences and sense of humor, (3) competencies to cope and tolerance of negative affect, (4) tolerance of failures and treating life as a challenge, and (5) optimistic life attitude and ability to mobilize in difficult situations. Cronbach’s alpha coefficient for the overall score was .89 in the validation study (Ogińska-Bulik and Juczyński 2008). In the present sample, the respective Cronbach’s alpha coefficients for the five abovementioned components were .79, .77, .76, .71, and .81, with the value for the overall score being .94.
Satisfaction with life
Participants’ well-being was measured by means of the Satisfaction With Life Scale (SWLS) (Diener et al. 1985). The scale consists of five items (e.g., “I am satisfied with my life”) rated on a Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). The higher the score, the higher the satisfaction with life. The SWLS has been shown to have good test–retest reliability (.82); its criterion and construct validity have been established across various populations (Diener et al. 1985; Pavot and Diener 2009; Sin and Lyubomirsky 2009). Cronbach’s α reliability coefficient for the Polish version of the SLWS was α = 0.81 (Juczyński 2012). Internal consistency was strong for the sample in the current study (α = .82).
Data analysis
We analyzed the data using SPSS, version 25. Descriptive statistics were used to introduce demographic characteristics. We used the independent t-test and one-way ANOVA with post hoc tests for multiple comparisons to determine the differences in outcome variable (health-related behavior) scores between groups divided according to demographic and health status criteria. Pearson’s correlation coefficient (r) served us to assess the relationship between resiliency, satisfaction with life, and health-related behavior. We used the PROCESS macro for SPSS to perform the mediation analysis (Hayes 2013). We tested the mediating role of satisfaction with life (mediator) in the relationship between resiliency (predictor; independent variable) and health-related behavior (dependent variable), using the bootstrapping method proposed by Hayes (2013), by drawing 5000 bootstrap samples. The mediation analyses allowed us to construct a more complex model structure. Mediating effects occur when the mediating variable decreases the predictive power of the independent variable for the dependent variable. To perform a power analysis for the mediation model, we applied MedPower (Kenny 2017). The power of the paths (sample N = 161) is satisfactory and ranges from .94 to .95. In order to determine the sample size for mediation analysis, a power analysis was conducted using G*Power (Faul et al. 2014). With a medium effect size (f2) of .15 (alpha of .05, a standard power level of .80, two predictors), a minimum sample size of 107 participants was required (Cohen 1992). The statistical significance level was set at p < .05. The research database is available in open repository (Zadworna et al. 2020).
Results
The mean age in the study sample was 76.65 (SD = 9.23). Most of the respondents were women (n = 103, 64%). The majority of the participants had high school education (n = 63, 37.1%), were widowers (n = 82, 50.9%), had children (n = 94, 58.4%), and assessed their current financial status as an average (n = 83, 51.6%). The demographic characteristics of the study sample, including the differences between the groups in terms of KZZ-S score, are presented in Table 1.
Three variables differentiated groups according to the general level of health-related behavior. Women had significantly higher KZZ-S scores than men: t(159) = −2.574, p < .05, with an average effect size (d = −0.40). Divorced participants (F(3, 156) = 5.808, p < .01, ηp2 = .11) and those with the lowest income (F(2, 157) = 3.248, p < .05, ηp2 = .04) had the lowest KZZ-S scores as well, but the effects size in the case of the latter was very low.
We performed Pearson’s correlation analysis to determine the relations between the variables (Table 2). The strongest relationship was found between the overall level of resiliency and satisfaction with life. The relationship is positive, indicating that a higher level of resiliency is accompanied by higher life satisfaction (r = .56; p < .01). Of the resiliency factors, the one for which we obtained the highest correlation coefficient with life satisfaction was Openness to new experiences and sense of humor (r = .53; p < .01). Satisfaction with life was also associated with a tendency to engage in health behavior (overall score and all factors). With regard to health behavior dimensions, the strongest correlation with satisfaction with life was observed in the case of Positive attitude towards life (r = .56; p < .01), which is the behavioral element associated with strengthening emotional health. Similarly, the total scores on resiliency and its factors were positively correlated with scores on health behavior. The highest correlation was observed between resiliency (and its component factors) and the health behavior factor named Positive attitude towards life (r = .54; p < .01). Determination and persistence in action—a factor of resiliency—was the most strongly correlated with general health behavior scores (r = .47; p < .01).
In order to determine the more complex relationship between health behavior, resiliency, and life satisfaction, we performed a mediation analysis, with the total KZZ-S score as the dependent variable (DV) and satisfaction with life as the mediator (M). Prior to testing the mediating effect of satisfaction with life in the relationship between resiliency and general health behavior, we carried out a regression analysis for the direct effect of resiliency and life satisfaction on health behavior.
The analysis revealed a significant direct effect between resiliency and general health behavior (βc = 0.47, SE = 0.07, t = 6.66, p < .001) as well as between resiliency and satisfaction with life (βa = 0.56, SE = 0.03, t = 8.55, p > .001) and between satisfaction with life and general health behavior (βb = 0.29, SE = 0.20, t = 3.59, p > .001) (see: Fig. 1). After the introduction of life satisfaction as a mediator, the strength of the relationship decreased but remained significant (βc’ = 0.30, SE = 0.08, t = 3.70, p > .001), which indicates partial mediation (R2 = 0.28, F = 30.27, p < .001; Z = 3.33, p < .001). The results indicate that people characterized by high resiliency were more likely to be satisfied with their life, which in turn led to higher levels of health behavior.

Model of relationships between resiliency, satisfaction with life, and health-related behavior in the study sample (N = 161)
Discussion
The present study focused on three research questions. The first of these concerned the links between general health behavior and certain sociodemographic characteristics in institutionalized older adults. The general level of health behavior in the sample was differentiated by gender, marital status, and financial status, although the differences were small. Other studies confirm that elderly women demonstrate a slightly higher level of health-promoting behavior than elderly men (Selivanova and Cramm 2014; Zadworna-Cieślak 2017, 2019). Admittedly, some studies conducted in nursing homes have yielded different results, but the analyzed behaviors and methods were different (Chen et al. 2015; Şenol et al. 2015).
Other studies have yielded similarly ambiguous results with regard to marital and financial status. The significance of sociodemographic factors for health behavior and their level seem to differ depending on the group of older people (institutionalized or non-institutionalized) and the type of the analyzed behavior (Kim et al. 2016; McCabe et al. 2005; Zadworna-Cieślak 2017, 2019).
The second research question concerned the nature of the relationship between the analyzed variables. Many studies have confirmed that resiliency and subjective well-being are associated (Beutel et al. 2010; Liu et al. 2012; Mayordomo et al. 2016), also—or especially—in the late-life period (Resnick et al. 2018). While this resource, as well as satisfaction with life, is linked to various aspects of positive functioning, they are both also related to health behavior (Kim et al. 2014; Perna et al. 2012; Strine et al. 2008).
Finally, the last question concerned the mediating effect of satisfaction with life in the relationship between general resiliency and health behavior. In compliance with the broaden-and-build theory (Fredrickson 2001), positive emotions support well-being. Resiliency promotes adaptation to life challenges, strengthens coping with stress, and aids tolerance of negative events and emotions. These characteristics undoubtedly contribute to the taking-up, maintenance, and modification of health behaviors. Because partial mediation was established, our findings can serve as an initial explanation of a possible mechanism whereby personality factors are favorably related to health behaviors and, presumably, state of health; in other words, personal factors may foster positive emotions and life satisfaction.
Although various types of health behavior seem to have different determinants (McCabe et al. 2005), our findings indicate that the significance of the above-mentioned factors is largest for emotional health-promoting behavior—Positive attitude towards life. Thus, building resiliency should be an important element of health promotion interventions, that focus on resources rather than deficits and risk factors (Perna et al. 2012). Institutionalization does not exclude life satisfaction (Cybulski et al. 2015). Senior citizens are capable of high resilience and wellbeing despite the difficult life challenges related to advanced age and deteriorating health. High resiliency has also been correlated with positive outcomes, such as successful aging, lower depression and longevity (MacLeod et al. 2016). One of the possible ways to achieve those outcomes may be health-promoting behavior.
The key challenge seems to be to determine how to support and/or encourage health behavior in older residents. Many studies indicate the effectiveness of interventions and prevention programs focused on institutionalized adults, improving their life satisfaction and health behavior, thus decreasing the level of cardiovascular risk factors and the risk of depression (Justine and Hamid 2012; Kim et al. 2003).
Limitations
Several limitations of the present study must be highlighted. Firstly, our research was conducted in Poland. Although there is a culture specificity of nursing home settings, caution should be taken when generalizing our results to other populations. The living conditions, facilities, and daily routines in institutions may impact the opportunities to undertake health-related behavior. The participants in our sample probably exhibited higher-than-average cognitive functioning, which means the generalization of its findings must be limited.
Secondly, the smaller number of male participants precludes analyses based on sex subgroups. In a future study kind of analysis, it could provide interesting results on how men and women differ in terms of general health behavior.
Another limitation is that even though we hypothesized causal relationships in the path model, the cross-sectional nature of the study precludes drawing causal conclusions. Only longitudinal data could determine the direction of these relationships adequately.
The final limitation is that we tested only satisfaction with life as a mediating factor between resiliency and health behavior. It must be assumed, however, that there are other important factors affecting the relationship between these variables. For example, we did not control for the health assessment, which can significantly change the nature of the analyzed relationships (Brudek et al. 2017).
Conclusions
Despite some limitations, the study is one of the first attempts to describe the health behavior in institutionalized older people in Poland. It provides encouragement to develop new ways of thinking about life in long-term care institutions. Our findings underscore the important role played by personal resources in strengthening interventions and supporting the efforts of nursing home residents to engage in health behavior. Nursing homes should change from a medically focused model to one that supports residents’ functional ability, health-promoting behavior, and quality of life. Approaches and strategies found to effectively promote health behaviors in other settings could be adapted for nursing homes. The staff of the nursing home have an opportunity to build on each resident’s personal resources and support seniors to maintain or strengthen various spheres of health.
References
Appelhof B, Bakker C, Van Duinen-van den Ijssel JCL, Zwijsen SA, Smalbrugge M, Verhey FRJ et al (2017) The determinants of quality of life of nursing home residents with young-onset dementia and the differences between dementia subtypes. Dement Geriatr Cogn Disord 43(5–6):320–329. https://doi.org/10.1159/000477087
Beutel ME, Glaesmer H, Wiltink J, Marian H, Brähler E (2010) Life satisfaction, anxiety, depression and resilience across the life span of men. Aging Male 13(1):32–39. https://doi.org/10.3109/13685530903296698
Borowiak E, Kostka T (2004) Predictors of quality of life in older people living at home and in institutions. Aging Clin Exp Res 16(3):212–220. https://doi.org/10.1007/bf03327386
Brudek P, Krok D, Telka E (2017) The health assessment and the dimensions of positive mental functioning among elderly people. In: Carlson C (ed) Mental health services: assessment and perspectives. Nova Science Publishers, New York, pp 25–48
Callegari C, Bertù L, Caselli I, Isella C, Ielmini M, Bonalumi C et al (2016) Resilience in older adults: influence of the admission in nursing home and psychopathology. Neuropsychiatry 6(4):117–123. https://doi.org/10.21767/NPY.1000129
Chad KE, Reeder BA, Harrison EL, Ashworth NL, Sheppard SM, Schultz SL et al (2005) Profile of physical activity levels in community-dwelling older adults. Med Sci Sports Exerc 37(10):1774–1784. https://doi.org/10.1249/01.mss.0000181303.51937
Chen Y-M, Li Y-P, Yen M-L (2015) Predictors of regular exercise among older residents of long-term care institutions. Int J Nurs Pract 22(3):239–246. https://doi.org/10.1111/ijn.12401
Chisholm L, Zhang NJ, Hyer K, Pradhan R, Unruh L, Lin F-C (2018) Culture change in nursing homes: what is the role of nursing home resources? Inquiry J Health Car 55:0046958018787043. https://doi.org/10.1177/0046958018787043
Cockerham WC (2014) Health behavior. In: Cockerham WC, Dingwall R, Quah SR (eds) The Wiley Blackwell Encyclopedia of health, illness, behavior, and society, 1st edn. John Wiley & Sons, Ltd., New York, pp 764–766. https://doi.org/10.1002/9781118410868.wbehibs296
Cohen J (1992) A power primer. Psychol Bull 112(1):155–159. https://doi.org/10.1037/0033-2909.112.1.155
Csapo R, Gormasz C, Baron R (2009) Functional performance in community-dwelling and institutionalized elderly women. Wien Klin Wochenschr 121(11–12):383–390. https://doi.org/10.1007/s00508-009-1151-5
Cybulski M, Krajewska-Kulak E, Jamiolkowski J (2015) Preferred health behaviors and quality of life of the elderly people in Poland. Clin Interv Aging 10:1555. https://doi.org/10.2147/CIA.S92650
Davis MC (2009) Building emotional resilience to promote health. Am J Lifestyle Med 3(1 Suppl.):60S–63S. https://doi.org/10.1177/1559827609335152
Diener E, Emmons RA, Larsen RJ, Griffin S (1985) The Satisfaction with Life Scale. J Pers Assess 49(1):71–75. https://doi.org/10.1207/s15327752jpa4901_13
Diener E, Pressman SD, Hunter J, Delgadillo-Chase D (2017) If, why, and when subjective well-being influences health, and future needed research. Appl Psychol Health Well Being 9(2):133–167. https://doi.org/10.1111/aphw.12090
Diener E, Oishi S, Tay L (2018) Advances in subjective well-being research. Nat Hum Behav 2(4):253–260. https://doi.org/10.1038/s41562-018-0307-6
Dobrzyn-Matusiak D, Marcisz C, Bąk E, Kulik H, Marcisz E (2014) Physical and mental health aspects of elderly in social care in Poland. Clin Interv Aging 9:1793. https://doi.org/10.2147/CIA
Faul F, Erdfelder E, Buchner A, Lang A-G (2008) G*power version 3.1.2 [computer software]. Universität Kiel, Germany. http://www.psycho.uni-duesseldorf.de/abteilungen/aap/gpower3/download-and-register. Accessed 2 October 2018
Fredrickson BL (2001) The role of positive emotions in positive psychology: the broaden-and-build theory of positive emotions. Am Psychol 56(3):218–226. https://doi.org/10.1037/0003-066x.56.3.218
Fullen MC, Richardson VE, Granello DH (2018) Comparing successful aging, resilience, and holistic wellness as predictors of the good life. Educ Gerontol 44(7):459–468. https://doi.org/10.1080/03601277.2018.1501230
Gerino E, Rollè L, Sechi C, Brustia P (2017) Loneliness, resilience, mental health, and quality of life in old age: a structural equation model. Front Psychol 8:2003. https://doi.org/10.3389/fpsyg.2017.02003
Gochman DS (2013) Handbook of health behavior research II: provider determinants. Springer Science & Business Media, New York
Harris JA, Castle NG (2019) Obesity and nursing home sare in the United States: a systematic review. Gerontologist 59(3):e196–e206. https://doi.org/10.1093/geront/gnx128
Hayes AF (2013) Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. Guilford Press, New York, NY, USA
Holmes SD, Galik E, Resnick B (2018) The mediating effect of resilience between social support for exercise and resident satisfaction in assisted living. J Hous Elderly 33(1):56–71. https://doi.org/10.1080/02763893.2018.1451796
Hrobonova E, Breeze E, Fletcher AE (2011) Higher levels and intensity of physical activity are associated with reduced mortality among community dwelling older people. J Aging Res 2011:651931. https://doi.org/10.4061/2011/651931
Isaksson U, Santamäki-Fischer R, Nygren B, Lundman B, Åström S (2007) Supporting the very old when completing a questionnaire. Res Aging 29(6):576–589. https://doi.org/10.1177/0164027507305924
Juczyński Z (2012) Measurement tools in health promotion and psychology [in Polish]. Wydawnictwo Naukowe PWN, Warsaw
Justine M, Hamid TA (2012) A multicomponent exercise program for institutionalized older adults: effects on depression and quality of life. J Gerontol Nurs 36(10):32–41. https://doi.org/10.3928/00989134-20100330-09
Kenny DA (2017) MedPower: An interactive tool for the estimation of power in tests of mediation [Computer software]. https://davidakenny.shinyapps.io/MedPower/. Accessed 4 April 2019
Kim C-G, June K-J, Song R (2003) Effects of a health-promotion program on cardiovascular risk factors, health behaviors, and life satisfaction in institutionalized elderly women. Int J Nurs Stud 40(4):375–381. https://doi.org/10.1016/s0020-7489(02)00102-5
Kim ES, Kubzansky LD, Soo J, Boehm JK (2016) Maintaining healthy behavior: a prospective study of psychological well-being and physical activity. Ann Behav Med 51(3):337–347. https://doi.org/10.1007/s12160-016-9856-y
Kim ES, Park N, Sun JK, Smith J, Peterson C (2014) Life satisfaction and frequency of doctor visits. Psychosom Med 76(1):86–93. https://doi.org/10.1097/psy.0000000000000024
Kim S‐Y, Jeon E‐Y, Sok SR, Kim K‐B (2006) Comparison of health-promoting behaviors of noninstitutionalized and institutionalized older adults in Korea. J Nurs Scholarsh 38(1):31–35. https://doi.org/10.1111/j.1547-5069.2006.00074.x
Kostka T, Jachimowicz V (2010) Relationship of quality of life to dispositional optimism, health locus of control and self-efficacy in older subjects living in different environments. Qual Life Res 19(3):351–361
Liu Y, Wang Z-H, Li Z-G (2012) Affective mediators of the influence of neuroticism and resilience on life satisfaction. Pers Individ Differ 52(7):833–838. https://doi.org/10.1016/j.paid.2012.01.017
MacLeod S, Musich S, Hawkins K, Alsgaard K, Wicker ER (2016) The impact of resilience among older adults. Geriatr Nurs 37(4):266–272. https://doi.org/10.1016/j.gerinurse.2016.02.014
Mayordomo T, Viguer P, Sales A, Satorres E, Meléndez JC (2016) Resilience and coping as predictors of well-being in adults. J Psychol 150(7):809–821. https://doi.org/10.1080/00223980.2016.1203276
McCabe BW, Hertzog M, Grasser CM, Walker SN (2005) Practice of health-promoting behaviors by nursing home residents. West J Nurs Res 27(8):1000–1016. https://doi.org/10.1177/0193945905278879
McCabe BW, Walker SN, Clark KA (1997) Health promotion in long-term care facilities. Int J Nurs Sci 2:153–167
Ogińska-Bulik N, Juczyński Z (2008) The Resiliency Measurement Scale [in Polish]. Now Psychol 3:39–56
Ogińska-Bulik N, Zadworna-Cieślak M, Rogala E (2015) The role of personal resources in prediction of health behaviors in seniors [in Polish]. Probl Hig 96(3):570–577
Palank CL (1991) Determinants of health-promotive behavior: a review of current research. Nurs Clin North Am 26:815–832
Pavot W, Diener E (2009) Review of the Satisfaction with Life Scale. In: Diener E (ed) Assessing well-being: the collected works of Ed Diener. Springer Netherlands, Dordrecht, pp 101–117
Peel NM, McClure RJ, Bartlett HP (2005) Behavioral determinants of healthy aging. Am J Prev Med 28(3):298–304. https://doi.org/10.1016/j.amepre.2004.12.002
Perna L, Mielck A, Lacruz ME, Emeny RT, Holle R, Breitfelder A, Ladwig KH (2012) Socioeconomic position, resilience, and health behaviour among elderly people. Int J Public Health 57(2):341–349. https://doi.org/10.1007/s00038-011-0294-0
Resnick B, Boltz M (2016) Incorporating function and physical activity across all settings. Annu Rev Gerontol Geriatr 36(1):293–321. https://doi.org/10.1891/0198-8794.36.293
Resnick B, Gwyther L, Roberto KA (2018) Resilience in aging, 2nd edn. Springer, New York
Richardson GE (2002) The metatheory of resilience and resiliency. J Clin Psychol 58(3):307–321. https://doi.org/10.1002/jclp.10020
Salguero A, Martínez-García R, Molinero O, Márquez S (2011) Physical activity, quality of life and symptoms of depression in community-dwelling and institutionalized older adults. Arch Gerontol Geriatr 53(2):152–157. https://doi.org/10.1016/j.archger.2010.10.005
Selivanova A, Cramm JM (2014) The relationship between healthy behaviors and health outcomes among older adults in Russia. BMC Public Health 14(1):1183. https://doi.org/10.1186/1471-2458-14-1183
Şenol V, Ünalan D, Soyuer F, Argün M (2015) The relationship between health promoting behaviors and quality of life in nursing home residents in Kayseri. J Geriatr 2014:839685. https://doi.org/10.1155/2014/839685
Sin NL, Lyubomirsky S (2009) Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. J Clin Psychol 65(5):467–487. https://doi.org/10.1002/jclp.20593
Social Welfare Act of 12 March 2004 (consolidated text: Polish Official Journal of 2019, text 1508)
Strine TW, Chapman DP, Balluz LS, Moriarty DG, Mokdad AH (2008) The associations between life satisfaction and health-related quality of life, chronic illness, and health Behaviors among U.S. community-dwelling adults. J Community Health 33(1):40–50. https://doi.org/10.1007/s10900-007-9066-4
Swindell WR, Ensrud KE, Cawthon PM, Cauley JA, Cummings SR, Miller RA (2010) Indicators of “Healthy Aging” in older women (65–69 years of age). A data-mining approach based on prediction of long-term survival. BMC Geriatrics 10(1):55. https://doi.org/10.1186/1471-2318-10-55
World Medical Association/WMA (2013) Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 310(20):2191–2194. https://jamanetwork.com/journals/jama/fullarticle/1760318. Accessed 8 May 2019
Zadworna M, Idczak-Paceś E, Gołygowska A, Kossakowska K (2020) Health behavior of institutionalized older adults – Research data. osf.io/m8k2t. https://doi.org/10.17605/OSF.IO/M8K2T
Zadworna-Cieślak M (2020) Spirituality, satisfaction with life and health-related behavior of older residents of long-term care institutions — a pilot study. Explore 16(2):123–129. https://doi.org/10.1016/j.explore.2019.07.016
Zadworna-Cieślak M (2017) The measurement of health-related behavior in late adulthood: the Health-Related Behavior Questionnaire for Seniors. Rocz Psychol 20(3):599–617. https://doi.org/10.18290/rpsych.2017.20.3-3en
Zadworna-Cieślak M, Ogińska-Bulik N (2018) Specificity of health-related behaviours in middle and late adulthood. Health Probl Civiliz 12(1):7–13. https://doi.org/10.5114/hpc.2018.74184
Zadworna-Cieślak M, Ogińska-Bulik N (2019) Satisfaction with life in old age — the role of developmental tasks attainment and resiliency. Educ Stud Rev 28(1):23–35. https://doi.org/10.12775/PBE.2019.002
Acknowledgments
The authors would like to acknowledge Edyta Idczak-Paceś and Aleksandra Golygowska, a members of the Psychology Master's seminar group, for their support in data collection.
Funding
The study was supported in part by a grant from the Faculty of Educational Sciences, University of Lodz, Poland.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation and data acquisition were performed by Magdalena Zadworna and the methodology section and analysis were performed by Karolina Kossakowska. The first draft of the manuscript was written by Magdalena Zadworna and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Humans
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zadworna, M., Kossakowska, K. Health behavior among Polish institutionalized older adults: the effect of resiliency mediated by satisfaction with life. J Public Health (Berl.) 29, 725–733 (2021). https://doi.org/10.1007/s10389-020-01301-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-020-01301-3