
Abstract
Aim
To develop the ‘Stronger Towns Index': a deprivation index that took into account characteristics of areas encompassing towns that may be eligible for redevelopment funding and explore how this index was associated with self-rated health and migration within England between 2001 and 2011.
Subject and methods
All members of the ONS Longitudinal Study in England aged 16 and over in 2001 whose records included a self-rated health response and a valid local authority code.
Local authorities in England were ranked using a composite index developed using the five metrics set out in the Stronger Towns Funding: productivity, income, skills, deprivation measures, and the proportion of people living in towns.
The index was split into deciles, and logistic regression carried out on the association between decile and self-rated health in 2001 in the main sample (n = 407,878) and decile change and self-rated health in 2011 in a subsample also present in 2011, with migration information (n = 299,008).
Results
There were areas in the lowest deciles of Town Strength who did not receive funding. After multiple adjustment, LS members living in areas with higher deciles were significantly more likely (7% to 38%) to report good health than those in the lowest decile in 2001. Remaining in the same decile between 2001 and 2011 was associated with 7% lower odds of good self-rated health in 2011.
Conclusion
It is important to consider health in towns when allocating funding. Areas in the Midlands may have missed out on funding which might help mitigate poor health.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The British Government has talked recently about levelling up ‘to ensure that no community is left behind and provide associated funding.’ (MHCLG 2021). The Ministry of Housing, Communities and Local Government’s (MHCLG) announcement on the Stronger Towns Fund in 2018 suggested allocation of funding ‘based on a combination of productivity, income, skills, deprivation measures, and the proportion of people living in towns.’ (MHCLG 2019). MHCLG did not publish its methodology for calculating prioritisation of towns for funding at the outset. Subsequently, they shared some details and initially selected 541 of 1,082 towns in England above the median value income deprivation and assessed these towns further against seven core criteria: income deprivation, skills deprivation, productivity, EU Exit exposure; exposure to economic shocks, investment opportunity, and alignment to wider government intervention plans for low-priority areas (Reuben 2021). Ministers selected all 40 high-priority towns, 49 medium-priority, and 12 low-priority to apply for funding (NAO 2020). There was criticism of this selection in the media (Syal 2020), from the political opposition (Reed 2020), and from the National Audit Office. By March 2021, only 52 of 101 towns had been allocated funding (MHCLG and Jenrick 2020; BBC 2021). The funding allocation did not use the criteria they originally advertised. We were interested to see if the original criteria selection by MHCLG were associated with risk factors and outcomes that might be amenable to improvement with the addition of relatively small amounts of financial support. This could have justified their retention and use as criteria.
A fuller policy was set out in the government's White Paper 'Levelling Up' (HM Government 2022), which had a stated aim of reducing geographical disparities based on a mixture of new and existing policies (Harari and Ward 2022). The paper established four objectives, to: (1) boost productivity, pay and jobs, (2) spread opportunities and improve public services, (3) restore a sense of community, local pride and belonging and (4) empower local leaders and communities. Doubts were raised over the viability of plans for implementation of these objectives (Marmot 2022; Institute for Government 2022).
The amenability of each of the five original domains (productivity, income, skills, deprivation measures and the proportion of people living in towns) to improvement with additional financial support was considered. Income and skill levels are likely to change through longer term investments targeted at job creation and in education; both might also change through internal migration. Migration might also reflect changes in urban life due to the COVID-19 pandemic. Deprivation was measured using the Index of Multiple Deprivation (IMD) 2015 (Smith et al. 2015; MHCLG 2018), some components of which may be more amenable to change with relatively small place-based investment than others. In order to appraise interventions to reduce inequalities, a suitable framework of evidence is required (Davey et al. 2022). Murray et al. (2022) found the strongest association with not being in work in England and Wales was with self-rated measures of health, and they recommended that the UK government changed the measure used in their Levelling Up health goal from Healthy Life-Expectancy to a self-reported health measure.
Area level characteristics including deprivation have been shown to be associated with poor health independent of individual-level factors in many studies; see Oakes et al. (2015) for a recent review. Several different area-based measures of socio-economic position have been used in health research for England (Townsend et al. 1988; Carstairs and Morris 1991; Jarman 1983) including the IMD. These indices vary in the factors included and how they are weighted and combined (Allik et al. 2016). The most common are material deprivation, occupation, unemployment, education, and housing. The addition of the productivity and percentage of people living in towns components of the Stronger Town Index make our index somewhat different.
Research on migration and migration destinations within the UK suggests that health-selective migration changes the geographical distribution of poor health. Previous research using the ONS Longitudinal Study ('the LS') which comprises linked census records and life events data for approximately 1% of the population of England and Wales since 1971, found that between 1971 and 1991, inequalities in health increased between the least and most deprived areas, and that health selective migration, rather than changes in the deprivation of the area that non-migrants live in, accounted for the majority of change, and other research has shown relationships between migration and limiting long-term illness (LLTI) (Norman et al. 2005; Boyle et al. 2001; Wilding et al. 2016).
We chose to explore how general health was associated with our Stronger Towns Index. First, we looked at whether health in 2001 was associated with Town Strength, to justify its use as an index. We then looked at whether migration between 2001 and 2011 to an area of higher Town Strength was associated with good health in 2011 compared to migration to an area with lower Town Strength. Intuitively, we would expect healthier people to live in stronger places, because healthier people are attracted to stronger places, or because healthier people make places stronger, or stronger places make people healthier.
Methods
To construct a Stronger Towns index for England’s Local Authorities, we gathered data on the five dimensions that had originally been proposed by MHCLG. We chose local authorities as they constituted a geographic area both for which data would be available and that would be able to administer funds. It was plausible that local authorities could include small parts of towns or more than one town entirely.
For productivity, we used sub-regional estimate using experimental Office for National Statistics (ONS) data on regional and sub-regional productivity. Data were taken from Table J4: Nominal Gross Valued Added GVA (B) (excluding rental income) per hour worked (at Local Authority level). A lower productivity led to a higher rank, indicative of greater need of funding). For income, we used estimates of gross disposable household income by local authority (ONS 2018). For skills, we used aggregate 2011 Census counts of the proportion of people with qualifications below GCSE C or equivalent (ONS 2013a). For deprivation, we used the IMD 2015 (MHCLG 2018), based on the proportion of Lower Super Output Areas (LSOAs) in the lowest decile, then the proportion in the second decile, etc. For the proportion living in towns, local authorities were ranked on the proportion of persons in the LA identified as living in small, medium, or large towns. Equally ranked LAs were ordered by population (ONS 2019). A higher proportion of people living in towns gave a higher rank.
The rank scores for each dimension were summed to give an (equally weighted) overall score. The overall score was then converted to a rank value, with the highest rank (1) representing the highest level of assumed eligibility. Local authorities were then grouped into rank deciles, and their aggregate characteristics were examined. We then matched up the 101 towns asked to apply for funds to the local authority in which they sit, and assigned their rank using our index.
To explore the association between Town Strength and health, a sample from England (the Towns Fund is not available in Wales) was drawn from the 2001 round of the ONS LS which comprises approximately 1.1% of the population of England and Wales, whose census records have been linked every 10 years between 1971 and 2011. The LS is representative of the whole population of England and Wales, including those in non-private households, has minimal bias due to non-response or attrition, high tracing rates (Lynch et al. 2015), and high response rates (ONS 2013b). Further information about the data can be found in the study’s Cohort Profile (Shelton et al. 2019).
Demographic and socioeconomic indicators of age and sex and highest educational qualifications in 2001 were included as potential covariates. LLTI in 2001 was also included in the analysis. Respondents were asked: ‘Do you have any long-term illness, health problem, or disability which limits your daily activities or the work you can do?’ with a note to ‘include problems which are due to old age’. For the dependent variable, we chose self-rated general health; respondents were asked: ‘Over the last 12 months would you say your health has on the whole been:...’ — the outcome measure was good health, compared with fairly good and not good combined.
The sample we used varied by analysis. The main sample (n = 407,878) was all members in England aged 16 and over in 2001 and whose records included a self-rated health response and a valid local authority code. LS members’ self-rated health outcomes were linked to their Stronger Towns Index rank decile by the local authority codes. We then derived a migration and social mobility (2001–2011) variable from these deciles. This had three categories: moved to an area within a lower decile of Town Strength, did not move or moved to area within the same decile for Town Strength, moved to an area within a higher decile of Town Strength.
Multivariate logistic regression was used to model the associations between self-rated health and Stronger Towns Index rank in a subsample of those who were also present in 2011, with information on highest educational qualification, migration, and sex.
Results
Town strength
Table 1 shows the ten local authorities with the highest ranked ('weakest') index for Town Strength; these are mapped in Fig. 1. Local authorities in lower deciles tended to be in the economically deprived areas of the North of England, the Midlands and coastal areas. Five local authorities that contained towns that were selected to bid that did not receive funding from the first two tranches were ranked in the top 10 in our index. These were Redcar and Cleveland (Redcar), Doncaster (Doncaster and Stainforth), Walsall (Bloxwich and Walsall), County Durham (Bishop Auckland) and Rotherham. Table 2 shows the rank of the local authorities which are not in the top 100 in the index, in which there were towns which were flagged for funding. We identified 29 local authorities whose towns were invited to apply for funding, but which were not in our top 100 ranking local authorities. Within those 29, almost half (n = 14) have been awarded funding as of April 2021. We also identified 44 LAs that were in the highest 100 ranked in our index, but whose towns were not invited to apply for funding.

Local authority Stronger Town Index rank decile, England and Wales. Various data sources see paper. Analysis authors’ own
Association with health
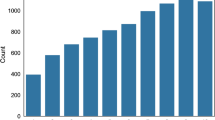
The proportion of adult LS members aged 16+ with good self-rated health in 2001 was 57% in Decile 1 with the lowest Town Strength, rising to 68% in Decile 10 with the highest Town Strength (Fig. 2). Bivariate analysis (not shown) revealed that significantly higher proportions of the LS members rated their health as good in higher deciles than in the lower deciles. It also revealed that there were significant differences in reporting good self-rated health by sex, age and education. Therefore, adjustment was made for these factors when modelling the association between self-rated health and decile by logistic regression. Table 3 shows the odds ratios for self-rated health - after adjustment for sex, age and education, LS members living in areas with higher deciles of Town Strength were significantly more likely (7% to 38%) to report good health than those in Decile 1.

Proportion of LS members aged 16+ with good self-rated health (SRH) in 2001, by local authority Stronger Town (ST) Index rank decile in their residential location in 2001 (N = 407,878). Data Source various (see paper) including ONS LS. Analysis authors’ own
Assocation with mobility
Table 4 shows a matrix of the proportion of people in each decile in 2001, by decile in 2011. The vast majority of people were resident in the same decile in 2011 as they were in 2001. The highest proportion of ‘stayers’ was in Decile 1 (the lowest decile for town strength). Bivariate probability analysis (not shown) revealed significant differences in the proportions of LS members reporting good self-rated health by change in decile; the lowest proportion among those who remained in Decile 1 and the highest among those who were in Decile 10 in 2011. We therefore looked at the association between good self-rated health and any positive change between decile compared to any negative change in deciles between 2001 and 2011. Moving to an area with a higher decile for Town Strength was not associated with higher odds of good self-rated health in 2011 when compared to moving to an area with lower Town Strength after adjustment for age, sex, and highest educational qualifications (OR=1.04, 95%CI [0.99-1.09]. Remaining in the same decile was however associated with lower odds of good self-rated health (OR=0.93, 95% CI [0.89, 0.96], n=299,008).
Discussion
Our Stronger Towns Index was built at local authority level using openly available versions of the original indicators or proxies thereof that were proposed by MCHLG. The geography of Town Strength was similar to other deprivation geographies, with high levels of deprivation in the North West and lower levels in the South East. By adding the proportion of people living in towns, it demonstrates that there is poverty beyond those regions. The MCHLG choice of towns does not capture the same areas as our index. Notably, our index identifies the Midlands as potentially missing out on funds. Also Swale in the South East did not get selected to apply for funding by 2021, yet scored very highly in our index and was the focus of media attention in late 2020 for having the second highest rate of COVID-19 infection (BBC 2020). Of the areas that were selected to apply for funding, half of those we ranked in the top ten for low Town Strength did not receive funding in the first two tranches.
People living in economically stronger areas, as indicated by Stronger Town Index rank decile, were significantly more likely to rate their health as good, even after accounting for factors known to be associated with self-rated health. Research has shown that migration is less frequent among those in poor health (Wilding et al. 2016). This extends research on the healthy migrant effect, but in relation to other migrants rather than just those who do not move. It was non-migration combined with remaining in similar places that was associated with lower odds of good health, perhaps demonstrating the resilience education provides for those who move to ‘weaker’ areas. This is of current policy interest, with national relocation of those in social housing from overcrowded locations, e.g. London to lower income areas.
Availability of data and materials
The results are derived from the ONS Longitudinal Study, which is only available through ONS Secure Research Service. The component records cannot be re-disseminated.
References
Allik M, Brown D, Dundas R, Leyland A (2016) Developing a new small-area measure of deprivation using 2001 and 2011 census data from Scotland. Health Place 39:122–130. https://doi.org/10.1016/j.healthplace.2016.03.006
BBC (2020) Covid rules ‘disregarded’ as Swale becomes second worst-hit area. BBC News, London. https://www.bbc.com/news/uk-england-kent-55044408. Accessed 7 Oct 2022
BBC (2021) Budget 2021: £1bn Towns Fund for 45 areas of England. BBC News, London. https://www.bbc.com/news/uk-england-56271275. Accessed 7 Oct 2022
Boyle P, Gatrell A, Duke-Williams O (2001) Do area-level population change, deprivation and variations in deprivation affect individual-level self-reported limiting long-term illness? Social Sci Med 53:795–799. https://doi.org/10.1016/S0277-9536(00)00373-7
Carstairs V, Morris R (1991) Deprivation and health in Scotland. Aberdeen University Press
Davey F, McGowan V, Birch J, Khun I, Lahiri A, Gkiouleka A, Arora A, Sowden S, Bambra C, Ford J (2022) Levelling up health: a practical, evidence-based framework for reducing health inequalities. Public Health Pract (Oxf) 4:100322. https://doi.org/10.1016/j.puhip.2022.100322
Harari H, Ward M (2022) Levelling up: What are the Government's proposals? House of Commons Library Briefing Paper no. 9463. UK Parliament, London. https://researchbriefings.files.parliament.uk/documents/CBP-9463/CBP-9463.pdf. Accessed 7 Oct 2022
HM Government (2022) Levelling Up the United Kingdom. CP 604. United Kingdom Government, London. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1052708/Levelling_up_the_UK_white_paper.pdf. Accessed 7 Oct 2022
Institute for Government (2022) Levelling up: the IfG view on the white paper. IfG Insight. Institute for Government, London. https://www.instituteforgovernment.org.uk/sites/default/files/publications/levelling-up-white-paper-ifg-view.pdf. Accessed 7 Oct 2022
Jarman B (1983) Identification of underprivileged areas. BMJ 286(6379):1705–1709. https://doi.org/10.1136/bmj.286.6379.1705
Lynch K, Leib S, Warren J, Rogers N, Buxton J (2015) Longitudinal Study 2001—2011 Completeness of census linkage. Office for National Statistics, London. https://www.ons.gov.uk/file?uri=/aboutus/whatwedo/paidservices/longitudinalstudyls/longitudinalstudy20012011completenessofcensuslinkage.pdf
Marmot M (2022) The government’s levelling up plan: a missed opportunity. BMJ 2022(376):o356. https://doi.org/10.1136/bmj.o356
Ministry of Housing, Communities & Local Government (2018) English Indices of Deprivation 2015 - LSOA Level. Ministry of Housing, Communities & Local Government, Wolverhampton, England.https://data.gov.uk/dataset/8f601edb-6974-417e-9c9d-85832dd2bbf2/english-indices-of-deprivation-2015-lsoa-level. Accessed 23 June 2020
Ministry of Housing, Communities & Local Government (2019) Stronger Towns Fund—Questions and answers. Ministry of Housing, Communities & Local Government, Wolverhampton, England. https://www.gov.uk/government/publications/stronger-towns-fund/stronger-towns-fund-questions-and-answers. Accessed 7 Oct 2022
Ministry of Housing, Communities & Local Government and HM Treasury (2021) New levelling up and community investments. Ministry of Housing, Communities & Local Government and HM Treasury, London. https://www.gov.uk/government/collections/new-levelling-up-and-community-investments. Accessed 7 Oct 2022
Ministry of Housing, Communities & Local Government, Jenrick R (2020) First Town Deals worth almost £180 million announced. Ministry of Housing, Communities & Local Government, Wolverhampton, England. https://www.gov.uk/government/news/first-town-deals-worth-almost-180-million-announced. Accessed 7 Oct 2022
Murray E, Head J, Shelton N, Beach B, Norman P (2022) Does it matter how we measure the health of older people in places for associations with labour market outcomes? A cross-sectional study. BMC Public Health 22(1):2252. https://doi.org/10.1186/s12889-022-14661-0
National Audit Office (2020) Review of the Town Deals selection process. National Audit Office, London. https://www.nao.org.uk/wp-content/uploads/2020/07/Review-of-the-Town-Deals-selection-process.pdf. Accessed 7 Oct 2022
Norman P, Boyle P, Rees P (2005) Selective migration, health and deprivation: A longitudinal analysis. Social Sci Med 60:2755–2771. https://doi.org/10.1016/j.socscimed.2004.11.008
Oakes J, Andrade K, Biyoow I, Cowan L (2015) Twenty years of neighborhood effect research: an assessment. Curr Epidemiol Reports 2:80–87. https://doi.org/10.1007/s40471-015-0035-7
Office for National Statistics (2013a) 2011 Census Quick Statistics: Highest level of qualification All usual residents aged 16 and over. Office for National Statistics, Titchfield, UK. https://www.nomisweb.co.uk/census/2011/qs501ew. Accessed 6 Oct 2022
Office for National Statistics (2013b) 2011 census statistics for England and Wales: March 2011 QMI, Office for National Statistics. Office for National Statistics, Titchfield, UK. https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/methodologies/2011censusstatisticsforenglandandwalesmarch2011qmi. Accessed 12 Feb 2021
Office for National Statistics (2018) Regional gross disposable household income by local authority. Office for National Statistics, Titchfield, UK. https://www.ons.gov.uk/economy/regionalaccounts/grossdisposablehouseholdincome/datasets/regionalgrossdisposablehouseholdincomegdhibylocalauthorityintheuk. Accessed 23 June 2020
Office for National Statistics (2019) Data on population living in towns was taken from analysis by ONS in the report "Understanding towns in England and Wales: an introduction". Office for National Statistics, Titchfield, UK. https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/articles/understandingtownsinenglandandwales/anintroduction/previous/v1. Accessed 9 July 2020
Reed S (2020) Questions Robert Jenrick must answer about Towns Fund Scandal—The Labour Party. The Labour Party, Newcastle upon Tyne, UK. https://labour.org.uk/press/questions-robert-jenrick-must-answer-about-towns-fund-scandal/ Accessed 7 Oct 2022
Reuben A (2021) Towns Fund: How were the winners chosen? BBC News, London. https://www.bbc.com/news/56283199. Accessed 7 Oct 2022
Shelton N, Marshall C, Stuchbury R, Grundy E, Dennett A, Tomlinson J, Duke-Williams O, Xun W (2019) Cohort Profile: the Office for National Statistics Longitudinal Study (The LS). Int J Epidemiol 48(2):383g–384g. https://doi.org/10.1093/ije/dyy243
Smith T, Noble M, Noble S, Wright G, McLennan D, Plunkett E (2015) The English Indices of Deprivation 2015: Research report. UK Government, London. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/464597/English_Indices_of_Deprivation_2015_-_Research_Report.pdf. Accessed 7 Oct 2022
Syal R (2020) Some of England’s most deprived towns left out of £3.6bn funding scheme. The Guardian, London. http://www.theguardian.com/society/2020/jul/21/some-of-englands-most-deprived-towns-left-out-of-36bn-funding-scheme. Accessed 7 Oct 2022
Townsend P, Phillimore P, Beattie A (1988) Health and deprivation: Inequality and the North. Routledge, London
Wilding S, Martin D, Moon G (2016) The impact of limiting long term illness on internal migration in England and Wales: New evidence from census microdata. Social Sci Med 167:107–115. https://doi.org/10.1016/j.socscimed.2016.08.046
Acknowledgements
The authors are grateful to the Office for National Statistics for sending us the proportions of people living in towns for each local authority.
The authors are grateful to the ESRC who funded the Stronger Towns event through their ESRC Business Boost Programme, and CeLSIUS, UCL in partnership with UCL Innovation and Enterprise, who hosted the event in 2019. The permission of the Office for National Statistics to use the Longitudinal Study is gratefully acknowledged, as is the help provided by staff of the Centre for Longitudinal Study Information and User Support (CeLSIUS). CeLSIUS is supported by the ESRC (Award Ref: ES/V003488/1). The authors alone are responsible for the interpretation of the data. Census output is Crown copyright and is reproduced with the permission of the Controller of HMSO and the Queen's Printer for Scotland.
Author information
Authors and Affiliations
Contributions
The index was designed collectively by the authors, and all authors worked on edits and revisions to the text.
Oliver Duke-Williams gathered data sets and implemented the index.
Jemima Stockton conducted the analyses of LS sample members having attached index values on the basis of their residential locations.
Nicola Shelton wrote the main draft of the paper.
Corresponding author
Ethics declarations
Ethics approval
This project was reviewed by the Office for National Statistics Microdata Release Panel (ONS-MRP). The ethical acceptability of research projects is one of the aspects considered by the ONS-MRP. If there are concerns about the ethical acceptability of a piece of research, the ONS-MRP has the option of referring the project to the National Statistician’s Data Ethics Advisory Committee (NSDEC). The National Statistician’s Data Ethics Advisory Committee agreed that the Longitudinal Study was consistent with the UK Statistics Authority’s ethical principles in UK Statistics Authority, 2022 (https://uksa.statisticsauthority.gov.uk/publication/nsdec-minute-and-agenda-july-2022/#pid-meeting-minute).
Consent for publication
The manuscript does not contain any individual person's data. All results are aggregated and outputs are checked by ONS for any unintended disclosure of personal information.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships which have, or could be perceived to have, influenced the work reported in this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Duke-Williams, O., Stockton, J. & Shelton, N. Levelling Up for health in towns? Development of a new deprivation index: the ‘Stronger Towns Index’ and its association with self-rated health and migration in England, between 2001 and 2011. J Public Health (Berl.) (2023). https://doi.org/10.1007/s10389-023-01944-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-023-01944-y