
Abstract
Aim
Musculoskeletal conditions impact our society owing to the associated burden, with significant implications for health systems and people’s quality of life. Patient-reported outcome measures (PROMs) are used to optimize the results of rehabilitation programs. The study aims to identify the PROMs used in rehabilitation programs after knee surgery.
Subject and methods
This rapid systematic review was conducted using MEDLINE® and CINAHL® databases, considering all studies carried out until December 2023, with a registered protocol (PROSPERO reference: CRD42024504263). Studies were included with adult participants undergoing knee surgery and using PROMs to measure outcomes before and after rehabilitation programs.
Results
Sixteen studies with 3469 participants in rehabilitation programs after knee surgery were included. Methodologically and according to the criteria recommended by the Joanna Briggs Institute, more than half of the studies were of high quality, with values of more than 80%, including randomized controlled trials, cohorts, and quasi-experimental designs. Outcomes were assessed before and after rehabilitation programs, using general (n = 6) and knee-specific (n = 11) PROMs. Of all the PROMs identified in the different studies selected for this systematic review, the ones used the most were KOOS (in 14 studies), EQ5D-5L, and WOMAC (in 3 studies).
Conclusion
This rapid systematic review shows the need to identify and implement PROMs during rehabilitation programs after knee surgery, measuring participants’ health status, symptoms, treatment satisfaction, and physical and mental performance. In this way, it is possible to make value-based comparisons with other interventions, improving and tailoring rehabilitation care.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Musculoskeletal diseases are a public health problem, and in recent years, they have taken a significant economic toll on health systems (Nguyen et al. 2024). They are one of the consequences of an aging population. They are considered the leading cause of disability in four of the six regions of the world, thus having a real impact on our society, not only because of the burden associated with them but also because of the costs they entail (Vos et al. 2020). One of the main musculoskeletal conditions is related to the knee joint, which is considered complex and vulnerable owing to its susceptibility to various types of injuries, particularly those originating in the ligaments, meniscus, and cartilage (Barbosa de Almeida and Esteves 2023). In most situations, knee injury is associated with physical disability, stiffness, pain, restriction of movement, and impairment of the person’s quality of life (Barbosa de Almeida et al. 2023; Truong et al. 2020). The implications for quality of life are significant, showing the influence of psychosocial and contextual factors on the process of recovering to carry out activities similar to before the traumatic event (Truong et al. 2020). After a knee injury, a few treatment options have been proposed, including surgery and rehabilitation programs. These forms of treatment are fundamental in the recovery process, improving the quality of life of people with musculoskeletal conditions by optimizing proprioception, strength, and muscle function, which are compromised immediately after surgery because of the reflex inhibition of motor neurons and immobilization (Khan et al. 2014). To tailor and individualize these rehabilitation programs to a given context, we evaluated the results obtained directly from those who have experienced this process. This evaluation uses patient-reported outcome measures (PROMs), which comprise tests applied since the 1960s (Churruca et al. 2021). These aim to obtain a standardized response, the coding of which leads to the knowledge (and quantification) of opinions, feelings, experiences, abilities, and perceptions (Deshpande et al. 2011). The evolution of PROMs has been significant in recent years, with the creation of dozens of scales that assess health status, functional status, symptoms and measures of symptom burden, experience with care, health behaviors, treatment satisfaction, economic impact, and specific dimensions of the patient experience such as physical performance, mental performance, anxiety, and depression (Deshpande et al. 2011). Despite the proliferation of PROMs and their development, which has led to better decisions in various areas of health, challenges remain when it comes to selecting these instruments for what you want to measure (Churruca et al. 2021). Therefore, in the research context, it is essential to look for the most objective measures so that the results can be comparable to make appropriate and objective clinical decisions. Given this need for knowledge regarding the selection of the different PROMs used in rehabilitation programs after knee surgery, we set out to identify the PROMs used in an outpatient rehabilitation program after knee surgery.
Methods
The methods for this study were established in the review protocol previously registered on the PROSPERO platform (CRD42024504263). This rapid systematic review was proposed in response to the need to update and produce scientific evidence on PROMs (Hamel et al. 2021) to answer the research question: what are the PROMs associated with rehabilitation programs after knee surgery in an outpatient setting? It was conducted according to the Rapid Review Guide of the World Health Organization (WHO) (Tricco et al. 2017) and followed the reporting guidelines of Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) (Page et al. 2021). The PCC strategy was used (Aromataris and Munn 2020): participants (patients who participated in a rehabilitation program after knee surgery), concept (PROMs used in rehabilitation programs), and context (outpatient rehabilitation intervention). On the basis of this search strategy, we present the eligible criteria for this review.
Eligibility criteria
Inclusion criteria – Studies were considered eligible if: 1. Participants were in rehabilitation programs after knee surgery; 2. Adult participants (> 18 years); 3. English-language publications; 4. Rehabilitation programs in which PROMs were applied. Exclusion criteria: 1. Studies with inpatient programs; 2. Previous surgeries on the ipsilateral knee; 3. Unconsolidated fractures; 4. Partial or total amputation of the lower limbs. Publications in book chapters, theses, literature reviews, editorials, or conference abstracts without a full paper were also excluded.
Search strategy
Terms indexed in MEDLINE® and CINAHL® were used, as shown in Table 1, with the respective Boolean operators, considering all the studies carried out until December 2023. When undertaking a rapid review, it is recommended to search a limited number of databases (Garritty et al. 2021).
Study selection
The selection of studies included randomized, prospective, and retrospective studies, both controlled and uncontrolled. All studies that used PROMs to evaluate participants in outpatient rehabilitation programs after knee surgery were considered. The results were uploaded and analyzed on the Rayyan® platform, duplicate studies were removed, and two reviewers blindly applied the eligibility criteria (JM & SM). The relevance of the studies to be included in the review was considered by analyzing the titles and abstracts. Then the full text of the articles was independently assessed and screened by the reviewers (JM & SM). Discrepancies during the screening process were discussed and resolved by a third independent reviewer.
Methodological quality assessment
The quality assessment of each of the included studies was based on the recommendations of the Joanna Briggs Institute, and the classification was summarized in a narrative and tabular format. Considering the recommendations, the sum of the points was classified from 70% of the items present. Thus, a score between 70 and 79% of the checklist criteria was classified as medium quality, between 80 and 90% was assigned high quality, and a score greater than 90% of the criteria was classified as excellent quality (Barker et al. 2023; Munn et al. 2023).
Data extraction and analysis
A reviewer (JM) used an instrument aligned with the review’s objective to extract data from the included studies. The data was summarized in tabular and narrative form using the Excel® platform, mapping the main results: country, participants, average age, type of surgery, methodology and study design, PROMs used and the times when they were applied, details of the rehabilitation programs and interventions. The different PROMs were grouped into two levels, general and specific to knee pathology, with evidence of the year in which they were constructed, number of items, and time taken to complete them. A second reviewer validated all the data extracted by the tool (SM).
Results
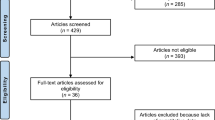
Sixteen studies met the inclusion criteria, reporting on PROMs applied to participants undergoing only knee surgery before and after rehabilitation programs in an outpatient setting (Arhos et al. 2020; Barker et al. 2021; Beynnon et al. 2011; Bigouette et al. 2019; Bruun-Olsen et al. 2013; Çelebi et al. 2015; DeJong et al. 2020; Hall et al. 2015; Hill and O’Leary 2013; Hsu et al. 2017; Jakobsen et al. 2014; Johnson et al. 2020; LeBrun et al. 2022; Markström et al. 2022; Moffet et al. 2015; Schache et al. 2019; Terradas-Monllor et al. 2021). Figure 1 shows the summary of the search results through the flowchart for this systematic review based on the current guidelines – PRISMA 2020.

PRISMA flowchart of study selection
After using the search strategy, 309 articles were identified, and duplicates were eliminated (n = 50). After analyzing the title and abstract, some articles were excluded because they did not refer to rehabilitation (n = 272). The entire text of the selected articles was analyzed. Some were excluded because the population was under 18 years old and with groups of participants also intervened in the hip (n = 5), others did not identify the study design used (n = 2), and others reported rehabilitation but did not apply PROMs before and after the rehabilitation program (n = 7). Some did not present the intervention they used in the rehabilitation process (n = 7).
The quality of all the studies included was high, with more than half scoring over 80% after applying the Joanna Briggs Institute evaluation criteria. In the experimental studies, the main weakness was that the outcome assessors were not blinded to the treatment assignment, while in the cohort studies, there was a lack of identification and strategies to deal with confounding factors.
The characteristics of the studies are structurally presented in Table 2 according to the year of publication, while the other variables (country, type of study, population, PROMs, and rehabilitation program) are presented in Table 1 in order of year of publication.
The 16 studies included in this review were carried out in different regions of the world, with Europe (n = 7) and the USA (n = 5) being the most prevalent, two studies in Australia and one each in Canada and Taiwan. The number of participants ranged from 24 to 980, with average ages ranging from 22 to 72. The types of surgery identified were anterior cruciate ligament reconstruction (n = 6), total knee arthroplasty (n = 9), and arthroscopic partial meniscectomy (n = 1).
In all the studies, the PROMs were administered to the participants at baseline, before the rehabilitation intervention began, and after it had ended. Assessments of outcomes after the end of the intervention varied over time, from 1 to 36 months. The PROMs identified take on a wide variety, differing in the number of questions/items, the time required to complete them, and the outcomes they measure. We can then group the PROMs into two sub-categories, classifying them as generic and specific to knee pathology. In this way, the results obtained from this rapid systematic review have been structured according to the year in which they were created, describing the specific characteristics of each PROM, such as the abbreviation, number of items, and completion time, as shown in Table 3.
Discussion
The most important results of this study show the diversity of PROMs used in rehabilitation programs after knee surgery. This variety is based on several particularities, namely the number and type of questions/items, the time needed to fill them in, the translations available for each one, the type of sub-scales, the cost/license required for their use, and the time lag in applying the PROMs (Hohmann et al. 2011; Park et al. 2018; Perez et al. 2017; Rolfson et al. 2016). Given this conceptualization and the results obtained in identifying the PROMs used in rehabilitation programs after knee surgery, it is recommended to collect the information reported by the participants through the application of generic and specific PROMs (Moreira et al. 2024; Rolfson et al. 2016).
Generic PROMs
Generic measures make assessing general health and/or health-related quality of life possible, considering the person’s physical, mental, and socio-cultural aspects (Rolfson et al. 2016). This study identified several generic PROMs, including the EQ5D-5L, HADS, SF-36, SF-12, VR-12, and the AM-PAC. The one most used in rehabilitation after knee surgery was the EQ5D-5L, a descriptive instrument that defines health in five dimensions: mobility, self-care, habitual activities, pain/discomfort, and anxiety/depression (Herdman et al. 2011). It was designed to be self-completed and allows you to assess your general health when filling it out using a vertical visual analogue scale from 0 to 100 (EQ-VAS). In the study carried out by Conner-Spady et al. (2015) on participants proposed for knee surgery, this instrument was considered essential in assessing the dimensions mentioned above, given the high convergent validity in the study population (Conner-Spady et al. 2015). Another of the general PROMs identified in this review was the HADS, which is an asset for researchers/health professionals to interpret emotional and cognitive characteristics related to symptoms of depression and anxiety (Çelebi et al. 2015; Terradas-Monllor et al. 2021). The scale consists of 14 questions, seven of which identify symptoms of depression, and the other seven identify symptoms of anxiety, with total scores ranging from 0 to 42 points. The application of this PROM is essential after knee surgery and during rehabilitation since throughout the recovery process, through the combination of the psychological process and the underpinnings of the fear-avoidance, fear-avoidance beliefs and behaviors are formed that drive some pain-related disability (Terradas-Monllor et al. 2021). The SF-36 was another PROM identified in one of the studies that applied for an exercise program after knee surgery (Hsu et al. 2017), or in a shorter version, the SF-12, which made it possible to assess health-related quality of life in its mental (MCS) and physical (PCS) components (Schache et al. 2019). Since it was developed, this tool has been used for studies in the field of rehabilitation (Moock et al. 2006). In recent years, several rehabilitation research studies have shown that this is a viable tool for measuring the health-related quality of life of patients taking part in rehabilitation programs (Moock et al. 2006; Moreira and Grilo 2019). Hsu et al. (2017) evaluated the eight domains of the SF-36 and showed that exercise improved all the domains of the physical element of the participants after knee surgery and only the domains of the mental component in the control group (Hsu et al. 2017). The VR-12 was one of the PROMs used, allowing the physical and mental components to be assessed in the same way as the SF-12 (Kazis et al. 1998) and emphasizing the usefulness of evaluating the health-related quality of life of participants in telerehabilitation programs after knee surgery (LeBrun et al. 2022). Another of the general PROMs identified, the AM-PAC, has been developed over the years for application in the context of clinical practice and research and is based on the conceptualization defined by the World Health Organization’s International Classification of Functioning, Disability, and Health. This instrument allows for a comprehensive and accurate assessment of functional outcomes related to the participant in an acute and/or post-acute care environment (DeJong et al. 2020).
Joint specific PROM
In addition to generic PROMs, several knee pathology-specific PROMs are also used to measure specific outcomes, and for this study, only those used in rehabilitation programs following knee surgery were considered. The most used was KOOS (Arhos et al. 2020; Barker et al. 2021; Beynnon et al. 2011; Bigouette et al. 2019; Bruun-Olsen et al. 2013; DeJong et al. 2020; Hall et al. 2015; Hill and O’Leary 2013; Hsu et al. 2017; Jakobsen et al. 2014; Johnson et al. 2020; Moffet et al. 2015; Schache et al. 2019), allowing the outcomes to be assessed after self-completion of 42 items: pain (9 items), symptoms (7 items), activities of daily living (17 items), sport and recreation function (5 items), and knee-related quality of life (4 items) (Roos et al. 2024). All items are scored from 0 to 4; for each subscale, the scores are transformed into scales from 0 to 100 (0 representing extreme knee problems and 100 representing no knee problems) (Hsu et al. 2017; Roos et al. 2024). This is a reliable tool for the participants we included in this study, confirmed by statistically significant results when comparing two groups in a rehabilitation program after anterior cruciate ligament surgery (Bigouette et al. 2019; Bruun-Olsen et al. 2013; Hill and O’Leary 2013).
WOMAC was another specific PROMs identified, often used in a rehabilitation program after knee surgery. It consists of 24 items grouped into three dimensions (Terradas-Monllor et al. 2021). A 5-point Likert scale was used to determine the score by the sum of the aggregate scores for the pain, stiffness, and physical function dimensions (Escobar et al. 1982). The TSK-11, GRS (perceived knee function), IKDC-SKF, and KOS-ADLS were also used in at least two studies each (Arhos et al. 2020; Johnson et al. 2020; Terradas-Monllor et al. 2021). These specific PROMs made it possible to measure the effect of the rehabilitation intervention, namely health-related quality of life. The specific PROMs identified in smaller numbers in this study were the IKDC, SOPA-B, LEAS, LKSS, and KOOS-JR, which measure various dimensions, including functional results associated with the knee joint, the evolution of pain, and physical performance throughout the rehabilitation program (Bigouette et al. 2019; Çelebi et al. 2015; LeBrun et al. 2022; Terradas-Monllor et al. 2021). Valuing these dimensions through specific PROMs, namely pain assessment, has been recommended in several studies as one of the aspects that can foster innovation and success in the implementation of interventions since it can make it possible to optimize procedures to reduce the level of chronic pain and improve health-related quality of life (Van Beest et al. 2022).
Analysis of the studies included in this rapid systematic review showed that specific PROMs were selected for a significant population of patients, including those participating in rehabilitation programs following knee surgery (Rolfson et al. 2016), and good measurement properties of the instrument. This rapid review shows the diversity of specific PROMs, which should be used with generic PROMs (Rolfson et al. 2016) to better respond to changes in the condition of interest and other coexisting conditions over time.
Limitations
This rapid review has some limitations, namely that only English language articles were included. This review included studies from several countries around the world, helping to increase the transferability of the conclusions; however, this can be considered a limitation given the specific context of each country and the different income levels in each country. It would be necessary in future studies to compare program participants and rehabilitation considering the PROMs specific to each type of surgery.
Conclusion
The use and diversity of PROMs have been increasing in rehabilitation programs after knee surgery, which is why it is essential to synthesize the instruments according to the outcomes they are intended to measure. By identifying the general and specific PROMs for each situation, it is possible to adapt each one more advantageously to the context and regional variations, guaranteeing the quality and continuous improvement of the care provided. Using this type of instrument to measure and compare outcomes before and after a rehabilitation program following the recovery process from knee surgery can be an asset for optimizing health practices, rationally allocating available resources, and improving care for people in need. In this sense, this systematic review can improve the consistency of the use of PROMs and enhance the results of a rehabilitation process after knee surgery.
Data availability
Available on request from the corresponding author.
Code availability
Not applicable.
References
Arhos EK, Capin JJ, Ito N et al (2020) Functional measures do not differ in late stage rehabilitation after anterior cruciate ligament reconstruction according to mechanism of injury. Int J Sports Phys Ther 15(5):744–754. https://doi.org/10.26603/ijspt20200744
Aromataris E, Munn Z (2020) JBI manual for evidence synthesis. Joanna Briggs Institute, North Adelaide
Barbosa de Almeida M, Esteves J (2023) The effects of electromyographic biofeedback training after meniscectomy: a randomized controlled trial. Sport Sci 16(1):10–18. https://doi.org/10.17026/dans-z9g-73ad
Barker KL, Room J, Knight R et al (2021) Home-based rehabilitation programme compared with traditional physiotherapy for patients at risk of poor outcome after knee arthroplasty: the CORKA randomised controlled trial. BMJ Open 11(8). https://doi.org/10.1136/bmjopen-2021-052598
Barker TH, Stone JC, Sears K et al (2023) Revising the JBI quantitative critical appraisal tools to improve their applicability: an overview of methods and the development process. JBI Evidence Synthesis 21(3):478–493. https://doi.org/10.11124/JBIES-22-00125
Beynnon BD, Johnson RJ, Naud S et al (2011) Accelerated versus nonaccelerated rehabilitation after anterior cruciate ligament reconstruction: a prospective, randomized, double-blind investigation evaluating knee joint laxity using roentgen stereophotogrammetric analysis. Am J Sports Med 39(12):2536–2548. https://doi.org/10.1177/0363546511422349
Bigouette JP, Owen EC, Lantz B et al (2019) Relationship between sports participation after revision anterior cruciate ligament reconstruction and 2-year patient-reported outcome measures. Am J Sports Med 47(9):2056–2066. https://doi.org/10.1177/0363546519856348
Bruun-Olsen V, Heiberg KE, Wahl AK et al (2013) The immediate and long-term effects of a walking-skill program compared to usual physiotherapy care in patients who have undergone total knee arthroplasty (TKA): a randomized controlled trial. Disabil Rehabil 35(23):2008–2015. https://doi.org/10.3109/09638288.2013.770084
Çelebi MM, Başkak B, Saka T et al (2015) Psychiatric and functional evaluation of professional athletes following anterior cruciate ligament reconstruction. Acta Orthop Traumatol Turc 49(5):492–496. https://doi.org/10.3944/AOTT.2015.14.0380
Churruca K, Pomare C, Ellis L et al (2021) Patient-reported outcome measures (PROMs): a review of generic and condition-specific measures and a discussion of trends and issues. Health Expect 24(4):1015–1024. https://doi.org/10.1111/hex.13254
Conner-Spady BL, Marshall DA, Bohm E et al (2015) Reliability and validity of the EQ-5D-5L compared to the EQ-5D-3L in patients with osteoarthritis referred for hip and knee replacement. Qual Life Res 24(7):1775–1784. https://doi.org/10.1007/s11136-014-0910-6
DeJong G, Hsieh CJ, Vita MT et al (2020) Innovative devices did not provide superior total knee arthroplasty outcomes in post-operative rehabilitation: results from a four-arm randomized clinical trial. J Arthroplasty 35(8):2054–2065. https://doi.org/10.1016/j.arth.2020.03.048
Deshpande P, Rajan S, Sudeepthi B et al (2011) Patient-reported outcomes: a new era in clinical research. Perspect Clin Res 2(4):137. https://doi.org/10.4103/2229-3485.86879
Escobar A, Quintana JM, Bilbao A et al (1982) Validation of the Spanish version of the WOMAC questionnaire for patients with hip or knee osteoarthritis
Garritty C, Gartlehner G, Nussbaumer-Streit B et al (2021) Cochrane rapid reviews methods group offers evidence-informed guidance to conduct rapid reviews. J Clin Epidemiol 130:13–22. https://doi.org/10.1016/j.jclinepi.2020.10.007
Hall M, Hinman RS, Wrigley TV et al (2015) Neuromuscular exercise post partial medial meniscectomy: Randomized controlled trial. Med Sci Sports Exerc 47(8):1557–1566. https://doi.org/10.1249/MSS.0000000000000596
Hamel C, Michaud A, Thuku M et al (2021) Defining rapid reviews: a systematic scoping review and thematic analysis of definitions and defining characteristics of rapid reviews. J Clin Epidemiol 129:74–85. https://doi.org/10.1016/j.jclinepi.2020.09.041
Herdman M, Gudex C, Lloyd A et al (2011) Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 20(10):1727–1736. https://doi.org/10.1007/s11136-011-9903-x
Hill GN, O’Leary ST (2013) Anterior cruciate ligament reconstruction: the short-term recovery using the Knee Injury and Osteoarthritis Outcome Score (KOOS). Knee Surg Sports Traumatol Arthrosc 21(8):1889–1894. https://doi.org/10.1007/s00167-012-2225-x
Hohmann E, Tetsworth K, Bryant A (2011) Physiotherapy-guided versus home-based, unsupervised rehabilitation in isolated anterior cruciate injuries following surgical reconstruction. Knee Surg Sports Traumatol Arthrosc 19(7):1158–1167. https://doi.org/10.1007/s00167-010-1386-8
Hsu WH, Hsu W, Shen WJ et al (2017) Circuit training enhances function in patients undergoing total knee arthroplasty: a retrospective cohort study. J Orthop Surg Res 12(1). https://doi.org/10.1186/s13018-017-0654-4
Jakobsen TL, Kehlet H, Husted H et al (2014) Early progressive strength training to enhance recovery after fast-track total knee arthroplasty: a randomized controlled trial. Arthritis Care Res 66(12):1856–1866. https://doi.org/10.1002/acr.22405
Johnson JL, Irrgang JJ, Risberg MA et al (2020) Comparing the responsiveness of the global rating scale with legacy knee outcome scores: a delaware-oslo cohort study. Am J Sports Med 48(8):1953–1960. https://doi.org/10.1177/0363546520924817
Kazis LE, Miller DR, Clark J et al (1998) Health-related quality of life in patients served by the department of veterans affairs: results from the health study. Arch Intern Med 158(6):626–632. https://doi.org/10.1001/archinte.158.6.626
Khan M, Evaniew N, Bedi A et al (2014) Arthroscopic surgery for degenerative tears of the meniscus: a systematic review and meta-analysis. CMAJ 186(14):1057–1064. https://doi.org/10.1503/cmaj.140433
LeBrun DG, Martino B, Biehl E et al (2022) Telerehabilitation has similar clinical and patient-reported outcomes compared to traditional rehabilitation following total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 30(12):4098–4103. https://doi.org/10.1007/s00167-022-06931-6
Markström JL, Grinberg A, Häger CK (2022) Fear of reinjury following anterior cruciate ligament reconstruction is manifested in muscle activation patterns of single-leg side-hop landings. Phys Ther 102(2). https://doi.org/10.1093/ptj/pzab218
Moffet H, Tousignant M, Nadeau S et al (2015) In-home telerehabilitation compared with faceto-face rehabilitation after total knee arthroplasty: a noninferiority randomized controlled trial. J Bone Joint Surg 97(14):1129–1141. https://doi.org/10.2106/JBJS.N.01066
Moock J, Kohlmann T, Zwingmann C (2006) Patient-reported outcomes in rehabilitation research: Instruments and current developments in Germany. J Public Health 14(6):333–342. https://doi.org/10.1007/s10389-006-0065-1
Moreira JMA, Grilo EN (2019) Quality of life after coronary artery bypass graft surgery - results of cardiac rehabilitation programme. J Exercise Rehab 15(5):715–722. https://doi.org/10.12965/jer.1938444.222
Moreira J, Mesquita M, Flamínio J, de Almeida M, Delgado B, Boto P (2024) Patient-reported outcome measures in knee injuries rehabilitation: a protocol for intervention. MethodsX 12:102647. https://doi.org/10.1016/j.mex.2024.102647
Munn Z, Stone JC, Aromataris E et al (2023) Assessing the risk of bias of quantitative analytical studies: introducing the vision for critical appraisal within JBI systematic reviews. JBI Evidence Synthesis 21(3):467–471. https://doi.org/10.11124/JBIES-22-00224
Nguyen AT, Aris IM, Snyder BD et al (2024) Musculoskeletal health: an ecological study assessing disease burden and research funding. Lancet Region Health 29. https://doi.org/10.1016/j.lana.2023.100661
Page MJ, McKenzie JE, Bossuyt PM et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372(71). https://doi.org/10.1136/bmj.n71
Park MS, Kang KJ, Jang SJ et al (2018) Evaluating test-retest reliability in patient-reported outcome measures for older people: a systematic review. Int J Nurs Stud 79:58–69. https://doi.org/10.1016/j.ijnurstu.2017.11.003
Perez JL, Mosher ZA, Watson SL et al (2017) Readability of orthopaedic patient-reported outcome measures: is there a fundamental failure to communicate? Clin Orthop Relat Res 475(8):1936–1947. https://doi.org/10.1007/s11999-017-5339-0
Rolfson O, Eresian Chenok K, Bohm E et al (2016) Patient-reported outcome measures in arthroplasty registries: report of the patient-reported outcome measures working group of the international society of arthroplasty registries: part I. Overview and rationale for patient-reported outcome measures. Acta Orthop 87:3–8. https://doi.org/10.1080/17453674.2016.1181815
Roos EM, Roos HP, Lohmander LS et al (2024) Knee injury and osteoarthritis outcome score -development of a self-administered outcome measure. JOSPT J Orthop Sports Phys Ther 78(2)
Schache MB, McClelland JA, Webster KE (2019) Incorporating hip abductor strengthening exercises into a rehabilitation program did not improve outcomes in people following total knee arthroplasty: a randomised trial. J Physiother 65(3):136–143. https://doi.org/10.1016/j.jphys.2019.05.008
Terradas-Monllor M, Navarro-Fernández G, Ruiz MA et al (2021) Postoperative psychosocial factors in health functioning and health-related quality of life after knee arthroplasty: a 6-month follow up prospective observational study. Pain Med 22(9):1905–1915. https://doi.org/10.1093/pm/pnab025
Tricco A, Langlois E, Straus S (2017) Rapid reviews to strengthen health policy and systems: A pratical guide. World Health Organization
Truong LK, Mosewich AD, Holt CJ et al (2020) Psychological, social and contextual factors across recovery stages following a sport-related knee injury: a scoping review. British J Sports Med 54(19):1149–1156. https://doi.org/10.1136/bjsports-2019-101206
Van Beest W, Boon WPC, Andriessen D et al (2022) Successful implementation of self-management health innovations. J Public Health 30(3):721–735. https://doi.org/10.1007/s10389-020-01330-y
Vos T, Lim SS, Abbafati C et al (2020) Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396(10258):1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
Funding
Open access funding provided by FCT|FCCN (b-on). The present publication was funded by Fundação Ciência e Tecnologia, IP national support through CHRC (UIDB/04923/2020).
Author information
Authors and Affiliations
Contributions
JM and SM conceptualized the study, developed the research protocol, identified articles for full-text review, extracted data from studies that met the inclusion criteria, synthesized, and analyzed the data. JM wrote the manuscript. All authors approved the final submitted version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study was submitted and approved by the Ethics Committee of the Nacional School of Public Health – NOVA University of Lisbon (CE-ENSP n°3/2022). This work is a rapid systematic review and thus no ethical approval is required.
Consent to participate and publish
All analyzed studies were responsible for acquiring written informed consent from the respective participants.
Consent for publication
All analyzed studies were responsible for acquiring written informed consent from the respective participants.
Competing interests
The authors have no conflicts of interest that are relevant to declare for the study that was designed.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Moreira, J., Miguel, S., Delgado, B. et al. Patient-reported outcome measures in rehabilitation after knee surgery: a rapid systematic review. J Public Health (Berl.) (2024). https://doi.org/10.1007/s10389-024-02283-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-024-02283-2