
Abstract
Being out of HIV care (OOC) is associated with increased morbidity and mortality. We assessed implementation of Lost & Found, a clinic-based intervention to reengage OOC patients. OOC patients were identified using a nurse-validated, real-time OOC list within the electronic medical records (EMR) system. Nurses called OOC patients. Implementation occurred at the McGill University Health Centre from April 2018 to 2019. Results from questionnaires to nurses showed elevated scores for implementation outcomes throughout, but with lower, more variable scores during pre-implementation to month 3 [e.g., adoption subscales (scale: 1–5): range from pre-implementation to month 3, 3.7–4.9; thereafter, 4.2–4.9]. Qualitative results from focus groups with nurses were consistent with observed quantitative trends. Barriers concerning the EMR and nursing staff shortages explained reductions in fidelity. Strategies for overcoming barriers to implementation were crucial in early months of implementation. Intervention compatibility, information systems support, as well as nurses’ team processes, knowledge, and skills facilitated implementation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Identifying and reengaging out of HIV care (OOC) patients is important for optimizing engagement along the HIV care continuum [1, 2]. OOC patients experience greater morbidity and mortality [3,4,5], and increased risk of HIV transmission due to unsuppressed viral loads [6, 7]. Identifying and reengaging OOC patients requires consistent updates to patient data, including changes in living situation, HIV care, and contact information, which are often difficult to maintain [8]. Moreover, imprecise OOC definitions erroneously identify patients with valid reasons for not presenting to clinic, such as having changed care providers, moved away, or died, resulting in unnecessary efforts to reengage patients who are not actually OOC [8,9,10,11,12,13]. Methods to overcome these challenges include using large multi-jurisdictional datasets or data-sharing agreements, but these may be impeded by legal, financial, or infrastructural barriers [14,15,16,17]. Adapting existing, evidence-informed, clinic-based approaches for patient reengagement offers a viable alternative [18, 19].
Clinic-based approaches show promise for reengaging OOC patients [18, 19]. In addition to promoting patient reengagement, such efforts improve accuracy of patient care statuses and enhance overall data quality in clinical databases [8, 18,19,20]. However, beyond improvements in data quality, no studies have reported metrics to guide implementation of clinic-based reengagement interventions, nor have any been designed with an explicit focus on implementation [17]. Implementation science methods could help identify and mitigate challenges inherent to adopting such reengagement interventions [21].
Lost & Found is a clinic-based intervention for reengaging OOC patients, created and implemented at the Chronic Viral Illness Service of the McGill University Health Centre (CVIS-MUHC) [22, 23]. Lost & Found was designed to be adapted to varying contexts, and has successfully improved OOC patient reengagement at the CVIS-MUHC [23]. Insights gained from its implementation could guide efforts to adapt similar interventions elsewhere. We evaluated implementation of Lost & Found through mixed methods, describing quantitative trends in implementation outcomes and using qualitative data on implementation barriers and facilitators to provide additional context [24].
Methods
Lost & Found
Lost & Found consists of two core, evidence-based elements: identifying and contacting OOC patients (Fig. 1) [10, 18, 19, 22, 25, 26]. To identify OOC patients, we integrated an OOC risk prediction tool (OOC-RPT) into a pre-existing electronic medical records (EMR) database. The OOC-RPT uses clinical information (e.g., HIV-related lab results and demographic information) to automatically classify patients into high, intermediate, or low risk of negative HIV-related health outcomes and, based on this classification, as “potentially OOC” after 3, 6, or 12 months from their last HIV care visit, respectively [27, 28]. Specific criteria used to determine risk levels are detailed in Fig. 1. Potential OOC patients are organized into an “OOC list” to be reviewed by nurses who validate individual OOC statuses, based on their knowledge of a given patient’s sociodemographic, psychosocial, clinical, or other factors (Fig. 2). Nurses contact patients confirmed as OOC and document reengagement efforts in an HIV follow-up module we created in the database (Fig. 3). Nurses received training in motivational communication to facilitate patient reengagement.

Schematic of the full Lost & Found intervention

Out-of-care list built into the clinical electronic medical record database. Note Only fictional patient data are presented in this figure

HIV care module built into the clinical electronic medical record database. Note Only fictional patient data are presented in this figure
Lost & Found was implemented at the CVIS-MUHC in Montréal, Canada over a 12-month period beginning in April 2018 [22]. A protocol outlining complete details of the intervention, its development, implementation strategies, and implementation frameworks is published elsewhere [22]. However, relevant information for this analysis is provided herein. We selected three implementation strategies to encourage uptake and sustainability of Lost & Found: (i) promote adaptability, wherein we differentiated core elements, critical to the intervention’s intent and effectiveness, from peripheral components, which can be adapted or adjusted [21, 29, 30]; (ii) planning, engaging, executing, evaluating, and reflecting (PEEER) cycles, or ‘cyclical tests of change,’ to adapt peripheral components of the intervention [21, 30]; and (iii) internal facilitation, whereby a study coordinator worked with stakeholders (nurses, primary investigators, database manager and developer) to identify and mitigate barriers to implementation [29, 30].
Study Design
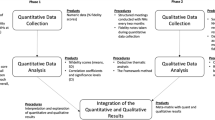
This mixed-methods assessment of Lost & Found was conducted as part of a type II implementation-effectiveness hybrid study, where intervention effectiveness and implementation were given equal consideration [22, 31]. A completed Standards for Reporting Implementation Studies (StaRI) checklist is provided in Supplementary material 1 [32]. In a prior evaluation of the intervention’s effectiveness, we demonstrated that OOC patients were more likely to reengage and to do so earlier in the context of Lost & Found [23]. In the current assessment, we used a convergent explanatory sequential mixed-methods design to evaluate its implementation (Fig. 4) [22, 33, 34]. Qualitative and quantitative data were collected in parallel, then qualitative data were analyzed and used to contextualize quantitative findings.

Convergent explanatory sequential mixed-methods design
Data Collection and Analysis
Study participants included all nurses working at the CVIS-MUHC (n = 5), those responsible for administering the Lost & Found intervention. Quantitative and qualitative data collection at each time point are described in Table 1. Data collection tools are provided in Supplementary material 2 and details regarding the number of focus group discussions and related participation by nurses are provided in Supplementary material 3.
Quantitative Data
Four implementation outcomes were studied: (i) feasibility, (ii) acceptability, (iii) adoption, and (iv) fidelity [35]. A thirty-six item questionnaire (i–iii) and fidelity checklist (iv) were administered to nurses at pre-implementation (1 month before implementation) and months 1, 2, 3, 6, and 12. Scales for feasibility and acceptability were inspired by the feasibility of implementation measure (FIM) and acceptability of implementation measure (AIM), respectively [36]. Adoption was measured using scales from the Service Provider Adopter and Innovation Characteristics Questionnaire (SPAICQ) [37, 38]. Content validity, discriminant content validity, reliability, structural validity, structural invariance, known-groups validity, and responsiveness to change have been demonstrated for FIM and AIM, but predictive validity assessments are ongoing [36]. Overall, the SPAICQ rates as excellent for norms and good for usability [39]. Predictive validity is considered good for the SPAICQ adopter characteristics subscale, but minimal for the innovation characteristics subscale [39].
Feasibility and acceptability were measured separately for Lost & Found’s core elements (identifying OOC patients, contacting patients), while adoption was measured for the full intervention. Feasibility, acceptability, and adoption were captured via 5-item agreement scales and scored from one to five, where a score of one indicates complete disagreement, and a score of five, complete agreement. We created and administered a short checklist to assess fidelity to intervention components that could not be collected through EMRs (e.g. adherence to motivational communication techniques). These were scored on scales from zero to one, where a score of zero indicated either an answer of “no” to using the intervention component or “never” using it as intended, while a score of one indicated an answer of “yes” to using the intervention component or using it as intended “most of the time”. Scores are typically presented as the mean for all nurses at a given time point. When discussing scores across time points, we took the median and inter-quartile range (IQR).
Additional patient-level data from the implementation phase (months 1–12) were extracted from EMRs to further inform nurses’ fidelity to intervention components. Extracted data include the number of individuals identified as potentially OOC and, among those, the number validated by nurses, confirmed OOC, and who received contact attempts. Only patients with clinic visits within 5 years of the start of implementation and during implementation were included. We present monthly totals for each patient-level fidelity outcome.
Qualitative Data
Focus Groups One-hour audio-recorded focus group discussions were held with nurses in pre-implementation and months 1, 2, 3, 6, and 12, led by DL. Discussions took place in English and were guided by a semi-structured interview schedule. The study coordinator (BL1) was in attendance to learn about and, following the focus group discussions, address barriers to implementation mentioned throughout. BL1 and DL independently coded verbatim transcriptions of recordings in NVivo-12 using deductive content analysis [40, 41]. Transcripts were reviewed and coded for correspondence with items in the Tailored Implementation for Chronic Diseases (TICD) checklist, a comprehensive list of 57 implementation determinants (i.e. barriers and facilitators) [42]. Discrepancies were resolved by consensus.
Logbook Information about important events or conversations between stakeholders were recorded in a logbook by the study coordinator and used to further contextualize focus group results.
Mixed Methods
To triangulate quantitative and qualitative data, we developed a convergence coding matrix to map TICD determinants onto implementation outcomes (Supplementary material 4) [42]. This process was guided by a simplified version of a causal chain we developed to understand the relationship between implementation outcomes and overall effectiveness (Fig. 5) [22, 35, 37, 43, 44].

Simplified causal chain for study outcomes
The causal chain describes how each implementation outcome acts as an intermediate between upstream implementation outcomes and intervention effectiveness. Upstream implementation outcomes such as feasibility and acceptability are fundamental to adoption, fidelity, and ultimately effectiveness [22]. Determinants directly impacting an upstream implementation outcome indirectly impact downstream outcomes, but do not impact upstream ones. For example, if implementation stakeholders do not accept the intervention, it could still be inherently feasible to implement, but the lack of acceptability will prevent them from adopting it, ultimately rendering it ineffective.
Mixed-methods analyses were first performed by BL1, who explored trends in implementation outcomes using focus groups results, further contextualized by the logbook. To quantify the importance of a theme, we examined coverage, defined as the proportion of words coded as aligning with a determinant, a useful proxy when there is a large number of potential codes, as was the case in this study due to the large number of determinants [41, 45]. The top 10 barriers and facilitators discussed across focus groups, as determined by their coverage, were prioritized to explain quantitative trends, supported by the convergence coding matrix. Notably, determinants could act as both barriers and facilitators. Transcripts were reviewed again, and other potentially important events not identified in the 10 barriers and facilitators were considered. BL1 provided an inclusive account of potentially important determinants and events, after which they were collectively reviewed by BL1, DL, and JC to determine which best explained trends in implementation. Disagreements were resolved by consensus. TICD determinants are italicized throughout the text.
Results
The following sections describe patterns for each implementation outcome. These results are triangulated and explained by findings from qualitative content analyses. Supplementary material 5 summarizes how each determinant impacted implementation outcomes during implementation.
Feasibility
For each core element of the intervention (identifying OOC patients, contacting patients), nurses’ feasibility scores were lower and more variable in early study months (pre-implementation to month 3), followed by higher scores in later months (months 3–12) (Fig. 6). In pre-implementation, nurses perceived managing the OOC list to be less feasible (score of 3.6), but this outcome improved throughout implementation (median 4.4; IQR: 4.3–4.4), with a slight decline in month 2 to a score of 4.2. Conversely, in pre-implementation, nurses perceived phone calls as more feasible (score of 3.8) than managing the OOC list but reported lower feasibility in month 1 (score of 3.5). In month 3, feasibility of phone calls plateaued at 4.2, just below perceived feasibility of the OOC list.

Feasibility and acceptability of the phone calls and OOC list, all nurses by study month
Determinants directly impacting feasibility dominated focus group discussions. These included nature of the behaviour, information systems, assistance for organizational changes, compatibility, availability of necessary resources, and patient behaviours, needs, and preferences.
For identification of OOC patients, nurses recognized the inherent characteristics of this task (i.e. nature of the behaviour) as an important barrier during the pre-implementation focus group. They knew they would have to confirm statuses of patients on the OOC list on a case-by-case basis, many of whom would no longer be in care due to changing clinics or relocating to another jurisdiction.
Assuming in the beginning, there’ll be a long list of patients, we probably won’t be able to get through them all right away.
-Nurse 1, pre-implementation
This concern likely contributed to low feasibility scores for managing the OOC list in pre-implementation. To make the list more manageable, following consultation with nurses and primary investigators, at the start of implementation the study coordinator removed patients without a visit in five years. Despite this, nurses had to assess the OOC status of 862 patients remaining on the list. The coordinator’s involvement in this matter, and support from clinical leadership who made temporary nurses available to conduct other day-to-day tasks, provided the necessary resources to facilitate “cleaning” the OOC list and implementation overall. Improvements to information systems (i.e., EMRs) also played an important role in implementation, including nurses’ views of the intervention as efficient, helping make reengagement easier and more sustainable.
We’ll be able to [identify patients] more systematically. We’ll be able to catch more that otherwise might fall through the cracks.
– Nurse 1, pre-implementation
Consequently, nurses’ views of the OOC list in month 1 are mostly positive, and feasibility scores increased after pre-implementation. However, perhaps due to the central role of the EMR database in Lost & Found implementation, information systems-related barriers were among the most frequently discussed, particularly in early implementation. For example, before the month 2 focus group, to improve functioning of the OOC list, the study coordinator changed how “HIV care visits” were defined such that laboratory measures without consultation with a member of the clinical team were no longer considered. This change resulted in a significant increase in the number of patients on the OOC list and likely contributed to the concomitant decline in feasibility scores. However, nurses acknowledged that many barriers, especially for information systems, were addressed by notifying the study coordinator, who provided assistance for organizational changes related to any aspect of the project:
[The study coordinator] is responsive and answers quickly. If there’s a solution, there’s usually something that’s found pretty quickly.
-Nurse 1, Month 3
By collaborating with the primary investigators, database manager, and other clinical staff, the study coordinator ensured that essential software updates were installed when problems arose. Ten updates to the EMR database were installed in the first 4 months, compared to three in the remaining eight. Only one update was made after month 7, and it had no impact on monitoring or reengaging OOC patients. Timing of these changes is consistent with lower and more variable scores for feasibility in early versus later study months. Supplementary material 6 contains a full history of intervention-related changes to the database.
Once identified, nurses attempted to reengage OOC patients with a phone call. Compatibility of this part of the intervention was consistently recognized as a facilitator. Before Lost & Found, nurses made their own efforts to call patients perceived as potentially OOC, likely contributing to compatibility of the intervention and potentially explaining higher pre-implementation feasibility scores for phone calls compared to managing the OOC list. Nurses explained that, before the intervention, they had invested time into reengaging patients they perceived as OOC, but that Lost & Found helped them accomplish this task more effectively:
We were already doing phone calls before; it’s part of the job. It’ll just be easier to do than before.
-Nurse 2, Month 6
Nurses considered monitoring and reengaging OOC patients as central to their nursing responsibilities and consistent with the culture of the clinic, further contributing to compatibility.
Availability of necessary resources was a frequently discussed barrier. Limited nursing resources remained a recurring issue throughout implementation:
If one of us is on vacation there’s only three of us. Then we’re busy enough with just the clinic stuff that we won’t necessarily have time to do it.
-Nurse 3, Month 12
This barrier may have contributed to lower feasibility scores throughout, including the decline from pre-implementation to month 1, when one nurse was absent.
Nurses also highlighted patient behaviours, needs, and preferences as barriers. For instance, some patients would not present despite a planned appointment. Nurses acknowledged that the main barriers preventing reengagement stemmed from challenges patients faced in their day-to-day lives. For example, until month 9, nurses were selecting “Other” over “Unwilling to engage in care” as the outcome of their reengagement efforts when patients refused reengagement, because they felt that “unwilling” was a misrepresentation of barriers faced by patients in accessing health care:
If they live far, if they have to ask to have time off, [… if they have to] get home in time to pick up kids from school, it constrains people into a small window that they can come to the clinic.
-Nurse 1, Month 6
Some of the barriers mentioned included non-HIV-related health issues, family and work responsibilities, as well as transportation issues.
Nurses also frequently expressed concern about potentially making patients feel confronted or guilty about their absences from care. It was feared this may discourage patients from reengaging altogether:
I’m trying not to confront them. I’m trying to be positive.
-Nurse 4, Month 2
Similar patient-related challenges persisted throughout the study, likely contributing to lower feasibility scores for phone calls compared to managing the OOC list.
Acceptability
Acceptability scores were high throughout the entire study, with patterns in acceptability of the OOC list and phone calls similar to those observed for feasibility (Fig. 6). A deviation from this pattern was observed in pre-implementation when the average acceptability score for managing the OOC list (4.88) was higher than for phone calls (4.71), while the average feasibility score for the OOC list (3.58) was lower than for phone calls (3.83). After pre-implementation, acceptability scores for the OOC list declined to their lowest in month 2 (average 4.62), then increased to their highest in month 3 (average 4.95). This decline mirrors the concomitant fall in feasibility scores. Thereafter, scores remained above 4.75 until study completion. Similar to feasibility scores, acceptability scores for phone calls decreased from pre-implementation (average 4.71) to month 1 (average 4.33) before plateauing near 4.7 in month 3.
Observability of the intervention was the most frequently reported facilitator directly affecting acceptability. Nurses consistently highlighted benefits of seeing the OOC list in real-time, including the categorization of patients into different risk categories, while simultaneously acknowledging limitations in functionality of the OOC list and related information systems in early implementation.
Little nicks in [the database] but generally it’s good. It’s kind of exciting to see when it works. When it pops up a name at the top and you say: ‘Oh, yes, that’s definitely an [out-of-care] patient’
-Nurse 1, Month 1
As an added facilitator of acceptability, nurses were among the primary sources of the recommendation, meaning they were central in developing Lost & Found, and relied upon previous reengagement efforts to do so. Nurses were frequently consulted in pre-implementation to ensure that proposed adaptations met their needs. Across focus groups, they made statements such as the following:
I’m looking forward to it. We’ve been asking for something. We’re always doing it anyways but hopefully with the tool, it’ll be more systematic.
-Nurse 1, pre-implementation
The central role of nurses likely contributed to high acceptability scores throughout the study and may explain why perceived acceptability scores consistently exceeded perceived feasibility across focus groups.
Nurses’ experience with patient reengagement, and their role in Lost & Found development, may also explain the discordance between pre-implementation acceptability and feasibility scores for the OOC list. Specifically, nurses may have been happy with its purpose (acceptability), but skeptical about how it would actually work (feasibility). The concordance in acceptability and feasibility trends for the OOC list during implementation suggests their pre-implementation concerns were adequately addressed.
Adoption
High levels of adoption were observed throughout the study (median score across subscales 4.4; IQR: 4.2–4.7), with more variability in pre-implementation to month 3 (range of scores from pre-implementation to month 3, 3.7–4.9; thereafter, 4.2–4.9) (Fig. 7). For all adoption subscales, average scores were higher in month 12 (median 4.7; IQR: 4.5–4.8) than in pre-implementation or month 1 (median 4.2; IQR: 4.1–4.6). We observed three general patterns for adoption subscales: (i) high “concern for OOC patients” scores were seen throughout the entire study (median: 4.8; IQR: 4.8–4.9); (ii) nurses’ self-efficacy and overall acceptability of Lost & Found dropped slightly in months 1 and 2 from pre-implementation (mean decrease of 0.24), then increased in month 3 (mean increase of 0.25); (iii) attitudes toward Lost & Found, its relative advantage compared to standard practice, and overall feasibility increased throughout the study from their lowest levels in pre-implementation to their highest in month 12 (median increase 0.58; IQR: 0.53–0.62), with some minor fluctuations throughout. The two aggregate adoption scales, adopter characteristics (an average of attitude, concern, and self-efficacy) and innovation characteristics (acceptability, feasibility, and relative advantage), each followed the third pattern (median increase of 0.35 from pre-implementation; IQR: 0.31–0.40). Consistent with the causal chain of implementation outcomes, patterns in adoption scores were consistent with those observed for feasibility and acceptability—slight declines in months 1 and 2, followed by either an increasing trend or consistently high scores.

Adoption subscales for Lost & Found, all nurses by study month
These trends seem to be largely explained by determinants impacting upstream implementation outcomes. For example, declines in self-efficacy in the first 2 months of implementation were likely related to feasibility, more specifically, nurses’ concerns about their ability to schedule patients with their doctors, related to the availability of necessary resources and referral process determinants:
Summer is coming so it’s been harder now because, for most doctors, the next availability is in [two months]. The longer it takes for an appointment, the less chance we have for the patient to show.
-Nurse 2, Month 2
However, two determinants, domain knowledge and skills needed to adhere, were among the most frequently discussed facilitators to adoption. Here, “domain knowledge” refers to nurses’ knowledge about OOC patients and HIV in general. Nurses at the CVIS-MUHC specialize in HIV care, meaning these two determinants likely exerted strong positive effects on adoption throughout. For example, patients could be prematurely identified by the EMR database when their upcoming appointments were just outside of the risk-category-specific window for amount of time since their previous clinical visit; a patient in the high-risk category with an upcoming appointment in 3 months and 1 week after their last clinical visit would be identified by the database as of the 3-month mark until they successfully attended their appointment or were removed from the OOC list. Nurses had strong existing relationships with many OOC patients, allowing them to differentiate truly OOC patients from those who were erroneously or prematurely identified by the EMR database, which they anticipated would facilitate adoption of the intervention:
There [are] so many patients that we could quickly remove just by looking at the list: ‘Oh, he’s at another clinic, he’s there, he’s there.’
-Nurse 2, pre-implementation
As highlighted when discussing feasibility, nurses’ domain knowledge also meant they understood many of the barriers faced by patients in remaining engaged in care, such as competing priorities and essential needs related to work or family responsibilities. This is reflected in their consistently high levels of concern for OOC patients. Their understanding of OOC patients likely contributed to their skills in reengaging patients over the phone, and ultimately their self-efficacy in encouraging patient reengagement:
[Patients] don’t know [nurse 2], but when she calls, she’s open and people feel a little more inclined to want to come back.
-Nurse 1, Month 6
Fidelity
Fidelity outcomes from patient-level data from EMRs are presented in Fig. 8. The number of patients on the OOC list declined from its peak of 862 in month 1 to a plateau (median 290; IQR: 281–310) beginning in month 5. Similarly, the highest number of patients were validated by nurses in the first 5 months, with a peak of 440 in month 2, followed by a plateau starting at month 6 (median 190; IQR:180–196). There were noticeable declines in patients validated in months 3 and 8. The number of patients confirmed as OOC, and subsequently called by nurses, was relatively stable across the study, following a similar pattern to the number of patients validated by nurses. True OOC patients made up an increasing proportion of patients on the list over the study. In month 1, true OOC patients made up only 12% of patients, compared to an average of 47% in months 5 to 12. Similar patterns were observed when stratified by risk category (Supplementary material 3). The number of calls made by nurses each month are presented in Fig. 9. One nurse, nurse 2, made 92.1% (1464/1589) of the calls throughout the study. This nurse reported consistently high adherence to the general principles of motivational communication, particularly empathetic, non-directive, and informative communication (Fig. 10). The other four nurses completed a maximum of 41 and a median of 7.5 [IQR: 2.5–12.5] calls in any given month. Nurses completed the fewest calls in months 3 and 8, consistent with lower validation rates during these months. All nurses reported using the OOC list and HIV follow-up module (where reengagement efforts are documented) throughout the study (Fig. 11). Increasingly over the study period, nurses used the OOC list as intended, defined as prioritizing patients with the longest clinical absences in the highest risk categories. Nurses tended to report using the HIV follow-up module as intended “some of the time” (mean score 0.67), where “as intended” is defined as conducting all reengagement activities in the EMR database and not elsewhere.

Fidelity outcomes from patient-level data in EMRs

Number of phone calls made, all nurses by month

Fidelity to motivational communication principles, Nurse 2* by study month. *Nurse 2 made 92.1% (1464/1589) of the phone calls throughout the study

Use and adherence to the OOC list and HIV follow-up module, all nurses by study month
Based on the qualitative analyses, nurses’ knowledge of their own practice was the most frequently occurring facilitator of fidelity. This allowed them to overcome inherent limitations to the EMR database and obtain patient information from other sources such as health registries. Similarly, nurses’ team processes facilitated fidelity to other aspects of Lost & Found. The five nurses emphasized a shared mandate, with individual, overlapping responsibilities:
We have different responsibilities. I think we manage to work it out amongst each other. There’s no clear division, we try to help each other.
- Nurse 4, month 12
Initial management and ‘clean-up’ of the OOC list were accomplished as a group, but nurse 2 remained primarily responsible for OOC patient reengagement throughout the study. This division of labour occurred naturally, with nurses insisting that no specific nurse be formally assigned to lead reengagement efforts. Notably, despite the disparity in phone calls made, across all implementation outcomes, scores are relatively consistent between nurses (Supplementary material 3).
As with adoption, observed trends in fidelity are largely explained by determinants impacting upstream implementation outcomes (feasibility, acceptability, and adoption). For example, there was a decrease in the number of patients validated, confirmed as OOC, and called (e.g. in months 1 and 3) when any nurse, especially nurse 2, was sick or on vacation, limiting the availability of necessary resources. In such instances, the remaining nurses would prioritize reengagement of high-risk patients, if any.
Similarly, information systems, an important determinant acting through feasibility, also impacted fidelity scores. For example, the increasing trend in use of the OOC list as intended is consistent with database improvements over the course of implementation, suggesting these changes facilitated fidelity. Information systems as a barrier also explains other trends in fidelity. For example, in month 8, two nurses were unable to access EMRs on their computers due to hospital server upgrades, ultimately leading to a concomitant decline in validated patients (Fig. 8). While nurses were able to access the software in subsequent months, access was inconsistent and not completely resolved until after implementation, when new computers were installed. Similarly, use of the HIV follow-up module as intended only “some of the time” (Fig. 11) likely reflects inherent limitations of data in the EMR database, forcing nurses to search elsewhere for patient information.
Finally, nurses’ focus on accommodating patients likely contributed to high levels of adherence to the general principles of motivational communication. Notably, they viewed these principles as part of their expertise as nurses, not necessarily as part of motivational communication.
Discussion
In this mixed-methods study, we examined implementation of an evidence-informed clinical intervention to reengage people living with HIV into care. To our knowledge, this is the first study to employ an implementation science or mixed-methods approach to clinic-based HIV care reengagement [17]. We found initial months to be crucial to successful implementation, while later months were essential to improving the fit of the intervention for the clinic. This is consistent with Proctor’s proposed salience of implementation outcomes, whereby early implementation is considered a critical time period for measurement and adaptation [35]. These findings are also consistent with other studies finding improved clinical data as a major benefit of HIV patient reengagement or retention efforts [8, 20]. As nurses validated patients’ OOC statuses over time, automated portions of our OOC definition became more specific, easing the burden on nurses.
Our results demonstrate that implementation of Lost & Found was rooted in the three selected implementation strategies: promoting adaptability, internal facilitation, and PEEER cycles. Packaging the intervention into peripheral components and core elements allowed us to delineate which aspects could be adapted, and which should remain untouched, respectively. Any aspect of the intervention adapted to the clinic or changed throughout implementation represents a peripheral intervention component. This strategy was apparent across adaptations, including changes to the EMR database and OOC criteria. Internal facilitation and PEEER cycles also played important roles in adapting the intervention. During early implementation, the study coordinator worked with various implementation stakeholders to ensure that timely changes to peripheral components were implemented. Nurses acknowledged that internal facilitation was a useful resource in addressing barriers to implementation. These changes were possible because the study coordinator was given resources to implement necessary changes, including finances for a software developer and support from clinical leadership to engage with stakeholders in addressing unanticipated challenges. This flexibility allowed the study coordinator to document, resolve, and monitor issues in a manner consistent with informal PEEER cycles conducted throughout [21]. Notably, a study coordinator acted as our internal facilitator, but other clinics might consider assigning this role to another member of the clinical team. We chose a study coordinator as they had no competing clinical responsibilities, but this may have come at the expense of closer contact with nurses.
Some determinants, such as information systems and availability of necessary resources, appeared to be directly tied to events impacting implementation outcomes, as demonstrated by decreases in the number of patients validated by nurses in months 3 and 8. Reengagement interventions tend to require significant effort and resources, meaning availability of necessary resources is likely to be pertinent regardless of where Lost & Found is implemented [11, 16, 46]. The predominance of information systems as a determinant in our clinic was likely related to our strategy to overcome the resource-intensive nature of identifying OOC patients and documenting reengagement efforts. Specifically, our OOC definition placed technology at the center of our approach. This is exemplified by the decline in patients validated in month 8; problems with accessing or the software itself prevented or limited reengagement activities. While information systems would be a less important determinant in clinics adopting Lost & Found with an OOC definition less dependent on technology, a new set of challenges would arise that were mitigated using our approach. For example, nurses requested a more complex OOC definition with a low threshold for identification, to ensure a larger proportion would be captured. With our approach, we could integrate their request into the EMR and automate some of their work. A simpler and higher threshold definition, such as one considering only patients with 12-month absences as OOC, could be less dependent on technology and potentially reduce nurses’ workload, at the expense of depriving some OOC patients from receiving reengagement efforts. Clinics using a different OOC definition would have to find ways to overcome its limitations, including how it is operationalized and accepted by clinical staff. Conversely, for contacting patients, some clinics may opt for additional methods, including text messages or emails. These strategies have been employed in other reengagement studies and warrant further study [17].
Other determinants seemed to have exerted their effects before data collection. Multiple discussions were had between implementation stakeholders that may have played an important role in tailoring the intervention to the clinic. The first formal meeting between nurses and primary investigators occurred in March 2017, just over a year before the start of implementation and data collection. Determinants such as compatibility and source of the intervention were discussed frequently across focus groups, but likely exerted their effects on implementation outcomes in these early stages of Lost & Found conception and development, helping to adapt the intervention for eventual implementation. Similarly, other determinants rarely mentioned throughout focus groups, such as quality of evidence supporting the recommendation, may have been important, but not discussed because they were considered obvious and inherent to discussions that occurred before data collection. In September and October 2017, we completed modified versions of the worksheets from the TICD framework to select our implementation strategies as a function of potential barriers and facilitators to successful implementation [22, 42]. This process may have allowed us to avoid certain barriers and capitalize on facilitators present in our clinic, allowing us to establish a foundation for the intervention throughout implementation. Our high pre-implementation scores may partially reflect this work done a priori. For example, observability of the OOC list was prioritized early in Lost & Found development and was a frequently mentioned facilitator across focus groups. It may be important to achieve high implementation scores in pre-implementation to tolerate a decline in early implementation, when most adaptation occurs.
While results of this study could help guide implementation of Lost & Found in different contexts, there are some notable limitations. First, this study was conducted at a single site, a multidisciplinary clinic in a publicly-funded quaternary care hospital in Canada. Some of our findings may not be generalizable to clinics with fewer financial or human resources, perhaps facing barriers not discussed here. Second, our findings are drawn from a small sample of stakeholders, which could further limit generalizability of our findings. We attempted to overcome this by corroborating findings from multiple data types and sources, including questionnaires, focus groups, and the facilitator’s logbook. Third, the scales used to measure implementation outcomes (FIM, AIM, and SPAICQ) are relatively new, and evidence regarding their validity and reliability is still accumulating [36, 39]. Fourth, some changes initiated and implemented without involvement from the study coordinator, or not mentioned in focus groups by nurses, may not have been accounted for or documented in this analysis. These could include changes in the distribution of work between nurses or their approach to phone calls. For example, despite nurses having collectively requested a shared responsibility for Lost & Found tasks and preferring to not assign a primary “Lost & Found nurse”, over time, we observed that one nurse made the large majority of phone calls to OOC patients. Fifth, CVIS-MUHC nurses were highly motivated to reengage OOC patients, even prior to Lost & Found. This strong facilitator for implementation may limit the generalizability of our findings to clinics with less buy-in from implementation stakeholders. Finally, our overall approach to this assessment focused solely on service providers, recognizing their essential role in implementation-related adaptations in order to, ultimately, improve patient outcomes. This approach aligns with Proctor’s evaluation framework for implementation research, whereby implementation outcomes are fundamental to service outcomes (e.g. effectiveness), which themselves influence client outcomes (e.g., patient satisfaction) [35]. A forthcoming analysis of questionnaires administered to patients upon reengagement will explore reasons for OOC to help guide the clinical team in its ongoing efforts to reengage and retain patients.
Conclusions
This study provides important insights into the implementation of Lost & Found, an evidence-informed clinic-based reengagement intervention for OOC patients. Early months of the intervention were crucial for successful implementation. Important determinants of implementation were identified that may influence future efforts to trial this intervention, including information systems, availability of necessary resources, compatibility of the intervention, and health professionals’ skills and knowledge. Implementation strategies were important for overcoming barriers to implementation. These findings could be leveraged to overcome challenges and determine priorities in scaling up Lost & Found for more robust effectiveness and implementation evaluations, including cost-effectiveness studies.
Data Availability
The datasets generated and/or analysed during the current study are not publicly available due to the risk of participants being linked to their statements and the resulting impact on their employment. However, data can be made available from the corresponding author upon reasonable request.
Abbreviations
- HIV:
-
Human immunodeficiency virus
- OOC:
-
Out of HIV care
- CVIS-MUHC:
-
Chronic Viral Illness Service of the McGill University Health Centre
- OOC-RPT:
-
OOC risk prediction tool
- PEEER:
-
Planning, engaging, executing, evaluating, and reflecting
- FIM:
-
Feasibility of implementation measure
- AIM:
-
Acceptability of implementation measure
- SPAICQ:
-
Service Provider Adopter and Innovation Characteristics Questionnaire
- IQR:
-
Inter-quartile range
- TICD:
-
Tailored Implementation for Chronic Diseases
References
Joint United Nations Programme on HIV/AIDS (UNAIDS). Ending AIDS: Progress towards the 90–90–90 targets [Internet]. Geneva, Switzerland; 2017. https://bit.ly/3G9Dwpm
The White House. National HIV/AIDS Strategy for the United States 2022–2025. Washington, DC: The Office of National AIDS Policy (ONAP); 2021. https://bit.ly/3pZJwve
Giordano TP, Gifford AL, White AC Jr, Almazor MES, Rabeneck L, Hartman C, et al. Retention in care: a challenge to survival with HIV infection. Clin Infect Dis. 2007;44(11):1493–9.
Mugavero MJ, Lin HY, Willig JH, Westfall AO, Ulett KB, Routman JS, et al. Missed visits and mortality among patients establishing initial outpatient HIV treatment. Clin Infect Dis. 2009;48(2):248–56.
Kendall CE, Raboud J, Donelle J, Loutfy M, Rourke SB, Kroch A, et al. Lost but not forgotten: a population-based study of mortality and care trajectories among people living with HIV who are lost to follow-up in Ontario, Canada. HIV Med. 2019;20(2):88–98.
Skarbinski J, Rosenberg E, Paz-Bailey G, Hall HI, Rose CE, Viall AH, et al. Human immunodeficiency virus transmission at each step of the care continuum in the United States. JAMA Intern Med. 2015;175(4):588–96.
Krentz HB, Vu Q, Gill MJ. Updated direct costs of medical care for HIV-infected patients within a regional population from 2006 to 2017. HIV Med. 2020;21(5):289–98.
Bove J, Golden MR, Dhanireddy S, Harrington RD, Dombrowski JC. Outcomes of a clinic-based, surveillance-informed intervention to relink patients to HIV care. J Acquir Immune Defic Syndr 1999. 2015;70(3):262.
Buskin SE, Kent JB, Dombrowski JC, Golden MR. Migration distorts surveillance estimates of engagement in care: results of public health investigations of persons who appear to be out of HIV care. Sex Transm Dis. 2014;41(1):35.
Hague JC, John B, Goldman L, Nagavedu K, Lewis S, Hawrusik R, et al. Using HIV surveillance laboratory data to identify out-of-care patients. AIDS Behav. 2019;23(1):78–82.
Fuente-Soro L, López-Varela E, Augusto O, Bernardo EL, Sacoor C, Nhacolo A, et al. Loss to follow-up and opportunities for reengagement in HIV care in rural Mozambique: a prospective cohort study. Medicine (Baltimore). 2020;99:e20236.
Sachdev DD, Mara E, Hughes AJ, Antunez E, Kohn R, Cohen S, et al. “Is a bird in the hand worth 5 in the bush?”: A comparison of 3 data-to-care referral strategies on HIV care continuum outcomes in San Francisco. Open Forum Infect Dis. 2020. https://doi.org/10.1093/ofid/ofaa369.
Krentz HB, McPhee P, Arbess G, Jackson L, Stewart AM, Bois D, et al. Reporting on patients living with HIV “disengaging from care”. Who is actually “lost to follow-up”? AIDS Care. 2021;33(1):114–20.
Sweeney P, Gardner LI, Buchacz K, Garland PM, Mugavero MJ, Bosshart JT, et al. Shifting the paradigm: using HIV surveillance data as a foundation for improving HIV care and preventing HIV infection. Milbank Q. 2013;91(3):558–603.
Gasner MR, Fuld J, Drobnik A, Varma JK. Legal and policy barriers to sharing data between public health programs in New York City: a case study. Am J Public Health. 2014;104(6):993–7.
Fanfair RN, Khalil G, Williams T, Brady K, DeMaria A, Villanueva M, et al. The Cooperative Re-Engagement Controlled trial (CoRECT): A randomised trial to assess a collaborative data to care model to improve HIV care continuum outcomes. Lancet Reg Health-Am. 2021;3: 100057.
Palacio-Vieira J, Reyes-Urueña JM, Imaz A, Bruguera A, Force L, Llaveria AO, et al. Strategies to reengage patients lost to follow up in HIV care in high income countries, a scoping review. BMC Public Health. 2021;21(1):1–11.
Bean MC, Scott L, Kilby JM, Richey LE. Use of an outreach coordinator to reengage and retain patients with HIV in care. AIDS Patient Care STDs. 2017;31(5):222–6.
Keller J, Heine A, LeViere AF, Donovan J, Wilkin A, Sullivan K, et al. HIV patient retention: the implementation of a North Carolina clinic-based protocol. AIDS Care. 2017;29(5):627–31.
Sitapati AM, Limneos J, Bonet-Vázquez M, Mar-Tang M, Qin H, Mathews WC. Retention: building a patient-centered medical home in HIV primary care through PUFF (Patients Unable to Follow-up Found). J Health Care Poor Underserved. 2012;23(3):81–95.
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):1–15.
Cox J, Linthwaite B, Engler K, Lessard D, Lebouché B, Kronfli N. A type II implementation-effectiveness hybrid quasi-experimental pilot study of a clinical intervention to re-engage people living with HIV into care, ‘Lost & Found’: an implementation science protocol. Pilot Feasibility Stud. 2020;6(1):1–11.
Linthwaite B, Kronfli N, Marbaniang I, Ruppenthal L, Lessard D, Engler K, et al. Increased reengagement of out-of-care HIV patients using lost & found, a clinic-based intervention. AIDS Lond Engl. 2021. https://doi.org/10.1097/qad.0000000000003147.
Palinkas LA, Cooper BR. Mixed methods evaluation in dissemination and implementation science. In: Dissemination and implementation research in health: Translating science to practice. New York, NY, USA: Oxford University Press; 2017. p. 335–53.
Udeagu CCN, Webster TR, Bocour A, Michel P, Shepard CW. Lost or just not following up: public health effort to re-engage HIV-infected persons lost to follow-up into HIV medical care. AIDS. 2013;27(14):2271–9.
Wohl AR, Dierst-Davies R, Victoroff A, James S, Bendetson J, Bailey J, et al. Implementation and operational research: the navigation program: an intervention to reengage lost patients at 7 HIV clinics in Los Angeles County, 2012–2014. JAIDS J Acquir Immune Defic Syndr. 2016;71(2):e44-50.
Robbins GK, Johnson KL, Chang Y, Jackson KE, Sax PE, Meigs JB, et al. Predicting virologic failure in an HIV clinic. Clin Infect Dis. 2010;50(5):779–86.
Woodward B, Person A, Rebeiro P, Kheshti A, Raffanti S, Pettit A. Risk prediction tool for medical appointment attendance among HIV-infected persons with unsuppressed viremia. AIDS Patient Care STDs. 2015;29(5):240–7.
Kilbourne AM, Neumann MS, Pincus HA, Bauer MS, Stall R. Implementing evidence-based interventions in health care: application of the replicating effective programs framework. Implement Sci. 2007;2(1):1–10.
Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM, et al. A refined compilation of implementation strategies: results from the Expert Recommendations for Implementing Change (ERIC) project. Implement Sci. 2015;10(1):1–14.
Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217.
Pinnock H, Barwick M, Carpenter CR, Eldridge S, Grandes G, Griffiths CJ, et al. Standards for reporting implementation studies (StaRI) statement. BMJ. 2017;356:i6795.
Watkins D, Gioia D. Fourth floor. Mixed methods research. Oxford: Oxford University Press; 2015.
Cox J, Linthwaite B, Lessard D, Engler K, Lebouché B, Kronfli N. Lost & Found: Interim results from an implementation science pilot study evaluating the implementation and effectiveness of an intervention to re-engage patients into HIV care. In: Canadian Association for HIV Research (CAHR) 2019. Saskatoon. Poster CSP1.01; 2019.
Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health Ment Health Serv Res. 2011;38(2):65–76.
Weiner BJ, Lewis CC, Stanick C, Powell BJ, Dorsey CN, Clary AS, et al. Psychometric assessment of three newly developed implementation outcome measures. Implement Sci. 2017;12(1):1–12.
Henderson JL, MacKay S, Peterson-Badali M. Closing the research-practice gap: factors affecting adoption and implementation of a children’s mental health program. J Clin Child Adolesc Psychol. 2006;35(1):2–12.
Henderson J, Hess M, Mehra K, Hawke LD. From planning to implementation of the YouthCan IMPACT project: a formative evaluation. J Behav Health Serv Res. 2020;47(2):216–29.
Lewis CC, Fischer S, Weiner BJ, Stanick C, Kim M, Martinez RG. Outcomes for implementation science: an enhanced systematic review of instruments using evidence-based rating criteria. Implement Sci. 2015;10(1):1–17.
Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–15.
QSR International Pty Ltd. NVivo. 2018. https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home
Flottorp SA, Oxman AD, Krause J, Musila NR, Wensing M, Godycki-Cwirko M, et al. A checklist for identifying determinants of practice: a systematic review and synthesis of frameworks and taxonomies of factors that prevent or enable improvements in healthcare professional practice. Implement Sci. 2013;8(1):1–11.
Carroll C, Patterson M, Wood S, Booth A, Rick J, Balain S. A conceptual framework for implementation fidelity. Implement Sci. 2007;2(1):1–9.
Rogers EM. Diffusion of innovations. New York: Simon and Schuster; 2010.
Creswell JW, Clark VLP. Chapter 7: Analyzing and interpreting data in mixed methods research. In: Creswell JW, Clark VLP, editors. Designing and conducting mixed methods research. 3rd ed. London: Sage publications; 2017.
Grimes RM, Hallmark CJ, Watkins KL, Agarwal S, McNeese ML. Re-engagement in HIV care: a clinical and public health priority. J AIDS Clin Res. 2016. https://doi.org/10.4172/2155-6113.1000543.
Acknowledgements
The authors wish to acknowledge the patient and nurse participants who were essential to this study and the resulting improvements to patient care at the MUHC. They also wish to acknowledge other clinicians and allied health professionals at the MUHC for their support of the project; Julie Bellingham and Chantal Burrell for their support in translating study documents; Costas Pexos and Jessica Lumia for supporting changes to the EMR database; Gino Curadeau, Cristian Machuca, Ellen Seguin, Vicky Lavazos, Jonathan Roger, Julia Slater, and Sharon Sandy for their ongoing support; and the I-Score patients committee for their assistance in developing study tools and procedures.
Funding
This study is funded by ViiV Healthcare. NK is supported by a career award from the Fonds de Recherche Québec – Santé (FRQ-S; Junior 1).
Author information
Authors and Affiliations
Consortia
Contributions
JC and NK are the co-principal investigators. JC is the study sponsor. BL is the research coordinator and internal facilitator. LR, EB, NO, and MB are nurses at the CVIS-MUHC. BL, JC, NK, DL and KE co-developed the analysis plan. BL, JC, and NK were responsible for obtaining ethics approval. DL led focus group discussions with nurses. BL and DL conducted the qualitative analysis. BL conducted quantitative analyses. BL wrote the first draft of this article and the protocol for ethics review. BL, JC, DL, and NK collaborated to complete subsequent drafts. All authors, including BL, contributed to study conception and critically reviewed drafts of the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
Nadine Kronfli reports research funding from Gilead Sciences, advisory fees from Gilead Sciences, ViiV Healthcare, Merck and Abbvie, and speaker fees from Gilead Sciences, Abbvie and Merck, all outside of the submitted work. Bertrand Lebouché has received consulting fees from ViiV Healthcare Merck and Gilead; research funding from Merck, Gilead, ViiV Healthcare; and payment for lectures from Merck, Gilead and ViiV Healthcare. Joseph Cox has received consulting fees from ViiV Healthcare, Merck, and Gilead; research funding from ViiV Healthcare, Merck and Gilead; and payment for lectures from Gilead. All other authors declare that they have no competing interests.
Ethics Approval and Consent to Participate
Approval was obtained by the Ethics Committee at the McGill University Health Centre (2018-4369), who reviewed and monitored this study. All efforts were be made to ensure the confidentiality of participants, including the use of randomised study codes, encryption of electronic documents on password protected hospital servers, secure storage of printed materials, and timely destruction of study documents. In lieu of individual informed consent of patients, authorization to access patient charts was obtained from the Director of Professional Services (DPS) of the MUHC Glen Site – Adult Sector. All nurses agreed to participate. They were not consented by a boss or direct supervisor, but instead by the research coordinator for this study. Participation was voluntary and nurses could withdraw at any time or decline to participate without affecting their employment. Given limited to no risk of harms to participants, no data monitoring committee was be involved in data oversight.
Consent for Publication
A signed informed consent form was obtained from each nurse by the research coordinator prior to inclusion in the study and scientific use of acquired data.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Linthwaite, B., Kronfli, N., Lessard, D. et al. Implementation of Lost & Found, An Intervention to Reengage Patients Out of HIV Care: A Convergent Explanatory Sequential Mixed-Methods Analysis. AIDS Behav 27, 1531–1547 (2023). https://doi.org/10.1007/s10461-022-03888-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-022-03888-y