
Abstract
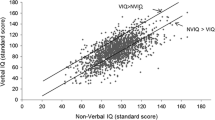
This study was a systematic review of research using the Wechsler Intelligence Scale for Children (WISC) with Autism Spectrum Disorder (ASD) to examine cognitive characteristics of children with ASD beyond the impact of revisions based on WISC and diagnostic criteria changes. The classic “islets of ability” was found in individuals with full-scale IQs < 100. The “right-descending profiles” were observed among high IQ score individuals. High levels on the Block Design and low Coding levels were consistently found regardless of the variation in intellectual functioning or diagnosis. This review identified patterns of cognitive characteristics in ASD individuals using empirical data that researchers may have previously been aware of, based on their experiences, owing to the increased prevalence of ASD.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
In 1943, autism spectrum disorder (ASD) was first described as an “autistic disorder of affective contact” (Kanner 1943). Since then, many similar cases have been reported worldwide, with this rapid increase in its prevalence in recent years attracting considerable attention (Fombonne 2005). The prevalence of ASD was initially approximately 4.5 or 10–20 persons in a population of 10,000 (Lotter 1966; Wing et al. 1976). However, over the past two decades, it has steadily increased, from 67 to 131–293 persons per 10,000 in the United States (Baio et al. 2018; Bertrand et al. 2001), 48–161 in Japan (Honda et al. 2005), 116 in the UK (Baird et al. 2006), and 264 persons per 10,000 in South Korea (Kim et al. 2011). This was primarily due to an increase in high IQ score cases without intellectual disabilities (Charman et al. 2011; Fombonne 2009).
During this period, the diagnostic criteria for ASD have changed. They were initially based on a report by Kanner (1943), followed by wide use of Rutter’s criteria internationally (Rutter 1978). In 1980, the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III; American Psychiatric Association 1980) categorized ASD as a subtype of “infantile autism” under pervasive developmental disorders (PDD). Thereafter, in the DSM-IIIR (American Psychiatric Association 1987), the diagnostic label for the subtype was changed to “autistic disorder,” and pervasive developmental disorder, not otherwise specified (PDDNOS) was added. Subsequently, in the DSM-IV (American Psychiatric Association 1994), “Asperger’s disorder” was introduced as individuals having no clinically significant delays in language development. The DSM-5 (American Psychiatric Association 2013) adopted the term ASD while the diagnostic terms “Asperger’s disorder” and “PDD” were removed.
The International Classification of Disease and Related Health Conditions (ICD) is another internationally recognized diagnostic guideline that has used the diagnostic term PDD with subtypes “childhood autism” and “Asperger’s syndrome” in ICD-10 (ICD-10; World Health Organization [WHO] 1992) since the 1990s. However, in an attempt at harmonization, the ICD-11(World Health Organization [WHO] 2018) adopted a similar disease classification as the DSM-5, including the term ASD. Although ASD’s diagnostic criteria and disease classification changed across the different editions of DSM and ICD, they presently have identical criteria.
The Wechsler scales are the most widely used measures of intelligence and have been translated, adapted, and standardized in many countries worldwide. The Wechsler Adult Intelligence Scale (WAIS; Wechsler 1939) was first developed after the Wechsler Intelligence Scales for Children (WISC; Wechsler 1949). Later, the WISC was revised several times, including the WISC-R (Wechsler 1974), WISC-III (Wechsler 1991), WISC-IV (Wechsler 2003), and WISC-V (Wechsler 2014). These revisions have encompassed various changes, eliminations, and incorporations of new tests even among the subtests. In the first edition of WISC, two index scores, verbal IQ (intelligence quotient), and Performance IQ, were calculated to identify intra-individual differences, along with Full-Scale IQ scores. As a result of the repeated revision of WISC, a procedure for analyzing intra-individual differences was created with four indexes: VCI (Verbal Comprehension Index), POI (Perceptual Organization Index), FDI (Freedom from Distractibility Index), and PSI (Processing Speed Index) (Wechsler 2003). Recently, the following five indexes were created based upon the Cattell-Horn-Carroll theory in WISC-V: VCI, VSI (Visual Spatial Index), FRI (Fluid Reasoning Index), WMI (Working Memory Index), and PSI (Wechsler 2014). To interpret results, both normative and personal strengths and weaknesses among the indexes were identified. Interpretation of fluctuations in the child’s index profile offers reliable and meaningful information regarding WISC performance because it identifies strong and weak areas of cognitive functioning relative to both same-age peers from the normal population (inter-individual approach) and the child’s own overall ability level (intra-individual approach). The WISC results provide clinically meaningful information in areas to develop individual support plans and treatment programs for children with neurodevelopmental disorders (Flanagan and Kaufman 2009).
The oldest reports on the WISC and ASD were by Gillies (1965) and Wassing (1965), both of which revealed low verbal-ability test scores in ASD cases. Later, Lockyer and Rutter (1970) reported the results of their study spanning 5–15 years of follow-ups and including 63 pediatric psychiatric cases that were diagnosed during the 1950s in the UK. Based on the WISC and WAIS subtest profiles from these cases, Lockyer and Rutter identified cognitive profiles common to ASD that Comprehension levels are low, while Block Design, Object Assembly, and Digit Span levels are high. Among them, Block Design has peaks. This pattern was decidedly noticeable among children with pronounced language delay. Lockyer and Rutter (1970) referred to this pattern of characteristics as the “islets of ability.” Thereafter, high Block Design scores and low Comprehension scores have consistently been reported and widely recognized as a typical cognitive profile of ASD (Asarnow et al. 1987; Ehlers et al. 1997; Freeman et al. 1985; Ghaziuddin and Mountain-Kimchi 2004; Happe 1994; Koyama et al. 2006, 2009; Mayes and Calhoun 2003; Shah and Firth (1993); Siegel et al. 1996; Szatmari et al. 1990).
Various hypotheses have been put forward regarding the relationship between ASD’s WISC profile and cognitive impairment. Lockyer and Rutter (1970) interpreted that high performance on the Block Design observed in the islets of ability were due to good perceptual organization in ASD. Based on the low verbal scores, they also hypothesized that ASD was caused by a central disorder of language and perception of sounds (Lockyer and Rutter 1970). Shah and Frith (1993) argued that autistic children do well on only those tasks that favor a piecemeal processing style, where children with no disorders are impeded by their tendency to look for overall meaning or be captured by the global or gestalt form at the expense of the local parts or details, and pointed out that weak central coherence was observed among children with autism (Shah and Frith 1993). Happe (1994) considered that the peak of Block Design in islets of ability was not due to only good perceptual organization but also due to the manifestation of their relatively local, as opposed to global, processing style by their weak central coherence (Happe 1994).
While Lockyer and Rutter (1970) focused on the islet of ability, they did not discuss the WISC profile with respect to Coding. In fact, the lowest subtest score in their data was Coding (Lockyer and Rutter 1970). For Coding, the child works within a specific time limit and uses a key to copy symbols that correspond with simple geometric shapes or numbers. In addition to processing speed, the subtest measures visual perception, visuomotor coordination, cognitive flexibility (shifting rapidly from one pair to another), attention skills, and possibly, motivation (Sattler 2004; Weiss et al. 2015). Factors such as problems of motor coordination (Mayes and Calhoun 2003) and cognitive flexibility (Hedvall et al. 2013) were pointed out for low Coding and PSI values in children with ASD.
Initially, Lockyer and Rutter (1970) saw the islets of ability in the WISC profile of ASD, which was associated with intellectual disability and demonstrated particularly low verbal-ability test scores. Later, Happe (1994) and Shah and Frith (1983, 1993) proposed good perceptual organization and weak central coherence, which were considered to be consistent with ASD’s WISC profile. More recently, cognitive characteristics, such as cognitive inflexibility and impairment of mentalizing (Baron-Cohen et al. 1985; Baron-Cohen 2004), were also proposed, and it has been considered that these, along with the WISC profile among children with ASD are consistent. However, within the half-century since the concept of ASD was proposed, the proportion of high IQ scores displayed by children with ASD increased (Fombonne 2009). Consequently, it has been observed that recent WISC profiles of ASD have changed from what had historically been identified as the WISC profile for children with ASD (Siegel et al. 1996; Mayes and Calhoun 2008; Charman et al. 2011). However, there are no reports that systematically discuss and examine this point.
WISC is a test with reliability and validity confirmed by its prolonged widespread use (Wechsler 1974, 2003), and the Composite Scale has been stable over time (Bartoi et al. 2015; Kieng et al. 2017). The content validity and constructs validity of the FSIQ and Composite Scale have been repeatedly verified, and evidence of interpretation methods have been accumulated. Thus, analyses of indexes with reliability and validity have been recommended for the utility of intra-individual analysis in recent years. Meanwhile, an intra-individual analysis using subtests is not recommended, due to low reliability and lack of evidence of interpretation validity of such an approach (Flanagan and Kaufmann 2009). However, the cognitive characteristics of ASD, such as weak central coherence and cognitive flexibility, which have been pointed out, cannot be captured by observing the current Composite Scales —VCI (Verbal Comprehension Index), POI (Perceptual Organization Index), FDI (Freedom From Distractibility Index), PSI (Processing Speed Index) (Wechsler 2003), VSI (Visual Spatial Index), FRI (Fluid Reasoning Index), WMI (Working Memory Index), and PSI (Wechsler 2014). It is difficult to derive an answer by discussing only the Composite Scale in response to the question of whether the cognitive characteristics of ASD that were identified on the subtest profile in previous WISC versions, including the islets of ability, are also displayed by current children with ASD. In order to supplement the instability of subtest, it is crucial to extract subtests common to the studies reported to date, find common features from multiple studies, and examine them. Therefore, in this study, we conducted a systematic literature search for empirical studies on WISC in ASD. To eliminate the effects of the revision of WISC from the extracted papers, six subtests—commonly employed by WISC, WISC-R, WISC-III, and WISC-IV (i.e., Similarities, Vocabulary, Comprehension, Block Design, Digit Span, and Coding)—were extracted, and the mean scores were compared. The purpose of this study is to delineate the cognitive characteristics of ASD beyond the impact of changes in diagnostic criteria and the revisions of the WISC. We hope that this review will provide updated information regarding recent WISC profiles of ASD to current clinicians engaged in child psychiatry.
Methods
Literature Review
This review selected literature adopting the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement (Liberati et al. 2009). Three databases of PubMed, PsychINFO, and Ichu-Shi were used for literature identification, and the searches were conducted between December 19–20, 2018. The selection criteria comprised all literature published before December 20, 2018, including peer-reviewed journal articles written in English and papers with one or more of the following keywords: autism, pervasive developmental disorder, PDD, Asperger, WISC, or Wechsler Intelligence Scale for Children (PubMed, n = 569; PsychINFO, n = 3,817; and Ichu-Shi, n = 37). After excluding duplicates, 4,208 papers were initially identified and from among those, 51 papers that discussed the mean scores of the subtests of WISC, WISC-R, WISC-III, or WISC-IV for participants with ASD or PDD were selected. From these, studies that did not include all the mean scores of six subtests of interest, studies using WAIS, and a study evaluating only PDD-NOS participants were excluded. Thus, we selected 27 papers.
Comparison of Scores
We compared the mean scores of the commonly employed six subtests (i.e., Similarities, Vocabulary, Comprehension, Block Design, Digit Span, and Coding). Moreover, the subtest profiles were compared between different intellectual levels and diagnoses.
Results
Systematic Review to Extract Relevant Studies
The 51 studies were extracted, following the PRISMA statement for systematic review. Table 1 presents the names of authors, year of publication, participants groups, the ultimately analyzed participants, diagnoses within the paper, number of cases, the mean age and age range of the target group, mean FSIQ, and the tests conducted. The ultimately analyzed participants refer to the group that met all selection criteria (to be further discussed later), and thus, were included in the final analysis. These 51 studies were published between 1970 and 2017, and the total number of participants ranged from 9 (Bartak et al. 1975) to 166 (Mouga et al. 2016). There were 4 WISC studies, 17 WISC-R studies, 23 WISC- III studies, and 10 WISC- IV studies. The Participant Groups refer to the groups that the studies include, multiple participant groups, which were separated into categories by diagnoses, test versions, and intellectual levels. For studies in which the same authors had assessed the same participants, only one was adopted. Finally,14 studies including mixed WAIS results were excluded, and another nine studies were removed because they did not include all the mean scores of six subtests of interest. Readers are encouraged to refer to the detailed reasons for exclusion that are stated below in Table 1. The studies by Bölte and Poustka (2004), Koyama et al. (2009), Kumazaki et al. (2015), and Calero et al. (2015) included results obtained after categorizing participants into groups by either gender or treatment response. However, these results were treated as one group.
Overall, 27 papers were ultimately selected. Of these, those that included multiple participants were separated into categories by diagnosis and intellectual level, and each category was counted as a separate group. Finally, the review participants comprised a total of thirty-four groups that were a part of the “ultimately analyzed participants (†).”
Mean Subtest Scores, Diagnostic Criteria, and Diagnoses
Table 2 provides details for the 34 studies that comprised the ultimately analyzed participants. Of these, the WISC reported in Bartak et al. (1975) and Ohta (1987), as well as the WISC-R in Lincoln et al. (1988), moreover, Allen et al. (1991), showed low Similarities, Vocabulary, and Comprehension scores, combined with particularly low Comprehension scores, which created a notable trough. Block Design displayed high scores that created a peak, while Digit Span and Coding indicated comparatively low scores. Thus, these groups demonstrated classic islets of ability profiles. While some of the remaining 30 groups displayed troughs in Comprehension scores and peaks in Block Design, the verbal levels did not stand out as consistently low. In fact, some groups demonstrated high verbal levels, suggesting different patterns.
Comparison of Three Groups
Comparison of Six Subtest Profiles by Intellectual Level (Fig. 1)
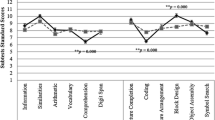
Based on the mean FSIQ of the ultimately analyzed participants, the groups were divided into three ranges: (a) mean FSIQ of ≤ 85; (b) mean FSIQ of 86–100, and (c) mean FSIQ of > 100. The relationships between intellectual levels and the six subtest profiles were then examined. The three graphs in Fig. 1 indicate the six subtest profiles. Among the seven groups with a mean FSIQ of ≤ 85, Allen et al. (1991), Bartak et al. (1975), Lincoln et al. (1988), and Ohta (1987) exhibited classic islets of ability profiles. Although in the report by Ehlers et al. (1997) participants with autism diagnoses (E1), and in that by Kuriakose (2014) and Mouga et al. (2016) participants with low IQ scores (M1) did not demonstrate typical profiles; there were troughs in Comprehension and peaks in Block Design. Therefore, overall, the groups exhibited classic islets of ability profiles. For the sixteen groups with mean FSIQ scores between 86–100, the included profiles were diverse though there were many classic islets of ability profiles with Comprehension troughs and Block Design peaks. Among the 11 groups with a mean FSIQ of ≥ 100, high verbal scores on Similarities and Vocabulary stood out. Apart from Nydēn et al. (2001) and Williams et al. (2006b), Coding had the lowest scores in the other nine groups, displaying right-descending profiles.

Comparison of six subtest profiles of the three groups based on intellectual level. a Seven groups with a mean FSIQ of ≤ 85. b Sixteen groups with a mean FSIQ of ≥ 86 and < 100. c Eleven groups with a mean FSIQ of ≥ 100. The order of subtests in figures for this study followed the order in the present WISC-IV manual. ASD, Autism Spectrum Disorder; PDD, Pervasive Developmental Disorder; WISC, Wechsler Intelligence Scales for Children
Comparison by Diagnosis and Intellectual Level (Fig. 2)
For the three intellectual-level–based groups, further examination was conducted by subdividing them by diagnosis into three groups: autism diagnoses (including autism, autistic children, and infantile autism), PDD or ASD diagnoses, and Asperger’s diagnoses. Among the groups with a mean FSIQ of ≤ 85—excluding Kuriakose (2014) and Mouga et al. (2016) participants with low IQ scores (M1) with ASD diagnoses—all represented autism diagnoses with no cases corresponding to Asperger’s disorder. Although low verbal levels were not detected by Ehlers et al. (1997) participants with autism diagnoses (E1), a trough-and-peak trend of low Comprehension levels and high Block Design levels was found, thereby confirming a typical islets of ability profile.

Comparison of six subtest profiles by diagnosis by intellectual level among three groups. a A comparison of six subtest profiles by diagnosis for those with a mean FSIQ of ≤ 85. b A comparison by diagnoses for those with a mean FSIQ of ≥ 86 and < 100. c A comparison by diagnosis for those with a mean FSIQ of ≥ 100. For those, a mean FSIQ of ≤ 85, no cases corresponded to an Asperger’s diagnosis. The order of subtests in figures for this study followed the order in the present WISC-IV manual. ASD Autism Spectrum Disorder, PDD Pervasive Developmental Disorder, WISC Wechsler Intelligence Scales for Children
Of the six groups with a mean FSIQ between 86–100 with autism diagnoses, except for de Bruin et al. (2006), the groups did not display extremely low verbal levels; however, they indicated troughs for Comprehension and peaks for Block Design, demonstrating islets of ability profiles. Conversely, while some diagnoses relating to PDD or ASD and Asperger’s confirm islets of ability profiles, they differed from the typical profile by having either Coding levels that were lower than Comprehension or their scores for Similarities, Vocabulary, or Digit Span levels were higher than Block Design rather than exhibiting the typical trough for Comprehension and peak for Block Design.
Among the groups with a mean FSIQ of ≥ 100, low Comprehension levels and high Block Design levels were observed among the four groups having autism diagnoses (in Foley-Nicpon et al. (2012) participants with autism diagnoses (F1); Mayes and Calhoun (2004, 2008); Williams et al. (2006b). However, the levels for Similarities and Vocabulary were higher than for Block Design, while Coding was lower than Comprehension, thereby resulting in an overall right-descending profile. Matsuura et al. (2014) and Calero et al. (2015) included PDD or ASD diagnoses showed similar right-descending profiles where Comprehension was lowest among the verbal tests and Coding was lowest in the overall test scores. Among the Asperger’s diagnoses group, high Similarities, Vocabulary, and Comprehension, together with low Coding test score levels were observed, resulting in overall right-descending profiles.
High Block Design and Low Coding
As seen in Table 2 and Fig. 1, the mean scores for Block Design levels were 8 or above for all 32 groups, excluding de Bruin et al. (2006) participants with autism diagnoses (B1) and Mouga et al. (2016) participants with low IQ scores (M1). In addition, most scored at a consistently high level with a mean score higher than the average level of 10–12. Although the prominence of high Block Design was unnoticeable because of the high language levels among the recently reported high-IQ cases, this review reaffirmed that Block Design remained consistently high.
Participants with right-descending profile and those with classic islets of ability showed Coding scores that were not high (6–8) in either group. Also, the low Coding pattern has consistently been observed after the number of participants with high intellectual levels began to increase in published studies; thus, resulting in WISC patterns differing from the classic islets of ability.
Furthermore, this trend of high Block Design and low Coding was seen across all groups, irrespective of intellectual levels or diagnosis. Therefore, this trend can be confirmed as a cognitive characteristic that exists widely among all ASD groups.
Discussion
This paper reviewed reports from 1970 to 2017 related to the ASD classic profile “islets of ability” (Lockyer and Rutter 1970). After examining the six subtest profiles based on intellectual levels and diagnosis, it was observed that the classic islets of ability profile was present in the autism diagnosis group with a mean FSIQ of < 100 and the PDD or ASD diagnosis group with a mean FSIQ of ≤ 85. On the other hand, for those groups with a mean FSIQ of ≥ 100 regardless of the diagnoses, the PDD or ASD diagnosis groups with a mean FSIQ of ≥ 86, and all Asperger’s diagnosis groups regardless of intellectual levels demonstrated right-descending profiles with high Similarities, Vocabulary, and Block Design together with low Coding rather than the classic islets of ability profile. In other words, the WISC profile of ASD individuals tended to demonstrate classic islets of ability profiles for those with low intellectual levels, whereas those with higher intellectual levels displayed right-descending profiles were.
In recent years, the prevalence of high-IQ score ASD has increased, and our results suggest that the WISC profile of children with ASD has transformed from the time when Kanner (1943) and Rutter (1978) proposed the concept of autism that centered on cases accompanying intellectual disability. Thus, answers to questions like “can any cognitive characteristics of ASD be captured by WISC?” and “can they exist perpetually without change?” are addressed in this study by demonstrating that high Block Design levels and low Coding levels continued to exist at the same levels, regardless of intellectual level, diagnostic name, and time-based changes.
This Block Design peak has been previously explained by Happe (1994) and Shah and Frith (1983, 1993) using the central coherence theory. Examples of related behaviors to the Block Design peak in ASD children include incredible dexterity in mold-fitting puzzles and in completing jigsaw puzzles. Today, ASD children with high intellectual ability are also patients of clinical practice, and the islets of ability on the WISC profile became less noticeable due to higher scores centered on the verbal test. However, Block Design scores remain high. In other words, the recent high scores of Block Design among children with ASD also indicate that good local information processing by weak central coherence is represented, despite being different from the previous profile on WISC.
Meanwhile, the low Coding in ASD were often discussed from the viewpoint of problems with motor coordination (Mayes and Calhoun, 2003; Szatmari et al. 1990). Hedvall et al. (2013) focused on the processing speed of children with ASD, and stated that Processing Speed subtests challenge the child’s capacity to work independently according to a given template and that they require graphomotor speed, accuracy, and mental flexibility/set shifting capacity to sustain attention to task, pointing out the effect of cognitive flexibility (Hedvall et al. 2013). In fact, observations of children with ASD during Coding tests indicate that even if there is no problem with the manual dexterity, the number of tasks that can be tackled is limited due to the difficulty of cognitive flexibility that shifts their attention toward next tasks. Such cases are not uncommon. Because the Coding results of children with ASD are associated with two problems, the problem with visuomotor coordination and the problem with cognitive flexibility, these scores can be considered consistently low.
Thus, if the evaluation scores of verbal tests (e.g., Similarities, Vocabulary, and Comprehension) are low together with consistently low Coding levels and contrastingly consistent high Block Design levels, these high Block Design levels would result in a prominent peak, thereby appearing as a classic islets of ability profile. In cases of individuals with high-IQ scores and high verbal scores, these verbal scores also create peaks that make the high Block Design less prominent, which might underline their right-descending profile.
Although the number of children with ASD with no islets of ability on WISC has increased in recent years, underlying problems of weak central coherence, cognitive flexibility and visuomotor coordination are still present. In fact, central coherence is associated with language and social development of ASD (Engel and Ehri 2020; Pellicano 2010), and poor cognitive flexibility was indicated to be related to the rigid and concrete bound behavior, occasionally transforming into perseverations of ASD (Lopez et al. 2005; Ozonoff and Jensen 1999). For example, cases in which children demonstrate difficulty seeing the whole picture because they concentrate too much on details, or cases in which they experience difficulty changing their perspectives once they presume are also observed frequently among children with ASD. Therefore, it may be of significant benefit for assessments and interventions to focus on weak central coherence and cognitive inflexibility to support such behaviors in clinical practice with children with ASD.
In this review, we demonstrated that the patterns of subtest performance of children with ASD are consistent with weak central coherence and limited cognitive flexibility. However, this observation cannot be interpreted as strong support for those hypotheses, because the individual studies included in the review did not disclose direct evidence that the subtest performance patterns are causally related to weak central coherence or cognitive inflexibility. Having said that, we still believe what we demonstrated constitutes beneficial reference material for clinicians to utilize when interpreting the WISC performances.
Today, ASD is known to be a clinical entity that combines multiple heterogeneous diseases. Based on the present review, when these diseases were combined into one, as ASD, the high Block Design performance and the low Coding performance on the WISC test were recognized as the coexisting neurocognitive endophenotypes. From this perspective, clarifying the path of how the neurocognitive endophenotypes will develop into the clinical phenotype of ASD should be an area of focus for future research (Viding and Blakemore 2007). Our proposition as a potential mean of clarifying this path is to examine the relationships between the clinically evaluated scores representing mentalizing, central coherence and cognitive flexibility, and the scores of Block Design as well as Coding among different types of ASD, ideally at several age points along the developmental course. Such examinations would reveal the mechanism of the endophenotypes’ development into the clinical phenotypes of ASD.
One of the limitations of this study was using only the six traditional subtests as subjects, thereby negating the examination of the other subtests. Each time WISC is revised, new subtests are also incorporated. In the future, the accumulation of knowledge about other subtests and newly adopted tests will therefore be required.
Change history
23 April 2021
A Correction to this paper has been published: https://doi.org/10.1007/s10803-021-05020-w
References
Allen, M. H., Lincoln, A. J., & Kaufman, A. S. (1991). Sequential and simultaneous processing abilities of high-functioning autistic and language-impaired children. Journal of Autism and Developmental Disorders, 21(4), 483–502.
American Psychiatric Association (1980). Diagnostic and Statistical Manual of Mental Disorders, 3rd Ed. (DSM-III). Washington DC: American Psychiatric Association.
American Psychiatric Association. (1987). Diagnostic and Statistical Manual of Mental Disorders, 3rd Ed. Revised. (DSM-IIIR). Washington DC: American Psychiatric Association.
American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders, 4th Ed. (DSM-IV). Washington DC: American Psychiatric Association.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders, 5th Ed. (DSM-5). Washington DC: American Psychiatric Association.
Asarnow, R. F., Tanguay, P. E., Bott, L., & Freeman, B. J. (1987). Patterns of intellectual functioning in non-retarded autistic and schizophrenic children. Journal of Child Psychology and Psychiatry 1987, 28(2), 273–280.
Baio, J., Wiggins, L., Christensen, D. L., Maenner, M. J., Daniels, J., Warren, Z., et al. (2018). Prevalence of autism spectrum disorder among children aged 8 years - Autism and developmental disabilities monitoring network, 11 Sites, United States, 2014. Morbidity and Mortality Weekly Report—Surveillance Summaries, 67(6), 1–23.
Baird, G., Simonoff, E., Pickles, A., Chandler, S., Loucas, T., Meldrum, D., & Charman, T. (2006). Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: The Special Needs and Autism Project (SNAP). The Lancet, 368(9531), 210–215.
Baron-Cohen, S. (2004). Autism: Research into causes and intervention. Pediatric Rehabilitation, 7(2), 73–78.
Baron-Cohen, S., Leslie, A. M., & Frith, U. (1985). Does the autistic child have a “theory of mind”? Cognition, 21(1), 37–46.
Bartak, L., Rutter, M., & Cox, A. (1975) A comparative study of infantile autism and specific development receptive language disorder. I. The children. British Journal of Psychiatry, 126(2), 127–145.
Bartoi, M. G., Issner, J. B., Hetterscheidt, L., January, A. M., Kuentzel, J. G., & Barnett, D. (2015). Attention Problems and Stability of WISC-IV Scores Among Clinically Referred Children. Applied Neuropsychology: Child, 4(3), 133–140.
Bertrand, J., Mars, A., Boyle, C., Bove, F., Yeargin-Allsopp, M., & Decoufle, P. (2001). Prevalence of autism in a United States population: The Brick Township, New Jersey, investigation. Pediatrics, 108(5), 1155–1161.
Bölte, S., & Poustka, F. (2004). Comparing the intelligence profiles of savant and nonsavant individuals with autistic disorder. Intelligence, 32(2), 121–131.
Bölte, S., Rudolf, L., & Poustka, F. (2002). The cognitive structure of higher functioning autism and schizophrenia: A comparative study. Comprehensive Psychiatry, 43(4), 325–330.
Calero, M. D., Mata, S., Bonete, S., Molinero, C., & Mar Gómez-Pérez, M. (2015). Relations between learning potential, cognitive and interpersonal skills in Asperger children. Learning and Individual Differences, 44, 53–60.
Cederlund, M., & Gillberg, C. (2004). One hundred males with Asperger syndrome: A clinical study of background and associated factors. Developmental Medicine and Child Neurology, 46(10), 52–60.
Charman, T., Pickles, A., Simonoff, E., Chandler, S., Loucas, T., & Baird, G. (2011). IQ in children with autism spectrum disorders: Data from the Special Needs and Autism Project (SNAP). Psychological Medicine, 41(3), 619–627.
de Bruin, E. I., Verheij, F., & Ferdinand, R. F. (2006). WISC-R subtest but no overall VIQ-PIQ difference in Dutch children with PDD-NOS. Journal of Abnormal Child Psychology, 34(2), 263–271.
Ehlers, S., Nyden, A., Gillberg, C., Sanberg, A. D., Dahlgren, S.-O., Hjelmquist, E., et al. (1997). Asperger syndrome, autism and attention disorders: A comparative study of the cognitive profiles of 120 children. Journal of Child Psychology and Psychiatry, 38(2), 207–217.
Engel, S., & Ehri, L., (2020). Reading Comprehension Instruction for Young Students with Autism: Forming Contextual Connections. Journal of Autism and Developmental Disorders, Published online 10 July 2020.
Flanagan, D. P., & Kaufman, A. S. (2009). Essentials of WISC-IV assessment. John Wiley & Sons.
Foley-Nicpon, M., Assouline, S. G., & Stinson, R. D. (2012). Cognitive and academic distinctions between gifted students with autism and Asperger syndrome. Gifted Child Quarterly, 56(2), 77–89.
Fombonne, E. (2005). Epidemiology of autistic disorder and other pervasive developmental disorders. Journal of Clinical Psychiatry, 66(Suppl 10), 3–8.
Fombonne, E. (2009). Epidemiology of pervasive developmental disorders. Pediatric Research, 65(6), 591–598.
Freeman, B. J., Lucas, J. C., Forness, S. R., & Ritvo, E. R. (1985). Cognitive processing of high-functioning autistic children: Comparing the K-ABC and the WISC–R. Journal of Psychoeducational Assessment, 3(4), 357–362.
Ghaziuddin, M., & Mountain-Kimchi, K. (2004). Defining the intellectual profile of Asperger syndrome: Comparison with high-functioning autism. Journal of Autism and Developmental Disorders, 34(3), 279–284.
Gillberg, C. (1991). Clinical and neurobiological aspects of Asperger syndrome in six family studies. In U. Frith (Ed.), Autism and asperger syndrome (pp. 122–146). Cambridge: Cambridge University Press.
Gillberg, I. C., & Gillberg, C. (1989). Asperger syndrome: Some epidemiological considerations: A research note. Child Psychology & Psychiatry & Allied Disciplines, 30(4), 631–638.
Gillies, S. (1965). Some abilities of psychotic children and subnormal controls. Journal of Mental Deficiency Research, 9(2), 89–101.
Happe, F. G. (1994). Wechsler IQ profile and theory of mind in autism: A research note. Journal of Child Psychology and Psychiatry, 35(8), 1461–1471.
Hedvall, Å., Fernell, E., Holm, A., Johnels, J. Å., Gillberg, C., & Billstedt, E. (2013). Autism, processing speed, and adaptive functioning in preschool children. The Scientific World Journal, 2013, ID158263.
Honda, H., Shimizu, Y., & Rutter, M. (2005). No effect of MMR withdrawal on the incidence of autism: A total population study. Journal of Child Psychology and Psychiatry, 46(6), 572–579.
Inada, N., & Kamio, Y. (2010). Short forms of the Japanese version WISC-III for assessment of children with autism spectrum disorders. Japanese Journal of Child and Adolescent Psychiatry, 51(Suppl), 11–19.
Kanner, L. (1943). Autistic disturbances of affective contact. Nervous Child, 2(3), 217–250.
Kieng, S., Rossier, J., Favez, N., & Lecerf, T. (2017). Long-term stability of the French WISC-IV: Standard and CHC index scores. European Review of Applied Psychology, 67, 51–60.
Kim, Y. S., Leventhal, B. L., Koh, Y. J., Fombonne, E., Laska, E., Lim, E.-C., et al. (2011). Prevalence of autism spectrum disorders in a total population sample. American Journal of Psychiatry, 168(9), 904–912.
Koyama, T., Kamio, Y., Inada, N., & Kurita, H. (2009). Sex differences in WISC-III profiles of children with high-functioning pervasive developmental disorders. Journal of Autism and Developmental Disorders, 39(1), 135–141.
Koyama, T., & Kurita, H. (2008). Cognitive profile difference between normally intelligent children with Asperger’s disorder and those with pervasive developmental disorder not otherwise specified. Psychiatry and Clinical Neurosciences, 62(6), 691–696.
Koyama, T., Tachimori, H., Osada, H., & Kurita, H. (2006). Cognitive and symptom profiles in high-functioning pervasive developmental disorder not otherwise specified and attention-deficit/hyperactivity disorder. Journal of Autism and Developmental Disorders, 36(3), 373–380.
Koyama, T., Tachimori, H., Osada, H., Takeda, T., & Kurita, H. (2007). Cognitive and symptom profiles in Asperger’s syndrome and high-functioning autism. Psychiatry and Clinical Neurosciences, 61, 99–104.
Kumazaki, H., Muramatsu, T., Kosaka, H., Fujisawa, T. X., Iwata, K., Tomoda, A., et al. (2015). Sex differences in cognitive and symptom profiles in children with high functioning autism spectrum disorders. Research in Autism Spectrum Disorders, 13, 1–7.
Kuriakose, S. (2014). Concurrent validity of the WISC-IV and DAS-II in children with autism spectrum disorder. Journal of Psychoeducational Assessment, 32(4), 283–294.
Li, G., Du, Y., Luan, F., Li, M., & Ousley, O. (2017a). IQ profiles and clinical symptoms of Chinese school-aged boys with autism spectrum disorder. The European Journal of Psychiatry, 31(2), 59–65.
Li, G., Jiang, W., Du, Y., & Rossbach, K. (2017b). Intelligence profiles of Chinese school-aged boys with high-functioning ASD and ADHD. Neuropsychiatric Disease and Treatment, 13, 1541–1549.
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P. A., et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Journal of Clinical Epidemiology, 151(4), w65–w94.
Lincoln, A. J., Courchesne, E., Kilman, B. A., Elmasian, R., & Allen, M. (1988). A study of intellectual abilities in high-functioning people with autism. Journal of Autism and Developmental Disorders, 18(4), 505–524.
Lockyer, L., & Rutter, M. (1970). A five- to fifteen-year follow-up study of infantile psychosis. IV. Patterns of cognitive ability. British Journal of Social and Clinical Psychology, 9(2), 152–163.
Lopez, R. B., Lincoln, J. A., Ozonoff, S., & Lai, Z. (2005). Examining the Relationship between Executive Functions and Restricted, Repetitive Symptoms of Autistic Disorder. Journal of Autism and Developmental Disorders, 35(4), 445–460.
Lotter, V. (1966). Epidemiology of autistic conditions in young children. Social Psychiatry, 1(4), 124–135.
Manjiviona, J., & Prior, M. (1999). Neuropsychological profiles of children with Asperger syndrome and autism. Autism, 3(4), 327–356.
Matsuura, N., Ishitobi, M., Arai, S., Kawamura, K., Asano, M., Inohara, K., et al. (2014). Distinguishing between autism spectrum disorder and attention deficit hyperactivity disorder by using behavioral checklists, cognitive assessments, and neuropsychological test battery. Asian Journal of Psychiatry, 12, 50–57.
Mayes, S. D., & Calhoun, S. L. (2003). Analysis of WISC-III, Stanford-Binet: IV, and academic achievement test scores in children with autism. Journal of Autism and Developmental Disorders, 33(3), 329–341.
Mayes, S. D., & Calhoun, S. L. (2004). Similarities and differences in Wechsler Intelligence Scale for Children, Third Edition (WISC-III) profiles: Support for subtest analysis in clinical referrals. Clinical Neuropsychology, 18(4), 559–72.
Mayes, S. D., & Calhoun, S. L. (2008). WISC-IV and WIAT-II profiles in children with high-functioning autism. Journal of Autism and Developmental Disorders, 38(3), 428–439.
McGonigle-Chalmers, M., & McSweeney, M. (2013). The role of timing in testing nonverbal IQ in children with ASD. Journal of Autism and Developmental Disorders, 43(1), 80–90.
Merchan-Naranjo, J., Mayoral, M., Rapado-Castro, M., Llorente, C., Boada, L., Arango, C., et al. (2012). Estimation of the intelligence quotient using Wechsler Intelligence Scales in children and adolescents with Asperger syndrome. Journal of Autism and Developmental Disorders, 42(1), 116–122.
Mouga, S., Cafe, C., Almeida, J., Marques, C., Duque, F., & Oliveira, G. (2016). Intellectual profiles in the autism spectrum and other neurodevelopmental disorders. Journal of Autism and Developmental Disorders, 46(9), 2940–2955.
Muraru, O., Honjo, S., Murase, S., Kaneko, H., Nomura, K., Ishii, T., et al. (2007). Might the Wechsler Intelligence Scale for Children Third edition (WISC-III) support the differential diagnosis between pervasive developmental disorder (PDD) and Attention-Deficit/Hyperactivity Disorder (ADHD)? Japanese Journal of Child and Adolescent Psychiatry, 48(Suppl), 31–42.
Nader, A. M., Jelenic, P., & Soulieres, I. (2015). Discrepancy between WISC-III and WISC-IV cognitive profile in autism spectrum: What does it reveal about autistic cognition? PLoS ONE, 10(12), e0144645.
Noterdaeme, M., Wriedt, E., & Hohne, C. (2010). Asperger’s syndrome and high-functioning autism: Language, motor and cognitive profiles. European Journal of Child and Adolescent Psychiatry, 19(6), 475–481.
Nydén, A., Billstedt, E., Hjelmquist, E., & Gillberg, C. (2001). Neurocognitive stability in Asperger syndrome, ADHD, and reading and writing disorder: a pilot study. Developmental Medicine and Child Neurology, 43(3), 165–171.
Ohta, M. (1987). Cognitive disorders of infantile autism: a study employing the WISC, spatial relationship conceptualization, and gesture imitations. Journal of Autism and Developmental Disorders, 17(1), 45–62.
Oliveras-Rentas, R. E., Kenworthy, L., Roberson, R. B., 3rd., Martin, A., & Wallace, G. L. (2012). WISC-IV profile in high-functioning autism spectrum disorders: Impaired processing speed is associated with increased autism communication symptoms and decreased adaptive communication abilities. Journal of Autism and Developmental Disorders, 42(5), 655–664.
Ozonoff, S., & Jensen, J. (1999). Brief Report: Specific executive function profiles in three neurodevelopmental disorders. Journal of Autism and Developmental Disorders., 29(2), 171–177.
Ozonoff, S., South, M., & Miller, J. N. (2000). DSM-IV-defined Asperger syndrome: Cognitive, behavioral and early history differentiation from high-functioning autism. Autism, 4(1), 29–46.
Pellicano, E. (2010). Individual Differences in Executive Function and Central Coherence Predict Developmental Changes in Theory of Mind in Autism. Developmental Psychology., 46(2), 530–544.
Planche, P., & Lemonnier, E. (2012). Children with high-functioning autism and Asperger’s syndrome: Can we differentiate their cognitive profiles? Research in Autism Spectrum Disorders, 6(2), 939–948.
Reinvall, O., Voutilainen, A., Kujala, T., & Korkman, M. (2013). Neurocognitive functioning in adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 43(6), 1367–1379.
Rutter, M. (1971). The description and classification of infantile autism. In D. Churchill, G. Alpern, & M. DeMyer (Eds.), Infantile autism. Springfield, IL.
Rutter, M. (1978). Diagnosis and definition of childhood autism. Journal of Autism and Childhood Schizophrenia, 8(2), 139–161.
Sattler, J. M. (2004). Assessment of Children WISC-IV AND WPPSI-III supplement. Sattler, Publisher, Incorporated.
Shah, A., & Frith, U. (1983). An islet of ability in autistic children: A research note. Journal of Child Psychology and Psychiatry, 24(4), 613–620.
Shah, A., & Frith, U. (1993). Why do autistic individuals show superior performance on the block design task? Journal of Child Psychology and Psychiatry, 34(8), 1351–1364.
Siegel, D. J., Minshew, N. J., & Goldstein, G. (1996). Wechsler IQ profiles in diagnosis of high-functioning autism. Journal of Autism and Developmental Disorders, 26(4), 389–406.
Stack, K., Murphy, R., Prendeville, P., & O’Halloran, M. (2017). WISC-IV UK profiles of children with autism spectrum disorder in a specialist autism service. Educational and Child Psychology, 34(2), 40–53.
Szatmari, P., Tuff, L., Finlayson, M. A., & Bartolucci, G. (1990). Asperger’s syndrome and autism: Neurocognitive aspects. Journal of the American Academy of Child and Adolescent Psychiatry, 29(1), 130–136.
Tymchuk, A. J., Simmons, J. Q., & Neafsey, S. (1977). Intellectual characteristics of adolescent childhood psychotics with high verbal ability. Journal of Mental Deficiency Research, 21(2), 133–138.
Venter, A., Lord, C., & Schopler, E. (1992). A follow-up study of high-functioning autistic children. Journal of Child Psychology and Psychiatry, 33(3), 489–507.
Viding, E., & Blakemore, S. J. (2007). Endophenotype Approach to Developmental Psychopathology: Implications for Autism Research. Behavior Genetics, 37, 51–60.
Wassing, H. E. (1965). Cognitive functioning in early infantile autism: An examination of four cases by means of the Wechsler Intelligence Scale for Children. Acta Paedopsychiatrica: International Journal of Child & Adolescent Psychiatry, 32(4), 122–135.
Wechsler, D. (1939). The measurement of adult intelligence. Williams & Wilkins.
Wechsler, D. (1949). Wechsler Intelligence Scale for Children: Manual. The Psychological Corp.
Wechsler, D. (1974). Manual for the Wechsler Intelligence Scale for Children, Revised. The Psychological Corporation.
Wechsler, D. (1991). Wechsler Intelligence Scale for Children-third edition (WISC-III). The Psychological Corporation.
Wechsler, D. (2003). Wechsler Intelligence Scale for Children-fourth edition (WISC-IV). The Psychological Corporation.
Wechsler, D. (2014). Wechsler Intelligence Scale for Children-fifth edition (WISC-V). Pearson.
Weiss, L. G., Saklofske, D. H., Holdnack, J. A., & Prifitera, A. (2015). WISC-V assessment and interpretation: Scientist-practitioner perspectives. Academic Press.
Williams, D. L., Goldstein, G., & Minshew, N. J. (2006a). Neuropsychologic functioning in children with autism: further evidence for disordered complex information-processing. Child Neuropsychology, 12(4–5), 279–298.
Williams, D. L., Goldstein, G., & Minshew, N. J. (2006b). The profile of memory function in children with autism. Neuropsychology, 20(1), 21–29.
Wing, L., Yeates, S. R., Brierley, L. M., & Gould, J. (1976). The prevalence of early childhood autism: Comparison of administrative and epidemiological studies. Psychological Medicine, 6(1), 89–100.
World Health Organization [WHO]. (1992). The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. WHO.
World Health Organization [WHO]. (2018). ICD-11 for mortality and morbidity statistics (ICD-11 MMS) 2018 version. WHO.
Zhang, S., Kaneko, H., Ishii, T. K., S., Nomura. K., Murase. S., , et al. (2007). Factor analysis of the WISC-III in a Japanese pervasive developmental disorders group. Japanese Journal of Child and Adolescent Psychiatry, 48(Suppl), 22–30.
Zielińska, M., Sterczynski, R., & Baginska, A. (2014). The profile of WISC-R scores in children with high-functioning autism. Psychiatria Polska, 48(4), 667–676.
Funding
This study was supported in part by JSPS KAKENHI Grant Number JP18H01087.
Author information
Authors and Affiliations
Contributions
MT and YK designed the study, performed the literature search and wrote the initial draft of the manuscript. All authors contributed to the discussions on the interpretation of collected papers and revised the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest:
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised due to retrospective open access.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Takayanagi, M., Kawasaki, Y., Shinomiya, M. et al. Review of Cognitive Characteristics of Autism Spectrum Disorder Using Performance on Six Subtests on Four Versions of the Wechsler Intelligence Scale for Children. J Autism Dev Disord 52, 240–253 (2022). https://doi.org/10.1007/s10803-021-04932-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-021-04932-x