
Abstract
Purpose: Evaluate the SpO2-SaO2 difference between Black and White volunteer subjects having a low perfusion index (Pi) compared to those having a normal Pi. Methods: The Pi data were abstracted from electronic files collected on 7183 paired SpO2-SaO2 samples (3201 Black and 3982 White) from a recently reported desaturation study of 75 subjects (39 Black and 36 White) where SaO2 values were sequentially decreased from 100 to 70%. The Pi values from that dataset were divided into two groups (Pi ≤ 1 or Pi > 1) for analysis. A Pi value ≤ 1 was considered “low perfusion” and a Pi value > 1 was considered “normal perfusion”. Statistical calculations included values of bias (mean difference of SpO2-SaO2), precision (standard deviation of the difference), and accuracy (root-mean-square error [ARMS]). During conditions of low perfusion (Pi ≤ 1, range [0.1 to 1]), overall bias and precision were + 0.48% ± 1.59%, while bias and precision were + 0.19 ± 1.53%, and + 0.91 ± 1.57%, for Black and White subjects, respectively. Results: During normal perfusion (Pi > 1, range [1 to 12]), overall bias and precision were + 0.18% ± 1.34%, while bias and precision were -0.26 ± 1.37%, and − 0.12 ± 1.31%, for Black and White subjects, respectively. ARMS was 1.37% in all subjects with normal perfusion and 1.64% in all subjects with low perfusion. Conclusion: Masimo SET® pulse oximeters with RD SET® sensors are accurate for individuals of both Black and White races when Pi is normal, as well as during conditions when Pi is low. The ARMS for all conditions studied is well within FDA standards. This study was conducted in healthy volunteers during well-controlled laboratory desaturations, and results could vary under certain challenging clinical conditions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Clinical conditions resulting in low peripheral perfusion are a recognized confounder of conventional pulse oximetry [1,2,3]. Early reports comparing the performance of different pulse oximeters during low perfusion demonstrated a variability in oxygen saturation (SpO2) accuracy between device brands [1, 2]. Some manufacturers have features to address low perfusion, such as indicators when pulse oximetry signals are not adequate. Masimo accounts for the potential errors resulting from low perfusion and other common confounders (e.g., motion) by developing advanced engineering design solutions and signal-processing techniques known as Masimo Signal Extraction Technology® (SET®). Recent reports suggested that pulse oximeter performance during poor perfusion can still vary amongst present-day device brands [4].
The effect of skin tone, and therefore race, on SpO2 accuracy is another topic of longstanding interest [5, 6]. Increased emphasis has been focused on this important subject since the 2020 publication by Sjoding, et al. [7]. In this report, investigators combined data from all pulse oximeter manufacturers together and retrospectively surveyed results from ICU patients across 178 hospitals, allowing as much as 10 min between the time stamps for SpO2 values measured by pulse oximetry and arterial blood gas saturation (SaO2) measurements made by CO-oximetry. The results showed a tendency for the SpO2 to read higher than SaO2 to a greater extent in Black patients than in White patients [7]. Furthermore, “occult hypoxemia”, defined by the investigators as a SpO2 reading 92–96% when the SaO2 was < 88%, was three times more common in Blacks than in Whites in this study [7]. Others found similar tendencies [8,9,10,11,12,13,14,15,16,17,18,19], but to less of an extent than that found by Sjoding, et al.
In response to these reports, we conducted a focused evaluation of the accuracy of Masimo SET® pulse oximeters with RD SET® sensors on healthy Black and White volunteers undergoing controlled desaturation studies in the laboratory [20]. The results revealed that Masimo SET® pulse oximeters deliver accurate values across the skin tone range, as the statistical bias (mean difference of SpO2-SaO2) and precision (standard deviation of difference) were − 0.20 + 1.40% for Black and − 0.05 + 1.35% for White subjects, and occult hypoxemia was rare and did not occur in Black subjects.
Recently, data from a well-known and longstanding pulse oximeter testing laboratory were reported in a non-peer reviewed preprint paper, which raised new concerns regarding the potential combined confounders of low perfusion coupled with dark skin pigmentation resulting in greater differences between SpO2 and SaO2 [21].
In light of these concerns, we performed a secondary analysis of the dataset presented in our recently published study on Black and White subjects undergoing controlled desaturations. The goal of this subgroup analysis is to assess the accuracy of Masimo SET® pulse oximetry with RD SET® sensors during conditions of normal and low perfusion for both Black and White subjects.
2 Methods
The Perfusion Index (Pi) data were retrospectively abstracted from electronic files collected during a laboratory desaturation study conducted between September 2015 and July 2021 and recently published in this journal [20].
The Pi is the measured ratio of pulsatile to the non-pulsatile signal in the plethysmography waveform of the infrared light emitting diode (LED). Masimo devices support a Pi ranging from 0.02 to 20%, as a non-invasive measure of the pulse strength of arteriolar blood volume interrogated by the pulse oximeter sensor. Pi is clearly related to peripheral tissue perfusion [22], but it also depends on other variables that affect local arteriolar volume, including vessel compliance [23].
This study analyzed 7183 paired SpO2-SaO2 samples (3201 Black and 3982 White) from 75 subjects (39 Black and 36 White) collected during a desaturation protocol wherein SaO2 values were sequentially decreased to obtain six stable plateau values between 100 and 70%. During each stable plateau, arterial blood gas (ABG) samples were obtained from a radial arterial cannula, and simultaneous SpO2 and Pi readings were recorded using Masimo RD SET® sensors (Masimo Corporation, Irvine, California). The ABG samples were analyzed on a Radiometer ABL-835 Flex CO-Oximeter (Radiometer Inc., Brea, California). The protocol included subject warming of the upper extremities and/or torso away from the pulse oximeter site. In addition, no subjects were actively cooled to decrease peripheral perfusion or Pi. The protocol was consistent with the ISO 80601-2-61 pulse oximetry standard and underwent review and approval by the Institutional Review Board of Ethical & Independent (E&I) Review Services (Lee’s Summit, MO).
Subjects who self-identified as Black had Massey Scale values ranging from 4 to 9 (median 6, interquartile range [IQR] 6–7), while those who self-identified as White ranged in Massey Scale values from 1 to 4 (median 2, IQR 2–3). Box plots representing the IQR of Massey Scale values for Black and White subjects are shown in Fig. 1, which show that the analysis was conducted on two distinct pigment groups. There was a median of 72 paired samples per subject for the Black population and 96 per subject for the White population. Additional details about the demographics, methodology, and results of the initial investigation can be found in the 2023 published study [20].

Box plots showing the interquartile range (IQR) of Massey Scale values for Black and White subjects. The box plot includes a horizontal red line within each box representing the median; the top and bottom of each box represent the upper and lower limits of the IQR, and the whiskers represent the minimum and maximum values (excluding outliers shown with red + symbol). (Color figure online)
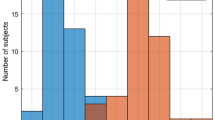
For this secondary evaluation, data are grouped by self-declared race (Black vs White) and perfusion status (Pi ≤ 1 or Pi > 1) for analysis. A Pi value ≤ 1 is considered “low perfusion” and a Pi value > 1 is considered “normal perfusion”. These values are comparable to the Pi thresholds for normal and low perfusion determined in previous studies [21, 22, 24]. The distribution of Pi values in this study is shown in Fig. 2. The Massey Scale distribution is further characterized by displaying the histogram of subjects contributing to the normal and low perfusion groups in Fig. 3a and b, respectively. Of the 75 subjects in the study, 73 subjects (37 Black and 36 White) contributed data to the normal perfusion group, while 35 subjects (21 Black and 14 White) contributed data to the low perfusion group. Note that 33 subjects had both normal and low perfusion data pairs obtained during different sample collections.

Pi distribution histogram (sample count on y-axis, Pi on x-axis) from self-identified Black (salmon tint bars) and White (blue tint bars) subjects. (Color figure online)

Massey Scale distribution histogram from self-identified Black (salmon tint bars) and self-identified White (blue tint bars) subjects contributing data to the Pi > 1 (Fig. 3a) and Pi ≤ 1 (Fig. 3b) groups. The vertical dashed lines indicate the IQR for each group. (Color figure online)
Statistical calculations include values of bias (mean difference of SpO2-SaO2), precision (standard deviation of the difference), and accuracy (root-mean-square error [ARMS]). Since the blood gas sampling procedure used replicates nested within each subject, the precision and ARMS are adjusted for repeated measures using a random effects model (MATLAB, fitlme function). This model provides equivalent results to those described in Bland and Altman [25], but it accounts for multiple sources of variation. The incidence of occult hypoxemia, defined by previous investigators as a SpO2 reading 92–96% when the SaO2 is < 88% [7], is also assessed during low perfusion conditions.
3 Results
Low perfusion (Pi ≤ 1) was registered in 624 of the 7183 SpO2-SaO2 data pairs during the desaturation study, while the remaining 6,559 data pairs had normal perfusion (Pi > 1). Figure 4 shows scatter plots of SpO2 versus SaO2 measured by CO-oximeter, along with the residual plots of the SpO2-SaO2 difference versus SaO2, for subjects with low perfusion (red dots, Pi ≤ 1), normal perfusion (black dots, Pi > 1), as well as the combined spectrum of Pi values (all data). In the scatter plots (Fig. 4a, b and c), the solid lines show linear regression best-fits, and the dotted lines indicate the ± standard deviation of the fit. The scatter plots for subjects with Pi ≤ 1 and for subjects with Pi > 1 are visually similar. In the residual plots (Fig. 4d, e and f), the solid lines show the mean difference of SpO2-SaO2 (bias), and the dotted lines indicate the limits of agreement. Bias and precision of subjects with low and normal perfusion are comparable at + 0.48 ± 1.59% and + 0.18 ± 1.34%, respectively, with low perfusion results slightly higher. Occult hypoxemia did not occur in any subjects during low perfusion (Fig. 4f). The mean SpO2-SaO2 difference between low and normal perfusion groups is + 0.3%, and the scatter distribution showed highly overlapping error distributions for both subjects with low and normal perfusion (Fig. 4a).

Scatter plot (SpO2 versus SaO2) along with performance metrics for all Pi data combined (a), Pi > 1 (b), and Pi ≤ 1 (c), as well as residual plot (SpO2-SaO2 versus SaO2) along with performance metrics for all Pi data combined (d), Pi > 1 (e), and Pi ≤ 1 (f). Red dots indicate Pi ≤ 1, black dots indicate Pi > 1. SEE = standard error estimate, Bias = mean SpO2-SaO2 difference, PRC = Precision (standard deviation of the bias). (Color figure online)
The mean SpO2-SaO2 difference (bias) and precision (standard deviation of the difference) obtained from Black, White, and all (combined) subjects with both low and normal perfusion are shown in Table 1, along with the number of data pairs and subjects in each group.
Table 2 shows a summary of the bias, precision, and accuracy (ARMS) obtained in Black and White subjects with Pi ≤ 1, Pi > 1, and all (combined) data during low oxygen saturation (SaO2 < 90%).
Subjects in both racial groups demonstrated a small positive bias during low perfusion (Pi ≤ 1) conditions, with White subjects experiencing greater bias (+ 0.91) than Black subjects (+ 0.19) during this condition. During normal perfusion (Pi > 1), both groups exhibited a small negative bias, with Black subjects experiencing a slightly greater bias (− 0.26) than White subjects (− 0.12). These results are graphically displayed in Fig. 5a. A plot of the difference between the biases (Δ bias) obtained for Black and White subjects at low (− 0.72) and normal (− 0.14) perfusion conditions is provided in Fig. 5b.

Bias (SpO2-SaO2) in Black (salmon tint bars) and White (blue tint bars) subjects with Pi ≤ 1 and Pi > 1 (Fig. 5a), and Fig. 5b similar plot showing the difference between the biases (Δ bias) of Black and White subjects. (Color figure online)
Scatter plots of SpO2-SaO2 (y-axis) versus SaO2 (x-axis) along with performance metrics for White subjects (blue dots, Fig. 6a) and Black subjects (salmon dots, Fig. 6b), are graphically displayed for both low (Pi ≤ 1) and normal (Pi > 1) peripheral perfusion groups. During low perfusion conditions, bias and precision are + 0.91 ± 1.57% for 14 White subjects (Fig. 6a) and + 0.19 ± 1.53% for 21 Black subjects (Fig. 6b), while under normal perfusion conditions, bias and precision are -0.12 ± 1.31% for 36 White subjects (Fig. 6a) and − 0.26 ± 1.37% for 37 Black subjects (Fig. 6b).

Scatter plot of SpO2-SaO2 versus SaO2, along with performance metrics for individual subjects with Pi ≤ 1 in White subjects (blue dots, Fig. 6a) and Black subjects (salmon dots, Fig. 6b). (Color figure online)
Each population included some data outliers, which were attributed to instability during the desaturation procedure. However, none of the outlier data points were excluded from this analysis. Figure 7 shows scatter plots of mean SpO2-SaO2 difference versus Pi plotted on a logarithmic scale for ease of comparison in the low range. The scatter did not exhibit any systematic bias trending with lower Pi in any of the population groups. Notably, Black individuals had a lower range of Pi values, with the lowest value = 0.14%, while the lowest recorded Pi value for White individuals was 0.36%.

4 Discussion
The data demonstrate that Masimo SET® pulse oximeters with RD SET® sensors are equally accurate when tested on healthy Black and White volunteers during conditions of normal as well as low peripheral perfusion. Under conditions of low perfusion (Pi ≤ 1), bias and precision were + 0.19 ± 1.53% for Black subjects and + 0.91 ± 1.57% for White subjects. In addition, the difference between the biases (mean difference of SpO2-SaO2) obtained from Black and White subjects during low perfusion was -0.71%. This difference is not likely to be relevant, because most commercially-available pulse oximeter devices display SpO2 only to the nearest 1%. In addition, occult hypoxemia did not occur in any subjects during low perfusion and occurred in only one data pair from a White subject during normal perfusion. Moreover, these results indicate an absence of racial differences in Masimo SET® pulse oximetry performance during conditions of poor perfusion in healthy volunteers. The overall accuracy (ARMS) based on entire dataset was 1.38%, 1.42% for Black, and 1.35% for White population, as reported previously [20]. During low perfusion conditions, the overall ARMS in all subjects was 1.64%. Notably, there were distribution outliers in both populations that are attributed to natural instability in the desaturation plateaus. However, we did not omit any of the outliers from the dataset.
The absence of relevant differences in SpO2-SaO2 between Black and White subjects throughout the Pi spectrum can be attributed to the engineering advancements of Masimo SET® pulse oximetry, which were designed to address the confounders of motion, low perfusion and skin pigment, as well as the calibration and validation paradigm utilized by Masimo. The U.S. FDA Guidance for medical-grade pulse oximeters requires only a minimum of two subjects, or 15% of the study pool, to have dark skin pigmentation during validation studies for 510(k) clearance. However, for over two decades, Masimo has adhered to a more stringent standard for evaluating the impact of skin pigment by calibrating and validating the performance of its devices using nearly equal numbers of dark skin and light skin individuals. The results of this study demonstrate that Masimo SET® technology is effective in minimizing the impact of low perfusion and skin pigment, enabling Masimo pulse oximeter devices to measure SpO2 accurately and reliably across the spectrum of perfusion conditions and skin tones.
The recent preprint manuscript from Gudelunas, et al. presented findings from a laboratory study that demonstrated greater pulse oximetry errors in dark-skinned subjects with low perfusion [21]. While the final version of the Gudelunas, et al. study had not completed peer review at the time of this publication, the preprint paper suggests several key methodology limitations. The study tested legacy (no longer manufactured) devices from Masimo and Nellcor, which could produce errant readings if paired with non-compliant sensors. Also, the methodology did not standardize sensor type or anatomic measurement site, as the Masimo device was tested using two different measurement sites (finger and ear), while the Nellcor device was tested using only the finger. In addition, it is unclear if measurements on different devices were collected simultaneously with two or more sensors on the same subject, which can lead to false readings from crosstalk interference without proper use of optical shielding [26]. Lastly, it is unclear whether the Pi data was properly standardized between the Masimo and Nellcor devices.
We believe the methodology utilized in our paper is scientifically robust; however, there are two notable limitations. First, this study used subjects who self-identified as being racially Black or White, and other ethnic groups (e.g., Asian, Hispanic) were not evaluated. However, study investigators included subjects whose skin pigmentation ranged across the spectrum (Massey Scale values 1 [minimal pigment] through 9 [very dark pigment]). Second, the data were collected from healthy volunteers using a controlled laboratory desaturation protocol; thus, clinical factors that can be observed in critically ill patients, such as tissue edema, anemia and hemoglobinopathies (e.g., sickle cell anemia, thalassemia, etc.) were not represented. However, controlling for these conditions helped minimize confounders that are present in clinical scenarios, allowing for greater focus on the topics of skin tone and Pi. Indeed, abnormal hemoglobin species (e.g., carboxyhemoglobin and methemoglobin) were measured and reported in the earlier paper by Barker and Wilson, and the values were similar (statistically the same) between Black and White groups [20]. Also, one can only ethically conduct desaturation studies using healthy volunteer subjects in a safe setting.
In conclusion, this secondary analysis of data from healthy Black and White volunteers demonstrated that Masimo RD SET® pulse oximeter sensors are accurate in both races during conditions of normal and low peripheral perfusion. Prospective clinical studies are recommended to further elucidate these results.
References
Morris RW, Nairn M, Torda TA. A comparison of fifteen pulse oximeters Part I: A clinical comparison; Part II: A test of performance under conditions of poor perfusion. Anaesth Intensive Care. 1989;17(1):62–73. https://doi.org/10.1177/0310057X8901700113.
Clayton DG, Webb RK, Ralston AC, Duthie D, Runciman WB. A comparison of the performance of 20 pulse oximeters under conditions of poor perfusion. Anaesthesia. 1991;46(1):3–10. https://doi.org/10.1111/j.1365-2044.1991.tb09303.x.
Webb RK, Ralston AC, Runciman WB. Potential errors in pulse oximetry. II. Effects of changes in saturation and signal quality. Anaesthesia. 1991;46(3):207–12. https://doi.org/10.1111/j.1365-2044.1991.tb09411.x.
Poorzargar K, Pham C, Ariaratnam J, Lee K, Parotto M, Englesakis M, Chung F, Nagappa M. Accuracy of pulse oximeters in measuring oxygen saturation in patients with poor peripheral perfusion: a systematic review. J Clin Monit Comput. 2022;36(4):961–73. https://doi.org/10.1007/s10877-021-00797-8.
Bickler PE, Feiner JR, Severinghaus JW. Effects of skin pigmentation on pulse oximeter accuracy at low saturation. Anesthesiology. 2005;102(4):715–9. https://doi.org/10.1097/00000542-200504000-00004.
Feiner JR, Severinghaus JW, Bickler PE. Dark skin decreases the accuracy of pulse oximeters at low oxygen saturation: the effects of oximeter probe type and gender. Anesth Analg. 2007;105(6 Suppl):S1823. https://doi.org/10.1213/01.ane.0000285988.35174.d9.
Sjoding MW, Dickson RP, Iwashyna TJ, Gay SE, Valley TS. Racial bias in pulse oximetry measurement. N Engl J Med. 2020;383:2477–8. https://doi.org/10.1056/NEJMc2029240.
Crooks CJ, West J, Morling JR, et al. Pulse oximeters’ measurements vary across ethnic groups: an observational study in patients with Covid-19 infection. Eur Respir J. 2022;59(4):2103246. https://doi.org/10.1183/13993003.03246-2021.
Fawzy A, Wu TD, Wang K, et al. Racial and ethnic discrepancy in pulse oximetry and delayed identification of treatment eligibility among patients With COVID-19. JAMA Intern Med. 2022. https://doi.org/10.1001/jamainternmed.2022.1906.
Valbuena VSM, Barbaro RP, Claar D, et al. Racial bias in pulse oximetry measurement among patients about to undergo extracorporeal membrane oxygenation in 2019–2020: a retrospective cohort study. Chest. 2022;161(4):971–8. https://doi.org/10.1016/j.chest.2021.09.025.
Wong AI, Charpignon M, Kim H, et al. Analysis of discrepancies between pulse oximetry and arterial oxygen saturation measurements by race and ethnicity and association with organ dysfunction and mortality. JAMA Netw Open. 2021;4(11):e2131674. https://doi.org/10.1001/jamanetworkopen.2021.31674.
Henry NR, Hanson AC, Schulte PJ, et al. Disparities in hypoxemia detection by pulse oximetry across self-identified racial groups and associations with clinical outcomes. Crit Care Med. 2022;50(2):204–11. https://doi.org/10.1097/CCM.0000000000005394.
Andrist E, Nuppnau M, Barbaro RP, Valley TS, Sjoding MW. Association of Race with pulse oximetry accuracy in hospitalized children. JAMA Netw Open. 2022;5(3):e224584. https://doi.org/10.1001/jamanetworkopen.2022.4584.
Gottlieb ER, Ziegler J, Morley K, Rush B, Celi LA. Assessment of racial and ethnic differences in oxygen supplementation among patients in the intensive care unit. JAMA Intern Med. 2022;182(8):849–58. https://doi.org/10.1001/jamainternmed.2022.2587.
Crooks CJ, West J, Morling JR, Simmonds M, Juurlink I, Briggs S, Cruickshank S, Hammond-Pears S, Shaw D, Card TR, Fogarty AW. Differential pulse oximetry readings between ethnic groups and delayed transfer to intensive care units. QJM. 2023;116(1):63–7. https://doi.org/10.1093/qjmed/hcac218.
Sudat SEK, Wesson P, Rhoads KF, Brown S, Aboelata N, Pressman AR, Mani A, Azar KMJ. Racial disparities in pulse oximeter device inaccuracy and estimated clinical impact on COVID-19 treatment course. Am J Epidemiol. 2022;29:164. https://doi.org/10.1093/aje/kwac164.
Valbuena VS, Seelye S, Sjoding MW, Valley TS, Dickson RP, Gay SE, Claar D, Prescott HC, Iwashyna TJ. Racial bias and reproducibility in pulse oximetry among medical and surgical inpatients in general care in the Veterans Health Administration 2013–19: multicenter, retrospective cohort study. BMJ. 2022;6:378. https://doi.org/10.1136/bmj-2021-069775.
Burnett GW, Stannard B, Wax DB, et al. Self-reported race/ethnicity and intraoperative occult hypoxemia: a retrospective cohort study. Anesthesiology. 2022;136(5):688–96. https://doi.org/10.1097/ALN.0000000000004153.
Chesley CF, Lane-Fall MB, Panchanadam V, et al. Racial disparities in occult hypoxemia and clinically based mitigation strategies to apply in advance of technological advancements. Respir Care. 2022. https://doi.org/10.4187/respcare.09769.
Barker SJ, Wilson WC. Racial effects on Masimo pulse oximetry: a laboratory study. J Clin Monit Comput. 2023;37(2):567–74. https://doi.org/10.1007/s10877-022-00927-w.
Gudelunas MK, Lipnick MS, Hendrickson CM, Vanderburg S, Okunlola B, Auchus I, Feiner JR, Bickler PE. Low perfusion and missed diagnosis of hypoxemia by pulse oximetry in darkly pigmented skin: a prospective study. medRxiv. 2022. https://doi.org/10.1213/ANE.0000000000006755.
Lima AP, Beelen P, Bakker J. Use of a peripheral perfusion index derived from the pulse oximetry signal as a noninvasive indicator of perfusion. Crit Care Med. 2002;30(6):1210–3. https://doi.org/10.1097/00003246-200206000-00006.
Coutrot M, Dudoignon E, Joachim J, Gayat E, Vallée F, Dépret F. Perfusion index: physical principles, physiological meanings and clinical implications in anaesthesia and critical care. Anaesth Crit Care Pain Med. 2021;40(6):100964. https://doi.org/10.1016/j.accpm.2021.100964.
Ozakin E, Yazlamaz NO, Kaya FB, Karakilic EM, Bilgin M. Perfusion index measurement in predicting hypovolemic shock in trauma patients. J Emerg Med. 2020;59(2):238–45. https://doi.org/10.1016/j.jemermed.2020.04.010.
Bland JM, Altman DG. Agreement between methods of measurement with multiple observations per individual. J Biopharm Stat. 2007;17(4):571–82. https://doi.org/10.1080/10543400701329422.
Kyriacou PA. Optical crosstalk and other forms of light interference in pulse oximeter comparison studies. J Clin Monit Comput. 2023. https://doi.org/10.1007/s10877-023-01060-y.
Acknowledgements
Authors would like to thank the following individuals for their significant contributions to this paper: Ammar Al-Ali, Walter Weber, Jerry Novak, Fenghua Tian, Ahmed Alghazi, Jennifer Pipp, and Thomas Doupe.
Funding
The only funding body was Masimo Corporation.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception, design, material preparation, data collection and analysis. The first draft of the manuscript was written by WCW, and VS, SJB, RS, LP all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
Vikrant Sharma, Rebecca Sorci, Linus Park and William C. Wilson are full-time paid employees of Masimo. Steven J. Barker is a part-time employee of Masimo.
Ethical approval
Data in this study were reported as part of a 2017 ClinicalTrials.gov-registered validation study (NCT03124602) of Masimo RD SET® sensors conducted in Masimo laboratories. Approval was granted by the Institutional Review Board of Ethical & Independent Review Services (E&I).
Consent to participate
Informed consent was obtained from all individual subjects included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sharma, V., Barker, S.J., Sorci, R. et al. Racial effects on masimo pulse oximetry: impact of low perfusion index. J Clin Monit Comput 38, 347–354 (2024). https://doi.org/10.1007/s10877-023-01113-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-023-01113-2