
Abstract
Purpose
Hidradenitis suppurativa (HS) is a chronic inflammatory skin disease that affects up to 1% of the population in Europe. The EQ-5D is the most commonly used generic instrument for measuring health-related quality of life among HS patients. This study aims to compare the measurement properties of the two adult versions of EQ-5D (EQ-5D-3L and EQ-5D-5L) in patients with HS.
Methods
We recruited 200 consecutive patients with HS (mean age 37 years, 38% severe or very severe HS) to participate in a multicentre cross-sectional survey. Patients completed the EQ-5D-3L, EQ-5D-5L, Dermatology Life Quality Index (DLQI) and Skindex-16 questionnaires.
Results
More than twice as many different health state profiles occurred in the EQ-5D-5L compared to the EQ-5D-3L (101 vs. 43). A significant reduction in ceiling effect was found for the mobility, self-care and usual activities dimensions. A good agreement was established between the EQ-5D-3L and EQ-5D-5L with an intraclass correlation coefficient of 0.872 (95% CI 0.830–0.903; p < 0.001) that was confirmed by a Bland-Altman plot. EQ-5D-5L improved both the absolute and relative informativity in all dimensions except for anxiety/depression. EQ-5D-3L and EQ-5D-5L demonstrated similar convergent validity with DLQI and Skindex-16. EQ-5D-5L was able to better discriminate between known groups of patients based on the number of comorbidities and disease severity (HS-Physician's Global Assessment).
Conclusion
In patients with HS, the EQ-5D-5L outperformed the EQ-5D-3L in feasibility, ceiling effects, informativity and known-groups validity for many important clinical characteristics. We recommend using the EQ-5D-5L in HS patients across various settings, including clinical care, research and economic evaluations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hidradenitis suppurativa (HS) is a chronic, inflammatory, recurrent skin disease that usually starts after puberty with painful, deep-seated lesions [1]. It typically affects the apocrine gland-bearing areas of the body, most commonly the axillary, inguinal and anogenital regions [2]. An average prevalence of up to 1% and a mean incidence of 6.0 per 100,000 person‐years have been reported in Europe [3,4,5,6]. Observed comorbidities fall into several categories: cardiovascular diseases, inflammatory and autoimmune diseases, hormone-related disorders and psychiatric illnesses [7, 8]. Therapeutic approaches currently include the use of topical therapies, systemic antibiotics, hormonal therapies, surgical options and biologics, such as adalimumab and infliximab (the latter currently off-label) [2, 9]. Patients often experience a substantial diagnostic delay of up to 7 years that represents a serious burden to both patients and healthcare systems [10,11,12,13].
Patients are likely to have a severely impaired health-related quality of life (HRQoL) due to the clinical symptoms of HS, associated comorbidities and side effects of treatments [14,15,16]. While disease-specific (e.g. HS Quality of Life [HS-QoL and HiSQOL] and HIDRAdisk [17,18,19,20]) and skin-specific HRQoL measures (e.g. Dermatology Life Quality Index, DLQI and Skindex instruments) are widely used in patients with HS [15], less empirical research has been conducted on general HRQoL in this patient population. The most commonly used instrument for measuring general HRQoL among HS patients is the EQ-5D questionnaire [15]. A main advantage of the EQ-5D health status measure is that it can be used to derive preference-based index scores for economic evaluations of health interventions [21]. In many countries, including the US, Canada, and numerous European countries, the EQ-5D is the recommended outcome measure to estimate quality-adjusted life years (QALYs) in cost-effectiveness analyses [22, 23]. Furthermore, being a generic HRQoL measure, the EQ-5D allows comparisons with general population normative data and across various patient populations, also outside of dermatology.
The economic burden of HS has received an increasing attention from healthcare providers and policymakers since 2015, when a biological drug, adalimumab was introduced in the treatment of HS [24,25,26]. In the US, for example, seven-month costs associated with adalimumab therapy amount to $63,953 (in 2018 prices) [27, 28]. Cost-effectiveness analyses weigh the costs and benefits (i.e. HRQoL improvement) of new treatments to guide financial decisions in healthcare. Having a central role in these analyses, EQ-5D results can help to demonstrate the value of these treatments, and hence, to improve patients’ access to new treatment approaches.
There are two adult versions of the EQ-5D, the EQ-5D-3L (hereafter 3L) developed in 1990 and the newer, EQ-5D-5L (hereafter 5L) that has been available since 2009 [29, 30]. A number of studies applied and validated the 3L in HS patients, whereas the use of the 5L is less common in this patient population [31,32,33,34,35,36]. So far, no head-to-head comparison studies have been performed to compare the measurement properties of the 3L and 5L among patients with skin diseases other than psoriasis [37,38,39].
The objective of the current study was to compare the measurement properties of the 3L and 5L descriptive systems of the EQ-5D in a common sample of patients with HS. We aim to test the following measurement properties: feasibility, agreement, ceiling effects, redistribution properties, inconsistency in responses, informativity, convergent and known-groups validity.
Methods
Study design and patient population
Between September 2017 and October 2019, we carried out a cross-sectional survey at three academic dermatology clinics in Hungary [40]. The inclusion criteria to this study were as follows: (i) ≥ 18 years of age; (ii) cognitive ability to understand the questionnaire; (iii) diagnosis of HS by a dermatologist; and (iv) signing a consent form prior to the data collection. The Scientific and Ethical Committee of the Medical Research Council in Hungary granted permission for conducting this study (ref. #40579-2/2017/EKU).
Data were collected through paper-based questionnaires completed by patients and their dermatologists. Patients were asked about socio-demographic characteristics, general health status and HRQoL. Each patient rated their current and worst HS-related pain intensity on a 10-cm-long, horizontal VAS from 0 (no pain at all) to 10 (pain as bad as it could be). Patients were also asked to assess their severity using the Patient’s Global Assessment (PtGA) VAS providing a range of scores from 0 to 100, where 0 indicated ‘not severe at all’ and 100 represented ‘very severe’.
Dermatologists provided information about clinical characteristics, comorbidities and affected body sites (i.e. localisation). Disease severity was evaluated by the following three measures: Hurley staging [41], HS-Physician’s Global Assessment (HS-PGA) [42] and Modified Sartorius Score [43].
Health-related quality of life measures
We used the validated Hungarian versions of standardised HRQoL measures. We measured general HRQoL by using the 3L, 5L and EQ visual analogue scale (EQ VAS). Following prior work [44], patients filled in the 5L before the 3L, in order to prevent the underuse of levels 2 and 4 on the 5L, and two skin-specific questionnaires were placed between the 5L and the 3L. The EQ VAS was completed only once (that of the 5L version).
For quantifying skin-specific HRQoL, we used Dermatology Life Quality Index (DLQI) and Skindex-16. These two skin-specific instruments assess quite different areas of HRQoL: while the DLQI mainly focuses on functional impairments, Skindex-16 is considered better at capturing the emotional and mental aspects of the skin disease [45, 46].
EQ-5D-3L and EQ-5D-5L
The EQ-5D is a generic measure of health status that comprises of two parts: a descriptive system and the EQ VAS [29]. The descriptive system focuses on five dimensions of health (mobility, self-care, usual activities, pain/discomfort and anxiety/depression). The EQ VAS records self-rated health on a 20-cm-long vertical health thermometer anchored at 0 (‘the worst health you can imagine’) to 100 (‘the best health you can imagine’). The timeframe of the questionnaire is the day of the completion (i.e. ‘your health today’.)
The 3L has three response levels for each dimension (no problems = 1, some/moderate problems = 2, extreme problems/unable to/confined to bed = 3) providing 243 unique health states [29]. The 5L has five levels for each dimension (no problems = 1, slight problems = 2, moderate problems = 3, severe problems = 4 and unable to/extreme problems = 5) allowing a total of 3125 distinct health states [30]. Note that wording of the most severe level of mobility in 3L ‘confined to bed’ is changed to ‘unable to walk about’ in the 5L, and the middle levels are also standardised to consistently use ‘moderate’ in all dimensions of the 5L. In addition to these changes, there are a number of other minor differences between the Hungarian 3L and 5L versions that affect both modifiers [e.g. ‘very strong’(3L) vs. ‘extreme’(5L)] and descriptors [e.g. ‘anxiety/feeling down’(3L) vs. ‘anxiety/depression’(5L)] [47].
We computed index scores using the Hungarian value sets, where 3L and 5L index scores have been derived parallel from a representative sample of the Hungarian general population using composite time trade-off approach [47]. The scoring range for the 3L and 5L are from 1 (‘11111’, full health) to − 0.865 (‘33333’ on the 3L) and − 0.848 (‘55555’ on the 5L), respectively. An index score of zero indicates dead, and negative values represent health states worse than dead.
Dermatology Life Quality Index (DLQI)
DLQI is the most widely used HRQoL instrument in clinical practice and research in patients with skin diseases [48]. It consists of 10 items covering the following aspects of health over the past week: symptoms and feelings, daily activities, leisure, work or school, personal relationships and treatment. Each item is scored on a four-point scale: ‘not at all’ or ‘not relevant’ = 0, ‘a little’ = 1, ‘a lot’ = 2 and ‘very much’ = 3. DLQI total score is calculated by summing the score of each item, resulting in a maximum score of 30, where a higher score refers to a worse HRQoL.
Skindex-16
Skindex-16 is skin-specific HRQoL instrument with a one-week recall period [49]. It comprises 16 items, each is rated on a 7-item bipolar scale, where the endpoints are labelled ‘never bothered’ and ‘always bothered’. The responses are categorised into three subscales: symptoms (items 1–4), emotions (items 5–11) and functioning (items 12–16). Subscale scores are transformed to a linear scale of 0-100, where higher scores indicate more impaired levels of HRQoL.
Statistical analyses
Data analysis was built on previous studies that compared the measurement properties of the 3L and 5L in other patient and general population samples [39, 44, 50,51,52].
Feasibility and ceiling effects
Feasibility was determined by examining the percentage of missing responses by dimension. The proportion of missing data was documented, and no missing imputation technique was performed. Histograms were plotted to visualise the empirical distributions of the 3L and 5L index scores. To assess ceiling effects, we computed the proportion of patients having ‘no problems’ on one or all dimensions (‘11111’) and compared them between the 3L and 5L by using McNemar’s test. We expected a reduction in those selecting ‘no problems’ for the 5L compared to the 3L due to the two extra response levels. Both absolute and relative (%) reduction in ceiling effects were determined when moving from 3L to 5L.
Agreement
A Bland-Altman plot was drawn to visualise the agreement between the 3L and 5L [53]. The intraclass correlation coefficient (ICC) was used as an index of parallel forms reliability that reflects both the degree of correlation and agreement between the 3L and 5L [54]. The ICC represents the proportion of total variance that is attributable to the differences between individuals, as opposed to the differences between the two instruments (3L and 5L). ICC values were calculated using a two-way random model with absolute agreement [55]. We rated ICC values as poor if 0–0.39, fair if 0.40–0.59, good if 0.60–0.74 and excellent if 0.75–1 [56].
Redistribution properties
We assessed redistribution properties from 3L to 5L by cross-tabulating 3L-5L response pairs. We computed the proportion of consistent and inconsistent 3L-5L response pairs. We considered levels 1, 3 and 5 in the 5L descriptive system matched pairs of the 1, 2 and 3 levels in the 3L. Thus, 3L responses differing at least two levels from their 5L pairs were considered ‘inconsistent’ [44]. For example, a patient reports ‘some problems washing or dressing’ (level 2) in the 3L and ‘unable to wash or dress’ in the 5L (level 5). The average size of inconsistency was assessed according to the following weights: 0 = 3L responses are not more than one level away from their 5L pairs, 1 = 3L responses are two levels away from their 5L pairs, 2 = 3L responses are three levels away from their 5L pairs and 3 = 3L responses are four levels away from their 5L pairs [44].
Informativity
We hypothesised that the 5L with its two extra levels improves discriminatory power of the 3L in terms of informativity [57]. Shannon’s (H') and Shannon’s evenness (J') indices were used to assess informativity of each of the five dimensions [58, 59]. H’ represents the extent to which the information is evenly distributed across all responses. J' combines the evenness of a distribution and the number of response levels used. H' and J' were calculated using the following formulas, where L refers to the number of levels in a dimension of the descriptive system, and pi is the proportion of patients reporting their health in the ith level:
H′ values range between 0 and log2L (= 1.58 for the 3L and 2.32 for the 5L), where higher the H′, the more informative the item and the better the discriminatory power are. J′ can take values between 0 (i.e. all responses are concentrated in one response level; worst discriminatory power) and 1 (i.e. even distribution across response levels; best discriminatory power) [39].
Convergent and validity
Spearman’s rank order correlations were conducted to explore the convergent validity of the five dimensions and index scores with other scales. We hypothesised the EQ-5D dimensions and index scores to moderately correlate with EQ VAS, DLQI and Skindex-16, and weakly with disease severity measures, including HS-PGA, Modified Sartorius Score and PtGA VAS [31, 33, 35]. For pain scales, we hypothesised a moderate or strong correlation with the pain/discomfort dimension and index scores of the EQ-5D and a weak correlation with all other dimensions [60,61,62]. Correlation coefficients (ρ) were interpreted as very weak (< 0.20), weak (0.20–0.39), moderate (0.40–0.59) and strong correlation (0.60 ≤) [63].
Known-groups validity
Known-groups validity was examined by comparing subsets of patients defined based on clinical characteristics. We hypothesised that patients with higher body mass index (BMI), with more comorbidities, inguinal or perianal localisation or higher disease severity have lower EQ-5D index scores [31,32,33, 35, 64,65,66,67]. We used Mann–Whitney and Kruskal Wallis tests to look for differences in 3L and 5L index scores between groups. For each known group, we estimated effect sizes according to the following formulas:
where k denotes the number of groups and n refers to the sample size. Effect size values were considered as small if ≥ 0.01, moderate if ≥ 0.06 and large if ≥ 0.14 [68]. Then, relative efficiency (RE) was computed as the ratio of the ESs of the 5L and 3L index scores. A RE value of > 1 indicated that the 5L was more efficient in discriminating between known groups compared to the 3L. All the statistics were two-sided, and p < 0.05 was considered statistically significant. Data were analysed with Stata 13 (StataCorp, TX, USA).
Results
Patient characteristics
A total of 200 consecutive patients with HS participated in the survey (Table 1). The majority of the patients were male (61.5%), and the mean age was 37.13 ± 12.43 years. Mean disease duration was 4.76 ± 6.72 years. Overall, 46.0% of the patients had at least one comorbidity, with cardiovascular disease (16.5%), acne vulgaris (7.0%), inflammatory bowel disease (7.0%), diabetes (6.0%) and psychiatric illness (6.0%) being the most commonly reported. A total of 80.7% of the patients were overweight or obese (BMI ≥ 25). Almost half of the patients had Hurley III stage disease (48.5%). According to HS-PGA scores, over one-third of the patients had severe or very severe HS (Table 1).
Feasibility
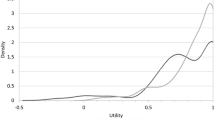
One patient did not complete the 5L questionnaire, and there were two partially incomplete 3L and one 5L descriptive systems. There were two missing values on the EQ VAS. For 3L, 43 distinct health state profiles were observed versus 101 for the 5L. There was a great dispersion of both 3L and 5L profiles among HS patients with few clustering. One and 10 patients had negative index scores in the 3L and 5L, respectively. There were more patients between index scores of 0.2 to 0.6 and 0.7 to 0.8 with the 3L, whereas the 5L allowed more observations for mild (index score 0.9-1) and very severe health states (index score < 0.2) (Fig.1).

Distribution of EQ-5D-3L and EQ-5D-5L index scores
Ceiling effects
Patients reported the most problems with pain/discomfort (‘any problems’: 75.4% in 3L and 77.4% in 5L), while the least problems occurred with self-care (‘no problems’: 19.5% in 3L and 18.3% in 5L) (Table 2). Absolute reduction in ceiling effects was the highest for self-care (8.8%), whereas relative reduction was the highest for usual activities (15.5%). We found increased ceiling effects for the 5L in the dimension of anxiety/depression with absolute and relative increases of 5.0% and 11.4%, respectively. Ceiling effect reduction was statistically significant for the mobility, self-care and usual activities dimensions. The proportion of ‘11111’ profiles decreased from 16.0% on the 3L to 14.6% on the 5L. The absolute and relative ceiling effect reductions in the proportion of full health (‘11111’) responses were 1.4% and 9.4%, respectively. There were four (2.0%) ‘the best health you can imagine’ (= 100) and no ‘the worst health you can imagine’ (= 0) responses on the EQ VAS.
Agreement
A good agreement was established between the 3L and 5L with an ICC of 0.872 (95% CI 0.830–0.903; p < 0.001). This finding was supported by the Bland-Altman plot (Fig. 2). Mean 3L index scores of HS patients were higher than those of the 5L (0.78 ± 0.21 and 0.76 ± 0.30; p < 0.031). Differences between 3L and 5L index scores tended to increase at lower mean index scores. Below the index score of 0.5, a higher 3L index score was found for almost all 3L-5L index score pairs falling out of the 95% limits of agreement.

Bland-Altman plot of the EQ-5D-3L and EQ-5D-5L index scores in HS. The horizontal line represents the mean of the differences (d) between 3L and 5L index scores, while the 95% limits of agreement, obtained as d ± 1.96 *SD of d, are indicated by dashed lines
Redistribution properties and inconsistencies
Responses covered nearly all levels for both EQ-5D versions (Table 3). There were 79 (8.0%) inconsistent response pairs, provided by 21 (10.5%) patients. The size of inconsistency was generally low, ranging from 1.00 (self-care, usual activities and pain/discomfort) to 1.2 (anxiety/depression). The rate of inconsistent 3L-5L response pairs varied between 3.5% (mobility and self-care) and 15.1% (anxiety/depression) (Table 2).
Informativity
The 5L improved the absolute discriminatory power (H') of the questionnaire in all dimensions (3L: 0.71 to 1.38 vs. 5L: 1.25 to 2.06) indicating that the two extra levels of the 5L were effectively used (Table 2). Similarly, the relative discriminatory power (J') increased for all dimensions (3L: 0.45 to 0.87 vs. 5L: 0.54 to 0.89) with the exception of anxiety/depression (3L: 0.87 vs. 5L: 0.77). The average H' and J' values improved when moving from the 3L (H' = 1.11 and J' = 0.70) to the 5L (H' = 1.73 and J' = 0.74).
Convergent validity
The results supported the majority of our hypotheses, with some interesting exceptions; for example, the EQ-5D pain/discomfort dimensions and index scores correlated strongly with the DLQI and the functioning subscale of Skindex-16 (Table 4). Furthermore, the self-care and mobility dimensions of the EQ-5D demonstrated weak correlations with the symptoms and emotions subscales of Skindex-16.
When comparing the 3L and 5L, index scores of both measures showed moderate correlations with EQ VAS (0.535 vs. 0.592). The 5L exhibited stronger correlations with EQ VAS for all dimensions except for anxiety/depression (range of coefficients: − 0.449 to − 0.350 for the 3L and − 0.505 to − 0.385 for the 5L). The 5L produced stronger correlations in the dimensions of mobility, self-care and pain/discomfort with DLQI and all Skindex-16 subscale scores. However, 3L index scores correlated stronger with DLQI and all Skindex-16 subscale scores, with the exception of the symptoms subscale. Considering disease severity scales, the 5L resulted in a stronger correlation with PtGA VAS (5/5 dimensions), Modified Sartorius Score (3/5 dimensions) and HS-PGA (2/5 dimensions). The 5L demonstrated a better convergent validity with current pain intensity VAS for four dimensions, including the pain/discomfort dimension (3L: 0.534 vs. 5L: 0.591). Three dimensions of the 3L, including pain/discomfort, were better correlated with the worst pain intensity VAS scores than those of the 5L. The correlations between index scores and pain scales revealed an improved performance of the 3L and 5L with worst and current pain intensities, respectively.
Known-groups validity
Comparisons across known groups of patients provided consistent evidence for most of our hypotheses with the exception of the impact of perianal localisation on HRQoL. Contrasting the 3L and 5L, in almost every subgroups of patients, the mean 5L index scores were lower, while the medians were higher than their respective mean and median 3L index scores (Table 5). Patients with gluteal or inguinal localisation or more severe disease, as assessed by the Hurley classification system or HS-PGA, had more impaired HRQoL on both the 3L and 5L. In addition, the 5L detected significantly lower index scores in patients with more comorbidities. Effect sizes were mostly small or moderate. Known-groups validity analysis resulted in insignificant difference between groups defined by the majority of localisations both with the 3L and 5L versions. Overall, the 5L was able to better discriminate between known groups of patients based on the number of comorbidities, HS-PGA groups and inguinal localisation (RE > 1), whereas the 3L exhibited a better known-groups validity for body mass index, Hurley stages and gluteal localisation (RE < 1).
Discussion
This study aimed to compare the measurement performance of two adult versions (3L and 5L) of the EQ-5D questionnaire in a sample of patients diagnosed with HS. A considerable proportion of HS patients were able to report more problems on the 5L than on the 3L, particularly for mobility, self-care and usual activities dimensions. We found reduced ceiling effects, improved informativity and better known-groups validity for many relevant clinical characteristics for the 5L.
Both acute and chronic pain are common problems reported in HS, and pain medication is usually necessary to improve health outcomes in these patients [69]. Among the five dimensions, the most problems occurred in pain/discomfort, whereby 75.4% (3L) to 77.4% (5L) reported to have ‘any problems’. The pain/discomfort dimension of both the 3L and 5L showed a moderate or moderate-to-strong correlation with current and the worst pain VAS scores suggesting that pain is well captured by the pain/discomfort domain of the EQ-5D. This corroborates with the literature in patients with skin burn, arthritis and Crohn’s disease [60,61,62].
Ceiling effects were smaller on the 5L for all dimensions with the exception of anxiety/depression, whereby ceiling effects increased by 5.0%. Furthermore, the AD dimension of the 3L showed a stronger correlation with most other outcome measures than that of the 5L. This may be attributable to the different wording used in the descriptor of AD in the Hungarian 3L (3L: ‘anxiety/feeling down’ vs. 5L: ‘anxiety/depression’). This corresponds to previous findings from a 3L-5L comparison study with psoriasis patients in Hungary, whereby the AD dimension of the 3L correlated stronger with both the EQ VAS and DLQI [37].
We found lower mean index scores in the 5L than in the 3L. As the two Hungarian value sets were developed in a parallel valuation study from a common sample using the same preference elicitation technique (i.e. composite time trade-off) and modelling approach, the majority of the differences between index scores are attributable to the differences in wording between the two descriptive systems [47]. This difference between 3L and 5L index scores tended to increase at lower values (Fig. 2). For example, we observed a large difference between the average 3L and 5L index scores in patients with ‘severe’ and ‘very severe’ HS-PGA (0.79 vs. 0.73 and 0.62 vs. 0.53), whereas mean index scores were nearly identical with the two questionnaire versions for the milder severity groups. This suggests that an estimated health gain from an improvement from a ‘very severe’ to ’mild’ HS-PGA health state is substantially larger with the 5L (0.32) than with the 3L (0.22), possibly leading to more favourable cost-effectiveness estimates for HS treatments.
Strengths of the study include the multicentre design, the diverse patient population and the large number of outcome measures available to assess disease severity, pain and HRQoL in HS. The lack of any HS-specific HRQoL instruments available in Hungarian language and the relatively small proportion of patients with lower EQ-5D index scores may be considered as limitations of the study. Moreover, a substantial proportion of patients in the sample had severe HS. On the one hand, we believe that the distribution of the sample across severity groups well represents the treated HS population at large in Hungary, since this was a multicentre study carried out at three academic dermatology clinics. HS patients are almost exclusively treated at these institutions, as systemic and surgical treatments are only available here. On the other hand, the precise epidemiology of HS in Hungary is currently unknown. Compared to the baseline characteristics of HS patients in large international registries [70,71,72,73], the proportion of patients with severe HS is higher in our sample that might somewhat limits the external generalizability of the results. A further limitation concerns the positioning of the 3L and 5L within the wider questionnaire caused an ordering effect. The last limitation is that we could not compare the responsiveness and test-retest reliability of the 3L and 5L due to the cross-sectional nature of the study.
In conclusion, our work suggests that the 5L outperforms the 3L version of the EQ-5D in many measurement properties. We recommend the use of the 5L in HS patients across various settings, including clinical care, research and economic evaluations. Future work is recommended to focus on other measurement properties, such as responsiveness, test-retest reliability and comparing the acceptability of the two descriptive systems in terms of ease of understanding and better reflection of health status in this patient population.
Data availability
All data of this study are available from the corresponding author upon reasonable request.
References
Sabat, R., Jemec, G. B. E., Matusiak, L., Kimball, A. B., Prens, E., & Wolk, K. (2020). Hidradenitis suppurativa. Nature Reviews Disease Primers, 6(1), 18.
Zouboulis, C. C., Desai, N., Emtestam, L., Hunger, R. E., Ioannides, D., Juhasz, I., et al. (2015). European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. Journal of the European Academy of Dermatology and Venereology, 29(4), 619–644.
Kirsten, N., Petersen, J., Hagenstrom, K., & Augustin, M. (2020). Epidemiology of hidradenitis suppurativa in Germany - an observational cohort study based on a multisource approach. Journal of the European Academy of Dermatology and Venereology, 34(1), 174–179.
Theut Riis, P., Pedersen, O. B., Sigsgaard, V., Erikstrup, C., Paarup, H. M., Nielsen, K. R., et al. (2019). Prevalence of patients with self-reported hidradenitis suppurativa in a cohort of Danish blood donors: a cross-sectional study. British Journal of Dermatology, 180(4), 774–781.
Nguyen, T. V., Damiani, G., Orenstein, L. A. V., Hamzavi, I., & Jemec, G. (2020). Hidradenitis Suppurativa: An Update on Epidemiology, Phenotypes, Diagnosis, Pathogenesis, Comorbidities and Quality of Life. Journal of the European Academy of Dermatology and Venereology. https://doi.org/10.1111/jdv.16677
Killasli, H., Sartorius, K., Emtestam, L., & Svensson, A. (2020). Hidradenitis Suppurativa in Sweden: A Registry-Based Cross-Sectional Study of 13,538 Patients. Dermatology, 1-8.
Fimmel, S., & Zouboulis, C. C. (2010). Comorbidities of hidradenitis suppurativa (acne inversa). Dermatoendocrinol, 2(1), 9–16.
Dauden, E., Lazaro, P., Aguilar, M. D., Blasco, A. J., Suarez, C., Marin, I., et al. (2018). Recommendations for the management of comorbidity in hidradenitis suppurativa. Journal of the European Academy of Dermatology and Venereology, 32(1), 129–144.
Ingram, J. R., Collier, F., Brown, D., Burton, T., Burton, J., Chin, M. F., et al. (2019). British Association of Dermatologists guidelines for the management of hidradenitis suppurativa (acne inversa) 2018. British Journal of Dermatology, 180(5), 1009–1017.
Saunte, D. M., Boer, J., Stratigos, A., Szepietowski, J. C., Hamzavi, I., Kim, K. H., et al. (2015). Diagnostic delay in hidradenitis suppurativa is a global problem. British Journal of Dermatology, 173(6), 1546–1549.
Loget, J., Saint-Martin, C., Guillem, P., Kanagaratnam, L., Becherel, P. A., Nassif, A., et al. (2018). [Misdiagnosis of hidradenitis suppurativa continues to be a major issue. The R-ENS Verneuil study]. Annales de Dermatologie et de Vénéréologie, 145(5), 331-338.
Ingram, J. R. (2020). The epidemiology of hidradenitis suppurativa. British Journal of Dermatology, 183(6), 990–998.
Kokolakis, G., Wolk, K., Schneider-Burrus, S., Kalus, S., Barbus, S., Gomis-Kleindienst, S., et al. (2020). Delayed diagnosis of hidradenitis suppurativa and its effect on patients and healthcare system. Dermatology, 236(5), 421–430.
Matusiak, L. (2018). Profound consequences of hidradenitis suppurativa: A review. British Journal of Dermatology, 183(6), e171–e177.
Chernyshov, P. V., Zouboulis, C. C., Tomas-Aragones, L., Jemec, G. B., Svensson, A., Manolache, L., et al. (2019). Quality of life measurement in hidradenitis suppurativa: position statement of the European Academy of Dermatology and Venereology task forces on Quality of Life and Patient-Oriented Outcomes and Acne, Rosacea and Hidradenitis Suppurativa. Journal of the European Academy of Dermatology and Venereology, 33(9), 1633–1643.
Gooderham, M., & Papp, K. (2015). The psychosocial impact of hidradenitis suppurativa. Journal of the American Academy of Dermatology, 73(5 Suppl 1), S19-22.
Chiricozzi, A., Bettoli, V., De Pita, O., Dini, V., Fabbrocini, G., Monfrecola, G., et al. (2019). HIDRAdisk: an innovative visual tool to assess the burden of hidradenitis suppurativa. Journal of the European Academy of Dermatology and Venereology, 33(1), e24–e26.
Kirby, J. S., Thorlacius, L., Villumsen, B., Ingram, J. R., Garg, A., Christensen, K. B., et al. (2019). The Hidradenitis Suppurativa Quality of Life (HiSQOL) score: development and validation of a measure for clinical trials. British Journal of Dermatology
Pinard, J., Vleugels, R. A., Joyce, C., Merola, J. F., & Patel, M. (2018). Hidradenitis suppurativa burden of disease tool: Pilot testing of a disease-specific quality of life questionnaire. Journal of the American Academy of Dermatology, 78(1), 215-217.e212.
Sisic, M., Kirby, J. S., Boyal, S., Plant, L., McLellan, C., & Tan, J. (2017). Development of a Quality-of-Life Measure for Hidradenitis Suppurativa. J Cutan Med Surg, 21(2), 152–155.
Rabin, R., & de Charro, F. (2001). EQ-5D: A measure of health status from the EuroQol Group. Annals of Medicine, 33(5), 337–343.
Rencz, F., Gulacsi, L., Drummond, M., Golicki, D., Prevolnik Rupel, V., Simon, J., et al. (2016). EQ-5D in central and Eastern Europe: 2000–2015. Quality of Life Research, 25(11), 2693–2710.
Kennedy-Martin, M., Slaap, B., Herdman, M., van Reenen, M., Kennedy-Martin, T., Greiner, W., et al. (2020). Which multi-attribute utility instruments are recommended for use in cost-utility analysis? A review of national health technology assessment (HTA) guidelines. The European Journal of Health Economics, 21(8), 1245–1257.
Tappenden, P., Carroll, C., Stevens, J. W., Rawdin, A., Grimm, S., Clowes, M., et al. (2017). Adalimumab for treating moderate-to-severe hidradenitis suppurativa: An evidence review group perspective of a nice single technology appraisal. Pharmacoeconomics, 35(8), 805–815.
Argyropoulou, M., Kanni, T., Kyprianou, M., Melachroinopoulos, N., & Giamarellos-Bourboulis, E. J. (2019). Cost-savings of adalimumab in hidradenitis suppurativa: a retrospective analysis of a real-world cohort. British Journal of Dermatology, 180(5), 1161–1168.
Willems, D., Charokopou, M., Evers, S., & Hiligsmann, M. (2020). Early health economic modelling for a treatment candidate in hidradenitis suppurativa. J Med Econ [Epub ahead of print]. https://doi.org/10.1080/13696998.2020.1840181, 1.
Yang, E. J., Beck, K. M., Bhutani, T., Feldman, S. R., & Shi, V. Y. (2019). Pharmacy costs of systemic medications for hidradenitis suppurativa in the United States. Journal of Dermatological Treatment, 30(5), 519–521.
Matusiak, Ł, Jemec, G. B., & Szepietowski, J. C. (2019). Pharmacological development in hidradenitis suppurativa. Current Opinion in Pharmacology, 46, 65–72.
EuroQol--a new facility for the measurement of health-related quality of life (1990). Health Policy, 16(3), 199-208.
Herdman, M., Gudex, C., Lloyd, A., Janssen, M., Kind, P., Parkin, D., et al. (2011). Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res, 20(10), 1727–1736.
Matusiak, L., Bieniek, A., & Szepietowski, J. C. (2010). Psychophysical aspects of hidradenitis suppurativa. Acta Dermato Venereologica, 90(3), 264–268.
Vinding, G. R., Knudsen, K. M., Ellervik, C., Olesen, A. B., & Jemec, G. B. (2014). Self-reported skin morbidities and health-related quality of life: a population-based nested case-control study. Dermatology, 228(3), 261–268.
Riis, P. T., Vinding, G. R., Ring, H. C., & Jemec, G. B. (2016). Disutility in patients with hidradenitis suppurativa: A cross-sectional study using EuroQoL-5D. Acta Dermato Venereologica, 96(2), 222–226.
Hamzavi, I. H., Sundaram, M., Nicholson, C., Zivkovic, M., Parks-Miller, A., Lee, J., et al. (2017). Uncovering burden disparity: A comparative analysis of the impact of moderate-to-severe psoriasis and hidradenitis suppurativa. Journal of the American Academy of Dermatology, 77(6), 1038–1046.
Kjaersgaard Andersen, R., Theut Riis, P., & Jemec, G. B. E. (2018). Factors predicting the self-evaluated health of hidradenitis suppurativa patients recruited from an outpatient clinic. Journal of the European Academy of Dermatology and Venereology, 32(2), 313–317.
Sampogna, F., Abeni, D., Gieler, U., Tomas Aragones, L., Lien, L., & Poot, F., et al. (2020). Exploring the EQ-5D Dimension of Pain/Discomfort in Dermatology Outpatients from a Multicentre Study in 13 European Countries. Acta Dermato Venereologica, 100(8), adv00120.
Poor, A. K., Rencz, F., Brodszky, V., Gulacsi, L., Beretzky, Z., Hidvegi, B., et al. (2017). Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L in psoriasis patients. Quality of Life Research, 26(12), 3409–3419.
Yfantopoulos, J., Chantzaras, A., & Kontodimas, S. (2017). Assessment of the psychometric properties of the EQ-5D-3L and EQ-5D-5L instruments in psoriasis. Archives of Dermatological Research, 309(5), 357–370.
Buchholz, I., Janssen, M. F., Kohlmann, T., & Feng, Y. S. (2018). A systematic review of studies comparing the measurement properties of the three-level and five-level versions of the EQ-5D. Pharmacoeconomics, 36(6), 645–661.
Gergely, L. H., Gáspár, K., Brodszky, V., Kinyó, Á., Szegedi, A., Remenyik, É., et al. (2020). Validity of EQ-5D-5L, Skindex-16, DLQI and DLQI-R in patients with hidradenitis suppurativa. Journal of the European Academy of Dermatology and Venereology, 34(11), 2584–2592.
Hurley, H. (1989). Dermatologic surgery, principles and practice. Dermatologic surgery, principles and practice. Marcel Dekker, New York, 729-739.
Kimball, A. B., Kerdel, F., Adams, D., Mrowietz, U., Gelfand, J. M., Gniadecki, R., et al. (2012). Adalimumab for the treatment of moderate to severe Hidradenitis suppurativa: a parallel randomized trial. Annals of Internal Medicine, 157(12), 846–855.
Sartorius, K., Emtestam, L., Jemec, G. B., & Lapins, J. (2009). Objective scoring of hidradenitis suppurativa reflecting the role of tobacco smoking and obesity. Br J Dermatol, 161(4), 831–839.
Janssen, M. F., Birnie, E., Haagsma, J. A., & Bonsel, G. J. (2008). Comparing the standard EQ-5D three-level system with a five-level version. Value Health, 11(2), 275–284.
Both, H., Essink-Bot, M. L., Busschbach, J., & Nijsten, T. (2007). Critical review of generic and dermatology-specific health-related quality of life instruments. J Invest Dermatol, 127(12), 2726–2739.
Paudyal, P., Apfelbacher, C., Jones, C., Siddiqui, S., El-Turki, A., DeGiovanni, C., et al. (2020). "DLQI Seems to be 'Action', and Skindex-29 Seems to be 'Emotion'": Qualitative Study of the Perceptions of Patients with Psoriasis or Eczema on Two Common Dermatology-specific Quality of Life Measures. Acta Dermato Venereologica, 100(8), adv00105.
Rencz, F., Brodszky, V., Gulácsi, L., Golicki, D., Ruzsa, G., Pickard, A. S., et al. (2020). Parallel valuation of the EQ-5D-3L and EQ-5D-5L by Time trade-off in Hungary. Value Health, 23(9), 1235–1245.
Finlay, A. Y., & Khan, G. K. (1994). Dermatology Life Quality Index (DLQI)–a simple practical measure for routine clinical use. Clinical and Experimental Dermatology, 19(3), 210–216.
Chren, M. M., Lasek, R. J., Sahay, A. P., & Sands, L. P. (2001). Measurement properties of Skindex-16: a brief quality-of-life measure for patients with skin diseases. Journal of Cutaneous Medicine and Surgery, 5(2), 105–110.
Janssen, M. F., Pickard, A. S., Golicki, D., Gudex, C., Niewada, M., Scalone, L., et al. (2013). Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Quality of Life Research, 22(7), 1717–1727.
Thompson, A. J., & Turner, A. J. (2020). A Comparison of the EQ-5D-3L and EQ-5D-5L. Pharmacoeconomics, 38(6), 575–591.
Kangwanrattanakul, K., & Parmontree, P. (2020). Psychometric properties comparison between EQ-5D-5L and EQ-5D-3L in the general Thai population. Quality of Life Research, 29(12), 3407–3417.
Bland, J. M., & Altman, D. G. (1986). Statistical methods for assessing agreement between two methods of clinical measurement. Lancet, 1(8476), 307–310.
Koo, T. K., & Li, M. Y. (2016). A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine, 15(2), 155–163.
Shrout, P. E., & Fleiss, J. L. (1979). Intraclass correlations: uses in assessing rater reliability. Psychol Bull, 86(2), 420–428.
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychological Assessment, 6(4), 284.
Bas Janssen, M. F., Birnie, E., & Bonsel, G. J. (2007). Evaluating the discriminatory power of EQ-5D, HUI2 and HUI3 in a US general population survey using Shannon’s indices. Quality of Life Research : An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 16(5), 895–904.
Shannon, C. E. (1948). A mathematical theory of communication. Bell System Technical Journal, 27(3), 379–423.
Shannon, C. E., & Weaver, W. (1949). The mathematical theory of communication.
Rencz, F., Lakatos, P. L., Gulacsi, L., Brodszky, V., Kurti, Z., Lovas, S., et al. (2019). Validity of the EQ-5D-5L and EQ-5D-3L in patients with Crohn’s disease. Quality of Life Research, 28(1), 141–152.
Bilbao, A., García-Pérez, L., Arenaza, J. C., García, I., Ariza-Cardiel, G., Trujillo-Martín, E., et al. (2018). Psychometric properties of the EQ-5D-5L in patients with hip or knee osteoarthritis: reliability, validity and responsiveness. Quality of Life Research, 27(11), 2897–2908.
Spronk, I., Bonsel, G. J., Polinder, S., van Baar, M. E., Janssen, M. F., & Haagsma, J. A. (2020). Exploring the relation between the EQ-5D-5L pain/discomfort and pain and itching in a sample of burn patients. Health Qual Life Outcomes, 18(1), 144.
Swinscow, T. D. V., & Campbell, M. J. (2002). Statistics at square one: Bmj London. 0727915525
Jørgensen, A. R., Holm, J. G., Ghazanfar, M. N., Yao, Y., Ring, H. C., & Thomsen, S. F. (2020). Factors affecting quality of life in patients with hidradenitis suppurativa. Archives of Dermatological Research, 312(6), 427–436.
Kluger, N., Ranta, M., & Serlachius, M. (2017). The Burden of Hidradenitis Suppurativa in a Cohort of Patients in Southern Finland: A Pilot Study. Skin Appendage Disorders, 3(1), 20–27.
Alavi, A., Anooshirvani, N., Kim, W. B., Coutts, P., & Sibbald, R. G. (2015). Quality-of-life impairment in patients with hidradenitis suppurativa: a Canadian study. American Journal of Clinical Dermatology, 16(1), 61–65.
Katoulis, A. C., Liakou, A. I., Rotsiamis, N., Bonovas, S., Bozi, E., Rallis, E., et al. (2017). Descriptive epidemiology of hidradenitis suppurativa in greece: A study of 152 cases. Skin Appendage Disorders, 3(4), 197–201.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Abingdon. United Kingdom: Routledge.
Horváth, B., Janse, I. C., & Sibbald, G. R. (2015). Pain management in patients with hidradenitis suppurativa. Journal of the American Academy of Dermatology, 73(5 Suppl 1), S47-51.
Bettoli, V., Cazzaniga, S., Scuderi, V., Zedde, P., Di Landro, A., & Naldi, L. (2019). Hidradenitis suppurativa epidemiology: from the first Italian registry in 2009 to the most recent epidemiology updates - Italian Registry Hidradenitis Suppurativa project 2. Journal of the European Academy of Dermatology and Venereology, 33(Suppl 6), 4–6.
Grimstad, O., Tzellos, T., Dufour, D. N., Bremnes, O., Skoie, I. M., Snekvik, I., et al. (2019). Evaluation of medical and surgical treatments for hidradenitis suppurativa using real-life data from the Scandinavian registry (HISREG). Journal of the European Academy of Dermatology and Venereology, 33(6), 1164–1171.
Kimball, A. B., Crowley, J. J., Papp, K., Calimlim, B., Duan, Y., Fleischer, A. B., et al. (2020). Baseline patient-reported outcomes from UNITE: an observational, international, multicentre registry to evaluate hidradenitis suppurativa in clinical practice. Journal of the European Academy of Dermatology and Venereology, 34(6), 1302–1308.
Prens, E. P., Lugo-Somolinos, A. M., Paller, A. S., Kerdel, F., Duan, Y., Teixeira, H. D., et al. (2020). Baseline characteristics from UNITE: An observational, international, multicentre registry to evaluate Hidradenitis Suppurativa (Acne Inversa) in clinical practice. American Journal of Clinical Dermatology, 21(4), 579–590.
Acknowledgements
The authors are grateful for their current and former colleagues and students for their contribution to the data collection or questionnaire development: András Bánvölgyi, Márta Péntek, László Gulácsi, Szimonetta Dropsa, Dávid Fehér and Viktoria Vig.
Funding
Open Access funding provided by Corvinus University of Budapest. This research was supported by the Higher Education Institutional Excellence Program 2020 of the Ministry for Innovation and Technology in Hungary in the framework of the 'Financial and Public Services' research project (TKP2020-IKA-02) at the Corvinus University of Budapest.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design, interpretation of data and critical revision of the manuscript. Data collection was performed by LHG, KG, ÁK and NK. Data analysis was performed by AB, VB, ÁS, ZB and FR. The manuscript was drafted by AB and FR. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
In connection to this article, AB, FR and ZB have received grant support from the Higher Education Institutional Excellence Program 2020 of the Ministry of Human Capacities in the framework of the ‘Financial and Public Services’ research project (TKP2020-IKA-02) at the Corvinus University of Budapest. All other authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Scientific and Ethical Committee of the Medical Research Council in Hungary (Reference No. 40579-2/2017/EKU).
Informed consent
Informed consent was obtained from all patients included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bató, A., Brodszky, V., Gergely, L.H. et al. The measurement performance of the EQ-5D-5L versus EQ-5D-3L in patients with hidradenitis suppurativa. Qual Life Res 30, 1477–1490 (2021). https://doi.org/10.1007/s11136-020-02732-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-020-02732-x