
Abstract
Identifying correlates of treatment response may help to improve outcomes for adolescents and young people with substance use disorder (SUD). We assessed treatment response in an adolescent/young person-specific community-based residential SUD programme located in NSW, Australia. Participants (N = 100) were aged 16–24 years and recruited between 2018 and 2020 from a cohort study investigating treatment outcomes over time. We assessed treatment response using available data at 1-year follow-up (n = 24). Approximately one third (n = 9) of participants were classified as responders at 1-year follow-up (i.e. scoring below the clinical cut-off on the Brief Symptom Inventory Global Severity Index). At treatment entry, responders had higher levels of self-efficacy (d = 1.04), better functional status (d = 1.09), and less borderline personality disorder (BPD) symptoms (d = 1.26). Exploratory whole-sample analyses indicated over half of participants (56%) screened positively for a diagnosis of BPD at treatment entry, which was associated with more severe global psychiatric symptoms (d = .85), poorer functional status, (d = .76), lower self-efficacy (d = .73), higher substance use severity (d = .46), yet better cognitive functioning (d = .75). Findings suggest that comorbid BPD is common in this setting and may contribute to poorer outcomes for adolescents and young people with SUD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Globally, substance use disorder (SUD) in young people is diverse in its prevalence, onset, and course, though there is consensus that use in this sensitive developmental period is associated with increased burden of disease (Degenhardt et al., 2016) and adverse long-term outcomes (McCabe et al., 2022). Earlier initiation of substance use (e.g. in adolescents aged 12–17 years) increases the risk of transitioning to SUD (Volkow et al., 2021). In Australia, thirty percent of young people aged 14–24 drink alcohol at risky levels at least monthly and nearly one quarter have engaged in illicit drug use over a 12-month period (AIHW, 2020). Evidence-based approaches for prevention, early intervention, and treatment of SUD in adolescents and young people are a significant area of need given the potential impacts of substance use on neuromaturation (Luciana & Feldstein Ewing, 2015; Squeglia, 2020) and psychosocial growth during this rapid period of development that marks the transition from puberty to adulthood (Gray & Squeglia, 2018).
In contrast to adult SUD populations, treatment studies for young people with SUD are scarce (Stockings et al., 2016). A recent review included studies published between 2016 and 2019 and highlighted that family-based approaches, cognitive behavioural therapy (CBT), and multicomponent interventions (i.e. family-based or CBT approaches combined with motivational interviewing and/or contingency management) have the strongest level of evidence supporting them as well-established interventions for adolescent SUD (Fadus et al., 2019), in line with the previous reviews of outpatient SUD treatments for adolescents (Hogue et al., 2014, 2018; Waldron & Turner, 2008). In a recent overview of reviews on outpatient psychosocial interventions for young people (including adolescents) with SUD, 43 reviews were identified from 1990 to 2018. Despite the volume of evidence, only six reviews were rated as moderate-high methodological quality, raising concerns about the validity of the evidence base (Snowdon et al., 2019).
In contrast to outpatient interventions, residential SUD treatments are more intensive and provide a level of care suited to people experiencing severe and complex SUD who may present with cooccurring psychosocial complexities and/or psychiatric comorbidities (Reif et al., 2014). Typically, these are multicomponent treatments including psychosocial interventions, milieu-based therapy, vocational training, accommodation, and medical care integrated in community, hospital, or prison settings. A number of reviews have charted the evidence for community-based residential treatment studies over the past 20 years (Brunette et al., 2004; Cleary et al., 2009; de Andrade et al., 2019; Drake et al., 2008; Malivert et al., 2012; Reif et al., 2014; Smith et al., 2006; Vanderplasschen et al., 2012), though the quality of evidence varies due to methodological heterogeneity. Most studies involve adult and, less frequently, young adult populations. In contrast, though it is recommended that services are specifically targeted to young people rather than being integrated into adult services (Christie et al., 2020), there are fewer studies of community-based residential treatment programmes designed specifically for adolescents and/or young people. One review of community-based residential treatment for adolescent populations highlighted several methodological weaknesses and mixed findings of the eight included studies from 1990 to 2009 (Tripodi, 2009). More recent studies provide evidence to support this treatment modality (Marceau et al., 2021a, 2021b; Uliaszek et al., 2019a, 2019b), though stability of these outcomes over time is inconclusive (Edelen et al., 2009).
Though there is a lack of consensus regarding its definition in SUD research, treatment retention is commonly associated with improved outcomes in SUD treatment (Dacosta‐Sánchez et al., 2022; Turner & Deane, 2016) resulting in many studies seeking to identify factors associated with treatment completion and/or non-completion, including dropout. Four of the most consistent dropout risk factors are younger age, the presence of personality disorder, cognitive deficits, and lower levels of treatment alliance (Brorson et al., 2013). The first meta-analysis in this area estimated a high overall dropout rate of 30% and identified several predictors ranging from SUD-related variables, participant demographics, and treatment characteristics (Lappan et al., 2020). Significantly, this meta-analysis included studies of adult populations (i.e. > 18 years), but adolescent-specific treatments were excluded.
Relatively fewer studies have examined dropout risk factors in residential SUD treatment programmes specifically targeting adolescents and young people. A recent study predicting dropout reported associations with more severe adolescent emotional and social difficulties, less parental involvement in treatment, and challenges with parenting during childhood and adolescence in combination with mental health and substance use difficulties during adolescence (Uliaszek et al., 2019a, 2019b). Conversely, adolescents who report greater levels of therapeutic engagement show increased treatment retention (Abdel-Salam & Gunter, 2014). Admission characteristics of having commercial health insurance, a family history of SUD, living with only one biological parent, and a history of physical or sexual abuse were associated with non-completion for male adolescents (Neumann et al., 2010).
In line with studies of treatment retention, investigating the issue of treatment response more broadly is a perennial issue in psychotherapy research (Lambert, 2013). An overarching aim is to match the most beneficial treatment to a particular individual (e.g. in the treatment of depression: Cohen & DeRubeis, 2018). There are multiple ways to investigate treatment response, including studies investigating the characteristics of those who show clinical improvement (i.e. responders) in contrast to those who do not (i.e. nonresponders). Studies of treatment response in residential SUD programmes specifically targeting adolescents and young people are relatively sparse compared to the adult literature. Some studies have focused on young adult populations in adult residential treatment settings; for example, polysubstance use and attention deficit hyperactivity disorder are associated with treatment nonresponse (Andersson et al., 2021). Other studies have focused on treatment mechanisms in residential settings; for example, how changes in proposed mechanisms influence outcome (Kelly et al., 2011) and the role of the therapeutic alliance (Urbanoski et al., 2012) for young adults.
Given the importance of studying treatment response in residential settings specifically for the treatment of SUD in young people, the aims of the current study were as follows: First, we sought to determine rates of treatment response in a community-based residential programme for young people aged 16–24 years with SUD. Second, to investigate potential concomitants, we assessed the influence of pre-treatment characteristics including sociodemographics, substance use characteristics and severity, psychiatric symptom severity, borderline personality disorder, cognitive functioning, self-efficacy, and functional status, as well as treatment duration, on treatment response. Third, we conducted exploratory analyses to investigate the influence of identified concomitants of treatment response, including effects on outcomes at 1-year follow-up.
Methods
Participants
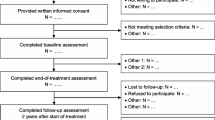
Participants were recruited into the Triple Care Farm (TCF) cohort study of young people in residential SUD treatment comprising milieu therapy and group dialectical behaviour therapy over a 10-year period (Marceau et al., 2021b). Specifically, we used data from cohort B (N = 100; data collection period: 2018–2020) to investigate treatment response and nonresponse in this sample. Cohort B data were utilised as it included a longitudinal follow-up at 1-year, allowing us to examine durable effects of treatment. Participants were recruited from TCF, a community-based residential treatment programme for young people aged 16–24 years located in the NSW Southern Highlands, Australia. The treatment model at TCF is a 12-week holistic psychosocial programme incorporating general principles from milieu treatment, individual and group therapy, and structured worker-resident activities throughout the day and evening. The setting is a forested farm with residential huts and common areas. It is non-religious and has a health-based multidisciplinary focus. It is a voluntary service without inpatient care and no secure offender facilities. The 12-week residential treatment programme is followed by community aftercare. Referrals to the programme are received Australia-wide, and most young people entering the service are self-referrals. Participants were eligible for the study if they received a diagnosis of substance use disorder upon referral to treatment, were aged 16–24 years, had completed detoxification prior to treatment entry to the residential programme, and had fluency in English to a level needed to understand study requirements (Marceau et al., 2021b). The participant cohort in this study were previously assessed at the following time points: baseline; 6 weeks (mid-treatment); 12 weeks (end-of-treatment); 6 months; and 1 year. We have previously reported on changes in primary and secondary outcomes over time (Marceau et al., 2021b). For the purposes of the current study, we used all available data at 1-year follow-up (n = 24) to calculate treatment response.
Ethics approval was granted by the University of Wollongong Health and Medical Human Research Ethics Committee (reference 2017/233) and the Aboriginal Health and Medical Research Council (AH&MRC; reference 1319/17). During recruitment of cohort B, adult participants (i.e. those aged 18 years and older) provided written informed consent following a full explanation of study procedures (n.b., for participants under 18 years of age, legal guardians provided consent, while these participants provided assent to participate in the study).
Measures
Clinical Assessment
Following routine intake assessment, participants took part in a semi-structured interview conducted by a research assistant (psychologist) to obtain sociodemographic and substance use characteristics.
Substance Use Severity
The Severity of Dependence Scale (SDS; Gossop et al., 1995) is a self-report questionnaire used to measure severity of use for participants’ primary problematic substance. Participants rated 5 items on a scale from 0 to 3 (example items include “How strong is your desire or craving to use the substance?” and “Have you experienced any problems as a result of your substance use?”). Higher scores indicate more severe substance dependence.
Psychiatric Symptom Severity
The Brief Symptom Inventory (BSI; Derogatis, 1993) was used to measure psychiatric symptoms. This 53-item self-report questionnaire consists of nine subscales (somatisation, obsessive compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism) and three global indices (Global Severity Index, Positive Symptoms Distress Index, Positive Symptoms Total). Participants indicated how much each item had distressed or bothered them during the past 7 days (including today) on a scale from 0 to 4 (example items include “Feeling no interest in things” and “Feeling so restless you couldn’t sit still”). Higher scores indicate more severe psychiatric symptoms.
Borderline Personality Disorder
Participants completed the McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD), a validated BPD diagnosis screening tool (Zanarini et al., 2003). In this 10-item self-report scale, participants provide a yes/no response to indicate whether they have experienced symptoms over the past 2 weeks (example item: “Have any of your closest relationships been troubled by a lot of arguments or repeated breakups?”). Consistent with the previous reports, scores greater than or equal to seven were used as a clinical cut-off to indicate the presence of BPD (Zanarini et al., 2003).
Specific BPD symptoms were assessed during a semi-structured interview. Participants rated the severity of all BPD symptoms over the past 2 weeks on a scale from 1 to 6 (from 1 “none of the time” to 6 “all of the time”) as per DSM-5 criteria (American Psychiatric Association, 2013). Higher scores indicate more severe BPD symptoms. This method shows reliability and validity as a dimensional measure of BPD symptoms (Miller et al., 2018; Woodbridge et al., 2021).
Cognitive Functioning
The Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005) was used as a brief measure of overall cognitive functioning. The MoCA was originally developed to detect mild cognitive impairment in dementia populations but is now widely used in other clinical populations including SUD populations (Marceau et al., 2016). Domains assessed include executive function, working memory, short-term memory, language, and visuospatial ability, and the outcome measure for the current study was total MoCA score, with higher scores indicating better cognitive functioning.
Self-Efficacy
The Brief Situational Confidence Questionnaire (BSCS; Breslin et al., 2000) was used to assess self-efficacy. During this 8-item self-report questionnaire, participants are presented with scenarios including possible precipitants to relapse and must rate their confidence from 0 to 100 in resisting relapse (example item: “Urges and temptations e.g. if I suddenly had an urge to drink or use drugs; if I were in a situation where I had often used drugs or drank heavily; if I began to think of how good a rush or high had felt”). Higher scores indicate greater self-efficacy to resist using drugs.
Functional Status
The World Health Organisation Quality of Life-8 (The WHOQOL Group, 1998) is an 8-item self-report questionnaire developed from the World Health Organisation Quality of Life Instrument Abbreviated Version. Participants rate their functioning from 1 to 5 over the past 2 weeks across a range of domains influencing quality of life (example items include “Do you have enough energy for everyday life?” and “How satisfied are you with your ability to perform daily living activities?”). Higher scores indicate better functioning.
Treatment Duration
This variable was represented by total days spent in treatment.
Treatment Response
The BSI Global Severity Index was designated as the primary outcome measure in the previous cohort study (Marceau et al., 2021b) and was therefore used to calculate treatment response and nonresponse in the present study. To maximise available data at the 1-year follow-up endpoint of the study, treatment response and nonresponse were designated by using the established clinical cut-off for the BSI Global Severity Index (i.e. scores ≥ 63). Data were available for n = 24 participants at 1-year follow-up, which represented an attrition rate of 51% based on the subsample of follow-up assessments due during the funding period (Marceau et al., 2021b). Participants with clinically significant levels of psychiatric symptoms at 1-year follow-up were considered nonresponders, while participants scoring in the normal range were considered to show a favourable treatment response.
Statistical Analyses
Analyses were performed using IBM Statistical Package for the Social Sciences (SPSS version 29.0; IBM Corp, 2022). During data cleaning, Little’s Missing Completely at Random (MCAR; Little, 1988) test was non-significant (chi-square = 267.838, df = 281, p = 0.704); thus, we assumed no non-random patterns for missing values.
To investigate concomitants of treatment response, a series of between-group comparisons of responders versus nonresponders were performed using t-tests and chi-squared tests, with non-parametric alternatives used where necessary.
Further exploratory analyses were conducted to investigate the influence of identified concomitants of treatment response and nonresponse, including effects on outcomes at 1-year follow-up. Specifically, this involved additional between-group comparisons as above, bivariate correlations, and a multiple linear regression model to predict outcome at 1-year follow-up.
Results
Rates of Treatment Response
Using the Brief Symptom Inventory Global Severity Index clinical cut-off, we found that 62.5% of young people (n = 15) were classified as nonresponders at 1-year follow-up, resulting in only approximately one third of young people (37.5%; n = 9) showing a favourable response to treatment.
Characteristics Associated with Treatment Response
To investigate concomitants of treatment response, we assessed the influence of pre-treatment variables including sociodemographics, substance use characteristics and severity, psychiatric symptoms, borderline personality disorder, cognitive functioning, self-efficacy, and functional status, as well as treatment duration. Specifically, we conducted a between-group comparison of these characteristics for responders versus nonresponders at 1-year follow-up (see Table 1).
Sociodemographics
Sociodemographic characteristics at treatment entry did not significantly differ between groups. Participants were of a similar age (nonresponders: M = 20.3 years; responders: M = 20.9 years) and primarily male (86.7% of nonresponders (n = 13); 66.7% of responders (n = 6)). Similar levels of education were observed (nonresponders: M = 9.9 completed school years; responders: M = 10.7 completed school years), and most participants were unemployed (66.7% of nonresponders (n = 10); 77.8% of responders (n = 7)), living in rental accommodation (73.3% of nonresponders (n = 11); 77.8% of responders (n = 7)), and single (73.3% of nonresponders (n = 11); 77.8% of responders (n = 7)) at the time of treatment entry.
Substance Use Characteristics and Severity
There were no significant between-group differences in substance use characteristics and severity. Approximately half of the sample reported cannabis as their primary substance of concern at treatment entry (53.3% of nonresponders (n = 8); 50.0% of responders (n = 4)), while approximately one third of responders (37.5% (n = 3)) reported amphetamine-type stimulants, and one quarter of nonresponders (26.7% (n = 4)) reported alcohol. Severity indicators over 3 months prior to treatment entry showed low levels of injecting drug use for both groups (0% of nonresponders; 16.7% of responders (n = 1)), with approximately one third of participants overdosing from any drug (36.4% of nonresponders (n = 4); 33.3% of responders (n = 2)), and a small percentage being arrested (18.2% of nonresponders (n = 2); 16.7% of responders (n = 1)). Both groups showed severe levels of dependence based on pre-treatment Severity of Dependence Scale (SDS) scores (nonresponders: M = 10.2; responders: M = 10.7).
Psychiatric Symptoms
Global psychiatric symptoms were in the clinical range (scores ≥ 63) for both groups at treatment entry (Brief Symptom Inventory Global Severity Index (BSI GSI): nonresponders: M = 73.8; responders: M = 67.8). As BSI GSI was used to classify treatment response at 1-year follow-up, the absence of a significant pre-treatment difference suggested that both groups commenced treatment with comparable symptom severity. Similarly, global positive symptoms (BSI Positive Symptoms Distress Index (PSD) and Positive Symptoms Total (PST)) did not significantly differ between groups (BSI PSD: nonresponders: M = 69.5; responders: M = 64.3; BSI PST: nonresponders: M = 70.8; responders: M = 64.8). Moreover, BSI subscale scores, as indicators of specific psychiatric symptom patterns, indicated no significant differences between groups. There was, however, a trend (p = 0.063) toward nonresponders showing greater severity of depression symptoms (M = 72.5) compared to responders (M = 62.8) at treatment entry.
Borderline Personality Disorder Symptom Count
The number of pre-treatment borderline personality disorder (BPD) symptoms endorsed based on the McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD) was significantly higher for nonresponders (M = 8.0) compared to responders (M = 5.7), representing a large effect (p = 0.022, d = 1.26).
Cognitive Functioning
Assessment of cognition at treatment entry indicated that both groups showed similar levels of cognitive functioning (nonresponders: M = 27.3; responders: M = 27.4).
Self-Efficacy
Nonresponders reported significantly lower self-efficacy at treatment entry (M = 33.8) in contrast to responders (M = 56.6), representing a large effect (p = 0.044, d = 1.04).
Functional Status
Pre-treatment functional status was significantly lower for nonresponders (M = 2.4) compared to responders (M = 3.3), representing a large effect (p = 0.035, d = 1.09).
Treatment Duration
The total number of days spent in treatment was similar for both groups (nonresponders: M = 55.0 days; responders: M = 57.4 days), indicating a comparable treatment dose.
Exploratory Analyses: Impact of BPD on Treatment Response and Outcomes
Given that global severity of BPD symptoms at treatment entry displayed the largest effect in distinguishing responders from nonresponders, we conducted further exploratory analyses to better understand the expression and impact of BPD symptoms in the current sample.
Firstly, we used the MSI-BPD clinical cut-off (i.e. scores ≥ 7) to estimate the prevalence of BPD in the total sample at treatment entry. Over half of participants (n = 56: 56%) screened positively for a potential diagnosis of BPD. Between-group comparison of pre-treatment characteristics for young people with and without a potential comorbid BPD diagnosis is presented in Table 2, including basic sociodemographics, primary substance of concern and substance use severity, global psychiatric symptom severity, cognitive functioning, self-efficacy, and functional status, as well as treatment duration. The comorbid BPD group was significantly younger (M = 20.3) than the SUD-only group (M = 21.2, p = 0.043, d = 0.41), but there were no between-group differences regarding gender, education level, or primary substance of concern. Both groups also spent a comparable length of time in treatment (SUD-only: M = 51.6 days; comorbid BPD: M = 48.6 days). Severity of global psychiatric symptoms was significantly higher for the comorbid BPD group (M = 71.9) compared to the SUD-only group (M = 62.6), representing a large effect (p = < 0.001, d = 0.85). Participants with comorbid BPD also reported significantly higher levels of substance use severity (M = 10.1) compared to their SUD-only counterparts (M = 8.7), representing a medium effect (p = 0.049, d = 0.46). Medium-large effects were also found for functional status (SUD-only: M = 3.5; comorbid BPD: M = 3.0; p = 0.001, d = 0.76), self-efficacy (SUD-only: M = 54.8; comorbid BPD: M = 37.2; p = 0.002, d = 0.73), and cognition (SUD-only: M = 25.3; comorbid BPD: M = 27.2; p = 0.003, d = 0.75), with the comorbid BPD group showing poorer functioning, lower self-efficacy, and better cognitive functioning than the SUD-only group at treatment entry.
Next, we assessed the influence of specific symptoms of BPD on treatment response. Specifically, we compared ratings of pre-treatment symptom severity in responders versus nonresponders. Table 3 shows the profile of BPD symptom severity for each group. Nonresponders had significantly higher severity in two symptom domains: “unstable relationships” (M = 4.4, p = 0.019, d = 1.07) and “paranoid ideation” (M = 4.7, p = 0.021, d = 1.05) compared to responders (M = 2.4 and M = 3.0, respectively), representing large effects.
In the final stage of our exploratory analyses, we assessed the impact of pre-treatment BPD symptom severity on outcomes measured at 1-year follow-up. Initially, we used bivariate correlations to explore possible associations between specific BPD symptom severity and substance use severity, self-efficacy, and functional status at 1-year follow-up (see Table 4).
Given the significant associations between substance use severity at 1-year follow-up and the severity of several specific BPD symptoms (i.e. “real or imagined abandonment”; “unstable relationships”; “impulsivity”; “mood dysregulation”; “chronic emptiness”; “dissociation”), we implemented a multiple linear regression model to assess the unique contribution of each symptom in predicting severity of substance use at 1-year follow-up. The overall model explained a significant proportion of the variance (F (6, 17) = 5.51, p = 0.002, adjusted R-squared = 0.54), but the only BPD symptom that significantly predicted substance use severity was “dissociation” (B = 1.19, p = 0.010), with more severe dissociative symptoms predicting greater substance use severity at 1-year follow-up (see Table 5).
Discussion
We assessed rates of treatment response in a community-based residential programme specifically for adolescents and young people with substance use disorder (SUD), based on clinical severity of global psychiatric symptoms using the Brief Symptom Inventory Global Severity Index at 1-year follow-up. Concomitants of treatment response were assessed, including pre-treatment sociodemographics, substance use characteristics and severity, psychiatric symptom severity, borderline personality disorder (BPD), cognitive functioning, self-efficacy, and functional status, as well as treatment duration. We conducted exploratory analyses to investigate the influence of identified concomitants of treatment response, including effects on outcomes at 1-year follow-up.
Our classification indicated that approximately two thirds of participants were identified as nonresponders, with about one third showing a favourable response to treatment. Regarding concomitants of treatment response, we found that three of the assessed variables distinguished responders from nonresponders at treatment entry, with each showing a large effect: Nonresponders showed lower levels of self-efficacy (d = 1.04), poorer functional status (d = 1.09), and higher BPD symptom count (d = 1.26).
BPD symptom count showed the strongest effect in distinguishing responders from nonresponders, and thus, we conducted further exploratory analyses to investigate the impact of BPD on treatment response and outcomes. Over half of the sample screened positively for a potential diagnosis of BPD. Compared to their peers who screened negatively, those who screened positively for BPD were significantly younger and presented with more severe global psychiatric symptoms, poorer functional status, lower self-efficacy, higher substance use severity, and better cognitive functioning. To elucidate the unique impact of diverse BPD symptoms on treatment response, we assessed individual BPD symptom severity and found that nonresponders showed higher severity of two symptoms at treatment entry: “unstable relationships” and “paranoid ideation”. In addition, substance use severity at 1-year follow-up was associated with higher pre-treatment severity of six BPD symptom domains (i.e. “real or imagined abandonment”; “unstable relationships”; “impulsivity”; “mood dysregulation”; “chronic emptiness”; “dissociation”). No associations were found between specific BPD symptom severity and other assessed outcomes at 1-year follow-up (i.e. self-efficacy and functional status). In our model predicting outcome at 1-year follow-up using severity of the six identified BPD symptoms as predictors, only higher severity ratings of the “dissociation” BPD symptom at treatment entry was associated with substance use severity at 1-year follow-up.
The observed rate of nonresponse in the current study is high and in accordance with reported rates of adverse treatment outcomes in adult SUD treatment, including dropout (Lappan et al., 2020). The current study makes a significant contribution to the literature by providing an important estimate of treatment response in residential SUD programmes that are specifically designed for adolescents and young people.
We observed high rates of likely BPD in the adolescents and young people in the current study. BPD symptom count was significantly elevated for nonresponders (M = 8.0), and we would highlight that symptom count for responders was also observed to be relatively high (M = 5.7). This is particularly relevant in light of the less conservative clinical cut-off scores for the McLean Screening Instrument for Borderline Personality Disorder recommended in some contexts (Zimmerman & Balling, 2021), including a clinical cut-off of 5.5 for adolescents aged 12–17 in inpatient psychiatric treatment (Noblin et al., 2014). Our findings align with the high cooccurrence of SUD and BPD in adults that is well documented in the literature: Depending on index samples, approximately half of those with BPD meet criteria for at least one current SUD, and one quarter of those with SUD also meet criteria for BPD (Trull et al., 2018). In some cases, the prevalence of comorbid SUD may even be up to 84% for those with BPD (Shah & Zanarini, 2018). We provide an important estimate of rates of comorbid BPD in adolescents and young people with SUD.
We found an interesting pattern of treatment response-related associations with specific BPD symptom severity. Greater severity of “unstable relationships” and “paranoid ideation” symptoms was associated with treatment nonresponse at 1-year follow-up. More severe substance use at 1-year follow-up was associated with greater severity of six BPD symptoms (i.e. “real or imagined abandonment”; “unstable relationships”; “impulsivity”; “mood dysregulation”; “chronic emptiness”; “dissociation”), and more severe “dissociation” was a unique predictor of substance use severity at 1-year follow-up. Interestingly, criteria 9 of the BPD diagnostic criteria includes consideration of both paranoid, psychotic-like experiences and severe dissociative experiences (i.e. feelings of unreality). We found both aspects of criteria 9 to influence findings: “paranoid ideation” related to likelihood of being a nonresponder and “dissociation” related to higher severity of substance use. Recognition and greater understanding of this complex symptom could assist in helping young people most at risk of poor treatment outcomes in residential SUD treatment settings. In addition, a number of implicated symptoms are ostensibly related to interpersonal dysfunction: “Unstable relationships” was associated with both treatment nonresponse and higher substance use severity, along with an association between more severe “real or imagined abandonment” and higher substance use severity. On the other hand, associations between more severe “chronic emptiness” and “dissociation” symptoms and severity of substance use also represent complex symptom constellations worthy of further comment.
We speculate that this complex pattern of symptoms, including those that relate to interpersonal dysfunction, are highly relevant to the residential treatment context under consideration. Given the intensive and multifaceted social context of this form of residential SUD treatment (Marceau et al., 2021b), we propose that difficulties in interpersonal functioning, associated with problems in mentalisation (i.e. understanding the self and others in terms of mental states: Luyten et al., 2020), may present specific challenges that interfere with key relational treatment processes for adolescents and young people in this setting. Along with interpersonal dysfunction, the complex and poorly understood symptoms of “chronic emptiness” (Miller et al., 2020) and “dissociation” (Krause-Utz, 2022) were implicated. Dissociation in the context of BPD may often (but not always) be trauma-related, yet the complex nature of these symptoms and impacts on treatment outcomes are yet to be fully realised.
It has been proposed that high rates of comorbidity and overlapping symptoms in BPD and SUD may relate to shared transdiagnostic phenotypes related to impulsivity and externalising behaviours, proposed to stem from core deficits in executive functioning (Koudys & Ruocco, 2019). Our findings are in contrast given this pattern of BPD symptoms associated with treatment response and outcomes in this setting. We also found associations between higher “impulsivity” and “mood dysregulation” and severity of substance use, which shows more alignment with the expected pattern of results under this hypothesis.
In a study of young people aged 15–25 with BPD, BPD severity was associated with alcohol dependence and monthly or more frequent amphetamine and polysubstance use (Scalzo et al., 2017). While these findings suggest a possible pathway in which BPD may precede the development of SUD, multiple aetiological pathways are proposed ranging from common factors, secondary substance use or mental illness, and bidirectional models in the literature on cooccurring disorders more broadly (Mueser & Drake, 2007). In the aetiology of SUD, there is an increasing recognition of the key role that negative affective states play in the cyclical nature of addiction (Koob et al., 2020), which may overlap with emotion dysregulation and impulsivity in BPD (Trull et al., 2018), and the transition to compulsive use of substances to relieve increasing negative affect associated with withdrawal or stressful states (Zorrilla & Koob, 2019). From our pattern of results, we speculate that interpersonal dysfunction may also play an important role in the comorbidity of SUD and BPD. Marked impairments in social processing have been identified for both BPD and SUD, representing a further plausible transdiagnostic phenotype (Hanegraaf et al., 2021). This may relate to core deficits in interpersonal and self-functioning emphasised in the recent shift to dimensional models of personality disorder (Bach et al., 2022; Skodol et al., 2011). In fact, studies have begun to link these core deficits to the social processing domain outlined in the National Institute of Mental Health’s (NIMH) Research Domain Criteria (RDoC), to better understand neurobiological mechanisms in BPD (Hanegraaf et al., 2023).
In our study, we observed an interesting finding in that participants screening positive for comorbid BPD in addition to SUD showed better cognitive functioning. BPD (Koudys et al., 2018) and SUD (Fernández-Serrano et al., 2011) are associated with unique yet overlapping profiles of neurocognitive deficits, but the effects on cognition may not necessarily be cumulative. For example, in an investigation of the impact of comorbid personality disorder on cognitive functioning in a sample of female adults with SUD, participants who screened positive for comorbid personality disorder had greater self-reported dysfunction but better performance on most assessed cognitive domains compared to participants without comorbid personality disorder (Marceau et al., 2021a).
Implications for treatment indicate that comorbid SUD is associated with difficulty in achieving remission from BPD over time (Zanarini et al., 2004), while in SUD, comorbid personality disorder is a well-known risk factor for dropout from SUD treatment (Brorson et al., 2013). Given the complexity of treating cooccurring SUD and BPD, treatment approaches that are integrated and coordinated are recommended (Donald et al., 2019; Lubman et al., 2011), though there are few published studies supporting the evidence base in this area (Hall et al., 2018; Lee et al., 2015; Pennay et al., 2011). Moreover, this is particularly true for adolescents and young people with comorbid SUD and BPD.
In light of the challenge of treating comorbid SUD and BPD, screening for personality disorder is recommended in SUD treatment settings for adults (McMain & Ellery, 2008). Similarly, the use of a brief screening measure that could be administered by frontline clinicians to identify comorbid BPD in adolescents and young people may be a warranted first clinical step in identifying clients in SUD treatment who are potentially at risk of poorer treatment outcomes (Christie et al., 2020).
Many pre-treatment variables did not distinguish responders and nonresponders in our study. These included sociodemographics, substance use characteristics and severity, severity of psychiatric symptoms, and cognitive functioning. Treatment duration did not differ for responders and nonresponders. On the other hand, there was a trend toward more severe depression symptoms for nonresponders at intake. This aligns with the previous reports showing that comorbid depression may have a negative impact on treatment outcomes for adolescents with SUD, though findings are mixed (Hersh et al., 2014).
Alongside a more nuanced understanding of the mechanisms through which comorbid disorders such as BPD present and impact on SUD outcomes, improving treatment outcomes for adolescents and young people may necessitate a better understanding of treatment mechanisms (Witkiewitz et al., 2022). Some mediators of adolescent-specific SUD treatments have been identified (Black & Chung, 2014; Meisel et al., 2022), with the strongest support found for processes related to self-regulation and treatment engagement and adherence (Meisel et al., 2022). Moderators of SUD treatment outcomes for adolescents have also been identified, ranging from participant demographics and individual differences, psychiatric symptom severity and comorbid psychiatric disorders, and parent involvement (Bachrach & Chung, 2021). In parallel with the literature on mediators of SUD treatments, the small number and heterogeneity of studies highlight several gaps in knowledge of variables and processes influencing treatment outcomes for young people with SUD.
There are several limitations of the current study we must acknowledge. Firstly, we use a specific definition of treatment response based on clinical significance of global psychiatric symptoms at 1-year follow-up. While there are multiple ways to define treatment response (e.g. retention, dropout, relapse, changes in other relevant outcome measures), our definition was based on the reported primary outcome in our previous cohort study (Marceau et al., 2021b). Related to this, we acknowledge the need for future studies to adopt broader definitions of treatment success that also emphasise consumer-driven recovery-based outcomes (Alves et al., 2017). Second, our sample size used in characterising treatment response was small. However, through maximising available 1-year follow-up data, we were able to investigate potentially durable effects of treatment. In our previous study, we reported a 51% attrition rate at 1-year follow-up, which reflected completed assessments for the group of participants with interviews due during the funding period. This attrition rate is high but also representative of the challenges in completing longitudinal follow-up assessments in SUD populations (Hansten et al., 2000). Though our previous analysis showed minimal differences in baseline characteristics of participants who were lost to 1-year follow-up versus those who completed it (Marceau et al., 2021b), the findings reported here must be interpreted with caution due to unknown attrition bias. Third, we rely on the use of a BPD screening measure to confirm diagnosis, rather than the inclusion of dedicated diagnostic interviews. In saying this, our method of rating the severity of specific BPD symptoms has been used in previous reports and provides a useful dimensional measure of symptom severity (Miller et al., 2018; Woodbridge et al., 2021). Future studies with larger samples of adolescents and young people, diverse and broader measures of treatment outcome and recovery, and diagnostic interviews to confirm psychiatric comorbidities may lead to further knowledge of factors associated with treatment response in this population. Moreover, there are a wide range of potential factors influencing treatment response that could be fruitfully explored. The current study explored specific pre-treatment characteristics, but investigating factors that also dynamically change over the course of treatment may be useful. Assessing factors not only at the micro-level of the individual (e.g. their engagement and alliance in treatment, family/carer factors) but also at the macro-level of broader contextual determinants may be useful in future studies of treatment response in adolescents and young people with SUD.
In conclusion, community-based residential SUD programmes are important for adolescents and young adults who require more intensive treatments (Marceau et al., 2021b). We report a high rate of treatment nonresponse, with only one third of participants classified as treatment responders at 1-year follow-up. In exploring correlates of treatment response, nonresponders had higher BPD symptom count at treatment entry, poorer functional status, and lower self-efficacy. Pre-treatment sociodemographics, substance use characteristics and severity, psychiatric symptom severity, and cognitive functioning, as well as treatment duration, did not differ as a function of treatment response. Our findings show high rates of comorbid BPD in residential SUD treatment settings for adolescents and young adults, with over half of the current sample meeting screening criteria for BPD. A pattern of BPD symptoms relating to more severe interpersonal dysfunction, chronic emptiness, dissociation, and paranoid ideation was particularly relevant to treatment nonresponse and substance use severity at 1-year follow-up.
Data Availability
The datasets generated and/or analysed during the current study are not publicly available as participants did not give consent for release beyond the study. Please contact the corresponding author (EMM) for requests.
Code Availability
Not applicable.
References
Abdel-Salam, S., & Gunter, W. D. (2014). Therapeutic engagement as a predictor of retention in adolescent therapeutic community treatment. Journal of Child & Adolescent Substance Abuse, 23(1), 49–57. https://doi.org/10.1080/1067828X.2012.735556
AIHW. (2020). Alcohol, tobacco and other drugs in Australia. Web report. https://www.aihw.gov.au/reports/alcohol/alcohol-tobacco-other-drugs-australia/contents/priority-populations/younger-people
Alves, P., Sales, C., & Ashworth, M. (2017). Does outcome measurement of treatment for substance use disorder reflect the personal concerns of patients? A scoping review of measures recommended in Europe. Drug and Alcohol Dependence, 179, 299–308. https://doi.org/10.1016/j.drugalcdep.2017.05.049
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Andersson, H. W., Lauvsnes, A. D. F., & Nordfjærn, T. (2021). Emerging adults in inpatient substance use treatment: A prospective cohort study of patient characteristics and treatment outcomes. European Addiction Research, 27(3), 206–215. https://doi.org/10.1159/000512156
Bach, B., Kramer, U., Doering, S., di Giacomo, E., Hutsebaut, J., Kaera, A., & Renneberg, B. (2022). The ICD-11 classification of personality disorders: A European perspective on challenges and opportunities. Borderline Personality Disorder and Emotion Dysregulation, 9(1), 12–12. https://doi.org/10.1186/s40479-022-00182-0
Bachrach, R. L., & Chung, T. (2021). Moderators of substance use disorder treatment for adolescents. Journal of Clinical Child and Adolescent Psychology, 50(4), 498–509. https://doi.org/10.1080/15374416.2020.1790379
Black, J. J., & Chung, T. (2014). Mechanisms of change in adolescent substance use treatment: How does treatment work? Substance Abuse, 35(4), 344–351. https://doi.org/10.1080/08897077.2014.925029
Breslin, F. C., Sobell, L. C., Sobell, M. B., & Agrawal, S. (2000). A comparison of a brief and long version of the situational confidence questionnaire. Behaviour Research and Therapy, 38(12), 1211–1220. https://doi.org/10.1016/S0005-7967(99)00152-7
Brorson, H. H., Ajo Arnevik, E., Rand-Hendriksen, K., & Duckert, F. (2013). Drop-out from addiction treatment: A systematic review of risk factors. Clinical Psychology Review, 33(8), 1010–1024. https://doi.org/10.1016/j.cpr.2013.07.007
Brunette, M., Mueser, K., & Drake, R. (2004). A review of research on residential programs for people with severe mental illness and co-occurring substance use disorders. Drug and Alcohol Review, 23(4), 471–481. https://doi.org/10.1080/09595230412331324590
Christie, G. I. G., Cheetham, A., & Lubman, D. I. (2020). Interventions for alcohol and drug use disorders in young people: 10 key evidence-based approaches to inform service delivery. Current Addiction Reports, 7(4), 464–474. https://doi.org/10.1007/s40429-020-00336-6
Cleary, M., Hunt, G. E., Matheson, S., & Walter, G. (2009). Psychosocial treatments for people with co-occurring severe mental illness and substance misuse: Systematic review. Journal of Advanced Nursing, 65(2), 238–258. https://doi.org/10.1111/j.1365-2648.2008.04879.x
Cohen, Z. D., & DeRubeis, R. J. (2018). Treatment selection in depression. Annual Review of Clinical Psychology, 14, 209–236. https://doi.org/10.1146/annurev-clinpsy-050817-084746
IBM Corp. (2022). IBM SPSS Statistics for Windows, Version 29.0.
Dacosta-Sánchez, D., González-Ponce, B. M., Fernández-Calderón, F., Sánchez-García, M., & Lozano, O. M. (2022). Retention in treatment and therapeutic adherence: How are these associated with therapeutic success? An analysis using real-world data. International Journal of Methods in Psychiatric Research, 31, e1929. https://doi.org/10.1002/mpr.1929
de Andrade, D., Elphinston, R. A., Quinn, C., Allan, J., & Hides, L. (2019). The effectiveness of residential treatment services for individuals with substance use disorders: A systematic review. Drug and Alcohol Dependence, 201, 227–235. https://doi.org/10.1016/j.drugalcdep.2019.03.031
Degenhardt, L. S. E., Patton, G., Hall, W. D., & Lynskey, M. (2016). The increasing global health priority of substance use in young people. Lancet Psychiatry, 3(3), 251–264. https://doi.org/10.1016/s2215-0366(15)00508-8
Derogatis LR. (1993). BSI Brief Symptom Inventory: Administration, Scoring, and Procedural Manual (4th ed.). National Computer Systems.
Donald, F., Arunogiri, S., & Lubman, D. I. (2019). Substance use and borderline personality disorder: Fostering hope in the face of complexity. Australasian Psychiatry: Bulletin of the Royal Australian and New Zealand College of Psychiatrists, 27(6), 569–572. https://doi.org/10.1177/1039856219875061
Drake, R. E., O’Neal, E. L., & Wallach, M. A. (2008). A systematic review of psychosocial research on psychosocial interventions for people with co-occurring severe mental and substance use disorders. Journal of Substance Abuse Treatment, 34(1), 123–138. https://doi.org/10.1016/j.jsat.2007.01.011
Edelen, M. O., Slaughter, M. E., McCaffrey, D. F., Becker, K., & Morral, A. R. (2009). Long-term effect of community-based treatment: Evidence from the adolescent outcomes project. Drug and Alcohol Dependence, 107(1), 62–68. https://doi.org/10.1016/j.drugalcdep.2009.09.008
Fadus, M. C., Squeglia, L. M., Valadez, E. A., Tomko, R. L., Bryant, B. E., & Gray, K. M. (2019). Adolescent substance use disorder treatment: An update on evidence-based strategies. Current Psychiatry Reports, 21(10), 96. https://doi.org/10.1007/s11920-019-1086-0
Fernández-Serrano, M. J., Pérez-García, M., & Verdejo-García, A. (2011). What are the specific\ vs. generalized effects of drugs of abuse on neuropsychological performance. Neuroscience and Biobehavioral Reviews, 35(3), 377-406. https://doi.org/10.1016/j.neubiorev.2010.04.008
Gossop, M., Darke, S., Griffiths, P., Hando, J., Powis, B., Hall, W., & Strang, J. (1995). The Severity of Dependence Scale (SDS): Psychometric properties of the SDS in English and Australian samples of heroin, cocaine and amphetamine users. Addiction, 90(5), 607–614. https://doi.org/10.1046/j.1360-0443.1995.9056072.x
Gray, K. M., & Squeglia, L. M. (2018). Research review: What have we learned about adolescent substance use? The Journal of Child Psychology and Psychiatry, 59(6), 618–627. https://doi.org/10.1111/jcpp.12783
Hall, K., Simpson, A., O’Donnell, R., Sloan, E., Staiger, P. K., Morton, J., & Lubman, D. I. (2018). Emotional dysregulation as a target in the treatment of co-existing substance use and borderline personality disorders: A pilot study. Clinical Psychologist, 22(2), 112–125. https://doi.org/10.1111/cp.12162
Hanegraaf, L., van Baal, S., Hohwy, J., & Verdejo-Garcia, A. (2021). A systematic review and meta-analysis of ‘Systems for Social Processes’ in borderline personality and substance use disorders. Neuroscience and Biobehavioral Reviews, 127, 572–592. https://doi.org/10.1016/j.neubiorev.2021.04.013
Hanegraaf, L., Paton, B., Hohwy, J., & Verdejo-Garcia, A. (2023). Combining novel trait and neurocognitive frameworks to parse heterogeneity in borderline personality disorder. Journal of Personality. https://doi.org/10.1111/jopy.12811
Hansten, M. L., Downey, L., Rosengren, D. B., & Donovan, D. M. (2000). Relationship between follow-up rates and treatment outcomes in substance abuse research: More is better but when is “enough” enough? Addiction, 95(9), 1403–1416. https://doi.org/10.1046/j.1360-0443.2000.959140310.x
Hersh, J., Curry, J. F., & Kaminer, Y. (2014). What is the impact of comorbid depression on adolescent substance abuse treatment? Substance Abuse, 35(4), 364–375. https://doi.org/10.1080/08897077.2014.956164
Hogue, A., Henderson, C. E., Ozechowski, T. J., & Robbins, M. S. (2014). Evidence base on outpatient behavioral treatments for adolescent substance use: Updates and recommendations 2007–2013. Journal of Clinical Child and Adolescent Psychology, 43(5), 695–720. https://doi.org/10.1080/15374416.2014.915550
Hogue, A., Henderson, C. E., Becker, S. J., & Knight, D. K. (2018). Evidence base on outpatient behavioral treatments for adolescent substance use, 2014–2017: Outcomes, treatment delivery, and promising horizons. Journal of Clinical Child and Adolescent Psychology, 47(4), 499–526. https://doi.org/10.1080/15374416.2018.1466307
Kelly, J. F., Urbanoski, K. A., Hoeppner, B. B., & Slaymaker, V. (2011). “Ready, willing, and (not) able” to change: Young adults’ response to residential treatment. Drug and Alcohol Dependence, 121(3), 224–230. https://doi.org/10.1016/j.drugalcdep.2011.09.003
Koob, G. F., Powell, P., & White, A. (2020). Addiction as a coping response: Hyperkatifeia, deaths of despair, and COVID-19. The American Journal of Psychiatry, 177(11), 1031–1037. https://doi.org/10.1176/appi.ajp.2020.20091375
Koudys, J. W., Gulamani, T., & Ruocco, A. C. (2018). Borderline personality disorder: Refinements in phenotypic and cognitive profiling. Current Behavioral Neuroscience Reports, 5(1), 102–112. https://doi.org/10.1007/s40473-018-0145-x
Koudys, J. W., & Ruocco, A. C. (2019).A neurocognitive model of the comorbidity of substance use and personality disorders. In A. V. García (Ed.), Cognition and Addiction. Elsevier Science & Technology. https://doi.org/10.1016/B978-0-12-815298-0.00006-X
Krause-Utz, A. (2022). Dissociation, trauma, and borderline personality disorder. Borderline Personality Disorder and Emotion Dysregulation, 9(1), 14–14. https://doi.org/10.1186/s40479-022-00184-y
Lambert, M. J. (2013). Bergin and Garfield’s handbook of psychotherapy and behavior change (6th ed.). John Wiley & Sons.
Lappan, S. N., Brown, A. W., & Hendricks, P. S. (2020). Dropout rates of in-person psychosocial substance use disorder treatments: A systematic review and meta-analysis. Addiction, 115(2), 201–217. https://doi.org/10.1111/add.14793
Lee, N. K., Cameron, J., & Jenner, L. (2015). A systematic review of interventions for co-occurring substance use and borderline personality disorders. Drug and Alcohol Review, 34(6), 663–672. https://doi.org/10.1111/dar.12267
Little, R. J. A. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83(404), 1198–1202. https://doi.org/10.1080/01621459.1988.10478722
Lubman, D. I., Hall, K., Pennay, A., & Rao, S. (2011). Managing borderline personality disorder and substance use: An integrated approach. Australian Family Physician, 40(6), 376–381.
Luciana, M., & Feldstein Ewing, S. W. (2015). Introduction to the special issue: Substance use and the adolescent brain: Developmental impacts, interventions, and longitudinal outcomes. Developmental Cognitive Neuroscience, 16, 1–4. https://doi.org/10.1016/j.dcn.2015.10.005
Luyten, P., Campbell, C., Allison, E., & Fonagy, P. (2020). The mentalizing approach to psychopathology: State of the art and future directions. Annual Review of Clinical Psychology, 16(1), 297–325. https://doi.org/10.1146/annurev-clinpsy-071919-015355
Malivert, M., Fatséas, M., Denis, C., Langlois, E., & Auriacombe, M. (2012). Effectiveness of therapeutic communities: A systematic review. European Addiction Research, 18(1), 1–11. https://doi.org/10.1159/000331007
Marceau, E. M., Lunn, J., Berry, J., Kelly, P. J., & Solowij, N. (2016). The Montreal Cognitive Assessment (MoCA) is sensitive to head injury and cognitive impairment in a residential alcohol and other drug therapeutic community. Journal of Substance Abuse Treatment, 66, 30–36. https://doi.org/10.1016/j.jsat.2016.03.002
Marceau, E. M., Berry, J., & Grenyer, B. F. S. (2021a). Neurocognition of females with substance use disorder and comorbid personality disorder: Divergence in subjective and objective cognition. Applied Neuropsychology: Adult, 30(3), 368–378. https://doi.org/10.1080/23279095.2021.1948413
Marceau, E. M., Holmes, G., Cutts, J., Mullaney, L., Meuldijk, D., Townsend, M. L., & Grenyer, B. F. S. (2021b). Now and then: A ten-year comparison of young people in residential substance use disorder treatment receiving group dialectical behaviour therapy. BMC Psychiatry, 21(1), 362. https://doi.org/10.1186/s12888-021-03372-2
McCabe, S. E., Schulenberg, J. E., Schepis, T. S., McCabe, V. V., & Veliz, P. T. (2022). Longitudinal analysis of substance use disorder symptom severity at age 18 years and substance use disorder in adulthood. JAMA Network Open, 5(4), e225324. https://doi.org/10.1001/jamanetworkopen.2022.5324
McMain, S., & Ellery, M. (2008). Screening and assessment of personality disorders in addiction treatment settings. International Journal of Mental Health and Addiction, 6(1), 20–31. https://doi.org/10.1007/s11469-007-9093-5
Meisel, S. N., Pielech, M., Magill, M., Sawyer, K., & Miranda, R. (2022). Mechanisms of behavior change in adolescent substance use treatment: A systematic review of treatment mediators and recommendations for advancing future research. Clinical Psychology: Science and Practice. https://doi.org/10.1037/cps0000089
Miller, C. E., Lewis, K. L., Huxley, E., Townsend, M. L., & Grenyer, B. F. S. (2018). A 1-year follow-up study of capacity to love and work: What components of borderline personality disorder most impair interpersonal and vocational functioning? Personality and Mental Health, 12(4), 334–344. https://doi.org/10.1002/pmh.1432
Miller, C. E., Townsend, M. L., Day, N. J. S., & Grenyer, B. F. S. (2020). Measuring the shadows: A systematic review of chronic emptiness in borderline personality disorder. PloS One, 15(7), e0233970. https://doi.org/10.1371/journal.pone.0233970
Mueser, K. T., & Drake, R. E. (2007). Comorbidity: What have we learned and where are we going? Clinical Psychology: Science and Practice, 14(1), 64–69. https://doi.org/10.1111/j.1468-2850.2007.00063.x
Nasreddine, Z. S., Phillips, N. A., Bedirian, V., Charbonneau, S., Whitehead, V., Collin, I., & Chertkow, H. (2005). The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. Journal of American Geriatrics Society, 53, 695–699. https://doi.org/10.1111/jgs.15925
Neumann, A., Ojong, T. N., Yanes, P. K., Tumiel-Berhalter, L., Daigler, G. E., & Blondell, R. D. (2010). Differences between adolescents who complete and fail to complete residential substance abuse treatment. Journal of Addictive Diseases, 29(4), 427–435. https://doi.org/10.1080/10550887.2010.509276
Noblin, J. L., Venta, A., & Sharp, C. (2014). The validity of the MSI-BPD among inpatient adolescents. Assessment, 21(2), 210–217. https://doi.org/10.1177/1073191112473177
Pennay, A., Cameron, J., Reichert, T., Strickland, H., Lee, N. K., Hall, K., & Lubman, D. I. (2011). A systematic review of interventions for co-occurring substance use disorder and borderline personality disorder. Journal of Substance Abuse Treatment, 41(4), 363–373. https://doi.org/10.1016/j.jsat.2011.05.004
Reif, S., George, P., Braude, L., Dougherty, R. H., Daniels, A. S., Ghose, S. S., & Delphin-Rittmon, M. E. (2014). Residential treatment for individuals with substance use disorders: Assessing the evidence. Psychiatric Services, 65(3), 301–312. https://doi.org/10.1176/appi.ps.201300242
Scalzo, F., Hulbert, C. A., Betts, J. K., Cotton, S. M., & Chanen, A. M. (2017). Substance use in youth with borderline personality disorder. Journal of Personality Disorders, 1-16. https://doi.org/10.1521/pedi_2017_31_330
Shah, R., & Zanarini, M. C. (2018). Comorbidity of borderline personality disorder: Current status and future directions. Psychiatric Clinics of North America, 41(4), 583–593. https://doi.org/10.1016/j.psc.2018.07.009
Skodol, A. E., Clark, L. A., Bender, D. S., Krueger, R. F., Morey, L. C., Verheul, R., & Oldham, J. M. (2011). Proposed changes in personality and personality disorder assessment and diagnosis for DSM-5 Part I: Description and rationale. Personality Disorders, 2(1), 4–22. https://doi.org/10.1037/a0021891
Smith LA, Gates S, Foxcroft D. (2006). Therapeutic communities for substance related disorder. Cochrane Database of Systematic Reviews, CD005338. https://doi.org/10.1002/14651858.CD005338.pub2
Snowdon, N., Allan, J., Shakeshaft, A., Rickwood, D., Stockings, E., Boland, V. C., & Courtney, R. J. (2019). Outpatient psychosocial substance use treatments for young people: An overview of reviews. Drug and Alcohol Dependence, 205, 107582. https://doi.org/10.1016/j.drugalcdep.2019.107582
Squeglia, L. M. (2020). Alcohol and the developing adolescent brain. World Psychiatry, 19(3), 393–394. https://doi.org/10.1002/wps.20786
Stockings, E., Hall, W. D., Lynskey, M., Morley, K. I., Reavley, N., Strang, J., & Degenhardt, L. (2016). Prevention, early intervention, harm reduction, and treatment of substance use in young people. The Lancet Psychiatry, 3(3), 280–296. https://doi.org/10.1016/S2215-0366(16)00002-X
The WHOQOL Group. (1998). Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychological Medicine, 28, 551–558.
Tripodi, S. J. (2009). A comprehensive review: Methodological rigor of studies on residential treatment centers for substance-abusing adolescents. Journal of Evidence-Based Social Work, 6(3), 288–299. https://doi.org/10.1080/15433710802687037
Trull, T. J., Freeman, L. K., Vebares, T. J., Choate, A. M., Helle, A. C., & Wycoff, A. M. (2018). Borderline personality disorder and substance use disorders: An updated review. Borderline Personality Disorder and Emotion Dysregulation, 5(1), 15–15. https://doi.org/10.1186/s40479-018-0093-9
Turner, B., & Deane, F. P. (2016). Length of stay as a predictor of reliable change in psychological recovery and well being following residential substance abuse treatment. Therapeutic Communities, 37(3), 112–120. https://doi.org/10.1108/TC-09-2015-0022
Uliaszek, A. A., Al-Dajani, N., & Mills, L. (2019a). Predictors of attrition from residential treatment for youths with addictive behaviors. Journal of Child & Adolescent Substance Abuse, 28(1), 1–7. https://doi.org/10.1080/1067828X.2018.1561574
Uliaszek, A. A., Hamdullahpur, K., & Mills, L. (2019b). Examining the effectiveness of residential treatment among adolescents with problem substance use. Journal of Child & Adolescent Substance Abuse, 28(4), 221–228. https://doi.org/10.1080/1067828X.2019.1682736
Urbanoski, K. A., Kelly, J. F., Hoeppner, B. B., & Slaymaker, V. (2012). The role of therapeutic alliance in substance use disorder treatment for young adults. Journal of Substance Abuse Treatment, 43(3), 344–351. https://doi.org/10.1016/j.jsat.2011.12.013
Vanderplasschen, W., Colpaert, K., Autrique, M., Rapp, R. C., Pearce, S., Broekaert, E., & Vandevelde, S. (2012). Therapeutic communities for addictions: A review of their efectiveness from a recovery-oriented perspective. The Scientific World Journal, 2013, 427817. https://doi.org/10.1155/2013/427817
Volkow, N. D., Han, B., Einstein, E. B., & Compton, W. M. (2021). Prevalence of substance use disorders by time since first substance use among young people in the US. JAMA Pediatrics, 175(6), 640–643. https://doi.org/10.1001/jamapediatrics.2020.6981
Waldron, H. B., & Turner, C. W. (2008). Evidence-based psychosocial treatments for adolescent substance abuse. Journal of Clinical Child and Adolescent Psychology, 37(1), 238–261. https://doi.org/10.1080/15374410701820133
Witkiewitz, K., Pfund, R. A., & Tucker, J. A. (2022). Mechanisms of behavior change in substance use disorder with and without formal treatment. Annual Review of Clinical Psychology, 18(1), 497–525. https://doi.org/10.1146/annurev-clinpsy-072720-014802
Woodbridge, J., Reis, S., Townsend, M. L., Hobby, L., & Grenyer, B. F. S. (2021). Searching in the dark: Shining a light on some predictors of non-response to psychotherapy for borderline personality disorder. PloS One, 16(7), e0255055. https://doi.org/10.1371/journal.pone.0255055
Zanarini, M. C., Vujanovic, A. A., Parachini, E. A., Boulanger, J. L., Frankenburg, F. R., & Hennen, J. (2003). A screening measure for BPD: The McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD). Journal of Personality Disorders, 17(6), 568–573. https://doi.org/10.1521/pedi.17.6.568.25355
Zanarini, M. C., Frankenburg, F. R., Hennen, J., Reich, D. B., & Silk, K. R. (2004). Axis I comorbidity in patients with borderline personality disorder: 6-year follow-up and prediction of time to remission. The American Journal of Psychiatry, 161(11), 2108–2114. https://doi.org/10.1176/appi.ajp.161.11.2108
Zimmerman, M., & Balling, C. (2021). Screening for borderline personality disorder with the McLean Screening Instrument: A review and critique of the literature. Journal of Personality Disorders, 35(2), 288–298. https://doi.org/10.1521/pedi_2019_33_451
Zorrilla, E. P., & Koob, G. F. (2019). Impulsivity derived from the dark side: Neurocircuits that contribute to negative urgency. Frontiers in Behavioral Neuroscience, 13, 136. https://doi.org/10.3389/fnbeh.2019.00136
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions This work was supported by a NSW Health AOD Early Intervention Innovation Fund Non-Government Organisation Evaluation Grant. Project Air Strategy acknowledges the support from the NSW Ministry of Health.
Author information
Authors and Affiliations
Contributions
All authors contributed to the design of the study. LM contributed to the delivery of the intervention. EMM performed data analysis and wrote the first draft of the manuscript. All authors commented on the previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Approval was granted by the University of Wollongong Health and Medical Human Research Ethics Committee (reference 2017/233) and the Aboriginal Health and Medical Research Council (AH&MRC; reference 1319/17). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). Informed consent was obtained from all patients for being included in the study. During recruitment, adult participants (i.e. those aged 18 years and older) provided written informed consent following a full explanation of study procedures (n.b., for participants under 18 years of age, legal guardians provided consent, while these participants provided assent to participate in the study).
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Marceau, E.M., Holmes, G., Mullaney, L. et al. Factors Associated with Treatment Response at 1-Year Follow-Up from a Residential Substance Use Disorder Programme for Young People Aged 16–24 Years. Int J Ment Health Addiction (2023). https://doi.org/10.1007/s11469-023-01152-5
Accepted:
Published:
DOI: https://doi.org/10.1007/s11469-023-01152-5