
Abstract
Background
Epidermal growth factor receptor (EGFR) mutations (EGFRm) represent one of the most common genomic alterations identified among patients with non-small cell lung cancer (NSCLC). Several targeted agents for patients with EGFRm have been proven safe and effective, including the third-generation tyrosine kinase inhibitor (TKI) osimertinib. Nonetheless, some patients will present with or develop EGFR-TKI resistance mechanisms.
Objective
We characterized the genomic landscape of primary resistance to osimertinib among Hispanic patients with EGFR-mutant NSCLC.
Methods
An observational longitudinal cohort study was conducted with two groups of patients, those with intrinsic resistance (cohort A) and those with long-term survival (cohort B). All patients were treated and followed between January 2018 and May 2022. All patients were assessed for Programmed Cell Death Ligand 1 (PD-L1) expression and Bcl-2-like protein 11 (BIM)/AXL mRNA expression before starting TKI. After 8 weeks of treatment, a liquid biopsy was performed to determine the presence of circulating free DNA (cfDNA), and next-generation sequencing (NGS) was used to identify mutations at the time of progression. In both cohorts, overall response rate (ORR), progression-free survival (PFS), and overall survival (OS) were evaluated.
Results
We found a homogeneous distribution of EGFR-sensitizing mutations in both cohorts. For cohort A, exon 21 mutations were more common than exon 19 deletions (ex19dels) for cohort B (P = 0.0001). The reported ORR for osimertinib was 6.3% and 100% for cohorts A and B, respectively (P = 0.0001). PFS was significantly higher in cohort B (27.4 months vs. 3.1 months; P = 0.0001) and ex19del patients versus L858R (24.5 months, 95% confidence interval [CI] 18.2–NR), vs. 7.6 months, 95% CI 4.8–21.1; P = 0.001). OS was considerably lower for cohort A (20.1 months vs. 36.0 months; P = 0.0001) and was better for patients with ex19del, no brain metastasis, and low tumor mutation burden. At the time of progression, more mutations were found in cohort A, identifying off-target alterations more frequently, including TP53, RAS, and RB1.
Conclusion
EGFR-independent alterations are common among patients with primary resistance to osimertinib and significantly impact PFS and OS. Our results suggest that among Hispanic patients, other variables associated with intrinsic resistance include the number of commutations, high levels AXL mRNA, and low levels of BIM mRNA, T790M de novo, EGFR p.L858R presence, and a high tumoral mutational burden.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The prognosis of patients with EGFR mutations and primary resistance to osimertinib is utterly opposed to those with a high sensitivity to osimertinib. |
Patients with EGFR mutations with complex genotypes, including alterations in TP53 and RB1, and a high tumor mutation burden, require a different therapeutic approach to osimertinib as the first-line intervention. |
Early assessment of EGFR circulating free DNA (cfDNA) allows prediction of the disease course in patients with primary resistance to osimertinib. This information could allow the use of risk-adaptive therapeutic models. |
AXL mRNA expression levels are considerably higher among patients with EGFR mutations and primary resistance to osimertinib. In contrast, Bcl-2 interacting mediator of cell death (BIM) mRNA expression levels were significantly lower in cohort A. |
1 Introduction
Alterations in the epidermal growth factor receptor (EGFR) gene are among the most common oncogenic driver mutations in the pathogenesis of non-small cell lung cancer (NSCLC). Specific mutations in the EGFR gene are associated with increased sensitivity to EGFR tyrosine kinase inhibitors (EGFR-TKI), which offer the best possible results for treatment response in patients with an NSCLC diagnosis and EGFR mutations (EGFRm) [1, 2]. EGFRm presence has been reported in 10–50% of NSCLC cases, almost all in lung adenocarcinomas (LUADs). In addition, significant ethnic variations for EGFRm prevalence have been described, such as 8–15% in LUADs diagnosed in Caucasian patients versus 30–50% in East Asian populations [3, 4]. Among Hispanic populations in Latin America, the frequency of EGFRm in LUADs ranges from 14% in Argentina to 24–35% in Colombia and as high as 50% among Peruvian populations [5,6,7]. Evaluation of ancestry–mutation association showed that Native American ancestry is positively correlated with EGFRm [8, 9].
Among the EGFR-TKI-sensitizing mutations, exon 19 deletions (ex19dels) in the p.E746-A750 region and the point-substitution p.L858R (L858R) in exon 21 are the two most commonly described [10, 11]. These alterations represent ≈90% of EGFR-TKI-sensitizing mutations [12]. ex19dels and L858R are early clonal events that lead to tumor development in LUADs. They result in constitutive ligand-independent EGFR-tyrosine kinase activity and an increased affinity for first-generation (i.e., gefitinib, erlotinib, and icotinib), second-generation (i.e., afatinib and dacomitinib), and third-generation (i.e., osimertinib and aumolertinib) EGFR-TKI [13]. Nowadays, the National Comprehensive Cancer Network recommends osimertinib as the preferred EGFR-TKI option as first-line treatment for NSCLC because it inhibits both EGFR-TKI-sensitizing and the EGFR resistance mutation p.Thr790Met (T790M), and it has shown efficacy in patients with central nervous system (CNS) metastases [14].
The FLAURA trial (NCT02296125) recruited over 550 patients with ex19dels or L858R EGFR-mutated advanced NSCLC, from December 2014 to March 2016 [15]. In this study, the individuals were stratified according to EGFRm status and ethnicity (Asian/non-Asian), then half of the patients were treated with oral osimertinib and the other half were treated with other TKI [16,17,18]. After follow-up, the study demonstrated a better overall survival (OS) and a favorable OS rate in the group treated with osimertinib. Although the FLAURA trial and other studies have consistently shown the superior efficacy of osimertinib in comparison with first- and second-generation EGFR-TKI, some patients develop resistance mechanisms to third-generation TKI. These resistance mechanisms affect a patient's prognosis under TKI treatment. Most patients with advanced EGFRm NSCLC will achieve an objective response after treatment with TKI, but will eventually present disease progression. The extent and duration of responses are variable. However, approximately 10–15% of patients do not respond to treatment or have control of the disease for a short time, usually less than 3 months [19, 20].
Current evidence suggests two types of resistance mechanisms: EGFR dependent and EGFR independent. Some EGFR-dependent resistance mechanisms have been described for first-line and second-line treatment, including acquired EGFRm (C797S, L718/G719, G796/C797, L792, L798, and EGFR amplification). These profiles pose a significant challenge in selecting the most effective treatment based on resistance patterns after disease progression. Regarding the EGFR-independent mechanisms of acquired resistance, the activation of bypass pathways via amplifications (i.e., epithelial growth factor receptor or ERBB2/HER2, MET, fibroblast growth factor receptor 1 or FGFR1, and KRAS), fusions of alternative receptor tyrosine kinase (RTK) genes (i.e., RET, anaplastic lymphoma kinase [ALK], fibroblast growth factor receptor 3 [FGFR3], and neurotrophic receptor tyrosine kinase 1 [NTRK1]), as well as activating mutations and fusions of members of the downstream RAS-RAF-MEK-MAPK and PI3K/AKT/PTEN/mTOR pathways have been proposed as possible explanations [21]. Additional mechanisms of acquired resistance shared by TKI of all three generations include the phenotypic transformation to small-cell lung cancer (SCLC), epithelial-mesenchymal transition (EMT), the conversion to squamous cell carcinoma (SCC), activation of the Wnt/β-catenin pathway, hormonal signaling, and cell cycle were observed in some EGFR mutant cases compared to wild-type EGFR cases [22,23,24,25].
It has been proposed that acquired resistance could emerge from the expansion of original pre-treatment resistant clones and new resistance mechanisms developed as an adaptative response to TKI exposure. On the other hand, intrinsic resistance mechanisms are still a matter of debate and secondary activating pathways remain poorly understood [19, 20, 26]. Herein, we characterize the clinical, molecular, and genomic features associated with an intrinsic resistance pattern to osimertinib therapy in treatment-naïve patients with EGFRm NSCLC [24, 25].
2 Methods
2.1 Study Design and Patients
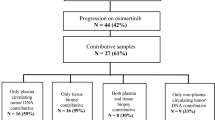
An observational longitudinal cohort study was conducted by the Latin American Consortium for Investigation of Lung Cancer (CLICaP) using the data deposited in a centralized database (CLICaP Real World Data/Evidence database). Patients included in the EGFRm NSCLC database were assessed from January 2018 to May 2022. All patients were residents of Bogota, DC, Colombia, and demographic variables such as age, sex, and smoking history were collected from the clinical record. Eligible patients were those with EGFRm analyzed by molecular diagnosis (N = 578) (Fig. 1). Among these patients, we defined cohort A as cases with intrinsic resistance to first-line osimertinib with measurable disease progression within the first 3 months of treatment (N = 16). In contrast, cohort B were patients with long-term responses to osimertinib treatment or progression-free survival (PFS) with osimertinib > 18 months. Finally, this control group was selected from a cohort of long survivors with genomic evaluation by next-generation sequencing (NGS) and complete clinical follow-up. Cases with similar clinical characteristics were sought without being able to match them, due to the unusual nature of patients with primary resistance.

The design and distribution of the study cohorts. We identified 578 potentially eligible patients. Cases with intrinsic resistance to first-line osimertinib (measurable disease progression within the first 3 months of treatment) were identified (cohort A). Control group patients were selected for convenience from a cohort of long survivors with genomic evaluation by NGS and complete clinical follow-up. Cases with similar clinical characteristics were sought without being able to match them due to the unusual nature of patients with primary resistance (cohort B). BIM Bcl-2 interacting mediator of cell death, ddPCR droplet digital polymerase chain reaction, EGFR epidermal growth factor receptor, EGFRm epidermal growth factor receptor mutation, NGS next-generation sequencing, NSCLC non-small cell lung cancer, PFS progression-free survival
At diagnosis, tumor tissue was acquired from all included patients to undergo molecular characterization, including PD-L1 expression by immunohistochemistry (IHC) and a standardized NGS test. A liquid biopsy was also obtained before starting osimertinib to evaluate Bcl-2 interacting mediator of cell death (BIM) polymorphisms. In the baseline tumor tissue, BIM and AXL mRNA expression levels were quantified using reverse transcription-polymerase chain reaction (RT-PCR). Cohort A and B patients received first-line osimertinib (80 mg orally once daily) until disease progression or unacceptable toxicity was documented. Patients were followed for 48 months and assessed for progression. After 8 weeks of treatment with osimertinib, a new liquid biopsy was performed to estimate the EGFRm status by droplet digital PCR (ddPCR). The NGS test in liquid biopsy was repeated when progression was found, and tissue collection was attempted when there was suspicion of histological transformation (SCLC). The study design and patient inclusion are summarized in Fig. 1.
2.2 Follow-Up and Clinical Outcomes
Patients included in the study were assessed clinically every month. Radiological follow-ups were completed every 9–12 weeks. Clinical, demographic, and molecular variables (including all mutations and tumor mutational burden [TMB]) were stored in a centralized and deidentified database at the CLICaP/Foundation for Clinical and Applied Cancer Research—FICMAC (Bogotá, Colombia). All included patients provided signed informed consent. In addition, an Institutional Review Board and Privacy Board waiver was obtained to facilitate retrospective clinical-pathological and molecular data (Lung Cancer-FICMAC/CLICaP Platform—Registration No. 2012/014, Kayre, Bogotá, Colombia, and Research Ethics Committee of Universidad El Bosque—Registration No. PCI-2018-10171).
Overall response rate (ORR) was defined as the sum of complete responses (CRs) and partial responses (PRs), as assessed by an independent, blinded radiologist according to the Response Evaluation Criteria in Solid Tumors (RECIST) V1.1. For PFS, time to event was calculated from the date of treatment start until radiographic disease progression as assessed by a blinded radiologist according to RECIST V1.1 or death by any cause. Observations for patients who did not experience progression were censored at the patient-specific last follow-up. OS was estimated from diagnosis until death by any cause or loss to follow-up.
2.3 PD-L1 Testing
PD-L1 expression was determined by IHC using the Dako 22C3 pharmDx kit, considering more than 100 tumor cells in the slide section for accurate PD-L1 readings. PD-L1 testing was completed on biopsies taken at diagnosis. For survival analyses, patients were stratified according to PD-L1 status (i.e., ≥ 50%, 1–49%, and < 1% subgroups). Patients with unknown PD-L1-expression status were also included in this study.
2.4 cfDNA Detection (Week 8) by Droplet Digital PCR Analysis
The first blood sample was collected at the time of diagnosis before the start of treatment. Circulating free DNA (cfDNA) was quantified using the QX200 Droplet Digital PCR System (Bio-Rad Laboratories, Hercules, CA). For the EGFR multiplex assays, a final PCR mix volume of 20 μL was manually loaded into wells of a DG8 cartridge (Bio-Rad Laboratories) with 70 μL of Droplet Generation Oil for probes (Bio-Rad Laboratories). After droplet generation by the QX200 Droplet Generator (Bio-Rad Laboratories), 40 μL of the sample was transferred into a 96-well PCR plate and amplified with a C1000 Touch Thermal Cycler (Bio-Rad Laboratories), using the following thermal cycling conditions: 95 °C for 10 min, 40 cycles at 94 °C for 30 s, 55 °C for 1 min (2 °C/s), and 98 °C for 10 min, and a final cooling step to 12 °C (1 °C/s). The droplets were analyzed using the QX200 Droplet Reader (Bio-Rad Laboratories), and data were analyzed using QuantaSoft software version 1.7.4.0917 and QuantaSoft Analysis Pro software version 1.0.596 (Bio-Rad Laboratories). Thresholds were placed manually, and the fractions of positive and negative droplets were used to calculate the concentration and fractional abundance of target DNA sequences with their 95% Poisson-based confidence intervals (CI). EGFRm primers and probes were based on previous studies [27, 28].
2.5 AXL and BIM mRNA Quantification by RT-PCR Analyses
Samples were lysed in a buffer containing EDTA, SDS, and proteinase K. Then RNA was extracted with phenol-chloroform-isoamyl alcohol, followed by precipitation with isopropanol in the presence of glycogen and sodium acetate. RNA was homogenized in water and treated with DNAse I to avoid DNA contamination. Complementary DNA (cDNA) was synthesized using M-MLV (Moloney Murine Leukemia Virus Reverse Transcriptase) retro-transcriptase enzyme. cDNA was added to Taqman Universal Master Mix in a 12.5-μL reaction with specific primers and probes for each gene. The primer and probe sets were designed using the LightCycler® Probe Design Software 2.0 (Roche Diagnostics Corporation, Indianapolis, Indiana) according to their Ref Seq (National Center for Biotechnology Information). Quantification of gene expression was performed using the LightCycler® 480 Real-Time PCR System (Roche Diagnostics Corporation, Indianapolis, Indiana) and calculated according to the comparative Ct method. The final results were determined as follows: 2-(ΔCt sample-ΔCt calibrator), where ΔCt values of the calibrator and sample are determined by subtracting the Ct value of the target gene from the value of the endogenous gene (β-actin). Commercial RNA controls were used as calibrators (Stratagene, La Jolla, CA, USA). In quantitative experiments, a sample was considered non-viable when the standard deviation (SD) of the Ct values was ≥ 0.30 in two independent analyses. To dichotomize the mRNA expression levels, AXL 1.42 (high AXL [AXL-H] ≥ 1.42) and BIM 0.98 (high BIM [BIM-H] ≥ 0.98) were used as cut-off points; the cut-off points are based on the values described in the existing evidence [29, 30].
2.6 Next-Generation Sequencing
cDNA synthesis prior to library preparation for the RNA panel was carried out using SuperScript™ VILO™ cDNA Synthesis Kit (Thermo Fisher Scientific, 2018, 11754050). Library preparation was carried out using the Oncomine™ Comprehensive Assay Plus (Thermo Fisher Scientific, A49667) and RNA Oncomine™ Fusion's assay (Thermo Fisher Scientific) kits following the instructions of the manufacturer and using a total of 10 ng input DNA and/or RNA per sample (minimum 0.83 ng/μL sample DNA concentration). A maximum of seven DNA samples were prepared per run (six samples if both DNA and RNA analyses were required) on an Ion 540™ Chip (Thermo Fisher Scientific, A27765) using the Ion S5™ sequencing system (see the electronic supplementary material, Supplementary Data 1 and 2). The DNA panel can identify hotspot mutations and copy number variations (CNVs), full coding DNA sequences (CDSs), and RNA fusions (Supplementary Table 1 shows the genes and alterations included in the analysis). Template preparation was performed on the Ion Chef System (Thermo Fisher Scientific) using the Ion PGM Hi-Q Chef Kit and/or the Ion One Touch™ 2 System using the Ion PGM Template OT2 200 Kit. Sequencing was performed using the Ion PGM Hi-Q Sequencing Kit on the Ion Torrent Personal Genome Machine. TMB was measured by running the Oncomine Tumor Mutation Load Assay (Thermo Fisher Scientific, A37909), which enables accurate measurements of somatic mutations without needing a matched normal sample. This assay covers a large genomic footprint of 1.7 Mb, encompassing 1.2 Mb of exonic sequence, to enable accurate mutation counts for samples with a range of TMBs. For the analysis, TMB–high (TMB-H) was defined as ≥ 10 mutations/megabase [mut/Mb]) using the same cut-off as in the KEYNOTE-158 study (NCT02628067) [31].
2.7 Next-Generation Sequencing Data Analysis
Ion Torrent Suite™ Browser version 5.0 and Ion Reporter™ version 5.0 were used to analyze the NGS data. The Torrent Suite™ Browser was used to perform initial quality control, including chip loading density, median read length, and the number of mapped reads. The Coverage Analysis plugin was applied to all data to assess amplicon coverage for regions of interest. Variants were identified by the Ion Reporter filter chain 5% Oncomine™ Variants (5.0). A cut-off of 500X coverage was applied to all analyses. All identified variants were checked for correct nomenclature using Alamut Visual v.2.7.1 (Interactive Biosoftware). Any discrepancies in variant identification between Ion Reporter and Alamut were validated manually using the Integrative Genomics Viewer and NextGENe® v2.4.2 (SoftGenetics®) [32, 33].
2.8 Statistical Analysis
All analyses were conducted on IBM SPSS Statistics software version 25.0 (SPSS Inc. Chicago, IL, USA). Descriptive analyses were used to provide an overview of the study population characteristics. Categorical variables were assessed via the Chi-square test or, whenever appropriate, Fisher’s Exact test. OS and PFS were reported as Kaplan–Meier survival curves. Univariable regression analysis models were generated to assess potential confounders. Mann–Whitney U test with a two-sided P value was established to determine statistically significant outcomes. There were no adjustments made for multiple comparisons, and in all cases, the significance level was 0.05.
3 Results
3.1 Baseline Patient Characteristics
The clinical information derived from 32 Hispanic patients with NSCLC and EGFRm is summarized in Table 1. Demographic characteristics indicate that all patients were diagnosed at stage IV, and most patients had an adenocarcinoma histology type (96.9%), mainly solid or lepidic patterns (56.3%). There is a higher proportion of female patients in both cohorts (60%), and at least 65% had a negative smoking history. Most patients had pleuropulmonary compromise (87.5%) and good functional status (Eastern Cooperative Oncology Group, ECOG performance status 0–1, 90.7%). Samples were obtained from the lung or pleural space in 90.6%. Most patients had a liquid biopsy at progression (96.9%), and in two cases, tumor tissue was obtained by repeated biopsy. Both cases confirm the suspicion of differentiation to SCLC. Overall, the distribution of EGFR-sensitizing mutations was comparable in the population, including ex19dels and L858R mutations. However, patients in cohort A had significantly more frequent alterations in exon 21 than in cohort B in exon 19 (P = 0.0001). Seven patients had secondary EGFRm (21.9%), which occurred more frequently in cohort B (P = 0.32). A baseline T790M mutation was identified in five cases, four in cohort A (P = 0.16), with a mean allele frequency of 39 (SD ± 20). Thirteen patients (87.5%) in cohort A had more than three co-mutations at the time of diagnosis, a significantly higher finding than for cohort B (P = 0.0001). Almost all baseline TP53 commutations (82.4%) and those involving the RAF pathway were identified among patients in cohort A (P = 0.001 and P = 0.009). Besides EGFR and TP53 genes, the main commutations identified at baseline included RB1, AT-rich interactive domain-containing protein 1A [ARID1A], and BRAF. Fig. 2 shows the primary baseline genomic alterations identified in both cohorts, and Supplementary Table 2 details the variants detected at diagnosis (see the electronic supplementary material).

Genomic characteristics (including copy number variation and TMB) of patients with mutations in cohorts A and B. EGFR epidermal growth factor receptor, TMB tumor mutational burden, TMB-H tumor mutation burden–high, TMB-L tumor mutation burden–low
The baseline TMB was obtained in 27 patients, among whom 22 (68.8%) had a low TMB (TMB-L). It is important to note that cohort A included five patients (31.3%) with TMB-H, while in cohort A, all patients with available data (11/16; 68.8%) had TMB-L (P = 0.054). Based on the mRNA levels stratification, there was a statistically significant difference when AXL and BIM levels were compared among both cohorts (81.3%, N = 13, cohort A patients had AXL-H; 93.8%, N = 15, had BIM-H; 75%, N = 12, cohort B patients had low AXL [AXL-L]; 85.7%, N = 14, had low BIM [BIM-L]). As shown in Supplementary Fig. 1, both differences in mRNA levels between cohorts A and B were statistically significant. Monitoring of response to osimertinib using ddPCR multiplex assays performed at week 8 was positive in 18 patients (56.3%); 93.8% and 18.8% of patients in cohorts A and B had cfDNA detectable by ddPCR, and this difference was statistically significant (P = 0.0001; Supplementary Fig. 2). In terms of PD-L1, most patients had < 1% (N = 3; 18.8%) and 1–49% (N = 11; 68.8%) in cohort A. Similarly, in cohort B, most patients had < 1% (N = 6; 37.5%) and 1–49% (N = 10; 62.5%). Only two patients had PD-L1 ≥ 50% in the study population, both from cohort A.
3.2 Outcomes Obtained with First-Line Osimertinib
The median time between the first sample and the start of therapy was 15 days, and the median time between the start of therapy and the first follow-up evaluation was 60 days (± 4 days). The ORRs for cohorts A and B were 6.3% and 100.0% (P = 0.0001), respectively. Only one of the patients with primary resistance to osimertinib had a short-lived PR, with subsequent multifocal progression, including the brain. On the contrary, in cohort B, 31.3% achieved a CR and 68.8% a PR. In both cohorts, the leading site of progression was the lung (≈60%), and cohort A patients had twice as many brain metastases, generally in the first 6 months after diagnosis (P = 0.67). PFS with osimertinib was 3.1 months (95% CI 0.47–7.0) for cohort A and NR for cohort B (P = 0.0001) (Fig. 3A). PFS was significantly higher in patients with ex19del compared with those with L858R mutations (24.5 months, 95% CI 18.2–NR, vs. 7.6 months, 95% CI 4.8–21.1; P = 0.001) (Supplementary Fig. 3; see the electronic supplementary material) and in those without brain metastases at diagnosis compared with patients with baseline brain metastases (24.5 months, 95% CI 18.5–30.5, vs. 7.2 months, 95% CI 1.1–13.2; P = 0.004) (Supplementary Fig. 4). The baseline T790M mutation also negatively impacted PFS (Supplementary Fig. 5); similarly, the presence of mutations in TP53 (P = 0.001), a higher number of commutations at diagnosis (P = 0.0001; Supplementary Fig. 6), and TMB-H (P = 0.017; Supplementary Fig. 7) were associated with worse PFS. In contrast, the PD-L1 expression level did not significantly affect PFS (P = 0.36). Given the biological differences between cohort A and B, high mRNA levels of AXL (P = 0.0001) and low BIM (P = 0.001) also affected PFS, as did the presence of cfDNA in liquid biopsies obtained 8 weeks after starting treatment with osimertinib (P = 0.001).

PFS (A) and OS (B) for cohorts A and B. PFS with osimertinib was 3.1 months (95% CI 0.47–7.0) for cohort A and NR for cohort B (P = 0.0001) (A). After a median follow-up of 25.1 months (95% CI 11.0–43.0), the OS for cohorts A and B was 20.1 months (95% CI 10.4–29.2) and NR (P = 0.0001) (B). CI confidence interval, OS overall survival, PFS progression-free survival, NR Not reached.
After a median follow-up of 25.1 months (95% CI 11.0–43.0), the OS for cohorts A and B was 20.1 months (95% CI 10.4–29.2) and NR (P = 0.0001, Fig. 3B). OS was higher for patients with ex19del (P = 0.002; Supplementary Fig. 3B), those without baseline brain metastases (P = 0.013; Supplementary Fig. 4B), those with two or fewer commutations (P = 0001; Supplementary Fig. 6B), and those with TMB-L (P = 0.0001; Supplementary Fig. 7B).
PD-L1 expression was significantly associated with OS, favoring the group of patients with a negative immunophenotype (PD-L1 < 1% 34.1 months, 95% CI 30.6–37.6, vs. PD-L1 1–49% 31.6 months, 95% CI 13.7–24.5, vs. PD-L1 ≥ 50% 19.1 months, 95% CI 13.7–24.5; P = 0.029). Low mRNA expression levels for AXL (P = 0.001) and high mRNA expression levels for BIM (P = 0.0001) and the absence of detectable cfDNA at week 8 of treatment (P = 0.001) were also significantly associated with OS (Supplementary Fig. 8A–C). Contrary to the findings for PFS, the presence of baseline T790M did not significantly impact OS (P = 0.06; Supplementary Fig. 5B). Univariate analysis showed that the variables that most negatively influenced PFS and OS were the presence of brain metastases (P = 0.002), evidence of a more significant number of commutations (P = 0.001), TMB-H (P = 0.0001), and the high levels of mRNA of AXL (P = 0.01) and low BIM (P = 0.02).
3.3 Genomic Alterations Found in Liquid Biopsy After Progression to Osimertinib
Figure 4 summarizes the main alterations in the liquid biopsy after progression to osimertinib (31 patients had a liquid biopsy, and one patient had pleural effusion cell block analysis). Sixty-four genomic alterations were found at the time of progression, 45 in cohort A (70%) and 19 in cohort B (30%). In cohort A, six patients (37.5%) lost the EGFR-sensitizing mutation, a condition that did not occur in any patient in cohort B (P = 0.01). In addition, in cohort A, off-target alterations were dominant, mainly in TP53 (13/35.5%), the RAS pathway (13/35.5%), PI3K (4/8.8%), and RB1 (2/4.4%). In contrast, most alterations in cohort B were due to on-target (6/31.2%) or included MET amplification (3/15.8%), the RAS pathway (2/10.5%), GNAS (2/ 10.5%), or RB1 (2/10.5%). After the second line, two patients had transformation to small cell carcinoma (6.3%), confirmed by biopsy, with mutations in TP53 and RB1. Post-osimertinib mean TMB was 5.0 (SD ± 3.6), with no significant differences between the two cohorts. Supplementary Fig. 9 shows a representative case of primary resistance to osimertinib, including genomic variations throughout the history of the disease (see the electronic supplementary material).

Genomic alterations were identified at osimertinib progression (liquid biopsy in blood or pleural fluid) considering mutations (A) and amplifications (B). All patients in cohort A had two or more commutations, while in cohort B, only three had a commutation. C Amplifications identified at the time of progression to osimertinib
3.4 Second-Line Therapy
Thirty-one patients received second-line treatment (95.6%), mainly with the IMPOWER-150 study schedule (75%) or with the carboplatin/pemetrexed/bevacizumab combination (12.5%). The ORR for the second line was 68.8% (23 cases achieved PR), with no statistically significant difference between the two cohorts. The median PFS obtained with the second line was 8.1 months (95% CI 3.2–12.1) and 11.2 months (95% CI 9.8–12.5; P = 0.22) for cohorts A and B, respectively. The only variable that affected PFS for the second line was PD-L1 expression (PD-L1 < 1% 7.8 months, 95% CI 6.4–8.7, vs. PD-L1 1–49% 9.2 months, 95% CI 8.7–11.2, vs. PD-L1 ≥ 50% 11.6 months, 95% CI 7.3–13.7; P = 0.021).
4 Discussion
The mutational landscape for EGFR-TKI-sensitizing alterations plays a significant role in determining treatment efficacy for patients with NSCLC, and an in-depth understanding of this landscape offers an improved therapeutic approach. Nonetheless, the alterations that involve primary resistance to treatment with osimertinib among patients with EGFRm NSCLC have not been extensively characterized according to the observed ethnic variation in low-middle-income countries. In this study, we characterized the molecular determinants present in tumors of patients who do not respond to first-line treatment with osimertinib and compared them to patients with durable responses to osimertinib. Our results demonstrated that potential factors associated with poor survival outcomes under osimertinib treatment include the presence of three or more commutations (mainly including the TP53 gene), high levels of AXL mRNA, low levels of BIM mRNA, T790M gene de novo presence, TMB-H, and EGFR p.L858R variant presence.
Although TKI-acquired resistance has been extensively studied, there are more studies about the molecular interactions that bypass the action of TKI than primary resistance [34]. After exposure to osimertinib, ORR was considerably lower in cohort A (6.3%), with lung involvement as the leading site of progression and two times higher brain involvement. EGFRm are associated with the progression of the disease, and the brain is one of the primary sites of metastasis; in fact, patients with T790M usually have a higher brain compromise [35].
TMB-H, high expression levels of AXL mRNA, and low mRNA levels of BIM were commonly identified in patients with intrinsic resistance. These alterations could add genomic instability burden to the tumor and, in fact, resistance to TKI inhibitors [36, 37]. AXL is a tyrosine kinase receptor that transduces signals from the extracellular matrix into the cytoplasm by binding growth factor GAS6, thus regulating many physiological processes, including cell survival, cell proliferation, migration, and differentiation [38]. High expression of the AXL protein in tumors is reported to be associated with poor prognosis and acquired resistance to targeted therapy in several types of cancer, including glioblastoma, breast cancer, lung cancer, and acute myeloid leukemia [39, 40]. Recently, Taniguchi et al. showed that osimertinib stimulated AXL, which binds to the HER family proteins EGFR and HER3 through a negative feedback loop involving the suppression of sprouty RTK signaling antagonist 4 (SPRY4). In sequence, activated AXL was associated with EGFR and HER3 in maintaining cell survival and inducing the emergence of cells tolerant to osimertinib [36]. Likewise, AXL hyperactivity also includes resistance through EMT closely associated with tumor heterogeneity and induces variations in pathways, including MET, platelet-derived growth factor receptor (PDGFR), and MAPK [39, 41, 42]. In our study, 81% of the cases in cohort A had high levels of AXL mRNA expression, values that were 1.5 times higher than those observed in cohort B.
As mentioned above, low levels of BIM mRNA were associated with a worse prognosis. BIM is a BH3-only protein that directly activates the ultimate effectors of apoptosis BAK (BCL-2 antagonist or killer) and BAX (BCL-2-associated X protein) [43]. Recently, Karachaliou and colleagues assessed the role of BIM mRNA expression in patients treated in the EURTAC study [44]. The analysis shows that PFS and OS were significantly longer for patients with high BIM expression than for those with low/intermediate BIM mRNA expression. Patients with low BIM expression could derive only a meager benefit from treatment with EGFR-TKI alone. Still, they could benefit from synthetic lethality combinations, including small molecules that mimic the BH3 motif [30]. Previous evidence suggested that gefitinib combined with the BH3 mimetic ABT-737 (an analog of navitoclax) substantially increases apoptosis compared with each agent alone in EGFR-mutant H1650 cells with low BIM expression [37, 45].
PFS and OS were also significantly lower among patients with primary resistance. In cohort A, patients with ex19del had a higher PFS (and presence of brain metastasis) than those with L858R. Hong et al. had previously described that L858R could have a negative prognostic value in NSCLC patients. In their cohort, patients with mutations in exon 21 had a PFS of almost 8 months [46,47,48]. In a similar way, in a Korean cohort of patients, ex19del and no brain involvement were associated with a better PFS under TKI treatment [49]. However, for the same cohort, PFS was negatively affected by the presence of T790M, even under treatment with third-line TKI osimertinib. This finding could be explained under the theory of T790M as one possible intrinsic resistance mechanism. However, T790M can also favor other resistance mechanisms, MET amplification among them [50]. In our study, cohort A reported a big proportion of basal L858R mutation, whereas cohort B had ex19del predominately. It is essential to address that the presence of ex19del has been associated with better outcomes [3, 8]. However, commutations alter disease progression by modulating the sensitivity to TKI and facilitating more aggressive tumor biology. ex19del alterations are associated with TMB-L impacting OS and not PFS. As Choi et al. demonstrated, the presence of ex19del is associated with a good OS, even under treatment with first-line TKI [51]. However, in our study, patients were treated with a third-generation TKI with better efficacy than other first- or second-generation TKI. In the absence of L858R mutation, the better outcomes under TKI could be related to the description of EGFR ex19del as a more sensitizing mutation that causes changes in phosphorylation and downstream signaling that result in a better response to osimertinib [52, 53].
TMB has been characterized as a possible predictor factor of targeted therapy response. Previous studies have reported the association between TMB-H with outcomes and a shorter time to treatment discontinuation among patients with EGFR-mutated NSCLC under TKI treatment. A cohort presented by Offin et al. showed a negative relationship between a higher TMB and OS [54]. Some authors mention that TMB-H can be associated with the sub-clone presence that could favor resistant cell populations under TKI treatment. TMB could be a marker of propensity towards mutagenesis, mainly among EGFR-mutant NSCLC [55, 56]. Interestingly, after osimertinib treatment, TMB was not different between the cohorts, suggesting that genomic heterogenicity could be pre-established before selection under TKI.
Regarding the genomic alterations presented after progression to osimertinib, almost two-thirds were identified among patients in the cohort classified as having primary resistance. For this group, some patients lost the EGFR-sensitizing mutation. In vitro studies have suggested that this loss could be a possible mechanism of TKI resistance, at least for first- or second-generation TKI [57]. Remarkably, for the cohort with primary resistance, the genomic alterations identified were off-target mutations. TP53 and KRAS pathway RB1 were the most common. In the context of the EGFR-independent resistance mechanism, TP53 and RB1 tumor suppressor genes could be identified in almost 50% of LUAD among Caucasian patients [26, 58, 59]. According to the evidence, TP53 alterations appear during advanced disease, playing a key role in tumor progression more than tumor initiation. TP53/RB1 mutations in NSCLC are associated with transformation to SCLC under TKI treatment [60, 61]. The two patients who presented phenotypic transformation had TP53 and RB1 mutations at the time of biopsy confirmation. KRAS is another EGFR-independent resistance mechanism that was reported in our study. Although EGFR and KRAS commutations are rare, KRAS amplification could favor resistance through ERBB-family upregulation [20, 62] As expected, in cohort B, MET amplification was a common mutation. It is known that under treatment with TKI, MET alterations can be found in almost 5% and 20% of patients treated with first- and second-generation EGFR-TKI and osimertinib, respectively [23, 63, 64].
This study, as with other studies focused on specific genomic characterization of primary resistance, has some limitations, such as the small sample size and the specific population that affects external validity. Also, based on the characteristics of the patients, matching both cohorts was not feasible, which might limit the extent of the comparison between cohorts.
5 Conclusions
Understanding the molecular mechanisms that favor primary resistance to EGFR-TKI is fundamental to choosing NSCLC treatment and finding new molecular targets. Targeting EGFR could force the selection of tumors with other molecular pathway alterations that allow tumor progression. EGFR-independent mechanisms of resistance (or off-target alterations) were found in a population with primary resistance. Treatment with the third-generation TKI osimertinib produces very limited survival outcomes for patients with off-target alterations. These data evidence the need for molecular profiling of patients before the beginning of treatment and the challenge of developing new therapeutic approaches based on specific molecular alterations. As the presence of cfDNA at the time of progression was associated with poor outcomes, liquid biopsy reinforces its role in monitoring the prognosis among NSCLC Hispanic patients.
Data availability
The datasets presented in this article are not readily available because the Colombian organic law of data protection limits access to genetic information in an open format. Requests to access the datasets should be directed to the corresponding author, who will release it upon formal request to the Ministry of Health of Colombia following the requirements of Law 1581 of 2012, paragraph 201811601170851 of 2018.
References
O’Leary C, Gasper H, Sahin KB, Tang M, Kulasinghe A, Adams MN, et al. Epidermal growth factor receptor (EGFR)-mutated non-small-cell lung cancer (NSCLC). Pharmaceuticals. 2020;13(10):1–16.
Piotrowska Z, Sequist LV. Epidermal growth factor receptor-mutant lung cancer new drugs, new resistance mechanisms, and future treatment options. Cancer J. 2015;21(5):371–2.
Midha A, Dearden S, Mccormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res. 2015;5(9):2892–911.
Campbell JD, Lathan C, Sholl L, Ducar M, Vega M, Sunkavalli A, et al. Comparison of prevalence and types of mutations in lung cancers among black and white populations. JAMA Oncol. 2017;3(6):801–9.
Arrieta O, Cardona AF, Martín C, Más-López L, Corrales-Rodríguez L, Bramuglia G, et al. Updated frequency of EGFR and KRAS mutations in NonSmall-cell lung cancer in Latin America: the Latin-American consortium for the investigation of lung cancer (CLICaP). J Thorac Oncol. 2015;10(5):838–43.
Gimbrone NT, Sarcar B, Gordian ER, Rivera JI, Lopez C, Yoder SJ, et al. Somatic mutations and ancestry markers in hispanic lung cancer patients. J Thorac Oncol. 2017;12(12):1851–6.
Leal LF, de Paula FE, de Marchi P, de Souza VL, Pinto GDJ, Carlos CD, et al. Mutational profile of Brazilian lung adenocarcinoma unveils association of EGFR mutations with high Asian ancestry and independent prognostic role of KRAS mutations. Sci Rep. 2019;9(1):3209.
Chen J, Yang H, Teo ASM, Amer LB, Sherbaf FG, Tan CQ, et al. Genomic landscape of lung adenocarcinoma in East Asians. Nat Genet. 2020;52(2):177–86.
Koivunen JP, Kim J, Lee J, Rogers AM, Park JO, Zhao X, et al. Mutations in the LKB1 tumour suppressor are frequently detected in tumours from Caucasian but not Asian lung cancer patients. Br J Cancer. 2008;99(2):245–52.
Morgillo F, della Corte CM, Fasano M, Ciardiello F. Mechanisms of resistance to EGFR-targeted drugs: lung cancer. ESMO Open. 2016;1(3): e000060.
Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl Med. 2004;21(20):2129–39.
Sharma SV, Bell DW, Settleman J, Haber DA. Epidermal growth factor receptor mutations in lung cancer. Nat Rev Cancer. 2007;7:169–81.
D’Angelo SP, Pietanza MC, Johnson ML, Riely GJ, Miller VA, Sima CS, et al. Incidence of EGFR Exon 19 deletions and 1858R in tumor specimens from men and cigarette smokers with lung adenocarcinomas. J Clin Oncol. 2011;29(15):2066–70.
National Comprehensive Cancer Network. Non-Small Cell Lung Cancer Early and Locally Advanced [Internet]. NCCN Clinical Practice Guidelines in Oncology. 2022. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Accessed 28 Nov 2022.
Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med. 2018;378(2):113–25.
Ramalingam SS, Yang C-HJ, Khoon Lee C, Kurata T, Kim DW, John T, et al. Osimertinib as first-line treatment of EGFR mutation-positive advanced non-small-cell lung cancer. J Clin Oncol. 2017;36:841–9.
Reungwetwattana T, Nakagawa K, Cho BC, Cobo M, Cho EK, Bertolini A, et al. CNS response to osimertinib versus standard epidermal growth factor receptor tyrosine kinase inhibitors in patients with untreated EGFR-mutated advanced non-small-cell lung cancer. J Clin Oncol. 2018;36:3290–7.
Lorenzi M, Ferro A, Cecere F, Scattolin D, del Conte A, Follador A, et al. First-line osimertinib in patients with EGFR-mutant advanced non-small cell lung cancer: outcome and safety in the real world: FLOWER study. Oncologist. 2021;27(2):E87-115.
Jackman D, Pao W, Riely GJ, Engelman JA, Kris MG, Jänne PA, et al. Clinical definition of acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors in non-small-cell lung cancer. J Clin Oncol. 2010;28(2):357–60.
Wang J, Wang B, Chu H, Yao Y. Intrinsic resistance to EGFR tyrosine kinase inhibitors in advanced non-small-cell lung cancer with activating EGFR mutations. OncoTargets Therapy. 2016;9:3711–26.
Passaro A, Jänne PA, Mok T, Peters S. Overcoming therapy resistance in EGFR-mutant lung cancer. Nat Cancer. 2021;2:377–91.
Dong L, Lei D, Zhang H. Clinical strategies for acquired epidermal growth factor receptor tyrosine kinase inhibitor resistance in non-small-cell lung cancer patients. Oncotarget. 2017;8(38):64600–6.
Minari R, Bordi P, Tiseo M. Third-generation epidermal growth factor receptor-tyrosine kinase inhibitors in T790M-positive non-small cell lung cancer: review on emerged mechanisms of resistance. Transl Lung Cancer Res. 2016;5(6):695–708.
Blakely CM, Watkins TBK, Wu W, Gini B, Chabon JJ, McCoach CE, et al. Evolution and clinical impact of co-occurring genetic alterations in advanced-stage EGFR-mutant lung cancers. Nat Genet. 2017;49(12):1693–704.
Jordan EJ, Kim HR, Arcila ME, Barron D, Chakravarty D, Gao JJ, et al. Prospective comprehensive molecular characterization of lung adenocarcinomas for efficient patient matching to approved and emerging therapies. Cancer Discov. 2017;7(6):596–609.
Santoni-Rugiu E, Melchior LC, Urbanska EM, Jakobsen JN, de Stricker K, Grauslund M, et al. Intrinsic resistance to EGFR-tyrosine kinase inhibitors in EGFR-mutant non-small cell lung cancer: differences and similarities with acquired resistance. Cancers (Basel). 2019;11(7):923.
Oxnard GR, Paweletz CP, Kuang Y, Mach SL, O’Connell A, Messineo MM, et al. Noninvasive detection of response and resistance in egfrmutant lung cancer using quantitative next-generation genotyping of cell-free plasma DNA. Clin Cancer Res. 2014;20(6):1698–705.
Zhu G, Ye X, Dong Z, Lu YC, Sun Y, Liu Y, et al. Highly sensitive droplet digital PCR method for detection of EGFR-activating mutations in plasma cell-free DNA from patients with advanced non-small cell lung cancer. J Mol Diagn. 2015;17(3):265–72.
Karachaliou N, Chaib I, Cardona AF, Berenguer J, Bracht JWP, Yang J, et al. Common co-activation of AXL and CDCP1 in EGFR-mutation-positive non-smallcell lung cancer associated with poor prognosis. EBioMedicine. 2018;29:112–27.
Karachaliou N, Codony-Servat J, Teixidó C, Pilotto S, Drozdowskyj A, Codony-Servat C, et al. BIM and mTOR expression levels predict outcome to erlotinib in EGFR-mutant non-small-cell lung cancer. Sci Rep. 2015;5:17499.
Marabelle A, Le DT, Ascierto PA, di Giacomo M, de Jesus-Acosta A, et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/ mismatch repair-deficient cancer: results from the phase II KEYNOTE-158 study. J Clin Oncol. 2020;38(1):1–10.
Thorvaldsdóttir H, Robinson JT, Mesirov JP. Integrative Genomics Viewer (IGV): high-performance genomics data visualization and exploration. Brief Bioinform. 2013;14(2):178–92.
Robinson JT, Thorvaldsdóttir H, Winckler W, Guttman M, Lander ES, Getz G, et al. Integrative genomics viewer. Nat Biotechnol. 2011;29(1):24–6.
Nan X, Xie C, Yu X, Liu J. EGFR TKI as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer. Oncotarget. 2017;8(43):75712–26.
Chen Y, Deng J, Liu Y, Wang H, Zhao S, He Y, et al. Analysis of metastases in non-small cell lung cancer patients with epidermal growth factor receptor mutation. Ann Transl Med. 2021;9(3):206–206.
Taniguchi H, Yamada T, Wang R, Tanimura K, Adachi Y, Nishiyama A, et al. AXL confers intrinsic resistance to osimertinib and advances the emergence of tolerant cells. Nat Commun. 2019;10(1):259.
Su W, Zhang X, Cai X, Peng M, Wang F, Wang Y. BIM deletion polymorphism predicts poor response to EGFR-TKIs in nonsmall cell lung cancer: An updated meta-analysis. Medicine. 2019;98(10): e14568.
Zhu C, Wei Y, Wei X. AXL receptor tyrosine kinase as a promising anti-cancer approach: functions, molecular mechanisms and clinical applications. Mol Cancer. 2019;18(1):153.
Zhang Z, Lee JC, Lin L, Olivas V, Au V, Laframboise T, et al. Activation of the AXL kinase causes resistance to EGFR-targeted therapy in lung cancer. Nat Genet. 2012;44(8):852–60.
Wu Z, Bai F, Fan L, Pang W, Han R, Wang J, et al. Coexpression of receptor tyrosine kinase AXL and EGFR in human primary lung adenocarcinomas. Hum Pathol. 2015;46(12):1935–44.
Brand TM, Iida M, Stein AP, Corrigan KL, Braverman CM, Luthar N, et al. AXL mediates resistance to cetuximab therapy. Cancer Res. 2014;74(18):5152–64.
Meyer AS, Miller MA, Gertler FB, Lauffenburger DA. The receptor AXL diversifies EGFR signaling and limits the response to EGFR-targeted inhibitors in triple-negative breast cancer cells. Sci Signal. 2013;6(287):ra66.
Letai A, Bassik M, Walensky L, Sorcinelli M, Weiler S, Korsmeyer S. Distinct BH3 domains either sensitize or activate mitochondrial apoptosis, serving as prototype cancer therapeutics. Cancer Cell. 2002;2(3):183–92.
Costa C, Molina MA, Drozdowskyj A, Gimeńez-Capitán A, Bertran-Alamillo J, Karachaliou N, et al. The impact of EGFR T790M mutations and BIM mRNA expression on outcome in patients with EGFR-Mutant NSCLC treated with erlotinib or chemotherapy in the randomized phase III EURTAC trial. Clin Cancer Res. 2014;20(7):2001–10.
Cragg M, Kuroda J, Puthalakath H, Huang D, Strasser A. Gefitinib-induced killing of NSCLC cell lines expressing mutant EGFR requires BIM and can be enhanced by BH3 mimetics. PLoS ONE. 2007;4(10):1681–9.
Hong W, Wu Q, Zhang J, Zhou Y. Prognostic value of EGFR 19-del and 21–L858R mutations in patients with non-small cell lung cancer. Oncol Lett. 2019;18(4):3887–95.
Kuan FC, Kuo LT, Chen MC, Yang CT, Shi CS, Teng D, et al. Overall survival benefits of first-line EGFR tyrosine kinase inhibitors in EGFR-mutated non-small-cell lung cancers: a systematic review and meta-analysis. Br J Cancer. 2015;113(10):1519–28.
Leal JL, Alexander M, Itchins M, Wright GM, Kao S, Hughes BGM, et al. EGFR Exon 20 insertion mutations: clinicopathological characteristics and treatment outcomes in advanced non-small cell lung cancer: EGFR Exon 20 insertion mutations in NSCLC. Clin Lung Cancer. 2021;22(6):e859–69.
Jung HA, Woo SY, Lee SH, Ahn JS, Ahn MJ, Park K, et al. The different central nervous system efficacy among gefitinib, erlotinib and afatinib in patients with epidermal growth factor receptor mutation-positive non-small cell lung cancer. Transl Lung Cancer Res. 2020;9(5):1749–58.
Suda K, Murakami I, Katayama T, Tomizawa K, Osada H, Sekido Y, et al. Reciprocal and complementary role of MET amplification and EGFR T790M mutation in acquired resistance to kinase inhibitors in lung cancer. Clin Cancer Res. 2010;16(22):5489–98.
Choi YW, Jeon SY, Jeong GS, Lee HW, Jeong SH, Kang SY, et al. EGFR Exon 19 deletion is associated with favorable overall survival after first-line gefitinib therapy in advanced non-small cell lung cancer patients. Am J Clin Oncol. 2018;41(4):385–90.
Okabe T, Okamoto I, Tamura K, Terashima M, Yoshida T, Satoh T, et al. Differential constitutive activation of the epidermal growth factor receptor in non-small cell lung cancer cells bearing EGFR gene mutation and amplification. Cancer Res. 2007;67(5):2046–53.
Zhu J, Zhong W, Zhang G, Li R, Zhang X, Guo A, et al. Better survival with EGFR exon 19 than exon 21 mutations in gefitinib-treated non-small cell lung cancer patients is due to differential inhibition of downstream signals. Cancer Lett. 2008;265(2):307–17.
Offin M, Rizvi H, Tenet M, Ni A, Sanchez-Vega F, Li BT, et al. Tumor mutation burden and efficacy of EGFR-tyrosine kinase inhibitors in patients with EGFR-mutant lung cancers. Clin Cancer Res. 2019;25(3):1063–9.
Cheng ML, Oxnard GR. Does TMB impact the effectiveness of TKIs in EGFR-mutant NSCLC? Clin Cancer Res. 2019;25(3):899–900.
Lin C, Shi X, Zhao J, He Q, Fan Y, Xu W, et al. Tumor mutation burden correlates with efficacy of chemotherapy/targeted therapy in advanced non-small cell lung cancer. Front Oncol. 2020;10:480.
Tabara K, Kanda R, Sonoda K, Kubo T, Murakami Y, Kawahara A, et al. Loss of activating EGFR mutant gene contributes to acquired resistance to EGFR tyrosine kinase inhibitors in lung cancer cells. PLoS ONE. 2012;7(7):e41017.
Jakobsen JN, Santoni-Rugiu E, Grauslund M, Melchior L, Sørensen JB. Concomitant driver mutations in advanced EGFR-mutated non-small-cell lung cancer and their impact on erlotinib treatment. Oncotarget. 2018;9(40):26195–208.
Lee T, Lee B, la Choi Y, Han J, Ahn MJ, Um SW. Non-small cell lung cancer with concomitant EGFR, KRAS, and ALK mutation: clinicopathologic features of 12 cases. J Pathol Transl Med. 2016;50(3):197–203.
Marcoux N, Gettinger SN, Grainne O, Arbour KC, Neal JW, Husain H, et al. EGFR-mutant adenocarcinomas that transform to small-cell lung cancer and other neuroendocrine carcinomas: clinical outcomes. J Clin Oncol. 2019;37(4):278–85.
Jamal-Hanjani M, Wilson GA, McGranahan N, Birkbak NJ, Watkins TBK, Veeriah S, et al. Tracking the evolution of non-small-cell lung cancer. N Engl J Med. 2017;376(22):2109–21.
Stewart EL, Tan SZ, Liu G, Tsao MS. Known and putative mechanisms of resistance to EGFR targeted therapies in NSCLC patients with EGFR mutations-a review. Transl Lung Cancer Res. 2015;4(1):67–81.
Piotrowska Z, Isozaki H, Lennerz JK, Gainor JF, Lennes IT, Zhu VW, et al. Landscape of acquired resistance to osimertinib in EGFR-mutant NSCLC and clinical validation of combined EGFR and RET inhibition with osimertinib and BLU-667 for acquired RET fusion. Cancer Discov. 2018;8(12):1529–39.
Tetsu O, Hangauer MJ, Phuchareon J, Eisele DW, McCormick F. Drug resistance to EGFR inhibitors in lung cancer. Chemotherapy. 2016;61(5):223–35.
Acknowledgements
Dora Lucia Vallejo-Ardila is supported by the Department of Science, Technology, and Innovation (COLCIENCIAS-Colombia) as part of her PhD overseas 679 scholarship program.
Funding
Open Access funding provided by Colombia Consortium.
Author information
Authors and Affiliations
Consortia
Contributions
Diego F. Chamorro: Conceptualization, methodology, formal analysis, investigation, data curation, writing-original draft, writing and review-editing, supervision. Andrés F. Cardona: Conceptualization, methodology, formal analysis, investigation, data curation, writing-original draft, writing and review-editing, supervision. July Rodríguez: Conceptualization, methodology, formal analysis, investigation, data curation. Alejandro Ruiz-Patiño: Conceptualization, methodology, formal analysis, investigation, data curation. Oscar Arrieta: Conceptualization, methodology, formal analysis, investigation, data curation. Darwin A. Moreno-Pérez: Leonardo Rojas: Formal analysis, investigation, data curation. Zyanya Lucia Zatarain-Barrón: Formal analysis, investigation, data curation. Dora V. Ardila: Formal analysis, investigation, data curation. Lucia Viola: Formal analysis, investigation, data curation. Gonzalo Recondo: Formal analysis, investigation, data curation. Juan B. Blaquier: Formal analysis, investigation, data curation. Claudio Martín: Formal analysis, investigation, data curation. Luis Raez: Formal analysis, investigation, data curation. Suraj Samtani: Formal analysis, investigation, data curation. Camila Ordóñez-Reyes: Formal analysis, investigation, data curation. Juan Esteban Garcia-Robledo: Formal analysis, investigation, data curation. Luis Corrales: Formal analysis, investigation, data curation. Carolina Sotelo: Formal analysis, investigation, data curation. Luisa Ricaurte: Formal analysis, investigation, data curation. Mauricio Cuello: Formal analysis, investigation, data curation. Sergio Mejía: Formal analysis, investigation, data curation. Elvira Jaller: Formal analysis, investigation, data curation. Carlos Vargas: Formal analysis, investigation, data curation. Hernán Carranza: Formal analysis, investigation, data curation. Jorge Otero: Formal analysis, investigation, data curation. Pilar Archila: Formal analysis, investigation, data curation. Maritza Bermudez: Formal analysis, investigation, data curation. Tatiana Gamez: Formal analysis, investigation, data curation. Alessandro Russo: Formal analysis, investigation, data curation. Umberto Malapelle: Formal analysis, investigation, data curation. Diego de Miguel Perez: Formal analysis, investigation, data curation. Vladmir C. Cordeiro de Lima: Helano Freitas: Formal analysis, investigation, data curation. Erick Saldahna: Formal analysis, investigation, data curation. Christian Rolfo: Formal analysis, investigation, data curation. Rafael Rosell: Formal analysis, investigation, data curation.
Corresponding author
Ethics declarations
Funding
This study was sponsored by the stipend PCI-2018-10171 of Universidad El Bosque (Bogotá, Colombia) and approved by the Institutional Ethics Committee (reference No. 019-2021). The CLICaP and the Foundation for Clinical and Applied Cancer Research—FICMAC (Bogotá, Colombia) supported some lab experiments through research grant 023-2019.
Conflict of interest
Andrés F. Cardona discloses financial research support from Merck Sharp & Dohme, Boehringer Ingelheim, Roche, Bristol-Myers Squibb, and the Foundation for Clinical and Applied Cancer Research—FICMAC. Additionally, he was linked to and received honoraria as an advisor to, participated in speakers' bureau for, and gave expert testimony to Merck Sharp & Dohme, Boehringer Ingelheim, Roche, Bristol-Myers Squibb, Pfizer, Novartis, Celldex Therapeutics, Foundation Medicine, Eli Lilly, and the Foundation for Clinical and Applied Cancer Research—FICMAC. Oscar Arrieta reports personal fees from Pfizer, grants and individual fees from Astra Zeneca, grants and individual fees from Boehringer-Ingelheim, personal fees from Lilly, individual fees from Merck, personal fees from Bristol Myers Squibb, and grants and personal fees from Roche, outside the submitted work. Gonzalo Recondo reports personal fees from Pfizer, Roche, Amgen, Bayer, Takeda, MSD, and Merck Serono, and research grants from Amgen and Janssen, outside of the submitted work. Juan Blaquier has nothing to disclose.
Ethics approval
All included patients provided signed informed consent. In addition, an Institutional Review Board and Privacy Board waiver was obtained to facilitate retrospective clinical-pathological and molecular data (Lung Cancer-FICMAC/CLICaP Platform—Registration No. 2012/014, Kayre, Bogotá, Colombia, and Research Ethics Committee of Universidad El Bosque—Registration No. PCI-2018-10171).
Consent to participate
See the ethics approval statement.
Consent for publication
Not applicable.
Code availability
Not applicable.
Additional information
CLICaP: Latin American Consortium for the Investigation of Lung Cancer.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Chamorro, D.F., Cardona, A.F., Rodríguez, J. et al. Genomic Landscape of Primary Resistance to Osimertinib Among Hispanic Patients with EGFR-Mutant Non-Small Cell Lung Cancer (NSCLC): Results of an Observational Longitudinal Cohort Study. Targ Oncol 18, 425–440 (2023). https://doi.org/10.1007/s11523-023-00955-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11523-023-00955-9