
Abstract
Background
Reverse total shoulder arthroplasty (RSA) is a standard treatment for proximal humeral fractures (PHF) and its sequelae. In this study we analyzed the clinical outcomes of primary vs. secondary RSA for displaced PHF in elderly patients.
Methods
We retrospectively reviewed 68 cases of primary or secondary RSA for displaced PHF. For 51 patients (28 primary RSA, 23 secondary RSA), a minimum 12-month follow-up with clinical and radiological assessment was available. Clinical assessment comprised joint active range of motion, DASH, Constant–Murley Score (CMS), Subjective Shoulder Value, and Visual Analog Scale for pain. Outcomes and complications of patients with primary RSA were compared with those of patients with secondary RSA.
Results
Follow-up data were available for 45 women and six men with a mean age of 73 years (range, 59–87) at the time of implantation. In 28 cases, primary RSA was performed; in 23 cases, RSA was performed as a revision procedure for fracture sequelae after failed plating, nailing, or hemiarthroplasty. The mean age- and gender-related CMS was 82.2 ± 34.2% (raw mean CMS: 46.8 ± 19.6 points). Among nine of the 51 patients with follow-up data (17.6%), ten complications occurred with six surgical revisions. Primary RSA (n = 28) resulted in better clinical shoulder function compared with secondary RSA (n = 23). Significantly more complications and revision surgeries were observed following secondary than primary RSA (p = 0.013).
Conclusion
In this study, primary RSA for displaced PHF in the elderly was associated with better clinical function and lower complication and revision rates than secondary RSA. Predictive parameters for failure of humeral head-preserving fracture fixation and anatomic hemiarthroplasty should be carefully evaluated. Primary RSA should be considered when surgical treatment of PHF is indicated in elderly patients.
Zusammenfassung
Hintergrund
Die inverse Schulterendoprothesenversorgung (RSA) stellt eine Standardbehandlung für die proximale Humerusfraktur (PHF) und ihre Folgen dar. In der vorliegenden Studie analysierten die Autoren die klinischen Ergebnisse der primären vs. sekundären RSA bei einer dislozierten PHF älterer Patienten.
Methoden
Retrospektiv wurden 68 Fälle mit primärer oder sekundärer RSA bei dislozierter PHF ausgewertet. Bei 51 Patienten (28 mit primärer RSA, 23 mit sekundärer RSA) waren Daten über eine mindestens 12-monatige Follow-up-Phase mit klinischer und radiologischer Untersuchung verfügbar. Zur klinischen Untersuchung gehörten der Bewegungsumfang des Gelenks, DASH („disability of shoulder, arms and hand questionnaire“), Constant-Murley-Score (CMS), Subjective Shoulder Value und Visuelle Analogskala für Schmerz. Ergebnisse und Komplikationen der Patienten mit primärer RSA wurden mit denen der Patienten mit sekundärer RSA verglichen.
Ergebnisse
Für 45 Frauen und 6 Männer mit einem Durchschnittsalter von 73 Jahren (Spanne: 59–87) zum Zeitpunkt der Implantation gab es Follow-up-Daten. In 28 Fällen wurde eine primäre RSA durchgeführt; in 23 Fällen erfolgte die RSA als Revisionsoperation wegen Frakturfolgen nach fehlgeschlagener Plattenversorgung, Nagelung oder Hemiarthroplastik. Der durchschnittliche alters- und geschlechtsbezogene CMS betrug 82,2 ± 34,2 % (Rohdurchschnittswert des CMS: 46,8 ± 19,6 Punkte). Bei 9 der 51 Patienten mit Follow-up-Daten (17,6 %) kam es zu 10 Komplikationen mit 6 chirurgischen Revisionen. Die primäre RSA (n = 28) führten zu einer besseren klinischen Schulterfunktion als die sekundäre RSA (n = 23). Nach sekundärer RSA wurden signifikant mehr Komplikationen und Revisionseingriffe als nach primärer RSA festgestellt (p = 0,013).
Schlussfolgerung
In der vorliegenden Studie stand die primäre RSA bei dislozierter PHF älterer Patienten im Zusammenhang mit besserer klinischer Funktion und geringeren Komplikations- und Revisionsraten als die sekundäre RSA. Prädiktive Parameter für einen Misserfolg der den Humeruskopf erhaltenden Frakturfixation und der anatomischen Hemiarthroplastik sollten sorgfältig beurteilt werden. Wenn die chirurgische Behandlung einer PHF bei älteren Patienten indiziert ist, sollte die primäre RSA erwogen werden.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Proximal humeral fractures (PHF) are common in daily clinical routine and many PHF can be treated non-operatively [1, 2]. Several surgical options exist for the treatment of displaced and comminuted PHF [1,2,3,4]. Owing to its complexity, the operative treatment of PHF remains a surgical challenge. Consequently, high complication rates have been reported, especially for humeral head-preserving fracture fixation in elderly patients [1,2,3,4, 10].
If surgery is the treatment of choice and it is not possible to achieve a stable reconstruction by internal fixation, primary fracture arthroplasty is indicated. Varus displaced four-part fractures in elderly patients, displaced multiple-part fractures with a small humeral head fragment, non-reducible head-split fractures, and depressed fractures with more than 40% joint involvement carry a high risk of ischemia and necrosis and primary fracture arthroplasty is usually recommended for these fracture types [5, 6]. The functional success of anatomic fracture arthroplasty is related to the correct ingrowth of the tuberosities [7, 8]. In the case of rotator cuff insufficiency or fatty degeneration of the muscles, reversed fracture arthroplasty is an alternative option [9, 10]. Because of tuberosity-related complications with anatomic hemiarthroplasty, primary reverse total shoulder arthroplasty (RSA) is increasingly recommended as a surgical treatment option for elderly patients with displaced PHF [9, 11].
Recent meta-analyses compared outcomes of hemiarthroplasty (HA) and RSA for fracture management and concluded that the RSA group outperformed the HA group, with a lower rate of complications and better clinical function [12,13,14,15, 25].
The most recent studies demonstrated pain relief and only moderate functional limitations after primary RSA [12, 14]. However, two major problems limit the use of RSA for the treatment of comminuted PHF: the high complication rate of up to 36% (10–36%) that has been reported [16,17,18,19], and the severe limitation in external rotation [9, 20].
The purpose of this study was to analyze clinical results from primary vs. secondary RSA for the treatment of complex PHF in elderly patients. We hypothesized lower complication rates and better functional outcomes for primary RSA compared with secondary RSA.
Methods
This IRB-approved retrospective study was conducted at a level‑1 trauma center. Patients treated with primary or secondary RSA for displaced proximal humeral fractures between January 2010 and December 2013 (n = 151) were screened for inclusion. Per this study’s exclusion criteria, patients with pathologic fracture, preoperative glenohumeral joint infection, preoperative neurologic lesion of the affected arm, known dementia or death before follow-up were excluded. A total of 68 patients with a minimum of 12 monthsʼ follow-up since the index surgery with implantation of the same type of RSA (Delta Xtend, Depuy-Synthes, Warsaw, IN, USA) were finally included.
Of the remaining 68 patients, follow-up was available for 51 patients (75%) at a mean of 18.2 months (range, 12.2–45.0 months); 37 patients were examined clinically and 14 patients by questionnaire with assessment of the same functional outcome protocol. There were 45 women and six men with a mean age of 73 years (range, 59–87 years) at the time of implantation. In 28 cases, arthroplasty was implanted primarily (Fig. 1), in 23 cases secondarily. The interval between the index surgery and the revision procedure was 14.0 months (1.6–45.0 months).

A 74-year-old female patient: right shoulder with severely displaced type Resch 3GL proximal humeral fracture with metaphyseal comminution (a, b), treated with primary reverse total shoulder arthroplasty with refixation of the tuberosities using cable and cerclage wires (c, d)
Secondary RSA was implanted for varying indications: failure of locked plating (n = 9; Fig. 2), decompensation of an anatomic hemiarthroplasty (n = 9; Fig. 3), or failure of locked nailing (n = 5). Prior to revision, humeral head necrosis was found in four patients and one patient had a stiff shoulder. A bone defect of the glenoid cavity due to screw perforation was observed in one case. Intraoperatively, there were positive tissue cultures for one patient; however, further revision was not needed.

An 89-year-old female patient: left shoulder with humeral head necrosis and collapse after locking plate fixation (a, b), treated with secondary reverse total shoulder arthroplasty (c)

A 72-year-old female patient: right shoulder with failure of hemiarthroplasty 6 months after implantation for a comminuted proximal humeral fracture (a, b) and secondary modular conversion to reverse total shoulder arthroplasty (c, d)
Surgery was always performed under general anesthesia with the patient in beach-chair position. The deltopectoral approach was used in all cases. In terms of surgical techniques, there were two periods: From January 2010 to December 2011, no routine tuberosity refixation was performed. In 2012 and 2013, tuberosity refixation was performed routinely with cable cerclages. In the case of secondary arthroplasty, the decision of whether to reattach the tuberosities or not depended on their existence and bone quality.
Clinical and radiologic assessment
All patients (n = 51) were assessed according to joint active range of motion, DASH, Constant–Murley Score (CMS), Subjective Shoulder Value (SSV), and Visual Analog Scale (VAS) for pain. All patients with clinical examination (n = 37) underwent radiologic assessment after 12 months with shoulder X‑rays in two planes (anteroposterior view and axillary view) to analyze tuberosity healing, heterotopic ossification, and inferior notching. Owing to the lack of consensus criteria in the literature for tuberosity consolidation in RSA, we considered an anatomic healing as visualization of the tuberosity in union with the humeral shaft [21]. The inferior notching of the scapula neck was graded according to the classification of Sirveaux et al. [22].
Statistical analysis
Data were organized in Excel (Version 14.5.4, Microsoft Corporation, Redmond, USA). Analyses were performed in SPSS (Version 21.0, IBM, Chicago, IL, USA). Normal distribution was determined by the Kolmogorov–Smirnov test. For comparison between groups, the unpaired Student t test, chi-square test, or nonparametric Mann–Whitney U test for continuous variables was used. A p-value of <0.05 was considered significant.
Results
The mean age- and gender-related CMS of all patients (n = 51) was 82.2 ± 34.2% (median 75.6%; raw CMS: mean 46.8 ± 19.6 points; range, 14–94 points, median 48 points). The active forward flexion averaged 106.1 ± 44° (range, 25–180°), the mean abduction was 100.2 ± 44.9° (range, 30–180), and the mean external rotation was 5.6 ± 7.8° (range, 0–40°). The overall SSV averaged 58.3 ± 22.2% (range, 10–95%), the mean DASH score was 41.2 ± 22.7 (range, 0–80.8), and VAS pain averaged 2.5 ± 2.3 (range, 0–7).
Radiographic results
The radiographic results of 37 patients demonstrated five prostheses (13.5%) with inferior notching of the scapular neck. On the basis of the Sirveaux classification [22], scapular notching was grade 1 in two patients and grade 2 in three patients. Heterotopic ossifications were found in 15 cases (40.5%). Tuberosity refixation had been performed in 14 of these 37 cases (37.8%), of whom two patients demonstrated anatomic consolidation (14.2%). The cable cerclage was broken in four of 14 cases (28.6%). In the other patients (n = 8), a resorption of the tuberosities was found (57.1%).
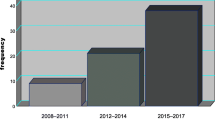
Ten complications occurred among nine of the 51 patients (17.6%) with follow-up data (Table 1). Prostheses that were implanted in the first years of our study period were affected by a higher complication rate (2010–2011: n = 8/29, 27.6%) than those that were implanted later (2012–2013: n = 2/22, 9.1%).
Primary vs. secondary arthroplasty
Overall, primary arthroplasty (n = 28) resulted in better clinical shoulder function compared with secondary arthroplasty (n = 23). We found a significantly better abduction, adduction, and forward flexion in patients with primary arthroplasty (Table 2). However, no significant difference was found between the external and internal rotation in primary and secondary RSA. Furthermore, we found no significant difference between the clinical outcome scores of primary and secondary RSA (Table 3).
More complications were observed after secondary (complication rate 8/23 = 34.8%) than after primary (complication rate 2/28 = 7.1%) RSA (p = 0.013). Furthermore, revision surgery had to be performed significantly more frequently following secondary (5/23 = 21.7% in 5 patients) than primary RSA (1/28 = 3.6% p = 0.045).
Discussion
The most important findings of this study were that primary RSA was associated with better clinical function and lower complication and revision rates than secondary RSA.
Several studies report on the functional results after primary RSA in PHF management. Klein et al. found a CMS of 67.9 in their study of 20 patients [11]. Bufquin et al. reported a CMS of 44 in their study of 43 patients [23], while in the study of Gallinet et al. comprising 19 patients the CMS was 53 [9].
Only few studies report on secondary RSA in fracture management. Cicak et al. found a CMS of 42 for 16 patients after failed open reduction and internal fixation (ORIF; [29]). In their study of 20 patients, Alentorn-Geli et al. reported a CMS of 26.6 [27], while Sebastia-Forcada et al. found a CMS of 22 after failed hemiarthroplasty in 6 patients [20].
In their study, Alentorn-Geli et al. compared secondary RSA (n = 20) with hemiarthroplasty (n = 12) for proximal humeral fracture sequelae after primary non-operative treatment [27]. The authors reported inferior functional results for secondary hemiarthroplasty with a gender- and age-related CMS of 26.6% after 39.6 months of follow-up. Dezfuli et al. compared results of RSA implanted as a revision procedure (n = 12 after failed hemiarthroplasty; n = 11 for failed fracture fixation; n = 13 after malunion or non-union) with primary RSA (n = 13; [28]). The authors found that primary RSA outperformed RSA as a revision procedure. The results of our study with larger groups of patients confirm their findings.
The complication rate of RSA for PHF is a major problem, with complication rates ranging from 0% [26, 27, 30, 31] to 68.4% [32].
Levy et al. reported a complication rate of 68.4% for secondary RSA [32]. Their results represent an early implantation period between 1999 and 2005. The complication rate may be reduced by senior surgeons [33, 34], and our results confirm this hypothesis of a learning curve. Prostheses that were implanted in the first year of our study period were linked toa higher complication rate (2010–2011: 27.6%) than those that were implanted later (2012–2013: 9.1%).
Recent studies report lower complication rates compared with earlier studies. Sebastia-Forcada et al. [20] found good results for pain reduction, clinical function, and revision rates in RSA for PHF with low complication rates (6.5%). Dezfuli et al. [28] reported a complication rate of 12%. In the literature, the most common complications are postoperative dislocations, nerve injuries, and infections. Farshad et al. [35] reported that dislocation with instability, hematoma, infection, and glenoidal complications were often an indication for revision surgery. The revision rate in the literature varies from 0% to 31.0% [32]. In our study, six surgical revisions were necessary (revision rate: 11.8%). Like Farshad et al., our revisions were indicated for postoperative dislocation, infection, hematoma, and periprosthetic fracture.
Several authors reported that RSA is favorable to ORIF or hemiarthroplasty for PHF in the elderly [5, 12, 13]. In view of the favorable outcomes of primary RSA versus RSA as a revision procedure for failed fracture fixation or failed hemiarthroplasty in the elderly, primary RSA should be considered when surgical treatment of PHF is indicated in elderly patients.
Limitations
The limitations of our study include the fact that it was non-randomized and retrospective with a minimum follow-up of 12 months. Further research is needed to better quantify the results and differences and especially the long-term results after RSA. The influence of scapular notching and deltoid muscle insufficiency, as seen in RSA for rotator cuff deficiency, may affect the long-term outcome.
Although our study is based on a larger sample size than other studies [9, 20, 21, 24, 28, 31, 32], it may be underpowered to detect statistically significant differences for clinical outcome scores regarding primary versus secondary arthroplasty.
Practical conclusion
-
Primary reverse total shoulder arthroplasty (RSA) for displaced proximal humeral fractures (PHF) in the elderly is associated with better clinical function and lower complication and revision rates than secondary RSA.
-
Predictive parameters for failure of humeral head-preserving fracture fixation and anatomic humeral head replacement should be carefully evaluated.
-
When in doubt, primary RSA should be considered if surgical treatment of PHF is indicated in elderly patients.
References
Burkhart KJ, Dietz SO, Bastian L, Thelen U, Hoffmann R, Muller LP (2013) The treatment of proximal humeral fracture in adults. Dtsch Arztebl Int 110:591–597
Roux A, Decroocq L, El Batti S, Bonnevialle N, Moineau G, Trojani C et al (2012) Epidemiology of proximal humerus fractures managed in a trauma center. Orthop Traumatol Surg Res 98:715–719
Lill H, Ellwein A, Katthagen C, Voigt C (2012) Osteoporotic fractures of the proximal humerus. Chirurg 83:858–865
Katthagen J, Grabowski S, Huber M, Jensen G, Voigt C, Lill H (2016) Epidemiology and treatment reality of proximal humeral fractures at a level‑1 trauma center. Obere Extremität 11:112–118
Gradl G, Pape HC, Tingart M, Arbab D (2014) Fractures of the proximal humerus in the elderly: Osteosynthesis versus joint replacement. Orthopade 43:339–346
Nho SJ, Brophy RH, Barker JU, Cornell CN, MacGillivray JD (2007) Management of proximal humeral fractures based on current literature. J Bone Joint Surg Am 89(Suppl 3):44–58
Loew M, Heitkemper S, Parsch D, Schneider S, Rickert M (2006) Influence of the design of the prosthesis on the outcome after hemiarthroplasty of the shoulder in displaced fractures of the head of the humerus. J Bone Joint Surg Br 88:345–350
Reuther F, Muhlhausler B, Wahl D, Nijs S (2010) Functional outcome of shoulder hemiarthroplasty for fractures: A multicentre analysis. Injury 41:606–612
Gallinet D, Clappaz P, Garbuio P, Tropet Y, Obert L (2009) Three or four parts complex proximal humerus fractures: hemiarthroplasty versus reverse prosthesis: a comparative study of 40 cases. Orthop Traumatol Surg Res 95:48–55
Schliemann B, Theisen C, Barz L, Weimann A, Raschke M (2016) Reosteosynthese vs. Prothese nach fehlgeschlagener Humeruskopfosteosynthese. Obere Extremität 11(4):239–247
Klein M, Juschka M, Hinkenjann B, Scherger B, Ostermann PA (2008) Treatment of comminuted fractures of the proximal humerus in elderly patients with the delta III reverse shoulder prosthesis. J Orthop Trauma 22:698–704
Anakwenze OA, Zoller S, Ahmad CS, Levine WN (2014) Reverse shoulder arthroplasty for acute proximal humerus fractures: a systematic review. J Shoulder Elbow Surg 23:e73–80
Wang J, Zhu Y, Zhang F, Chen W, Tian Y, Zhang Y (2016) Meta-analysis suggests that reverse shoulder arthroplasty in proximal humerus fractures is a better option than hemiarthroplasty in the elderly. Int Orthop 40:531–539
Shukla DR, McAnany S, Kim J, Overley S, Parsons BO (2016) Hemiarthroplasty versus reverse shoulder arthroplasty for treatment of proximal humeral fractures: a meta-analysis. J Shoulder Elbow Surg 25:330–340
Ferrel JR, Trinh TQ, Fischer RA (2015) Reverse total shoulder arthroplasty versus hemiarthroplasty for proximal humeral fractures: a systematic review. J Orthop Trauma 29:60–68
Zumstein MA, Pinedo M, Old J, Boileau P (2011) Problems, complications, reoperations, and revisions in reverse total shoulder arthroplasty: a systematic review. J Shoulder Elbow Surg 20:146–157
Kirchhoff C, Biberthaler P (2013) Indication for primary fracture prosthesis of the shoulder. Unfallchirurg 116:1015–1029
Brorson S, Rasmussen JV, Olsen BS, Frich LH, Jensen SL, Hrobjartsson A (2013) Reverse shoulder arthroplasty in acute fractures of the proximal humerus: a systematic review. Int J Shoulder Surg 7:70–78
Namdari S, Horneff JG, Baldwin K (2013) Comparison of hemiarthroplasty and reverse arthroplasty for treatment of proximal humeral fractures: a systematic review. J Bone Joint Surg Am 95:1701–1708
Sebastia-Forcada E, Cebrian-Gomez R, Lizaur-Utrilla A, Gil-Guillen V (2014) Reverse shoulder arthroplasty versus hemiarthroplasty for acute proximal humeral fractures. A blinded, randomized, controlled, prospective study. J Shoulder Elbow Surg 23:1419–1426
Gallinet D, Adam A, Gasse N, Rochet S, Obert L (2013) Improvement in shoulder rotation in complex shoulder fractures treated by reverse shoulder arthroplasty. J Shoulder Elbow Surg 22:38–44
Sirveaux F, Favard L, Oudet D, Huquet D, Walch G, Mole D (2004) Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff. Results of a multicentre study of 80 shoulders. J Bone Joint Surg Br 86:388–395
Bufquin T, Hersan A, Hubert L, Massin P (2007) Reverse shoulder arthroplasty for the treatment of three- and four-part fractures of the proximal humerus in the elderly: a prospective review of 43 cases with a short-term follow-up. J Bone Joint Surg Br 89:516–520
Levy JC, Badman B (2011) Reverse shoulder prosthesis for acute four-part fracture: tuberosity fixation using a horseshoe graft. J Orthop Trauma 25:318–324
Cuff DJ, Pupello DR (2013) Comparison of hemiarthroplasty and reverse shoulder arthroplasty for the treatment of proximal humeral fractures in elderly patients. J Bone Joint Surg Am 95:2050–2055
Valenti P, Katz D, Kilinc A, Elkholti K, Gasiunas V (2012) Mid-term outcome of reverse shoulder prostheses in complex proximal humeral fractures. Acta Orthop Belg 78:442–449
Alentorn-Geli E, Guirro P, Santana F, Torrens C (2014) Treatment of fracture sequelae of the proximal humerus: comparison of hemiarthroplasty and reverse total shoulder arthroplasty. Arch Orthop Trauma Surg 134:1545–1550
Dezfuli B, King JJ, Farmer KW, Struk AM, Wright TW (2016) Outcomes of reverse total shoulder arthroplasty as primary versus revision procedure for proximal humerus fractures. J Shoulder Elbow Surg 25:1133–1137
Cicak N, Klobucar H, Medancic N (2015) Reverse shoulder arthroplasty in acute fractures provides better results than in revision procedures for fracture sequelae. Int Orthop 39:343–348
Ockert B, Biermann N, Haasters F, Mutschler W, Braunstein V (2013) Reverse shoulder arthroplasty for primary fracture treatment. Displaced three and four part fractures of the proximal humerus in the elderly patient. Unfallchirurg 116:684–690
Young SW, Segal BS, Turner PC, Poon PC (2010) Comparison of functional outcomes of reverse shoulder arthroplasty versus hemiarthroplasty in the primary treatment of acute proximal humerus fracture. ANZ J Surg 80:789–793
Levy JC, Virani N, Pupello D, Frankle M (2007) Use of the reverse shoulder prosthesis for the treatment of failed hemiarthroplasty in patients with glenohumeral arthritis and rotator cuff deficiency. J Bone Joint Surg Br 89:189–195
Walch G, Bacle G, Ladermann A, Nove-Josserand L, Smithers CJ (2012) Do the indications, results, and complications of reverse shoulder arthroplasty change with surgeon’s experience? J Shoulder Elbow Surg 21:1470–1477
Kempton LB, Ankerson E, Wiater JM (2011) A complication-based learning curve from 200 reverse shoulder arthroplasties. Clin Orthop Relat Res 469:2496–2504
Farshad M, Grogli M, Catanzaro S, Gerber C (2012) Revision of reversed total shoulder arthroplasty. Indications and outcome. BMC Musculoskelet Disord 13:160
Funding
Open Access funding provided by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. C. Katthagen, E. Hesse, H. Lill, B. Schliemann, A. Ellwein, M.J. Raschke and J. Imrecke declare that they have no competing interests.
The study protocol was approved by the local ethics committee of the Medizinische Hochschule Hannover (1840–2013) and complied with the principles of the Declaration of Helsinki.
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Katthagen, J.C., Hesse, E., Lill, H. et al. Outcomes and revision rates of primary vs. secondary reverse total shoulder arthroplasty for proximal humeral fractures. Obere Extremität 15, 35–41 (2020). https://doi.org/10.1007/s11678-020-00559-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11678-020-00559-z