
Abstract
To investigate the association between the Emergency Medical Service dispatcher’s initial stroke triage and prehospital stroke management, primary admission to hospitals offering revascularization treatment, prehospital time delay, and rate of acute revascularization. In an observational cohort study, patients with acute ischemic stroke (AIS) in Denmark (2017–2018) were included if the emergency call to the Emergency Medical Dispatch Center (EMDC) was made within three hours after symptom onset. Among 3546 included AIS patients, the EMS dispatcher identified 74.6% (95% confidence interval (CI) 73.1–76.0) correctly as stroke. EMS dispatcher stroke recognition was associated with a higher rate of primary admission to a hospital offering revascularization treatment (85.8 versus 74.5%); producing an adjusted risk difference (RD) of 11.1% (95% CI 7.8; 14.3) and a higher rate of revascularization treatment (49.6 versus 41.6%) with an adjusted RD of 8.4% (95% CI 4.6; 12.2). We adjusted for sex, age, previous stroke or transient ischemic attack, and stroke severity. EMDC stroke recognition was associated with shorter prehospital delay. For all AIS patients, the adjusted difference was − 33.2 min (95% CI − 44.4; − 22.0). Among patients receiving acute revascularization treatment (n = 1687), the adjusted difference was -12.6 min (95% CI − 18.9; − 6.3). Stroke recognition by the EMS dispatcher was associated with a higher probability of primary admission to a hospital offering acute stroke treatment, and subsequently with a higher rate of acute revascularization treatment, and with an overall reduction in prehospital delay.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Stroke is a time-critical condition requiring urgent treatment due to time-related, irreversible loss of brain cells and subsequent loss of physical and cognitive functions and increased mortality [1, 2]. Hence, a shorter treatment delay directly improves clinical outcomes [3,4,5,6,7,8,9,10,11,12], and the effect of reducing treatment delay may be observed continuously as the delay diminishes [13,14,15,16].
Activation of the Emergency Medical Service (EMS) by an emergency call to the Emergency Medical Dispatch Center (EMDC) is associated with a reduced prehospital delay, earlier emergency department (ED) arrival, and faster treatment than self-admission, referral from other medical facilities, and admission organized by general practitioners [17,18,19,20,21,22]. In the EMS system, a stroke may be identified either by the EMS dispatcher at the EMDC during the emergency call or by the EMS provider attending the patient on scene. The EMS dispatchers’ stroke identification directly affects treatment delay because the dispatchers determine the urgency level set for ambulances. A high urgency level to individuals with suspected stroke is associated with a reduced transport time [23] and an increased rate of thrombolysis compared with less urgent responses [24]. Patients whom the EMS dispatcher suspects suffer from a stroke also have a higher probability of being assessed prehospitally with a stroke screening tool than patients not suspected of stroke [25].
EMS dispatcher stroke recognition rates vary and are generally low with sensitivities ranging from 37 to 83%, and positive predictive values fall in the 30–68% range [26,27,28,29,30]. In Denmark, one-third of all stroke cases have been shown to be unrecognized by EMS dispatchers [27] which equals the performance in other countries [25, 31,32,33]. The use of a symptom-based stroke scale by an EMDC is associated with higher recognition of stroke/TIA [27, 33,34,35]. The use of a stroke assessment tool by the EMS dispatchers is recommended in the 2019 guideline from the American Stroke Association [36].
Studies focusing on EMS dispatcher stroke identification among potential candidates for acute revascularizing treatment are few [26, 33]. Associations between EMDC stroke triage and stroke management have not previously been isolated to a stroke subtype where acute treatment is well established or to a group of patients who from a timely perspective would all be considered candidates for acute stroke treatment at the time EMDC contact [26].
We aimed to evaluate the association between EMDC stroke triage and prehospital stroke management in patients with acute ischemic stroke (AIS) who contacted the EMDC within three hours of symptom debut. We compared patients with recognized stroke and patients with unrecognized stroke (EMDC stroke triage) with regards to primary admission to hospitals offering revascularization treatment, prehospital delay (time from emergency call to arrival at hospital), and the use of intravenous (i.v.) thrombolysis and/or endovascular treatment (EVT).
Methods
Study design and setting
This was a national observational cohort study including stroke patients (AIS) from all five health regions in Denmark. Patients with a final stroke diagnosis (AIS) were retrospectively identified in data from Danish healthcare registers in 2017 and 2018.
The emergency medical service (EMS)
In Denmark, healthcare including prehospital care is tax-financed and free for all citizens. Denmark is divided into five regions; each governed one EMDC and ambulance services [37]. In the study period, the ambulance services were managed partly by private contractors and partly by the regions. Extensive quality requirements for all ambulance services were described and controlled by the EMS authority of each region.
Ambulance personnel
All ambulances were manned with two EMS providers, counting at least one paramedic or an emergency medical technician intermediate (EMT-I). EMS providers did not use a symptom-based stroke assessment tool except in one region where a modified Cincinnati Prehospital Stroke Scale was being implemented during 2018 as part of a clinical study.
Stroke care system
In Denmark, treatment with i.v. thrombolysis has been centralized, producing an improved overall quality of care [38]. Hence, i.v. thrombolysis was not offered at all hospitals with an ED. In the study period, 11 hospitals offered acute stroke admission including i.v. thrombolysis. Among these 11 hospitals, three did not have a general ED, and acute admission was offered only to patients with suspicion of stroke. Furthermore, 14 hospitals had an ED but no acute stroke admission.
When stroke was suspected, either guided by the prenotification from the EMDC or by the patient’s clinical presentation, a telephone conference call from the EMS provider to a stroke neurologist was conducted; and it was decided whether the patient would be admitted directly to a stroke center or a general ED. Patients without suspicion of stroke would be admitted at the nearest ED. Because of the organization of the Danish hospitals, this nearest ED would not necessarily be located at a hospital with a stroke center with the capacity to initiate acute revascularization treatment. Hence, patients for whom a stroke was suspected, could experience a slightly longer prehospital transport to ensure a direct admission to nearest stroke center to offer immediate stroke diagnostics and treatment [39]. In the study period, EVT was offered at four Comprehensive Stroke Centers, with the relative timeline for most treatments of six hours. All Comprehensive Stroke Centers also performed i.v. thrombolysis.
Criteria-based dispatch reference work used in the EMDC and stroke triage
The EMDC was operated by EMS dispatchers who dispatched all emergency responses. Dispatch or triage was guided by criteria-based dispatch reference work (Danish Index) divided into main groups of symptoms (e.g., trauma, blocked airway, bleeding, burns, chest pain, etc.) specifying the level of urgency (A–E) [40]. Symptoms related to stroke and transient ischemic attack (TIA) produced a positive EMDC stroke triage. Symptoms of stroke triggered the most urgent level of response (level A); stroke symptoms that were considered to have resolved completely, interpreted as TIA, triggered a less urgent response level (level B) [41].
Level-A responses were dispatched within minutes; level-B responses, up to 30 min from the time of triage; level-C responses, within 1 or 2 h (C60 or C120); level D or E responses, within a varying period and when no treatment was needed. If a stroke was missed by the EMS dispatcher, the emergency response was dispatched from a non-stroke-associated symptom group (describing a non-stroke symptom) in the Danish Index, introducing the risk of a lesser urgent response level (non-A responses). Besides the urgency level, the criteria-based dispatch system provided a short text that served as a prenotification of the ambulance personnel.
Participants
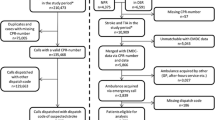
The study included all stroke patients diagnosed with AIS in Denmark in 2017 and 2018 for whom the initial healthcare contact was an emergency call made within three hours after symptom debut (Fig. 1). The three-hour time limit was chosen as all patients within this prehospital time window were potentially eligible for acute reperfusion treatment. The three-hour limit was chosen to allow for a realistic transport time and in-hospital evaluation before revascularization within the 4.5-h limit. Stroke diagnoses were established by stroke neurologists according to the World Health Organization stroke definition and registered in the Danish Stroke Registry (DSR).

Patient flow chart
DI danish index (determine EMDC triage), EMDC emergency medical dispatch center, recognized/unrecognized refers to the initial identification by the emergence medical service (EMS) dispatcher
Data sources
The DSR is a national clinical quality register holding information about patients diagnosed with stroke or TIA. The DSR was used to identify patients in 2017 and 2018. A sensitivity > 90% of all acute strokes has been reported for the DSR [42]. Information in the database covered final diagnosis, any acute revascularization treatment, patients’ basic characteristics, and their comorbidities, and the National Institute of Health Stroke Scale (NIHSS) for patients receiving acute stroke treatment.
Prehospital data from 2017 to 2018 were stored in databases linked to the computer-aided dispatch systems used by the individual EMDCs. The databases contained time stamps (recordings of the exact time at which various actions had occurred in the prehospital management (e.g., the initial call to the EMDC, ambulance dispatch, ambulance arrival at and departure from the location, and arrival at the hospital)). The databases also contained information about any chosen chapter and subheading in the Danish Index, indicating what symptom/description the EMS dispatcher found to be most fitting and describing the assigned level of urgency [40].
Exposure based on EMDC stroke triage
Our study population was divided into two groups depending on whether a stroke was recognized by the EMS dispatcher or not. All patients included in the study were subsequently diagnosed with stroke according to the guidelines.
Outcomes
The outcomes were: initial admission at a hospital offering i.v. thrombolysis or EVT, the use of i.v. thrombolysis or EVT, and prehospital delay.
Total prehospital delay accounted for all delays from the initial EMDC emergency call to a stroke admission including all subsegments in the prehospital management. Subsegments of total prehospital delay were: EMDC delay (time from EMDC call to ambulance arrival at the patient’s location/the scene); on-scene time (time from arrival to and departure from the scene); transport to hospital (time from scene departure to arrival at first hospital); and door-in-door-out (time from arrival to and departure from hospital) for patients with temporary admissions before transferal to a stroke admission including i.v. thrombolysis or EVT as indicated.
To calculate the true positive rate (sensitivity) of EMDC stroke triage, we used the diagnosis registered in the DSR as outcome (denominator).
Covariates
Sex, age at admission, previous stroke or TIA, and response level (A and B–as C and D was few) were used for the adjusted analysis. Stroke severity measured by the NIHSS (assessed at admission) was additionally used for adjustments for patients receiving acute stroke treatment—the only patients where NIHSS was persistently registered.
Statistics
Descriptive statistics on basic characteristics, primary admission to hospitals offering revascularization treatment, response levels, and stroke severity (for patients receiving acute stroke treatment) were performed comparing recognized with unrecognized stroke groups. The number of missing variables was low, and imputation was not used. Numbers were presented for all calculations. Differences in stroke management were calculated both as a risk difference (RD) and relative risk (RR) using linear regression and Poisson regression, respectively, both with robust variance and inverse probability of treatment weights (IPTW) for all adjusted analyses.
We calculated the true positive rate (sensitivity) for EMDC stroke triage to identify acute ischemic stroke.
To calculate prehospital delays, we used linear regression with robust variance and IPTW for adjusted analyses. Balanced diagnostics were conducted using the threshold criteria given by Zhang et al. [43]. To calculate a total association, we adjusted for sex, age, previous stroke or TIA, and stroke severity measured by the NIHSS. The NIHSS was assessed at admission before treatment and only for patients receiving either i.v. thrombolysis or EVT. Additionally, to calculate a direct association, the response level A was used for adjustment to show any residual association between EMDC triage and prehospital delay beyond the higher frequency of level-B responses dispatched in the unrecognized stroke group.
All data were analyzed using Stata 15 (StataCorp. College Station, TX: StataCorp LLC.).
Results
From 2017 to 2018, 8,261 patients had a verified stroke for which an emergency call to the EMDC initiated the healthcare contact (Fig. 1). We excluded 142 patients because of incomplete EMDC stroke triage, 1,172 patients with intracranial hemorrhage, 773 patients with missing data on symptom onset, and 2,628 patients with a contact with the EMDC more than three hours after symptom onset. Patients with AIS and an emergency call to the EMDC within three hours after symptom onset totaled 3546, constituting our study population (Fig. 1). The true positive rate of EMDC stroke triage (sensitivity) for AIS and a symptom duration ≤ 3 h was 74.6% (95% CI 73.1–76.0) – hence, 2645 patients had a stroke that was recognized by the EMS dispatcher and 901 patients had an unrecognized stroke. Recognized and unrecognized only refers to the initial contact with the EMDC – all patients were eventually diagnosed with stroke.
Patients with stroke recognized and unrecognized by the EMS dispatcher were comparable regarding their basic characteristics and comorbidity (Table 1). In addition, the median NIHSS was comparable between the EMDC triage groups among patients treated with i.v. thrombolysis and/or thrombectomy (Table 1). On a subgroup level, median NIHSS differed significantly among EVT-treated patients for recognized versus unrecognized stroke (14 vs. 17) (data not shown).
In the total study population (n = 3546), the proportion of patients with an initial admission to a hospital offering acute stroke treatment including i.v. thrombolysis and/or EVT was higher for patients with recognized stroke compared with unrecognized stroke; 85.8% (95% CI 84.4–87.1) versus 74.5% (95% CI 71.5–77.3) yielding an adjusted RD of 11.1% (95% CI 7.8; 14.3) (Table 2). Subsequently, a higher rate of revascularization treatment was seen in the group with recognized stroke; 49.6% (95% CI 47.7; 51.5) versus 41.6% (95% CI 38.4; 44.9) with an adjusted RD of 8.4% (95% CI 4.6; 12.2). For i.v. thrombolysis alone, an even greater difference was seen in favor of recognized stroke; 46.7% (95% CI 44.8–48.7) versus 37.7% (95% CI 34.5–41.0) with an adjusted RD of 9.5% (95% CI 5.7; 13.2) (Table 2). However, the proportion of patients receiving EVT did not differ between the two groups; 10.6% (95% CI 9.4; 11.8) in the recognized group and 10.5% (95% CI 8.6; 12.7) in the unrecognized group (Table 2).
Of the 1,565 patients treated with i.v. thrombolysis, only 66 patients received treatment after inter-hospital transfer. A need for inter-hospital transfer applied to more admissions in the unrecognized stroke group compared with the recognized stroke group; 8.6% (95% CI 5.8–12.1) versus 3.0% (95% CI 2.1–4.1) (Table 2). This higher rate of inter-hospital transfers among patients with unrecognized stroke was seen although these patients arrived later at a hospital not offering i.v. thrombolysis (median 118.0 versus 79.4 min). A need for interhospital transfer before EVT also applied to more admission in the unrecognized stroke group, but the difference was not statistically significant (Table 2).
Patients with stroke recognized by the EMS dispatcher almost exclusively received a level-A response (99.2%); patients with an unrecognized stroke received a level-A response in 69.0%, a level-B response in 30.4%, and a level-C or D-response in 0.6% of all dispatches (Table 2). The same magnitude of difference in receiving a level-A response was seen among patients who received i.v. thrombolysis and/or EVT with an adjusted RD of 24.7% (95% CI 19.6; 29.7) (Table 2).
For all patients (n = 3546), the total association (difference in means) between EMDC stroke triage and prehospital delay was − 33.2 min (95% CI − 44.4; − 22.0) in favor of recognized stroke. The total association was adjusted for sex, age at admission, and previous stroke and TIA (Table 3).
Among patients who received acute revascularizing treatment (n = 1,687), the EMDC stroke recognition was still associated with reduced prehospital delay (Table 3). The total association was -12.6 min (95% CI − 18.9; − 6.3) and the direct association was − 9.4 min (95% CI − 15.4; − 3.5). The analyses were adjusted for sex, age at admission, previous stroke and TIA and NIHSS and the direct association was also adjusted for ambulance level of urgency (Table 3).
All sub-elements of the prehospital delay contributed to the entire difference in prehospital delay, except for “transport to hospital” (time from departure from scene to arrival at hospital) (Table 4). Additional adjustments for response level (the direct association) removed the difference in delay from emergency call to arrival at the scene (EMDC delay) indicating that the delay was driven by the response level only (Table 4).
The association between the response level and total prehospital delay was − 44.8 min (95% CI − 66.9; − 22.6); and EMDC delay was − 10.3 min (95% CI − 11.9; − 8.6) – using response level B as reference (Table 3).
Discussion
In this national cohort study, we found that EMS dispatchers identified AIS with a high sensitivity when symptom onset had occurred within three hours of the patient contacting the EMDC. AIS identified by the EMS dispatchers was associated with both a greater probability of admission to a hospital offering revascularization treatment (85.8% versus 74.5%) and subsequently a greater rate of acute revascularization treatment (49.6% versus 41.6%).
EMS dispatcher stroke recognition was associated with a substantial reduction in prehospital delay compared with non-recognition, both in the overall study population (− 33.2 min) and in the time-critical patient group treated with i.v. thrombolysis and/or EVT (− 12.6 min). A direct association persisted with reduced delay for recognized stroke for all patients (− 26.8 min) and patients treated with i.v. thrombolysis and/or EVT (− 9.4 min) even when adjusting for the relatively frequent use of response level-B in the unrecognized stroke group.
Every minute counts when patients await thrombolysis [44]. Therefore, decreasing delay from symptom onset to thrombolysis remains the main focus in stroke management. We found a substantial reduction in prehospital delay for patients with recognized stroke even when restricting the focus to patients with AIS potentially eligible for acute revascularization within 4.5 h.
Reduced prehospital delay for stroke recognized by EMS dispatchers was also shown in a study by Caceres et al. (49.8 reduced to 41.8 min) [23]. They defined patients with stroke as those patients in whom the EMS providers suspected stroke in the prehospital environment. The study thus lacked a gold standard outcome measure. EMS dispatchers’ and EMS providers’ performance ability to identify patients with stroke is known to be similar with sensitivities of up to 60–70% [45], and the delay reductions reported by Caceres et al. therefore apply to identified patients with a mix of diagnoses (including stroke mimics).
Unlike us, Oostema et al. found no difference in total prehospital delay between EMDC stroke triage groups [25]. The frequency of the highest level of urgency (level A) was in favor of recognized stroke (87.3 versus 72.6%), like in our study, whereas the rate of thrombolysis was not. The discrepancy regarding prehospital delay and thrombolysis rate found in our study versus the findings in the study by Oostema et al. may possibly be explained by a difference in study setups. Oostema et al. included patients from only two centers, both offering thrombolysis. The risk of being admitted to a hospital without thrombolysis therefore did not exist in their study, and those admissions contributed to the lower rate of thrombolysis and the prehospital delay in our study. Disregarding, that no difference was found in overall prehospital delay, the on-scene time differed significantly and reached the same level as reported by us [25]. A difference in on-scene-time that have also been shown by Abbas et al. and Heemskerk et al. favoring recognized stroke [30, 46].
The additional on-scene time for unrecognized stroke found in our study did not depend on the response level and could be due to lacking EMS provider prenotification. If the EMS dispatcher does not recognize a stroke case, EMS providers may have to spend more time at the scene, evaluating the patient more extensively, before a suspicion of a stroke may come to mind.
Prehospital stroke identification is a complex process involving both the EMS dispatcher and the EMS providers. Any prehospital delay due to inability to recognize the condition is hence influenced by the performance of both groups. On the other hand, EMDC delay is not influenced by the EMS providers because it occurs before they arrive. The reduced EMDC delay for the recognized stroke group was mediated by the response level; hence, the response-level-adjusted analysis (direct association) showed no difference in EMDC delay between the groups (Table 4). This corresponds well with the standard operating procedure that all response levels other than level A may be dispatched with an allowed delay. It also demonstrates that a level-A response is equally fast, disregarding the type of indexation (positive or negative stroke triage). Response level B almost exclusively occurred in the unrecognized stroke group. Comparing response level B with response level A revealed a more than twofold increased EMDC delay, and an additional prehospital delay beyond this initial delay.
We reported the performance of EMDC triage and its association with stroke management in a group of patients with AIS where acute stroke treatment is well established and in a time-restricted manner so that all included patients could reach a hospital offering i.v. thrombolysis and/or EVT despite their initial geographical location—a group of patients that has not been reported on previously [26].
Only 66 of the patients with an EMDC contact occurring more than three hours after their initial call received i.v. thrombolysis in contrast to 1,565 patients in the group in which the initial healthcare contact occurred within the three-hour limit. This emphasizes that the time limit used in this study very precisely targets patients eligible for acute stroke treatment. By including patients from all geographical locations in Denmark and from two consecutive years based on a well-validated quality data source (the Danish Stroke Register), we believe that our results are generalizable to other stroke care systems – i.e., that our results have a high external validity.
As a limitation, a risk exists that we have underestimated the association between EMDC stroke triage and prehospital delay and acute revascularization treatment. A patient admitted to an ED, without acute stroke admission, due to a missing stroke identification may have lost the time for reperfusion therapy due to a late stroke identification. In that case, the patient would probably have remained at the first hospital to which they were admitted without inter-hospital transfer because acute treatment was considered timewise out of reach. In our study setup, this group would not contribute to measurable delay. For that reason, the results regarding prehospital delays must be considered in conjunction with the overall rate of i.v. thrombolysis associated with EMDC stroke triage (46.7% versus 37.7%) as a substantial group of patients with unrecognized stroke received no acute treatment. The importance of initial correct admission for receiving i.v. thrombolysis is illustrated by the fact that only a few patients (66 of 603) received i.v. thrombolysis after inter-hospital transfer. Despite having EDs without i.v. thrombolysis in Denmark, 19% of all patients with acute ischemic stroke (AIS) were treated with i.v. thrombolysis within the 4.5-h time limit in 2017 [47]; 22%, in 2018 [48]. Treatment with EVT for large-vessel occlusion was performed in 4.1% in 2017 [47]; 6.0%, in 2018 [48].
Another limitation to the study is a risk of residual unmeasured confounding because the prehospital stroke management consists of several steps of which we have only focused on the initial emergency call to the EMDC. A difference between the EMDC stroke triage groups could exist with unrecognized patients having an atypical presentation both at the initial emergency call and in later management. However, based on the available data, the groups seem to be fairy comparable (Table 1) where the small difference in previous stroke or TIA have been statistically balanced by the IPTW.
Conclusion
In summary, among a group of AIS patients all of whom had a timely, relevant contact to healthcare, a stroke recognized by the EMS dispatcher was associated with a reduced prehospital delay, a higher chance of primary admission to a hospital offering acute stroke treatment, and subsequently a higher chance of receiving acute revascularization treatment. Even among patients reaching acute stroke treatment in time, the group of patients with stroke recognized by EMDC experienced a substantial and clinically relevant reduced prehospital delay.
A focus on EMS dispatcher stroke recognition may reduce prehospital delay further.
Data availability statement
The datasets are available through the corresponding author upon reasonable request and permissions according to Danish legislation.
References
Saver JL (2006) Time is brain–quantified. Stroke (1970) 37(1):263–266
Wardlaw JM, Murray V, Berge E, del Zoppo GJ (2014) 2014 Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 7:000213
Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ et al (2015) A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 372(1):11–20
Froehler MT, Saver JL, Zaidat OO, Jahan R, Aziz-Sultan MA, Klucznik RP et al (2017) Interhospital transfer before thrombectomy is associated with delayed treatment and worse outcome in the STRATIS registry (Systematic evaluation of patients treated with neurothrombectomy devices for acute ischemic stroke). Circulation 136(24):2311–2321
Mohamad NF, Hastrup S, Rasmussen M, Andersen MS, Johnsen SP, Andersen G et al (2016) Bypassing primary stroke centre reduces delay and improves outcomes for patients with large vessel occlusion. Eur Stroke J 1(2):85–92
Sablot D, Gaillard N, Smadja P, Bonnec JM, Bonafe A (2017) Thrombectomy accessibility after transfer from a primary stroke center: Analysis of a three-year prospective registry. Int J Stroke 12(5):519–523
Prabhakaran S, Ward E, John S, Lopes DK, Chen M, Temes RE et al (2011) Transfer delay is a major factor limiting the use of intra-arterial treatment in acute ischemic stroke. Stroke 42(6):1626–1630
Kim JT (2017) Treatment with tissue plasminogen activator in the golden hour and the shape of the 4.5-hour time-benefit curve in the national united states get with the guidelines-stroke population. Circulation (New York, NY) 135(2):128–139
Sheth SA (2015) Time to endovascular reperfusion and degree of disability in acute stroke. Ann Neurol 78(4):584–593
Saver JL (2016) Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: a meta-analysis. JAMA J Am Med Assoc 316(12):1279–1288
Lees KR (2010) Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet (British edition) 375(9727):1695–1703
Emberson J, Lees KR, Lyden P, Blackwell L, Albers G, Bluhmki E et al (2014) Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet (London, England) 384(9958):1929–1935
Tsivgoulis G, Katsanos AH, Kadlecová P, Czlonkowska A, Kobayashi A, Brozman M et al (2017) Intravenous thrombolysis for ischemic stroke in the golden hour: propensity-matched analysis from the SITS-EAST registry. J Neurol 264(5):912–920
Advani R, Naess H, Kurz MW (2017) The golden hour of acute ischemic stroke. Scand J Trauma Resusc Emerg Med 25(1):54
Ebinger M, Kunz A, Wendt M, Rozanski M, Winter B, Waldschmidt C et al (2015) Effects of golden hour thrombolysis: a Prehospital Acute Neurological Treatment and Optimization of Medical Care in Stroke (PHANTOM-S) substudy. JAMA Neurol 72(1):25–30
Tsivgoulis G, Geisler F, Katsanos AH, Kõrv J, Kunz A, Mikulik R et al (2018) Ultraearly intravenous thrombolysis for acute ischemic stroke in mobile stroke unit and hospital settings. Stroke 49(8):1996–1999
García Ruiz R, Silva Fernández J, García Ruiz RM, Recio Bermejo M, Arias Arias Á, Del Saz SP et al (2018) Response to symptoms and prehospital delay in stroke patients is it time to reconsider stroke awareness campaigns? J Stroke Cereb Dis. 27(3):625–632
Nagao Y, Nakajima M, Inatomi Y, Ito Y, Kouzaki Y, Wada K et al (2020) Pre-hospital delay in patients with acute ischemic stroke in a multicenter stroke registry: K-PLUS. J Stroke Cereb Dis 29(11):105284
Pulvers JN, Watson JDG (2017) If time is brain where is the improvement in prehospital time after stroke? Front Neurol 8:617
Fladt J, Meier N, Thilemann S, Polymeris A, Traenka C, Seiffge DJ et al (2019) Reasons for prehospital delay in acute ischemic stroke. J Am Heart Assoc 8(20):e013101
Laurent E, Bonnaud I, Gaudron M, Lahondère A, Godillon L, Vannier S et al (2022) Factors associated with delayed revascularization in patients with ischemic stroke: a prospective study in one French region. Eur J Emerg Med 29(1):56–62
Duvekot MHC, Kerkhoff H, Venema E, Bos H, Smeekes D, Buijck BI et al (2022) Medical attention seeking by suspected stroke patients: Emergency medical services or general practitioner? Clin Neurol Neurosurg 218:107297
Caceres JA, Adil MM, Jadhav V, Chaudhry SA, Pawar S, Rodriguez GJ et al (2013) Diagnosis of stroke by emergency medical dispatchers and its impact on the prehospital care of patients. J Stroke Cereb Dis 22(8):e610–e614
Berglund A (2012) Higher prehospital priority level of stroke improves thrombolysis frequency and time to stroke unit: the Hyper Acute Stroke Alarm (HASTA) study. Stroke (1970) 43(10):2666–2670
Oostema JA, Chassee T, Reeves M (2018) Emergency dispatcher stroke recognition: associations with downstream care. Prehospital Emerg Care Off J Nat Assoc EMS Phys Nat Assoc State EMS Dir 22(4):466–471
Oostema JA, Carle T, Talia N, Reeves M (2016) Dispatcher stroke recognition using a stroke screening tool: a systematic review. Cerebrovasc Dis 42(5–6):370–377
Viereck S, Moller TP, Iversen HK, Christensen H, Lippert F (2016) Medical dispatchers recognise substantial amount of acute stroke during emergency calls. Scand J Trauma Resusc Emerg Med 24:89
Mattila OS, Puolakka T, Ritvonen J, Pihlasviita S, Harve H, Alanen A et al (2019) Targets for improving dispatcher identification of acute stroke. Int J Stroke Off J Int Stroke Soc 14(4):409–416
Dami F, Emery A, Pasquier M, Carron PN, Fuchs V, Yersin B et al (2017) Proposition and operational characteristics of a new dispatch scale to specifically identify acute strokes. Eur J Emerg Med Off J Eur Soc Emerg Med 24(3):202–207
Abbas AY, Odom EC, Nwaise I (2022) Association between dispatch complaint and critical prehospital time intervals in suspected stroke 911 activations in the national emergency medical services information system, 2012–2016. J Stroke Cerebrovasc Dis 31(3):106228
Oostema JA, Chassee T, Baer W, Edberg A, Reeves MJ (2019) Brief educational intervention improves emergency medical services stroke recognition. Stroke 50(5):1193–1200
Berglund A, von Euler M, Schenck-Gustafsson K, Castrén M, Bohm K (2015) Identification of stroke during the emergency call: a descriptive study of callers’ presentation of stroke. BMJ Open 5(4):e007661
Varjoranta T, Raatiniemi L, Majamaa K, Martikainen M, Liisanantti JH (2019) Prehospital and hospital delays for stroke patients treated with thrombolysis: A retrospective study from mixed rural-urban area in Northern Finland. Australas Emerg Care 22(2):76–80
Berglund A (2014) Face arm speech time test use in the prehospital setting, better in the ambulance than in the emergency medical communication center. Cerebrovasc Dis (Basel, Switzerland) 37(3):212–216
De Luca A, Giorgi Rossi P, Villa GF (2013) The use of Cincinnati Prehospital stroke scale during telephone dispatch interview increases the accuracy in identifying stroke and transient ischemic attack symptoms. BMC Health Serv Res 13:513
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Guidelines for the Early Management of Patients With Acute Ischemic Stroke et al (2019) Update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. https://doi.org/10.1161/STR.0000000000000211
Lindskou TA, Mikkelsen S, Christensen EF, Hansen PA, Jørgensen G, Hendriksen OM et al (2019) The Danish prehospital emergency healthcare system and research possibilities. Scand J Trauma Resusc Emerg Med 27(1):100
Hastrup S, Johnsen SP, Terkelsen T, Hundborg HH, von Weitzel-Mudersbach P, Simonsen CZ et al (2018) Effects of centralizing acute stroke services: a prospective cohort study. Neurology 91(3):e236–e248
Mikkelsen S, Lassen AT (2020) The Danish prehospital system. Eur J Emerg Med 27(6):394–395
Andersen MS, Johnsen SP, Sørensen JN, Jepsen SB, Hansen JB, Christensen EF (2013) Implementing a nationwide criteria-based emergency medical dispatch system: a register-based follow-up study. Scand J Trauma Resusc Emerg Med 21:53
https://www.ph.rm.dk/siteassets/prahospitalet/prahospitale-omrader/amk-vagtcentral/dansk-indeks-1.8---landsudgaven.pdf (Danish Criteria Based Dispatch Systeme for Emergencies) 2017 [1.8:[
Wildenschild C, Mehnert F, Thomsen RW, Iversen HK, Vestergaard K, Ingeman A et al (2014) Registration of acute stroke: validity in the Danish Stroke Registry and the Danish National Registry of Patients. Clin Epidemiol 6:27–36
Zhang Z, Kim HJ, Lonjon G, Zhu Y (2019) Balance diagnostics after propensity score matching. Ann Transl Med 7(1):16
Meretoja A, Keshtkaran M, Saver JL, Tatlisumak T, Parsons MW, Kaste M et al (2014) Stroke thrombolysis: save a minute, save a day. Stroke 45(4):1053–1058
Krebes S, Ebinger M, Baumann AM, Kellner PA, Rozanski M, Doepp F et al (2012) Development and validation of a dispatcher identification algorithm for stroke emergencies. Stroke 43(3):776–781
Heemskerk JL, Domingo RA, Tawk RG, Vivas-Buitrago TG, Huang JF, Rogers A et al (2021) Time is brain: prehospital emergency medical services response times for suspected stroke and effects of prehospital interventions. Mayo Clin Proc 96(6):1446–1457
DSR CC. Danish Stroke Registry (DSR) Annual Report 2017. Regionernes Kliniske Kvalitetsudviklingsprogram (RKKP); 2017.
DSR CC. Danish Stroke Registry (DSR) Annual Report 2018. Regionernes Kliniske Kvalitetsudviklingsprogram (RKKP); 2018.
Funding
Open access funding provided by Central Region of Denmark. The study was supported by a grant from the non-profit Danish foundation, TrygFonden (grant number 117615). The foundation did not influence the study, draft of manuscript or interpretation of results.
Author information
Authors and Affiliations
Contributions
All authors have contributed to this article by reviewing, commenting, and approving the final manuscript. MFG drafted the manuscript. MFG, HK, GA, and SPJ designed and conceptualized the study. MFG, SM, MBS, and HCC collected the data. MG and JV conducted the statistical analysis. MFG takes responsibility for the paper.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval and consent to participate
The Danish Patient Safety Authority approved the study (case no. 3–3013-3091/1) and the need for patient consent was waived. Data management was approved by the Danish Data Protection Agency (case no. 1–16-02–34-18).
Human and animal rights statement and Informed consent
The study was performed in accordance with the ethical standards in the 1964 Declaration of Helsinki and its later amendments.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gude, M.F., Valentin, J.B., Christensen, H.C. et al. Associations between emergency call stroke triage and pre-hospital delay, primary hospital admission, and acute reperfusion treatment among early comers with acute ischemic stroke. Intern Emerg Med 18, 2355–2365 (2023). https://doi.org/10.1007/s11739-023-03349-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-023-03349-x