
Abstract
Background
Obstructive sleep apnoea (OSA) is a common condition that is associated with several important comorbidities and increased mortality. Positive airway pressure (PAP) is an effective treatment for OSA that is associated with a reduction in mortality. This study investigated the prevalence and predictors of PAP prescription for OSA in Germany.
Methods
This retrospective observational study used an anonymized German claims research database. Adults (age ≥ 18 years) with treatment-naïve OSA who were or were not started on PAP were included.
Results
Of 22,317 participants, 12,297 (55%) were started on PAP; the remaining 10,020 individuals (45%) formed the control group (no PAP). Significant predictors of PAP prescription in multivariate logistic regression analysis were overweight/obesity, hypertension, heart failure, other cardiovascular diseases, gastro-oesophageal reflux disease, breathing abnormalities, vasomotor and allergic rhinitis, somatoform disorders and use of several medication classes (especially angiotensin receptor blockers, inhaled adrenergics or other inhaled drugs).
Conclusion
Only just over half of all individuals with OSA in the current analysis were prescribed PAP. The presence of a variety of comorbidities and use of several medication classes were significant predictors of PAP prescription. Future research should focus on identifying ways to increase PAP use in eligible individuals to optimize clinical outcomes.
Zusammenfassung
Hintergrund
Obstruktive Schlafapnoe (OSA) ist eine weit verbreitete Erkrankung, die mit einer Vielzahl relevanter Komorbiditäten und einer erhöhten Sterblichkeit einhergeht. Kontinuierlicher positiver Atemwegsdruck (PAP) ist eine wirksame Behandlung für OSA, die mit einer reduzierten Sterblichkeit einhergeht. In der vorliegenden Studie wurden die Prävalenz und die Prädiktoren für die Verordnung von PAP bei OSA in Deutschland untersucht.
Methode
Für diese retrospektive Beobachtungsstudie wurden anonymisierte deutsche Abrechnungsdaten von gesetzlichen Krankenkassen ausgewertet. In die Studie eingeschlossen wurden Erwachsene mit therapienaiver OSA, die mit oder ohne PAP behandelt wurden.
Ergebnisse
Von 22.317 Teilnehmern wurden 12.297 (55 %) auf PAP eingestellt; die übrigen 10.020 Personen bildeten die Kontrollgruppe (kein PAP). Signifikante Prädiktoren für die Verordnung von PAP waren in der multivariaten logistischen Regressionsanalyse Übergewicht/Fettleibigkeit, Bluthochdruck, Herzinsuffizienz, andere kardiovaskuläre Erkrankungen, gastroösophageale Refluxkrankheit, Atmungsanomalien, vasomotorische und allergische Rhinitis, somatoforme Störungen und die Einnahme verschiedener Medikamentengruppen (insbesondere Angiotensin-Rezeptorblocker, inhalative Adrenergika oder andere inhalative Medikamente).
Schlussfolgerung
In der aktuellen Analyse wurden nur etwas mehr als die Hälfte aller Personen mit OSA mit PAP behandelt. Das Vorhandensein einer Vielzahl von Begleiterkrankungen und die Einnahme mehrerer Medikamente waren signifikante Prädiktoren für die Verschreibung von PAP. Zukünftige Forschungsarbeiten sollten Strategien identifizieren, wie die Nutzung einer PAP-Therapie bei Personen mit OSA erhöht werden kann, um dadurch die klinischen Ergebnisse zu optimieren.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obstructive sleep apnoea (OSA) is a sleep-related breathing disorder characterized by frequent breathing cessation and/or reduction in airflow due to partial or complete obstruction of the upper respiratory airways [1]. Worldwide, OSA has been reported to affect nearly 1 billion adults aged 30–69 years [2], making it a common condition. For individuals with OSA who experience symptoms, these include excessive daytime sleepiness (EDS), mood alterations, and impairment of cognition [1, 3, 4]. In addition, the rate of several significant cardiovascular, cerebrovascular and metabolic comorbidities is increased in the presence of OSA, and OSA is also associated with higher all-cause mortality [5,6,7,8,9].
In addition to clinical anamnesis, polysomnography (PSG) and cardiorespiratory polygraphy (PG) are recommended for establishing a diagnosis of OSA and determining the most appropriate treatment option [1, 10, 11]. The gold standard treatment for individuals with moderate to severe OSA is positive airway pressure (PAP), which is highly effective in suppressing respiratory disturbances during sleep and improving symptoms [12, 13].
A retrospective cohort study based on German health claims data highlighted the value of positive airway pressure (PAP) therapy for the treatment of OSA [14]. The results showed that the mortality rate at 4 years after PAP prescription in individuals with OSA was significantly lower than that in subjects with OSA who were not treated with PAP (4.8% vs. 6.5%, respectively; p = 0.0175). In addition, the average length of stay per hospitalisation at 4‑year follow-up was significantly shorter in individuals with OSA who were treated with PAP therapy versus those who were not (7.9 vs. 9.3 days; p < 0.05) [14].
In Germany, the Federal Joint Committee (G-BA) issued a legally binding prerequisite for the initiation of PAP treatment within the framework of statutory health insurance (SHI) [15]. First, medical history should be taken and clinical examinations performed to exclude other forms of sleep-disordered breathing (SDB) and any other treatable underlying diseases (stages 1–2). Next, PG should be performed (stage 3). PSG is only indicated if the results of PG do not allow clear determination of the diagnosis, or to facilitate treatment (stage 4). If an indication for PAP is confirmed, initial therapy set-up should generally occur during two consecutive nights of PSG. PG should be repeated 6 months after CPAP initiation to monitor the effects of PAP therapy. Additional routine PG is not required, but follow-up examinations can be performed if problems with therapy arise.
Despite the therapeutic value of PAP and clearly defined procedures for its use in Germany, there are no current data on the number of patients with OSA being treated with PAP therapy. Therefore, the objective of this study was to collect data on the prevalence of PAP prescription among individuals with OSA in Germany, and to determine the predictors of PAP prescription in these individuals.
Methods
Study design and data source
This retrospective observational study used an anonymized German claims research database that included an approximately 5% sample of the German population who were covered by SHI. The dataset included more than 4 million insured persons from German SHI providers. Data were age- and sex-adjusted to the German population and are considered to be representative of this population in terms of morbidity, mortality and prescription drug use [16]. The dataset has been used previously to assess a large sample of the German SHI population for representative prevalence estimates of narcolepsy and chronic myeloid leukaemia [17, 18].
In accordance with the German Society for Epidemiology recommendations [19] and the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidelines [20], a detailed predefined analysis protocol was developed. The results of these analyses were reported according to the German Reporting Standard for Secondary Data Analyses [21].
Study methodology was similar to that in a previous analysis [22]. All data for healthcare services were retrieved from the German SHI billing records submitted by physicians, pharmacies and other healthcare providers, and are predominantly free of selection biases. Claims data are transferred directly from healthcare providers to a specialized data centre owned by the health insurance companies, which provides information technology and data warehousing. Claims data undergo regular audit (by insurers for reimbursement purposes) and are managed in accordance with German Social Law (paragraphs 287 SGB V and 75 SGB X). Prior to entry into the database, data were anonymized with respect to the following: identity of the insured individual; identity of the healthcare provider(s) and the specific insurance. Data included in this analysis cover the years 2015 to 2020.
Study participants
Individuals included in the analysis were aged ≥ 18 years at the index date. The PAP-treated group included previously untreated (i.e. treatment-naïve) individuals with a diagnosis of OSA who had had a PSG claim within 1.5 years after a claim for PG, and then a claim for CPAP within 1 year after PSG; the index date was defined as the date of first PAP prescription (Fig. 1).

Inclusion of positive airway pressure (PAP)-treated individuals with obstructive sleep apnoea (OSA); max. maximum, min. minimum, PG polygraphy, PSG polysomnography
To allow determination of predictors of PAP prescription, a control group was created that included individuals with newly diagnosed treatment-naïve OSA who were not prescribed PAP therapy or any other specific treatment for OSA (Fig. 2). This included two groups of patients: 1) individuals who underwent the same diagnostic process as the PAP-treated group, but did not receive PAP therapy (those with a claim for PSG between 1 January 2015 and 30 June 2018 and a claim for PG within the 1.5 years before PSG, plus at least one outpatient or inpatient diagnosis of OSA in the same quarter that PSG was performed and no claim for PAP therapy or other OSA-specific treatment); and 2) individuals who stopped the OSA diagnostic process after initial PG then had a subsequent OSA claim (coding for PG between 1 January 2016 and 30 June 2018 and at least one outpatient or inpatient OSA claim in the same quarter as the PG, plus no claims relating to OSA diagnoses or PAP prescription in the four quarters prior to inclusion, no PSG coding within 1.5 years after PG and no coding for PAP therapy between 1 Jan 2015 and 31 Dec 2020). Study participants were followed up for a minimum of 2.5 years, until January 2020.

Inclusion of untreated individuals with obstructive sleep apnoea (OSA) into the control group; PAP positive airway pressure, max. maximum, min. minimum, PG polygraphy, PSG polysomnography
Statistical analysis
Differences between individuals with OSA in the PAP-treated and control (untreated) groups were assessed using multivariate logistic regression (logit model). Categorical outcome variables were analysed descriptively using frequencies and percentages, and exact chi-squared values were used for between-group comparisons. Continuous variables are described using mean and standard deviation values, and two-sided t-tests were used for between-group comparisons. A two-sided p-value of < 0.05 was defined as indicating statistical significance. All statistical analyses were performed using MS Excel 2016 (Microsoft, Redmond, WA, USA) and SAS 9.4 (SAS Institute, Cary, NC, USA).
Results
Study population
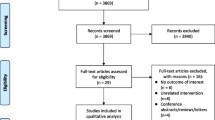
Of 4.83 million individuals in the age- and sex-stratified dataset, 78,823 had at least one diagnosis of OSA. Study inclusion criteria were met by 12,297 individuals treated with PAP, while 10,020 who did not receive PAP were included in the control group (Fig. 3). Average follow-up time per person was 3.5 years.

Participant inclusion flowchart; PAP positive airway pressure, OSA obstructive sleep apnoea, PG polygraphy, PSG polysomnography
Overall, the study population had a mean age of 58.2 ± 18.8 years and 67% were male (Table 1). Compared with the control group, individuals in the PAP-treated group were significantly more likely to be male, significantly older, had significantly higher rates of coronary artery disease without myocardial infarction, obesity, diabetes, hypertension and depression, and were significantly more likely to be receiving treatment with beta-blockers, lipid-modifying agents, angiotensin-converting enzyme inhibitors, and nonsteroidal anti-inflammatories and antirheumatics, although between-group differences in rates of depression and use of most medical therapies were numerically small (Table 1).
Diagnostic pathway
The average time between PG and PSG was 109 ± 98 days (median 81 days; interquartile range [IQR] 40–146), and there was a mean of 34 ± 64 days (median 9 days; IQR 2–33) between the initial PSG and the first PAP prescription. Thus, the average time between first PG and first PAP prescription was 173 ± 111 days (median 90 days; IQR 45–168). Overall, 82% of patients underwent PSG within 6 months after PG. Three quarters of patients had another PG and one in two patients had another PSG within 3 years after the index date.
Rate and predictors of PAP prescription
Just over half of the 22,317 individuals with OSA included in the current analysis (55%) were treated with PAP. Significant predictors of PAP prescription in multivariate logistic regression analysis were overweight/obesity, hypertension, heart failure, other cardiovascular diseases, gastro-oesophageal reflux disease, breathing abnormalities (ICD-10-GM code R06), vasomotor and allergic rhinitis, and somatoform disorders (Table 2). Use of a variety of medications, especially angiotensin receptor blockers, inhaled adrenergics or other inhaled drugs, was also a significant predictor of PAP prescription (Table 2).
Discussion
This analysis of German SHI data found that just over half of all eligible individuals with OSA were prescribed PAP. In the absence of data on variables used to phenotype individuals with OSA in clinical practice, predictors of PAP prescription in this insured population included the presence of a variety of comorbidities (especially metabolic and cardiovascular diseases) and use of several classes of medication. However, clinical variables might play a more important role in determining PAP prescription.
One potential explanation for the low rate of PAP prescription in the study population could be that a substantial proportion of individuals with mild sleep apnoea on cardiorespiratory polygraphy may not have been referred to a sleep laboratory for further investigation, and were instead managed using options other than PAP, such as weight reduction and avoiding the supine position during sleep. Overall, the current findings provide valuable real-world data that are representative of the individuals and activities in clinical practice, and can therefore help to inform the overall care of individuals with OSA.
There is currently a lack of data on rates of PAP prescription in patients with OSA, and about factors that predict the prescription of PAP therapy. A recent meta-analysis found significant associations between six factors and the purchase of a PAP device by patients with OSA [23]. These were older age, more years of education, higher income, current smoking, higher Epworth Sleepiness Scale score and higher apnoea–hypopnoea/respiratory disturbance index. Interestingly, the association between the presence of hypertension/cardiovascular disease and PAP device purchase did not reach statistical significance in that analysis [23]. In contrast, cardiovascular diseases, including hypertension and heart failure, were significant predictors of PAP initiation in treatment-naïve patients with OSA in the current study.
Overall, the number of comorbidities in our study population was high, especially coronary artery disease, obesity, chronic obstructive pulmonary disease, diabetes mellitus and arterial hypertension, which is consistent with database studies from other countries [24, 25]. Obesity is a well-known risk factor for the development of OSA [26], and overweight/obese patients were more likely to start PAP therapy in the current analysis.
The burden of mental health-related comorbidities in the study population was relatively high, with nearly a quarter of all participants (22.8%) having depression, similar to rates reported in other studies of individuals with OSA [27, 28]. Relatively high rates of mental health issues in patients with OSA may be due to a variety of factors. OSA symptoms such as EDS, fatigue, poor concentration, irritability, psychomotor issues and weight gain can overlap with symptoms of depression [29]. Alternatively, depression might also be caused by residual EDS, or depression could coexist with OSA symptoms (such as EDS) [30]. Data from a small study (n = 50) indicated a possible connection between depression and residual EDS in OSA, and suggested that PAP therapy might be able to improve both [31].
The German SHI claims data used for this analysis provide a comprehensive, patient-level picture of all reimbursed health-related services, allowing determination of epidemiological estimates and healthcare resource utilization. The large dataset is representative of the German population [16] and, with approximately 90% of the population enrolled in the SHI system and no opt-out possibility for this anonymized analysis, Germany offers a near-ideal setting to analyse population-based epidemiological estimates. Another strength of the current analysis are the objective and consistent definitions of PAP usage or non-usage (control group).
There are also several limitations that need to be considered when interpreting the findings of this study. Firstly, the maximum observational period of 6 years may not reflect the entire diagnostic process and some patients with later treatment of OSA might have been missed due to the specific timeframes applied. Secondly, the strict inclusion criteria applied to simulate the diagnostic scheme could have biased the study results. It is likely that these criteria have high specificity but poor sensitivity for identifying treatment-naïve OSA patients in the population. Thirdly, specific PSG and PG results were not available in the claims database used, and it was not possible to distinguish between diagnostic and titration PSGs. This means that there are no data on the severity of OSA, and therefore the specific indication for PAP therapy (which is primarily recommended for individuals with moderate to severe OSA). In addition, the control group did not receive treatment for OSA, not even alternatives to PAP such as mandibular repositioning devices. One potential limitation of the large population included in this study is that small between-group differences that achieved statistical significance may not be clinically significant, so this needs to be considered when interpreting the study data.
Conclusion
In this analysis of German SHI data, just over half of all eligible patients with OSA were prescribed PAP. This suggests that a significant proportion of individuals with OSA went untreated despite clear evidence of the benefits of and recommendations for treating OSA with PAP [12, 31]. The presence of a variety of comorbidities predicted the prescription of PAP therapy in the study population. Future research should focus on identifying ways to increase utilization of PAP in eligible individuals with OSA to optimize clinical outcomes.
References
Kapur VK, Auckley DH, Chowdhuri S et al (2017) Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med 13:479–504
Benjafield AV, Ayas NT, Eastwood PR et al (2019) Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med 7:687–698
Alomri RM, Kennedy GA, Wali SO et al (2021) Association between nocturnal activity of the sympathetic nervous system and cognitive dysfunction in obstructive sleep apnoea. Sci Rep 11:11990
Legault J, Thompson C, Martineau-Dussault M et al (2021) Obstructive sleep apnea and cognitive decline: a review of potential vulnerability and protective factors. Brain Sci 11:706
Mitra AK, Bhuiyan AR, Jones EA (2021) Association and risk factors for obstructive sleep apnea and cardiovascular diseases: a systematic review. Diseases 9:88
Linz D, Woehrle H, Bitter T et al (2015) The importance of sleep-disordered breathing in cardiovascular disease. Clin Res Cardiol 104:705–718
Reutrakul S, Mokhlesi B (2017) Obstructive sleep apnea and diabetes: a state of the art review. Chest 152:1070–1086
Marshall NS, Wong KK, Liu PY et al (2008) Sleep apnea as an independent risk factor for all-cause mortality: the Busselton Health Study. Sleep 31:1079–1085
Marshall NS, Wong KKH, Cullen SRJ et al (2014) Sleep apnea and 20-year follow-up for all-cause mortality, stroke, and cancer incidence and mortality in the busselton health study cohort. J Clin Sleep Med 10:355–362
Deutsche Gesellschaft für Schlafforschung und Schlafmedizin (DGSM) (2017) S3-Leitlinie Nicht erholsamer Schlaf/Schlafstörungen – Kapitel “Schlafbezogene Atmungsstörungen”. Somnologie 20:97–180
Epstein LJ, Kristo D, Strollo PJ Jr. et al (2009) Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med 5:263–276
Patil SP, Ayappa IA, Caples SM et al (2019) Treatment of adult obstructive sleep apnea with positive airway pressure: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med 15:335–343
Randerath W, Verbraecken J, de Raaff CAL et al (2021) European Respiratory Society guideline on non-CPAP therapies for obstructive sleep apnoea. Eur Respir Rev 30:210200
Woehrle H, Schoebel C, Oldenburg O et al (2020) Low long-term mortality in patients with sleep apnoea and positive airway pressure therapy: analysis of a large German healthcare database. Somnologie 24:151–158
Schneider U, Linder R, Hagenmeyer EG et al (2017) Stufendiagnostik nach der Richtlinie des G‑BA und Versorgungswirklichkeit bei vermuteter Schlafapnoe – eine analyse basierend auf Routinedaten der Techniker Krankenkasse. Gesundheitswesen 79(1):42–47
Andersohn F, Walker J (2016) Characteristics and external validity of the German Health Risk Institute (HRI) Database. Adv Pharmacoepidemiol Drug Saf 25:106–109
Kallweit U, Nilius G, Trümper D et al (2022) Prevalence, incidence, and health care utilization of patients with narcolepsy: a population-representative study. J Clin Sleep Med 18:1531–1537
Saußele S, Kohlbrenner K, Vogelmann T et al (2022) Incidence, prevalence, and real-world treatment patterns in chronic myeloid leukemia: results from a population-representative German claims data analysis. Oncol Res Treat 45:400–407
Hoffmann W, Latza U, Baumeister SE et al (2019) Guidelines and recommendations for ensuring Good Epidemiological Practice (GEP): a guideline developed by the German Society for Epidemiology. Eur J Epidemiol 34:301–317
von Elm E, Altman DG, Egger M et al (2008) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 61:344–349
Swart E, Bitzer EM, Gothe H et al (2016) A consensus German reporting standard for secondary data analyses, version 2 (STROSA-STandardisierte BerichtsROutine für SekundärdatenAnalysen). Gesundheitswesen 78:e145–e160
Häuser W, Schubert T, Vogelmann T et al (2020) All-cause mortality in patients with long-term opioid therapy compared with non-opioid analgesics for chronic non-cancer pain: a database study. BMC Med 18:162
Sawunyavisuth B, Ngamjarus C, Sawanyawisuth K (2022) A meta-analysis to identify factors associated with CPAP machine purchasing in patients with obstructive sleep apnea. Biomed Rep 16:45
Testelmans D, Spruit MA, Vrijsen B et al (2022) Comorbidity clusters in patients with moderate-to-severe OSA. Sleep Breath 26:195–204
Turino C, Bertran S, Gavaldá R et al (2017) Characterization of the CPAP-treated patient population in Catalonia. PLoS ONE 12:e185191
Nousseir HM (2019) Obesity: the major preventable risk factor of obstructive sleep apnea. J Curr Med Res Pract 4:1–5
Nilius G, Kallweit U, Trümper D et al (2022) Prevalence, incidence, and characteristics of CPAP treated OSA patients with residual excessive daytime sleepiness, as indicated by health-related data—a population representative study. Sleep Epidemiol 2:100044
Ronksley PE, Hemmelgarn BR, Heitman SJ et al (2011) Excessive daytime sleepiness is associated with increased health care utilization among patients referred for assessment of OSA. Sleep 34:363–370
Santamaria J, Iranzo A, Ma Montserrat J et al (2007) Persistent sleepiness in CPAP treated obstructive sleep apnea patients: evaluation and treatment. Sleep Med Rev 11:195–207
Ejaz SM, Khawaja IS, Bhatia S et al (2011) Obstructive sleep apnea and depression: a review. Innov Clin Neurosci 8:17–25
Schwartz DJ, Kohler WC, Karatinos G (2005) Symptoms of depression in individuals with obstructive sleep apnea may be amenable to treatment with continuous positive airway pressure. Chest 128:1304–1309
Acknowledgements
Editing assistance was provided by Nicola Ryan, independent medical writer, funded by ResMed Germany Inc.
Funding
This study was financially supported by ResMed.
Author information
Authors and Affiliations
Contributions
HW, CS and MA were involved in the conception, hypothesis development and design of the study, the analysis and interpretation of the data, and critical review of the manuscript. HW was also involved in preparation of the first draft of the manuscript. JHF, IF and PY were involved in interpretation of the data and critical review of the manuscript. MD was involved in conception, hypothesis development and design of the study, interpretation of the data analysis and critical review of the manuscript. KLS and DET were involved in study design and critical review of the manuscript. TV and SW were involved in conception and study design, analysis and interpretation of data, and critical review of the manuscript. All authors approved the final version of the manuscript and agreed with submission for publication.
Corresponding author
Ethics declarations
Conflict of interest
H. Woehrle has received lecture/consulting fees from Astra Zeneca, Allergopharma, Bioprojet, Boehringer Ingelheim, Chiesi, GSK, Novartis, Inspire, Jazz and ResMed, and research support from ResMed and Novartis. M. Arzt has received grant support from ResMed, the ResMed Foundation, Philips Respironics and the Else-Kroehner Fresenisus Foundation, and lecture and/or consulting fees from ResMed, WITA Italia and Philips Respironics. J.H. Ficker has received grants and personal/lecture fees from ResMed and Inspire. AG is an employee of ResMed. M. Deger, K.L. Sterling and D. Ehrsam-Tosi are employees and shareholders of ResMed. T. Vogelmann is owner of LinkCare GmbH, which has received consulting fees from ResMed, Nyxoah and Jazz Pharmaceuticals. S. Weinand is an employee of LinkCare GmbH. I. Fietze reports support and grants from ResMed and Löwenstein Medical, personal fees from ResMed and Bioprojet, and has an unpaid role as director of the German Sleep Foundation. C. Schoebel has received grants from Astra Zeneca, ResMed and Bayer, consulting fees from ResMed, Idorsia, Bristol-Myers Squibb and Astra Zeneca, and honoraria/lecture fees from Berlin Chemie, Takeda and Mementor; he also has unpaid roles as treasurer of the German Sleep Society, head of the Telemedicine Working Group of the German Society for Internal Medicine and treasurer of the Sleep Apnea Working Group of the German Cardiac Society. F, P. Young declares that he has no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies mentioned were in accordance with the ethical standards indicated in each case.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.

Scan QR code & read article online
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Woehrle, H., Arzt, M., Ficker, J.H. et al. Prevalence and predictors of positive airway pressure therapy prescription in obstructive sleep apnoea: a population-representative study. Somnologie (2023). https://doi.org/10.1007/s11818-023-00435-2
Accepted:
Published:
DOI: https://doi.org/10.1007/s11818-023-00435-2
Keywords
- Continuous positive airway pressure
- Obstructive sleep apnoea
- Population study
- Health claims data
- Predictors