
Abstract
Background
Today’s society is much more mobile than in the past. This increased mobility has resulted in different marriage/parenting groups. We wished to study the demographics of developmental dysplasia of the hip (DDH) in our area and compare/contrast our findings with those in the literature and specifically look for new findings compared to previous studies.
Methods
A retrospective review of all children with DDH from 2003 through 2012 was performed. The age at first visit, gestational age, pregnancy number, gender, race, and family history of DDH was collected. Statistical significance was a p-value < 0.05.
Results
There were 424 children (363 girls, 61 boys). Ethnicity was White in 80.8 %, Hispanic in 13.8 %, Black in 4.0 %, and Indo-Malay and Indo-Mediterranean in 0.7 % each; 66.8 % were unilateral; 14.2 % had a positive family history. The average gestational age was 38.1 weeks; 94.4 % were full term. The child was vertex presentation in 67.6 % and breech in 32.4 %; 52.8 % were delivered vaginally and 47.2 % by Cesarean section. The child was the first-born in 48.3 %. When compared to the birth statistics of our state, there was a higher proportion of Whites and Hispanics with DDH, and a lower, but not inconsequential, proportion of Blacks (p = 0.0018).
Conclusion
Mixing of gene pools and infant carrying methods (lack of swaddling or marked abduction) occurring with societal change likely explains the higher than expected proportion of DDH amongst those of Hispanic ethnicity and a lower than expected, but not rare, proportion in those of African ancestry.
Level of evidence
Level IV—retrospective case series.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Developmental dysplasia of the hip (DDH) encompasses a wide spectrum of pathology, ranging from a complete fixed dislocation at birth to asymptomatic acetabular dysplasia in the adult [1–5]. The demographics of DDH have been investigated by many authors [6]. There are no recent studies of the demographics of DDH in the United States, the last ones being from 1968 [7] and 1989 [8]. Today’s society is much more mobile than in the past. This increased mobility has resulted in different marriage/parenting groups, with subsequent mixing of gene pools resulting in gene pool changes. Similarly, with the intermingling of ethnic/racial groups, traditional infant carrying/transport methods may also change. The purpose of this study was to examine the demographics of DDH in our area and compare/contrast our findings with those in the literature and determine if there are any new findings compared to previous studies.
Materials and methods
All children with DDH treated at the authors’ institution over the 10-year period from 2003 through 2012 were identified by the ICD9 code of 754.3x and appropriate CPT codes (27256, 27257, 27258, 27259, 27146, 27147, 27151, 27156, and 27165). The charts and radiographs were reviewed to confirm the diagnosis. Children with teratologic, neuromuscular, and/or syndromic hip dysplasia were excluded. This study was approved by our local Institutional Review Board.
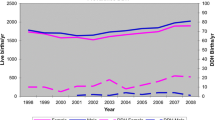
From the medical records, the age at the first visit to the orthopedic surgeon (which might be slightly older than the age at diagnosis), gestational age, pregnancy number, gender, race, family history of DDH, and treatment modality was collected. Race was classified as White, Black, Amerindian [Native American and Hispanic (Native American/Caucasian mestizos)], Indo-Malay (Asian origins), and Indo-Mediterranean (Middle East and Indian subcontinent) [9]. The demographic data of live births in Indiana from 2003 through 2011 were provided by the Indiana State Department of Health, Epidemiology Resource Center, Data Analysis Team, Indianapolis, Indiana. These were then compared to the proportions of DDH children in this study.
Continuous data are reported as the mean ± 1 standard deviation and categorical data as frequencies or percentages. Differences between groups of continuous data were analyzed using the non-parametric Mann–Whitney (two groups) or Kruskal–Wallis (>2 groups) tests due to the non-normal distribution of the data. Differences between groups of categorical data were analyzed using Fisher’s exact test (2 × 2 analyses) or Pearson’s χ2 test (>2 × 2 analyses). Statistical analyses were performed with Systat 10™ software (SPSS, 2000, Chicago, IL, USA). For all analyses, a p-value < 0.05 was considered to be statistically significant.
Results
There were 424 children [363 girls (85.6 %), 61 boys (14.4 %)] with DDH. The racial composition was White in 80.8 %, Amerindian (all Hispanic, no Native Americans) in 13.8 %, Black in 4.0 %, and Indo-Malay and Indo-Mediterranean in 0.7 % each. The DDH was unilateral in 66.8 %; of the unilateral cases, 74.4 % involved the left hip and 25.6 % involved the right hip. The average birth weight was 3,320 ± 574 g (range 624–4,916) and the average gestational age was 38.1 weeks (range 24–42); 94.4 % were full term, 5.1 % pre-term, and 0.5 % post-term. The child was a vertex presentation in 67.6 % and breech in 32.4 %; 52.8 % were delivered vaginally and 47.2 % by Cesarean section. The child was the first-born in 48.3 % and 51.7 % were multigravida births. There was a family history of DDH in 14.2 %. The median age at the first visit to the orthopedic physician was 1.6 months.
There were no differences between those patients with unilateral or bilateral DDH by gender, race, birth weight, gestational age, birth presentation (vertex vs. breech), method of delivery (vaginal vs. Cesarean section), birth order (first-born vs. multigravida), or family history. Similarly, there were no differences within the unilateral group by right versus left hip involvement for all the above same parameters. Finally, there were no differences between those cases with or without a family history of DDH by gender, race, birth weight, gestational age, birth presentation (vertex vs. breech), method of delivery (vaginal vs. Cesarean section), or birth order (first-born vs. multigravida).
Differences were noted by gender for birth weight, presentation, and method of delivery. Girls had a lower birth weight compared to boys (3,300 ± 548 g vs. 3,444 ± 707 g, p = 0.025), a higher proportion of vertex presentation (69.7 % vertex, 30.3 % breech) compared to boys (55.2 % vertex, 44.8 % breech) (p = 0.034), and fewer Cesarean section deliveries than boys (girls 45.2 %, boys 59.6 %, p = 0.046). The only difference by race was for birth weight [White = 3,349 ± 575 g (624–4,961), Hispanic 3,310 ± 451 g (2,466–4,423), Black 2,839 ± 775 g (1,077–3,657), p = 0.013].
First-born children had a younger median age at the first visit compared to multigravida births (1.4 vs. 1.9 months, p = 0.012). There was a higher proportion of breech compared to vertex presentation (first-born 40.2 % breech, 59.8 % vertex; multigravida 24.3 % breech, 75.7 % vertex; p = 0.002) and a higher proportion of delivery by Cesarean section (first-born 46.3 % vaginal, 53.7 % Cesarean; multigravida 58.5 % vaginal, 41.5 % Cesarean; p = 0.03).
There were a higher number of Hispanics and a lower number of Blacks with DDH than expected when compared to the proportion of live births in our state (p = 1.9 × 10−6) (Table 1). Statistical significance remained when excluding the small numbers in the Indo-Mediterranean and Indo-Malay groups (p = 3 × 10−7).
Discussion
Our data are very similar to the other DDH demographic studies regarding gender and laterality. DDH is more common in girls, with 12–30 % bilaterality, and increased in those with breech presentation or delivery [7, 10–46]. Breech presentation or birth in children with DDH ranges from 7.1 to 40 % [6], and was 32.4 % in this series. The percentage of Cesarean deliveries in this study was higher than in the overall state of Indiana from 2003 through 2011 (47.2 vs. 28.9 %, p < 0.0001). This likely reflects the higher incidence of breech presentation in children with DDH, as breech babies are much more likely to be born by Cesarean section. DDH is also increased in first-borns [10, 15, 18, 47–50]. In our series, 48.3 % of the children with DDH were first-born compared to the 38.9 % in the general Indiana population (p = 0.004). A positive family history is a well-known positive predictor of DDH [11, 12, 15, 17, 26, 34, 51–57]. There was a family history of DDH in 14.2 % of the children in our study.
An interesting new finding in this study was that the number of Black children with DDH was lower than expected, but not inconsequential/rare, when compared to the proportion of live births (4.0 vs. 11.7 %), while the number of Hispanic children with DDH was higher than expected (13.8 vs. 9.4 %). The proportion of DDH in Blacks being ~1/3 of that expected in Indiana is similar to that in New York state [~1/2 of that expected (2.4 vs. 5.1 %)] [7]. DDH was previously considered to be extremely rare in those of African descent [58–66]. Our study suggests that this is no longer true.
This is in contrast to Hispanic children. Hispanics in Indiana are predominantly immigrants from Mexico [67], with a genome admixture of Native American and Caucasian genes [9, 68–70]. The incidence of DDH is high in Native Americans (76.1/1,000) [6]. In a recent review of DDH [6], no study evaluated the incidence/prevalence of DDH in Hispanics. In this study, DDH in Hispanic children was ~33 % greater than expected (13.8 % DDH, 9.4 % normal population), likely due to the presence of Native American genes.
How can these differences be explained? The etiology of DDH is multifactorial, and includes the interaction of both genetic and environmental factors. Genetic mixing in this country of both Blacks and Native Americans with Caucasians can help explain these findings. Blacks in the United States demonstrate a range of 7–20 % admixture with Caucasian genes [71, 72]. The mixing of African genes, which have a lower propensity for DDH when compared to United States Caucasians [58, 64], will raise the prevalence of DDH in American Blacks. The reverse will occur in Hispanics. The mixing of Native American genes with Caucasians, which have a higher prevalence of DDH compared to Caucasians [6], will lower the prevalence of DDH compared to Native Americans, but be higher than that of Caucasians.
An environmental factor involves infant transport and clothing. DDH was very high in Native Americans in earlier studies [6, 73], due to tight swaddling of the infant in most Native American societies. There was a 10-fold increase in DDH (123.0 vs. 12.6) in Canadian Native Americans when infants were placed in a cradleboard [74]. Such tight swaddling is less common in today’s North American societies. Hispanics in this country possess the Native American genes for DDH, but which is no longer exacerbated by tight swaddling. This can explain why the proportion of DDH in Hispanics is higher than in Caucasians, but not as high as in earlier Native American studies. The opposite likely occurs in United States Black children. In traditional African cultures, children are not swaddled, but, rather, abducted across the mother’s pelvis, which protects the infant from DDH. In North America, Black children are not carried in such an abducted position, but, rather, transported in manners similar to Caucasians (e.g., standard baby strollers and car seats), where the hips are not markedly abducted, but neither tightly swaddled.
The influence of environment on genetic factors is well demonstrated by the markedly different incidences of DDH in two different northern circumpolar peoples, the Sámi and Inuit/Eskimos, which have similar environments regarding ambient temperatures. The Sámi, genetically originating from Caucasians [75], traditionally swaddled their young and had a very high incidence of DDH (25–40/1,000) [76–78]. The Inuit/Eskimos have a genetic origin very similar to Native Americans [9, 79, 80]; however, Inuit mothers carry their young in a hood (amauti) inside their parkas, which abducts the hips by straddling the mother’s back. They have an incidence of DDH similar to Caucasians [81]. Finally, DDH is very rare in cultures without swaddling (Southern Chinese, African Bantu, Thailand, North Korea, Sri Lanka [82, 83]).
There are several limitations to this study. First, it does not include all children with DDH in the state of Indiana, as there are likely some children cared for by other orthopedic surgeons outside of our institution. This prevented us from calculating an incidence rate. Next, race/ethnicity was determined from the medical record demographic sheet, which is entered by a clerk, not recorded by a physician. Thus, there is the possibility of some inaccuracy in that variable. Third, the family history of DDH was only that recorded in the medical record as recollected by the parents. Therefore, there is the possibility that some of the positive histories were negative, but also that some of the negative histories were actually positive but not known by the parents and, thus, not recorded. Other variables, such as birth order and birth weight, are likely very accurate.
In summary, this study has confirmed many of the previously known demographic findings for DDH, namely it being more common in girls, left hip, first-born, breech presentation, and Cesarean section delivery. However, it refutes prior studies denoting the extreme rarity of DDH in those of African ancestry. Roper [58] stated that “factors responsible for the primary defects in hip dysplasia are, for practical purposes, absent in the Bantu people”. Griffiths [60] stated that “the apparent rarity of true CDH in Africa remains unexplained”. The percentage of DDH in Blacks in this study (4.0 %) was lower than that of the general population in our state (11.7 %), but, on the other hand, not as extremely rare as quoted by Roper and Griffiths. The percentage of DDH in Hispanics is moderately higher than Caucasians. These two findings likely reflect a convergence of both genetic and environmental factors in the etiology of DDH. A physician evaluating a child for possible DDH of African ethnicity should not assume that the chances of DDH are markedly lower than in other ethnic groups, while the concern for DDH in those of Hispanic ancestry should still be the same, if not heightened.
References
American Academy of Pediatrics, Committee on Quality Improvement, Subcommittee on Developmental Dysplasia of the Hip (2000) Clinical practice guideline: early detection of developmental dysplasia of the hip. Pediatrics 105:896–905
Aronsson DD, Goldberg MJ, Kling TF Jr, Roy DR (1994) Developmental dysplasia of the hip. Pediatrics 94:201–208
Chan A, McCaul KA, Cundy PJ, Haan EA, Byron-Scott R (1997) Perinatal risk factors for developmental dysplasia of the hip. Arch Dis Child Fetal Neonatal Ed 76:F94–F100
Chan A, Foster BK, Cundy PJ (2001) Problems in the diagnosis of neonatal hip instability. Acta Paediatr 90:836–839
Harcke HT (1999) Developmental dysplasia of the hip: a spectrum of abnormality. Pediatrics 103:152
Loder RT, Skopelja EN (2011) The epidemiology and demographics of hip dysplasia. ISRN Orthop 2011:238607
Robinson GW (1968) Birth characteristics of children with congenital dislocation of the hip. Am J Epidemol 87:275–284
Hazel JR, Beals RK (1989) Diagnosing dislocation of the hip in infancy. West J Med 151:39–41
Eveleth PB, Tanner JM (1990) Worldwide variation in human growth, 2nd edn. Cambridge University Press, Cambridge
Ang KC, Lee EH, Lee PYC, Tan KL (1997) An epidemiological study of developmental dysplasia of the hip in infants in Singapore. Ann Acad Med Singapore 26:456–458
Mirdad T (2002) Incidence and pattern of congenital dislocation of the hip in Aseer region of Saudi Arabia. West Afr J Med 21:218–222
Kremli MK, Alshahid AH, Khoshhal KI, Zamzam MM (2003) The pattern of developmental dysplasia of the hip. Saudi Med J 24:1118–1120
Poul J, Bajerová J, Sommernitz M, Straka M, Pokorny M, Wong FYH (1992) Early diagnosis of congenital dislocation of the hip. J Bone Joint Surg Br 74:695–700
Noble TC, Pullan CR, Craft AW, Leonard MA (1978) Difficulties in diagnosing and managing congenital dislocation of the hip. Br Med J 2(6137):620–623
Heikkilä E (1984) Congenital dislocation of the hip in Finland. An epidemiologic analysis of 1035 cases. Acta Orthop Scand 55:125–129
Hadlow V (1988) Neonatal screening for congenital dislocation of the hip. A prospective 21-year survey. J Bone Joint Surg Br 70:740–743
Mamouri GH, Khatami F, Hamedi AB (2004) Congenital dislocation of the hip in newborns of Mashhad City. Internet J Ped Neonat, vol 4. Accessed 22 Nov 2008
Boo NY, Rajaram T (1989) Congenital dislocation of hips in Malaysian neonates. Singapore Med J 30:368–371
Bjerkreim I (1974) Congenital dislocation of the hip joint in Norway. IV. The incidence in southeast Norway. Acta Orthop Scand Suppl 157:75–88
Bjerkreim I, van der Hagen CB (1974) Congenital dislocation of the hip joint in Norway. V. Evaluation of genetic and environmental factors. Clin Genet 5:433–448
Bjerkreim I (1976) Congenital dislocation of the hip joint in Norway. A clinical-epidemiological study. J Oslo City Hosp 26:79–90
Paterson DC (1976) The early diagnosis and treatment of congenital dislocation of the hip. Clin Orthop Relat Res 119:28–38
Paterson D (1976) The early diagnosis and treatment of congenital dislocation of the hip. Aust N Z J Surg 46:359–366
Bower C, Stanley FJ, Kricker A (1987) Congenital dislocation of the hip in Western Australia. A comparison of neonatally and postneonatally diagnosed cases. Clin Orthop Relat Res 224:37–44
Abdinejad F, Takapouy J, Eskandari N (1996) Incidence of congenital dislocation of the hip in Shiraz. Med J Islamic Repub Iran 9:275–280
Wynne-Davies R (1970) A family study of neonatal and late-diagnosis congenital dislocation of the hip. J Med Genet 7:315–333
Carter CO, Wilkinson JA (1964) Genetic and environmental factors in the etiology of congenital dislocation of the hip. Clin Orthop Relat Res 33:119–128
Clausen I, Nielsen KT (1988) Breech position, delivery route and congenital hip dislocation. Acta Obstet Gynecol Scand 67:595–597
Tejavej A, Siripoonya P (1984) Breech presentation and the newborn hip. J Med Assoc Thai 67(Suppl 2):80–85
Luterkort M, Persson P-H, Polberger S, Bjerre I (1986) Hip joint instability in breech pregnancy. Acta Paediatr Scand 75:860–863
Czéizel A, Szentpétery J, Kellermann M (1974) Incidence of congenital dislocation of the hip in Hungary. Br J Prev Soc Med 28:265–267
Artz TD, Lim WN, Wilson PD, Levine DB, Salvati EA (1975) Neonatal diagnosis, treatment and related factors of congenital dislocation of the hip. Clin Orthop Relat Res 110:112–136
Phillips LI (1968) Congenital dislocation of the hip in the newborn. A survey at National Women’s Hospital 1954–68. N Z Med J 68:103–108
Romero MI, Julián M, Gaete V, Bedregal P, Pinto JI, Castiglione C (1989) Características epidemiológicas de la displasia congénita de caderas en una población chilena [Epidemiologic characteristics of congenital hip dysplasia in a Chilean population]. Rev Chil Pediatr 60:268–271
Hatzmann W, Skowronek B, Höffken H, Schröter A, Schmitz F-J, Werner-von-der-Burg W (1993) Hüftsonographische befunde an neugeborenen nach schwangerschaft und geburt in beckenendlage [Sonographic findings in the hip of newborn infants after pregnancy and labor from breech position]. Ultraschall Med 14:163–168
Padilla Esteban ML, Espert AN, de la Mano AC, Pardo JMG-S (1990) Incidencia en la enfermedad luxante de la cadera en 40.243 nacidos vivos (Parte II) [Frequency of congenital dislocation of the hip in 40,243 live births (Part II)]. An Esp Pediatr 33:539–541
Al-Umran K, Ahlberg A, Dawodu AH, El-Mouzan MI, Ahmad FA (1988) Neonatal screening for hip instability: five years experience. Ann Saudi Med 8:425–429
Kauppila O (1975) The perinatal mortality in breech deliveries and observations on affecting factors. A retrospective study of 2227 cases. Acta Obstet Gynecol Scand Suppl 39:1–79
Wray DG, Muddu BN (1983) Congenital dislocation of the hip. The high incidence of familial aetiology—a study of 130 cases. Br J Clin Pract 37:299–303
Szepesi J, Hattyár A, Molnár L (1993) A medencevégu fekvés hatása a csípok fejlodésére [The effect of breech presentation on the development of the hips]. Magy Traumatol Ortop Kézseb Plasztikai Seb 36:11–15
Rühmann O, Lazović D, Bouklas P, Gossé F, Franke J (1999) Sonographisches huftgelenk-screening be neugeborenen. Korrelation von anamnestischen risikofaktoren und hüftdysplasia [Ultrasound hip joint screening in newborn infants. Correlation of anamnestic risk factors and hip dysplasia]. Klin Pädiatr 211:141–148
Patterson CC, Kernohan WG, Mollan RAB, Haugh PE, Trainor BP (1995) High incidence of congenital dislocation of the hip in Northern Ireland. Paediatr Perinat Epidemiol 9:90–97
Khan MRH, Benjamin B (1992) Congenital hip instability in hospital born neonates in Abha. Ann Saudi Med 12:184–187
Fuentes Díaz A, Sánchez Navas L, Andreu Viladrich R (1997) Factores obstétricos y perinatales en la luxación congénita de cardera [Obstetric and perinatal risk factors for congenital dislocation of the hip]. An Esp Pediatr 46:29–32
Mufti MH (1988) Prime factors in the etiology of congenital dislocation of the hip and talipes equinovarus in Riyadh. Ann Saudi Med 8:29–34
Abdel-Kader M, Booz MK (1968) Experience with congenital dislocation of the hip in Kuwait. J Kwt Med Assoc 21
Czéizel A, Vizkelety T, Szentpéteri J (1972) Congenital dislocation of the hip in Budapest, Hungary. Br J Prev Soc Med 26:15–22
Wilkinson JA (1972) A post-natal survey for congenital displacement of the hip. J Bone Joint Surg Br 54:40–49
Padilla Esteban ML, Espert AN, Pardo JMG-S, de la Mano AC (1990) Incidencia en la enfermedad luxante de la cadera en 40.243 nacidos vivos (Parte I) [Incidence of congenital hip dislocation in 40,243 live births (Part I)]. An Esp Pediatr 33:535–538
Doig JR, Shannon FT (1975) Congenital dislocation of the hip. An evaluation of neonatal diagnosis. N Z Med J 82:367–369
Hoaglund FT, Healey JH (1990) Osteoarthrosis and congenital dysplasia of the hip in family members of children who have congenital dysplasia of the hip. J Bone Joint Surg Am 72:1510–1518
Dogruel H, Atalar H, Yavuz OY, Sayli U (2008) Clinical examination versus ultrasonography in detecting developmental dysplasia of the hip. Int Orthop 32:415–419
Coleman SS (1968) Congenital dysplasia of the hip in the Navajo infant. Clin Orthop Relat Res 56:179–193
Houston CS, Buhr RH (1988) Swaddling of Indian infants in northern Saskatchewan. Musk-Ox 36:5–14
Hanflig SS (1933) Familial congenital dislocation of the hip. N Engl J Med 209:545–547
Tsuchiya K, Suzuki T, Okuyama S, Mori K, Miyazaki K, Watanabe S et al (1959) Genetic study on congenital dislocation of the hip. J Japan Orthop Assoc 33:864–879
Rybak K, Zwierzchowska D, Zwierzchowski H (1984) Rodzinne wystepowanie wrodzonego zwichniecia biodra [Familial occurrence of congenital hip dislocation]. Chir Narzadow Ruchu Ortop Pol 49:545–547
Roper A (1976) Hip dysplasia in the African Bantu. J Bone Joint Surg Br 58:155–158
Edelstein J (1966) Congenital dislocation of the hip in the Bantu. J Bone Joint Surg Br) 48-B:397
Griffiths JC (1970) Dislocated hip in East African infants and children. Postgrad Med J 46:86–91
Omololu B, Ogunlade SO, Alonge TO (2005) Pattern of congenital orthopaedic malformations in an African teaching hospital. West Afr J Med 24:92–95
Skirving AP, Scadden WJ (1979) The African neonatal hip and its immunity from congenital dislocation. J Bone Joint Surg Br 61-B:339–341
Eidelman M, Chezar A, Bialik V (2002) Developmental dysplasia of the hip incidence in Ethiopian Jews revisited: 7-year prospective study. J Pediatr Orthop B 11:290–292
Reed TE (1969) Caucasian genes in American Negroes. Science 165(3895):762–768
Finley WH, Gustavson K-H, Hall TM, Hurst DC, Barganier CM, Wiedmeyer JA (1994) Birth defects surveillance: Jefferson County, Alabama, and Uppsala County, Sweden. South Med J 87:440–445
Burke SW, Macey TI, Roberts JM, Johnston C 3rd (1985) Congenital dislocation of the hip in the American Black. Clin Orthop Relat Res 192:120–123
Aponte R (2002) Latinos in Indiana: growth, distribution, and implications. Statistical Brief No. 14, the Julian Samora Research Institute, East Lansing, Michigan
Wang S, Ray N, Rojas W, Parra MV, Bedoya G, Gallo C et al (2008) Geographic patterns of genome admixture in Latin American Mestizos. PLoS Genet 4(3):e1000037
Haverluk T (1997) The changing geography of US Hispanics, 1850–1990. J Geogr 96:134–145
Rubi-Castellanos R, Martínez-Cortés G, Muñoz-Valle JF, González-Martín A, Cerda-Flores RM, Anaya-Palafox M et al (2009) Pre-Hispanic Mesoamerican demography approximates the present-day ancestry of Mestizos throughout the territory of Mexico. Am J Phys Anthropol 139:284–294
Burchard EG, Ziv E, Coyle N, Gomez SL, Tang H, Karter AJ et al (2003) The importance of race and ethnic background in biomedical research and clinical practice. N Engl J Med 348:1170–1175
Parra EJ, Marcini A, Akey J, Martinson J, Batzer MA, Cooper R et al (1998) Estimating African American admixture proportions by use of population-specific alleles. Am J Hum Genet 63:1839–1851
Blatt SH (2015) To swaddle, or not to swaddle? Paleoepidemiology of developmental dysplasia of the hip and the swaddling dilemma among the indigenous populations of North America. Am J Hum Biol 27:116–128
Salter RB (1968) Etiology, pathogenesis and possible prevention of congenital dislocation of the hip. Can Med Assoc J 98:933–945
Ross AB, Johansson Å, Ingman M, Gyllensten U (2006) Lifestyle, genetics, and disease in Sami. Croat Med J 47:553–565
Mellbin T (1962) The children of Swedish nomad Lapps. VII. Congenital malformations. Acta Orthop Scand 131(Suppl):62–66
Getz B (1955) The hip joint in Lapps and its bearing on the problem of congenital dislocation. Acta Orthop Scand Suppl 18:1–81
Eriksson AW, Lehmann W, Simpson NE (1980) Genetic studies on circumpolar populations. In: Milan FA (ed) The human biology of circumpolar populations. Cambridge University Press, Cambridge, pp 81–168
Raghavan M, DeGiorgio M, Albrechtsen A, Moltke I, Skoglund P, Korneliussen TS et al (2014) The genetic prehistory of the New World Arctic. Science 345:1255832
Harper AB (1980) Origins and divergence of Aleuts, Eskimos, and American Indians. Ann Hum Biol 7:547–554
Society for Applied Anthropology in Manitoba. Summary of SAAM presentations. Anthropol Pract 2001:10
Janecek M (1956) Prispevek k otazce vrozeneho vykloubení kloubu kycelniho u deti ve Severni Koreji [Congenital hip dislocation in children in Northern Korea]. Acta Chir Orthop Traumatol Cech 23:2–5
Corea JR (1992) Is congenital dislocation of the hip rare in Sri Lanka? Ceylon Med J 37:96
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Loder, R.T., Shafer, C. The demographics of developmental hip dysplasia in the Midwestern United States (Indiana). J Child Orthop 9, 93–98 (2015). https://doi.org/10.1007/s11832-015-0636-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11832-015-0636-1