
Abstract
Purpose
We performed a multidisciplinary investigation of young adults involved in motor vehicle collisions (MVCs) to elucidate injury mechanisms and the role of passive safety equipment such as seat belts and airbags.
Methods
MVCs resulting in death or serious injuries to the driver or passengers aged 16–24 years in southeastern Norway during 2013–2016 were investigated upon informed consent. We assessed the crash scene, the motor vehicle (MV) interior and exterior, and analyzed data from medical records, forensic autopsies and reports from police and civil road authorities.
Results
This study included 229 young adult occupants involved in 212 MVCs. The Maximum Abbreviated Injury Scale (MAIS) score was ≥2 in 111 occupants, of which 22 were fatalities. In 59% (65/111) of the cases with MAIS score ≥2 injuries, safety errors and occupant protection inadequacies were considered to have contributed to the injury outcome. Common errors were seatbelt non-use and misuse, carrying insecure luggage, and the seat back being too reclined. MAIS score ≥2 head/neck injuries were observed in side impacts despite correct seatbelt use, related to older MVs lacking side airbag curtains. The independent risk factors for MAIS score ≥2 injuries included not using a seatbelt, driving under the influence of alcohol or drugs, nighttime driving, side impacts, heavy collision partner, and MV deformation.
Conclusion
User safety errors (not using a seatbelt, seatbelt misuse, excessive seat-back reclining, and insecure cargo) and a lack of occupant protection in older MVs resulted in young adults sustaining severe or fatal injuries in MVCs.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Major enhancements in road infrastructure, vehicle safety, and the enforcement of traffic laws have substantially improved road safety in developed countries [1]. However, young drivers have been shown to have the highest crash risk and injury rates on the road [2,3,4]. In Norway, the rate of road traffic deaths has decreased markedly from approximately 13 to 2.5 per 100,000 persons/year over the last 50 years, which also reflects substantial improvements in the quality of prehospital and hospital care. However, road traffic injuries remain a public health concern, especially for the young population. From 2000 to 2020, 24% of the fatalities and 26% of severe injuries in road traffic incidents in Norway involved young adults aged 16–24 years. Approximately 71% of these victims were injured in motor vehicle collisions (MVCs) and were either drivers or passengers in four-wheeled cars [5].
The Norwegian government has implemented the Vision Zero road traffic safety project as the basis for national traffic safety activities [6], with the ambition of no one being killed or permanently disabled due to road traffic collisions in the future. This impressive goal requires targeted preventive action based on updated knowledge. However, few studies have been dedicated to understanding and investigating the factors underlying the injury severity for young occupants involved in MVCs [7]. Knowledge about what causes a collision and the specific injury mechanisms for occupants is essential. As the limits of human tolerance to impact forces is a central concept of Vision Zero, it is also essential to understand what protects occupants from being injured in a severe collision. Such understanding can lead to designing well-targeted and restrictive measures, and provide the groundwork for political solutions to enhance road safety for young adults.
Based on the aforementioned background, we designed a study focusing on young adults involved in major MVCs on Norwegian roads. We set out to identify the characteristics of a collision leading to injury, including the occupants’ movements inside the motor vehicle (MV) at the time of the collision, and the use and effects of seatbelts, airbags, and other safety measures. By characterizing the injuries sustained by the occupants and the underlying mechanisms, the goal was to determine which injuries are preventable.
Material and methods
Investigation protocol
This was a study of young adult occupants involved in high-energy MVCs collected from March 2013 to March 2016 in southeastern Norway. Overviews of the investigation protocol have been published previously [8, 9].
The criteria for inclusion were the occurrence of a high-energy MVC involving one or more occupants aged 16–24 years and at least one of the occupants in the MV being met by a trauma team in the admitting hospital. The investigation team was then alerted by the regional Emergency Medical Communication Centers (EMCCs). The team of investigators started the process of collecting data and was dispatched to the crash scene within 24 h of the collision to investigate the case MV in which the injured young adult had been sitting in. In brief, the collision investigators systematically assessed the exterior and interior environments of the MV, approached the involved occupants to ask them to participate in the study, and after receiving their consent performed an interview. Information was also obtained from emergency medical service personnel, staff from police and civil road authorities, and witnesses where available. Reports on the aftermath of the collision were collected from the EMCC records, police, and the collision-analysis groups of the Norwegian Public Roads Administration. The crash data, including information about road infrastructure and conditions, involved vehicles, and occupants, were collected and categorized in the dataset. With consent from participants or the next of kin, the medical records and autopsy reports were also retrieved.
The internal evaluation of the MV focused on contact points between the occupant and the MV interior (as documented by dents/deformations on the interior surfaces or deposited biological material such as blood, skin, or hair), use of seatbelts (friction marks thereon), safety equipment (number of front airbags, side airbags and side curtain airbags in the MV, airbag deployment, seatbelt pretensioners, and load limiters), and the presence of heavy insecure objects. The front and rear seat backs were inspected to determine whether seats had been displaced or damaged/distorted by the movements of heavy insecure objects. Any such displacement was measured and recorded in centimeters. An assessment of the passenger compartment’s integrity and measurements of component intrusions were also performed during the interior inspection.
The investigators subsequently performed a reconstruction of each occupant’s movements during the collision based on the information obtained from the examination of the MV’s exterior and interior examination and knowledge about the injuries that occurred. A person of approximately the same size was placed in the crashed MV in an attempt to determine the occupant’s movements and possible contact points within the MV’s interior. The reconstruction and technical investigations of the MV exterior, interior, and collision environment were documented using photographs, and a detailed collision report for each MVC was generated by the collision investigators.
Finally, all cases were reviewed by a multidisciplinary team consisting of physicians with expertise in traumatology and forensic medicine, and paramedics with expertise in collision investigations.
Calculation of collision speed and impacting forces
The principal direction of impact force and the instantaneous change in velocity (ΔV) were calculated manually. We superimposed the face of a compass over the illustration of an MV, with 0° (or 360°) aligned at its front. Collision impacts were then categorized into frontal (0 to 45°, 315 to 360°), side (226 to 314° on the left, 46 to 134° on the right), rear (135 to 225°), and rollover (at least 180° on the horizontal axis). The occurrence of an impact did not mutually exclude another impact. Side impacts were further categorized into nearside and offside based on the occupant’s position relative to the collision side.
MV types were classified into passenger car (station wagon, hatchback, or sedan), sport utility vehicle/minibus/minivan, and truck/bus.
Injury severity
The incident was considered fatal if death was due to injuries sustained during the collision and occurred within the first 30 days thereafter. The Abbreviated Injury Scale (MAIS) score, Maximum MAIS score, Injury Severity Score, and New Injury Severity Score were calculated for each case [10]. Data on the sex, height, and BMI of each occupant were also recorded.
We defined an occupant with an MAIS score of ≥2 in at least one body region as injured, while the others were coded as not injured (i.e., had MAIS score = 1 or 0).
Evaluation of safety errors and injury mechanisms
The likely injury mechanism and the significance of safety errors on the injury outcome for the involved young occupants were determined; that is, whether the injury severity might have been influenced by seatbelt use or misuse, MV crashworthiness, and the presence or absence of passive safety equipment in the case MV. A case-by-case review was performed to evaluate whether safety errors or the failure or absence of safety equipment might have contributed to the mechanism and the extent of injuries.
We defined that an occupant was unrestrained if they were not using any part of the seatbelt. Any incorrect use of the seatbelt (e.g., incorrect routing of the seatbelt under an arm or behind the back, improper twisting of the seatbelt, seatbelt being too loose across the hip or shoulder, or use of a lap belt only) were classified as seatbelt misuse. Improper sitting posture was classified as occupants sitting with their legs on the dashboard, leaning backward or forward while asleep, or having the headrest too low relative to the neck.
The presence of any insecure objects regarded as a potential safety hazard, including unrestrained fellow occupants, was also registered.
Toxicology
We obtained information on consumption of alcohol, medicinal and illicit drugs from hospital records or police reports. Unfortunately, blood tests were not performed consistently. However, medical records included health care takers’ description of observed behavior that indicated obvious signs of alcohol consumption or drug influence, which then lead to suspicion of impairment without blood toxicology. The legal limit for the blood alcohol concentration (BAC) in Norway was reduced from 0.5 to 0.2 g/kg in 2001. In 2012, Norway also introduced per se limits equivalent of BAC of 0.2 g/kg and 0.5 g/kg for 20 nonalcohol drugs [11]. We chose a threshold level for likely impairment of BAC of ≥ 0.5 g/kg for alcohol, and concentrations equivalent to a BAC of ≥ 0.5 for g/kg for psychoactive medicinal substances or illicit drugs. In cases where medical records clearly indicated obvious signs of alcohol consumption or drug influence, but no blood sample was collected, a BAC ≥ 0.5 g/kg for alcohol or equivalent to BAC ≥ 0.5 g/kg for nonalcohol drugs was assumed.
Data analyses
The independent Student’s t-test was used to evaluate differences in continuous variables according to the mean ΔV and collision-related characteristics and types of injuries.
We used a generalized estimation equation (GEE) to investigate the effects of possible explanatory variables (categorical and continuous) on the dependent variable of MAIS score ≥2 injuries (yes/no). The case MVs were entered as the subjects in the data set, and the occupant’s identifiers as within-subjects to adjust for possible intra-MV correlations. An exchangeable correlation structure was used in which constant correlations between any two observations within the MV were assumed. Univariable analyses were first performed to determine the effect of each explanatory variable on MAIS score ≥2 injuries, and we recorded those that had a significance level below 5%.
Variables with a significance level below 10% were entered into the multivariable GEE model to investigate their combined effect on MAIS score ≥2 injuries. The quasilikelihood information (QIC) criterion was used to select the model that provided the best fit to the data [12]; that is, the model with the lowest QIC value. We removed the variable with the weakest association in each analysis, and the calculations were rerun until all remaining explanatory variables were statistically significant. Variables that did not significantly predict the outcome were excluded from the final model.
Odds ratios (ORs) were used to explain the importance of the predictor variables; that is, estimating an occupant’s odds of having an MAIS score ≥2 injury. Estimates of the OR were obtained from the final model, and confidence intervals (CIs) were calculated for all OR values. An OR > 1 indicated a higher likelihood of an MAIS score ≥2 injury. All statistical analyses were performed using SPSS statistical software (version 25.0, IBM Corporation, Armonk, NY).
Ethics
This study was approved by the Regional Committee for Medical and Health Research Ethics and the Norwegian Prosecuting Authority. Informed consent was obtained from all cases studied or their next of kin.
Results
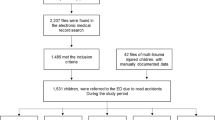
During the 3-year study period, we registered 273 occupants involved in high-energy MVCs. Twenty-eight cases (including 15 fatalities) were omitted since we did not obtain their consent to participate, and an additional 16 cases were excluded due to insufficient information on injury outcome, as outlined in Fig. 1.

Outline of the study. MAIS, Maximum Abbreviated Injury Scale
The demographics of the 229 finally included occupants are presented in Table 1. The median age of the included occupants was 19 years (interquartile range [IQR] = 18–21 years), and 66% (150/229) of them were male. Eight were treated at outpatient clinics only and 221 young adults were admitted to hospital. In total, 111 occupants (48%) sustained 1 or more MAIS score ≥2 injuries in the following body regions: 52 (47%) in the head/face/neck, 59 (53%) in the chest, 33 (30%) in the abdomen, 30 (27%) in the upper extremities, and 42 (37%) in the lower extremities. MAIS score ≥ 3 injuries were observed in 69 cases, and there were 22 fatalities.
The characteristics of the 145 case MVs and the collision-related circumstances are presented in Table 2. Most of the collisions occurred in rural areas (92%), on roads without a barrier between the opposing lanes (98%), and involved passenger cars (85%). Single-MV collision represented more than half of the cases (66%). The median speed for the case MVs at the time of the collision was 80 km/h (IQR = 60–100 km/h), and the median ΔV was 51 km/h (IQR = 39–68 km/h).
Safety errors or missing standard safety equipment that most likely contributed to the injuries were detected in 59% (65/111) of the occupants with MAIS score ≥2 injuries (Fig. 2). These 65 case characteristics and safety errors observed are described in detail in the Appendix, in Supplementary Tables 1, 2, 3, 4, and 5. In 33 cases, the occupant had been completely unrestrained, thereby exposing them to severe impacts with parts of the MV interior or other occupants, or to being ejected from the MV. There was evidence of a reclined sitting position/occupant posture or seatbelt misuse in 13 cases: 7 with the shoulder part of the seatbelt not in contact with the occupant due to seat back being in an excessively reclined position or the occupant sitting in a slouched position (e.g., sleeping), 5 with the shoulder part of the seatbelt being incorrectly routed under the arm, and 1 with the lap belt being too high over the abdomen. Insecure cargo resulted in secondary impacts to six occupants, and two were impacted by an unrestrained fellow occupant. In 11 cases, the lack of airbag protection was probably of significance, since these occupants all sustained head or neck injuries due to impacting side doors or pillars, which could have been prevented by deploying side airbags or side curtain airbags. Figures 3, 4, 5, 6, 7, 8, and 9 demonstrate safety errors revealed after reconstructions of occupant’s movements inside the MV during the collision.

Distribution of safety errors considered contributory to the injury outcome in the 111 occupants with Maximum Abbreviated Injury Scale (MAIS) score ≥2. Safety errors or inadequate occupant protection were observed in 59% (65/111) of the occupants with MAIS score ≥2 injuries, as described in detail in the Appendix (Supplementary Tables 1, 2, 3, 4, and 5). A high proportion of occupants with MAIS score 5 and 6 were either unrestrained, misused seat belts or driving old vehicles with inadequate protection. The proportion of various safety errors according to each MAIS score group was not significantly different

Reconstruction of injury mechanism for front-seat passenger and right rear-seat passenger involved a collision. The main impact was to the right front of the MV. Unrestrained front-seat and unrestrained rear-seat passenger. In addition to no seatbelt use, the forward movement of the rear-seat passenger displaced the front-seat passenger’s seat back forward, thereby increasing the forward momentum and impact load. Injuries: The front-seat passenger sustained fatal head injuries after impact with the windshield/A-pillar and chest injuries after impact with the dashboard

Reconstruction of injury mechanism for driver involved in a fatal rollover incident (a). Unrestrained driver was ejected through the side door window during the rollover incident, and the head squeezed between the car roof and the ground. Injury: Fatal head trauma (b)

Reconstruction of the injury mechanism for front-seat passenger involved in a collision. The main impact was to the left front of the MV. Seatbelt misuse due to improper occupant posture relative to seatbelt. The seatbelt did not tighten effectively across the occupant’s torso during the collision (a). The shoulder part of the seatbelt was too loose due to an overly reclined seat back that allowed for excessive movement of the head and torso forward and to the left (b), contributing to direct contact with the driver/driver’s seat back. Injuries: Traumatic head injury (DAI grade 3) and subdural hemorrhage

Reconstruction of injury mechanism for right rear-seat passenger involved in a frontal collision. Seatbelt misuse due to incorrect routing of the seatbelt and improper occupant posture relative to the seatbelt. The shoulder part seatbelt was routed under the right arm and the lap belt was too high over the abdomen (a). Moreover, the occupant’s legs were on top of luggage placed on the floor behind the rear seat back. The frontal collision caused excessive seatbelt loading directly on abdomen and the right part of the torso (b). Injuries: Decollement of abdominal wall, rupture of the diaphragm, herniation and laceration of the gastric ventricle and intestines, bilateral lung contusions, spleen rupture, and major liver injury

Reconstruction of injury mechanism for left rear-seat passenger involved in a fatal nearside collision (a). Seatbelt misuse due to incorrect routing of the shoulder part of the seatbelt under the left arm that allowed for excessive forward movement of the head (b) and torso and direct contact with the driver’s seat back. Insecure cargo in the trunk displaced the rear seatback >20 cm forwards, and increased the seatbelt loading on the torso. Injuries: Bruising and abrasion suggestive of seatbelt mark b) (c) was found under the left arm, as well as mandibular fracture, fatal traumatic brain injury, traumatic subarachnoid hemorrhage, C1-fracture, multiple rib fractures, and a major spleen rupture

Reconstruction of injury mechanism for left rear-seat passenger involved in a frontal collision. Seatbelt misuse due to incorrect routing of the seatbelt behind the back (a) allowing for excessive forward movement of the head and torso and direct contact with the driver seat back, displacing it >10 cm forward (b). Injuries: Luckily, only minor head contusion and lung contusions

Evidence of insecure heavy cargo in the trunk displacing the rear-seat row forwards in a frontal collision. Luckily, no occupants were sitting in the rear-seat row during the collision
The multivariable analysis (Table 3) revealed that independent factors for severe injury were related to the occupants, the road environment, and the collision type. The occupant-type and environment-type factors associated with MAIS score ≥2 injuries included not using a seatbelt (OR = 3.28, p = 0.009), driving under the influence of alcohol or drugs (DUI) (OR = 2.94, p = 0.026), nighttime driving (OR = 2.41, p = 0.027), and poor road lighting (OR = 2.50, p = 0.043). The collision-type factors associated with MAIS score ≥2 injuries were primary side impacts (OR = 3.38, p = 0.015), heavy collision partner (OR = 5.78, p = 0.035), and MV deformation (OR = 1.04 for each centimeter increase in deformation, p < 0.001). The speed at impact and ΔV were both associated with MAIS score ≥2 injuries in the univariable analysis, but did not reach significance in the multivariable model, which was attributable to the correlation with the extent of the MV deformation.
Discussion
This study has documented that safety errors and missing safety equipment in the MVs were present in 59% of the cases when young adults sustained MAIS score ≥2 injuries on Norwegian roads. In addition, it was found that many of the injuries and several fatalities could have been prevented by properly restraining and protecting the occupants using airbags.
A high-energy MVC results in the abrupt deceleration and deformation of the MV, exposing the occupants to a diversity of motions and potential impacts. Severe occupant injuries are almost invariably the result of direct contact to the head or chest. The occupant commonly makes contact with certain parts of the MV interior, such as the windshield, roof, or steering wheel. In some cases, the occupant will receive secondary impacts from moving objects within the MV [13]. The complexity of these movements needs to be considered when assessing the effects of various safety measures. Very occasionally there are reports of unrestrained occupants involved in extremely high-energy MVCs who miraculously survive, sometimes even being able to leave the crash scene without any significant injuries. The protective role of seatbelt use against the risk of most major injuries is well established [14], since this often prevents occupants from being thrown into MV structures or completely ejected from the MV [15]. A meta-analysis of 24 studies from 2000 onward found that seatbelt use can reduce fatal and nonfatal injuries the front-seat occupants by 60%, and fatal and nonfatal injuries in rear-seat occupants by 44% [16].
The present study has revealed that a considerable proportion (33/111, 30%) of the young adults who died or were severely injured were not using a seatbelt. The nine fatalities among these all sustained crush injuries due to impacts to the head or chest. The investigations performed in each case showed that a correctly restrained occupant most likely would have survived the impacts, since there was sufficient space to avoid impacts within the MV. We observed that the risk of MAIS score ≥2 injuries was 3.3-fold higher for unrestrained than restrained young adult occupants, after adjusting for other collision-related factors. This analysis also identified that several unrestrained occupants were fortunate to avoid severe injuries.
Why do young adults continue to drive unrestrained? A report from the World Health Organization suggested they do not use seatbelts for reasons such as the driving trip being short, simply forgetting, or being in a hurry [15]. Bad habits and misunderstanding of the safety effects of seatbelts have also been reported [15, 17, 18]. To complicate matters, young adults (and particularly males) have higher crash rates than other age groups [19], which has led to the increased crash risk being attributed to factors such as brain immaturity, susceptibility to high-risk driving behaviors (e.g., speeding), short driving experience, and DUI [2, 9, 20, 21].
DUI was associated with an almost threefold higher risk of severe injuries. Additionally, nighttime driving and driving on dark roads were independent risk factors for injuries with an MAIS score ≥2. Young adult drivers and passengers commonly combine alcohol consumption with reckless driving, speeding, and not using a seatbelt, which is why they have a higher risk of collisions and injuries during nighttime [7, 9, 20, 21]. Williams also suggested that late-night driving increased the crash risk due to driving being more difficult in darkness, particularly for newly licensed drivers [22]. Public transport is scarce at nighttime in rural areas of Norway, leading young people to drive more for social purposes or for pleasure. Possible preventive measures might include restricting young drivers to certain times of the day or, in particular, certain days of the week. Restrictions on nighttime driving and driving with peer teenage passengers have become part of graduated licensing systems in the USA [23] and New Zealand, and they are showing positive effects [7]. An alternative strategy has shown promising results in Norway, where instead of a graduated licensing system, the age limit for supervised practice is 16 years while the licensing age is 18 years, which gives the learner driver an opportunity to acquire more driving experience before being allowed to drive on their own [24]. Moreover, the especially strict Norwegian penalty point system for young drivers (who are punished with double the number of points in the first 2 years after they have obtained their driving license compared with older drivers) has showed promising results in reducing the risk of injury for young adult MV occupants [25].
The multivariable analysis also revealed associations of MAIS score ≥2 injuries with side impacts and MV deformation. Examinations of the MV interiors revealed that the following elements increased the injury severity during side impacts: improper sitting position, insecure cargo or fellow occupants, not using a seatbelt, improperly tightened shoulder part of the seatbelt, and lack of side airbags and side curtain airbags. Moreover, a reclined sitting position at the time of collision suggested that the occupant was not sitting optimally in relation to the door and B-pillar, resulting in the protective effect of side airbags being suboptimal, as described by previously by others [26].
If the shoulder part of the seatbelt is too loose, it will not tighten effectively across the occupant’s torso during a side impact, increasing the risk of excessive body movements and occupant-to-occupant injury. In two cases, we suspected an injury mechanism where the young adult occupant was injured by the intruding structure but also injured by contact with the adjacent occupant in the same seating row who had their shoulder part of the seatbelt too loose. Both Siegel et al. and Hillary et al. suggested an association between side impacts and increased injury severity [27, 28]. Compared with frontal impacts, seatbelts provide reduced protection in side impacts [29, 30], and occupant-to-occupant contact injuries are reportedly more prevalent [31]. Newland et al. also suggested that occupant-to-occupant injury is probably underreported since there is often little evidence in the MV available to investigators of impacts between two occupants. Those authors also demonstrated that drivers having a restrained front-seat passenger present during near-side impacts had an increased risk of MAIS score ≥ 3 injuries, with the risk further increasing if the passenger was not using a seatbelt [32].
The statistical analysis indicated that some variables were not independently predictive of the injury outcome. Some safety errors were present among both those with and without MAIS score ≥2 injuries, but the in-depth analysis still revealed that these errors had detrimental effects on occupant safety. Overall, misuse of seatbelts, unsafe seating positions, and insecure cargo were errors present for 18 occupants who suffered MAIS score ≥2 injuries. Six of them had the shoulder part of the seatbelt incorrectly routed under the arm, which during a collision increased the upper body and head movements and the pressure against the abdomen, resulting in severe head and abdominal injuries. Another six occupants with MAIS score ≥2 injuries had correctly routed seatbelts but overly reclined seat backs, in some cases where the seat back was nearly horizontal. We concluded that this seat-back position had significantly negative effects due to the seatbelt being loosely positioned across the body, thereby allowing excessive forward and sideways motions during rapid MV deceleration. All of the occupants directly impacted the MV interior. One-third of the occupant-related errors were insecure objects in the rear seat that either directly hit six of the drivers, or hit and displaced their seat backs, thereby increasing the seatbelt loading and occupant injuries.
Furthermore, we found that in 13 cases the MVs were older passenger cars lacking side airbags and side curtain airbags, which probably contributed to the injury severity in side impacts. Such airbags help mitigate impacts to the head, chest, abdomen, and pelvis since they provide coverage of the A-pillar, B-pillar, and side roof rail, and further serve as a containment barrier to prevent partial or complete ejection from the MV [33]. Moreover, older MVs also do not include modern crash-avoidance systems, and 81% of the MVs in the current study were older than 10 years. Høye [37] reported that older MVs in Norway are overrepresented in speeding and DUI crashes, and that male and young drivers are overrepresented in these types of crashes. Young adults are more likely to purchase older MVs since they are cheaper. Future government campaigns targeting young adults and parents should emphasize the importance of driving a modern MV equipped with adequate safety equipment. This should also include seatbelt reminders in the front and rear seats. Manufacturers should also be encouraged to equip their MVs with seatbelt interlock devices to prevent the vehicle from being started unless the occupants have fastened their seatbelts [34].
It is especially noteworthy that 89% of the MVCs occurred in rural areas in the present study. Previous research has also found higher rates of MVC fatalities in nonurban environments [35]. Possible contributory factors such as longer travel distances for rural drivers, more-lax attitudes toward MV safety measures, worse road safety (e.g., no barriers between opposing lanes), higher speed limits, greater alcohol consumption, and longer times to receive medical attention have been highlighted [35, 36].
Strengths and limitations
In-depth investigations of exterior and interior environments of the involved MVs provide far more information about occupant-related factors [37]. However, detailed multidisciplinary studies of real-world MVCs are challenging [9]. We were unable to confirm whether all of the occupants who received MAIS score ≥2 injuries were admitted to hospitals, although we consider this highly likely since occupants with serious injuries would be transported to a hospital, in which case we would have been alerted. One major strength of this study was that experienced collision investigators systematically and prospectively performed the on-scene collection of collision data.
Data obtained from various sources were compared and reviewed by a multidisciplinary team, including assessing seatbelt use or misuse at the time of the collision and the potential severity of other safety errors. The in-depth analyses, photographs, reconstructions of each occupant’s movements inside the MV, and knowledge about the occupants’ injuries provided us with essential detailed data on the factors relevant to MVCs for determining the injury mechanisms. To reduce errors and irregular assessments, data obtained from different sources were compared and reviewed by the same multidisciplinary team. Moreover, data were collected by the same collision investigators, and injury severity scoring was performed in a uniform manner, which should also have reduced the interrater variability. We consider this approach superior to utilizing existing databases.
The small sample of injured occupants with seatbelt misuse, driving with a reclined seat back, or the lack of protective side airbags or side curtain airbags is probably a limitation for identifying these factors as being associated with MAIS score ≥2 injuries. However, the design of the study made us to discover that the injury consequences of such safety errors were severe, and sometimes life threatening.
One limitation of this study is that information about speed and DUI is not always based on exact measurements, and not all occupants involved in the included MVCs were tested for alcohol and drugs. The prevalence of DUI may therefore have been underestimated.
Conclusion
This study has provided a detailed description of MVCs involving young adult MV occupants, and documented that safety errors and missing safety equipment in the MVs were present in 59% of the cases when the occupants sustained MAIS score ≥2 injuries on Norwegian roads. Our results show that these safety errors are easily avoidable and hence that the ambition of zero young people being killed or seriously injured in MVCs seems achievable. Future work should continue focusing on educational programs for young adults, promoting their awareness about correct seatbelt use, and underlining the importance of driving MVs with up-to-date active and passive safety equipment.
Alcohol consumption, high speeds, and nighttime driving continue to make significant contributions to injuries and fatalities. Future government campaigns should identify and specifically target young adult subgroups such as those who take extra risks or are sensation seekers or recidivist traffic violators. Restrictive measures such as MV impoundment, nonoverridable intelligent speed adaptation, and alcohol interlock devices may be promising measures in the future [37].
Key points
-
1.
The prevalence of young occupants not using a seatbelt continues to be high and has a negative impact on morbidity and mortality in a significant number of MVCs.
-
2.
Safety errors such as seatbelt misuse and improper sitting position are not uncommon and are likely to be an underestimated factor contributing to severe injuries.
-
3.
Most MVs driven by young adults are older and do not have adequate passive safety equipment.
Data availability
The data will not be deposited.
References
WHO. Global status report on road safety 2018. Geneva (Switzerland): World Health Organization; 2018. p. 2018.
McCartt AT, Mayhew DR, Braitman KA, Ferguson SA, Simpson HM. Effects of age and experience on young driver crashes: review of recent literature. Traffic Inj Prev. 2009;10(3):209–19.
Elvik R. Why some road safety problems are more difficult to solve than others. Accid Anal Prev. 2010;42(4):1089–96.
Regev S, Rolison JJ, Moutari S. Crash risk by driver age, gender, and time of day using a new exposure methodology. J Safety Res. 2018;66:131–40.
Statistics Norway. Road traffic accidents with sustained injuries 2000–2020 (Norwegian). 2020.
Norwegian Ministry of Transport and Communications. Report to the Parliament no. 33. National Transport Plan 2018–2029 (Norwegian). 2017.
Weiss HB, Kaplan S, Prato CG. Analysis of factors associated with injury severity in crashes involving young New Zealand drivers. Accid Anal Prev. 2014;65:142–55.
Skjerven-Martinsen M, Næss PA, Hansen TB, Gaarder C, Lereim I, Stray-Pedersen A. A prospective study of children aged <16 years in motor vehicle collisions in Norway: severe injuries are observed predominantly in older children and are associated with restraint misuse. Accid Anal Prev. 2014;73(21):151–62.
Breen JM, Næss PA, Hansen TB, Gaarder C, Stray-Pedersen A. Serious motor vehicle collisions involving young drivers on Norwegian roads 2013–2016: speeding and driver-related errors are the main challenge. Traffic Inj Prev. 2020;21:382–8.
Gennarelli TA, Wodzin E. Abbreviated injury scale (AIS 2005), Update 2008. Barrington, IL: Association for the Advancement of Automotive Medicine. 2008.
Vindenes V, Jordbru D, Knapskog A-B, Kvan E, Mathisrud G, Slørdal L, Mørland J. Impairment based legislative limits for driving under the influence of non-alcohol drugs in Norway. Forensic Sci Int. 2012;219(1–3):1–11.
Pan W. Akaike’s information criterion in generalized estimating equations. Biometrics. 2001;57(1):120–5.
Breen JM, Næss PA, Gaarder C, Stray-Pedersen A. Autopsy findings in drivers and passengers from fatal motor vehicle collisions: limited differences in injury patterns and toxicological test results. Forensic Sci Med Pathol. 2021;17:235–46.
Fouda Mbarga N, Abubakari A-R, Aminde LN, Morgan AR. Seatbelt use and risk of major injuries sustained by vehicle occupants during motor-vehicle crashes: a systematic review and meta-analysis of cohort studies. BMC Public Health. 2018;18(1):1413.
Toroyan T, Peden M. Youth and road safety. Geneva (Switzerland): World Health Organization; 2007.
Høye A. How would increasing seat belt use affect the number of killed or seriously injured light vehicle occupants? Accid Anal Prev. 2016;88:175–86.
Moe D, Nordtømme E, Øvstedal L, Roche-Cerasi I, Sakshaug K. Who are not using seatbelts, and what is the reason? Report no A12094 (Norwegian). Oslo: SINTEF; 2009.
Boakye KF, Khattak A, Everett J, Nambisan S. Correlates of front-seat passengers’ non-use of seatbelts at night. Accid Anal Prev. 2019;130:30–7.
Simons-Morton B, Lerner N, Singer J. The observed effects of teenage passengers on the risky driving behavior of teenage drivers. Accid Anal Prev. 2005;37(6):973–82.
Romer D, Lee Y-C, McDonald CC, Winstonet FK. Adolescence, attention allocation, and driving safety. J Adolesc Health. 2014;54(5 Suppl):S6-15.
Valen A, Bogstrand ST, Vindenes V, Frost J, Larsson M, Holtan A, Gjerde H. Driver-related risk factors of fatal road traffic crashes associated with alcohol or drug impairment. Accid Anal Prev. 2019;131:191–9.
Williams AF. Teenage drivers: patterns of risk. J Safety Res. 2003;34(1):5–15.
Ferguson SA, Teoh ER, McCartt AT. Progress in teenage crash risk during the last decade. J Safety Res. 2007;38(2):137–45.
Gregersen NP, Berg H-Y, Engström I, Nolén S, Nyberg A, Rimmö P-A. Sixteen years age limit for learner drivers in Sweden—an evaluation of safety effects. Accid Anal Prevn. 2000;32(1):25–35.
Bjørnskau T. Summary: road traffic risk in Norway 2017/18. Oslo: Institute of Transport Economics Norwegian Centre for Transport Research. Report no. 1782/2020. 2020.
Acierno S, Kaufman R, Rivara FP, Grossman DC, Mock C. Vehicle mismatch: injury patterns and severity. Accid Anal Prev. 2004;36(5):761–72.
Siegel JH, Mason-Gonzalez S, Dischinger P, Cushing B, Read K, Robinson R, Smialek J, Heatfield B, Hill W, Bents F, et al. Safety belt restraints and compartment intrusions in frontal and lateral motor vehicle crashes: mechanisms of injuries, complications, and acute care costs. J Trauma. 1993;34(5):736–58; discussion 758–9.
Hillary FG, Schatz P, Moelter ST, Lowry JM, Ricker JH, Chute DL. Motor vehicle collision factors influence severity and type of TBI. Brain Inj. 2002;16(8):729–41.
Viano DC, Parenteau CS. Severe injury to near- and far-seated occupants in side impacts by crash severity and belt use. Traffic Inj Prev. 2010;11(1):69–78.
Abbas AK, Hefny AF, Abu-Zidan FM. Seatbelts and road traffic collision injuries. World J Emerg Surg. 2011;6(1):18.
Viano DC, Parenteau CS. Occupant-to-occupant contact injury in motor vehicle crashes. Traffic Inj Prev. 2017;18(7):744–7.
Newland C, Belcher T, Bostrom O, Gabler H, Cha J-G, Wong HL, Tylko S, Dal Nevo R. Occupant-to-occupant interaction and impact injury risk in side impact crashes. Stapp Car Crash J. 2008;52:327–47.
Viano DC, Parenteau CS. Injury risks in frontal crashes by delta V and body region with focus on head injuries in low-speed collisions. Traffic Inj Prev. 2010;11(4):382–90.
Febres JD, García-Herrero S, Herrera S, Gutiérrez JM, López-García JR, Mariscall MA. Influence of seat-belt use on the severity of injury in traffic accidents. Euro Transp Res Rev. 2020;12(1):9.
Bakke HK, García-Herrero S, Herrera S, Gutiérrez JM, López-García JR, Mariscal MA. Fatal injury as a function of rurality-a tale of two Norwegian counties. Scand J Trauma, Resusc Emerg Med. 2013;21(1):14.
Zwerling C, Peek-Asa C, Whitten PS, Choi SW, Sprince NL, Jones MP. Fatal motor vehicle crashes in rural and urban areas: decomposing rates into contributing factors. Inj Prev. 2005;11(1):24–8.
Høye A. Speeding and impaired driving in fatal crashes-results from in-depth investigations. Traffic Inj Prev. 2020;21(7):425–30.
Acknowledgements
The authors thank the participants and their guardians for volunteering to participate in this study at a time of great hardship, the valuable cooperation of the regional EMCCs (Oslo/Akershus, Innlandet, Drammen, Kristiansand, and Tønsberg) and the police districts of southeastern Norway, Kim Ankersten and Geir Engely for data collection.
Funding
Open access funding provided by University of Oslo (incl Oslo University Hospital). The authors acknowledge financial support from the Gjensidige Foundation (grant number 1022396) and the Norwegian Ministry of Transport and Communication (grant number 11/1950). These funders had no role in the design and conduct of the study, the collection, analysis, and interpretation of the data, or in the preparation, review, and approval of the manuscript.
Author information
Authors and Affiliations
Contributions
Jan Mario Breen: conceptualization, methodology, investigation, formal analysis, data curation, writing—original draft, visualization. Pål Aksel Næss: conceptualization, methodology, investigation, writing—review and editing. Trond Boye Hansen: conceptualization, methodology, investigation. Christine Gaarder: conceptualization, methodology, investigation, writing—review and editing. Harald Klemmetsen: software development, formal analysis. Arne Stray-Pedersen: conceptualization, methodology, investigation, formal analysis, data curation, validation, writing—original draft, visualization, supervision, project administration, funding acquisition.
Corresponding author
Ethics declarations
Ethics approval
This study of cases was approved by the Regional Committee for Medical and Health Research Ethics, the Data Protection Official for Research, and the Higher Prosecution Authority of Norway.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Breen, J.M., Næss, P.A., Hansen, T.B. et al. Young adults in motor vehicle collisions in Norway: user safety errors observed in majority of cases with severe or fatal injuries. Forensic Sci Med Pathol 18, 456–469 (2022). https://doi.org/10.1007/s12024-022-00541-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12024-022-00541-x