
Abstract
Scrotal elephantiasis is a rare form of lymphedema of the scrotum. Its pathophysiology is diverse and often not clear, as there are only a few diagnostic tools available. Primary therapy consists, as usual for lymphedema, of conservative measures. However, due to anatomical and physiological findings, conservative therapy options are not always applicable. Although the only possible therapy in severe cases is the surgical resection, there is a lack in the literature regarding a standardized surgical approach. Surgical treatment of massive scrotal elephantiasis was performed in two patients according to a standardized strategy. After computed tomography and planning the operation, the penis and testicles were first exposed. Then, the reduction of the scrotum was performed, by holding the lateral flaps to the contralateral side and setting the cutoff line to the center. The cranial flap was decreased as in a modified abdominoplasty. After surgical treatment following the standardized approach, both patients showed functionally and esthetically positive results. Scrotal elephantiasis has a huge impact on life quality of the affected patients. With the described combination of intense conservative therapy and a standardized surgical procedure, these challenging patients can be helped.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Scrotal elephantiasis is a rare form of lymphedema of the scrotum. The pathophysiology is diverse and often not clear, as there are only a few diagnostic tools available [1]. Disorders of the lymphatic system can lead to hypertrophy and hyperplasia of the connective tissue, with an inflammatory process becoming chronic [2]. The high hydrostatic pressure in lymphatic vessels, due to obesity, might lead to chronic lymphedema in these patients. Chronic lymphedema leads to fibrosis of the soft tissue in stadium III (elephantiasis). Primary therapy consists, as usual for lymphedema, of conservative measures [3,4,5,6]. However, due to anatomical and physiological findings, conservative therapy options are not always applicable [1, 7]. Often, the only possible therapy consists of surgical resection. However, conservative as well as surgical treatments of genital lymphedema are challenging and not yet fully standardized [7].
At the University Hospital Regensburg, two patients suffering from extreme scrotal elephantiasis presented within two months of each other in the consultation-hour for lymphedema. Obesity in both patients was seen as the trigger of secondary lymphedema of the scrotum (Fig. 1). Filarial involvement of penis (ramhorn penis) could be excluded. In addition to physical restrictions due to the volume and weight of the scrotum, the patients were both highly psychologically burdened. Both patients reported multiple infections in the past. Micturition was only possible through a fistula terminating at the bottom of the scrotum. Scrotal skin was papillomatous, thickened, and edematous. There was no urinary excoriation of the scrotal skin. Inguinal lymph nodes were clinically and sonographically unsuspicious. Testis could not be examined by sonography, as they were buried too deep for sonography. Hormone level was normal. Although both patients had constant conservative decongestion therapy in an ambulant setting for years, lymphedema was progressive. Before presentating in our clinic, both patients had stationary decongestion therapy for 4 weeks (Lympho Opt Fachklinik, Hohenstadt, Germany). Weight losses of 18.6 kg (patient 1) and 60 kg (patient 2) were reached by conservative treatment. An overview of the patients’ anamnestic and clinical data is shown in Table 1.

Both patients after decongestive therapy and before surgery. a Patient 1. b Patient 2
Patients and Methods
Before first introduction to our clinic, patients had a stationary decongestion therapy, where a substantially loss of weight could be reached by complex decongestive therapy. In order to rule out differential diagnoses, such as tumor or scrotal hernia, and for localization of the testicles and penis, a computed tomography (CT) was performed before surgery. Erythrocyte concentrates were provided, expecting high bleeding during the operation. The operation was performed under general anesthesia, with a team of two surgeons. The first step was to uncover the penis through an incision along the fistula guiding directly to the glans penis. From there, the testicles could be localized with a sterile ultrasonic probe and uncovered. The scrotum was then longitudinally split into two flaps. Thereby, big vessels occurred with large diameters that made multiple vessel ligations necessary. Funiculus spermaticus on both sides were completely revealed and spared. The reduction of the scrotum was performed by holding the lateral flaps to the contralateral side and setting the cutoff line to the center comparable to the approach in a breast reduction surgery (Fig. 2). The cranial flap was decreased like a modified abdominoplasty. Finally, a Y-shaped incision was made with the center lying at the root of the penis, as seen in Fig. 3.

Draft of the incision lines before resection

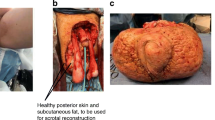
Different steps of operation. a Debulked penis and testes. b Wounds after resection of the scrotum. c Covering of the root of the penis with split skin. d Patient 1 after surgery. e Patient 2 after surgery. f Closed incision with negative pressure therapy (Prevena ® Incision management system, KCI, San Antonio, USA)
Due to the above process, a symmetrical scrotum could be reconstructed. Furthermore, both testicles could be saved, despite having strongly elongated spermatic cords. To avoid torsion, the spermatic cords were loosely enrolled without torque and fixed with absorbable sutures. The penis could be recovered by a micromesh skin graft with a thickness of 3/10 mm grafted from the upper leg. Skin closure was performed with non-resorbable monofile intracutaneous sutures. For better wound healing and wound hygiene, a closed incision negative pressure therapy (CINPT) was applied (Prevena® Incision Management System, KCI, San Antonio, USA) (Fig. 3).
Results
The combination of intense conservative therapy and the presented standardized surgical procedure led to functionally and esthetically positive results. A total scrotal weight reduction of 59 kg (19 kg conservative therapy and 40 kg surgical resection) for patient 1 and 57 kg (23 kg conservative therapy and 34 kg surgical resection) for patient 2 could be reached. Clinical data and histological findings are shown in Table 2. Patient 2 showed a postoperative superficial wound infection with Pseudomonas aeruginosa which was successfully treated with daily topical disinfection using hypochlorous acid (Granudacyn®, Mölnlycke, Germany). Both patients completed in-patient stay, fully mobilized, and were satisfied with their relief. Three months after therapy, no complications had occurred.
Discussion
The two patients discussed here had had a greatly reduced life quality and much suffering. Adequate mobility and personal hygiene had not been possible. Furthermore, pain and recurrent infections accompanied everyday life. Conservative therapy in an ambulant setting did not lead to disease regression. Due to intensive therapy in a stationary setting, a distinct weight loss of the scrotum was reached. However, both patients still suffered from a massive weight and volume excess. We therefore considered surgical treatment as the only option to release the patients of their burden. Surgical treatment can however lead to disastrous complications. Beside minor complications such as wound healing disorders and infections, there are major complications that must be discussed with the patient. Major complications could be the loss of the testes and epididymis or destruction of the penis. The loss of testes can lead to endocrinological failures. Infertility and lifetime hormone substitution could be the consequence. Destruction of the penis can occur due to infection or hypoperfusion [8]. The micromesh skin graft transferred to the penis could get contracture, making erections impossible. During the operation, hemostasis is very important, as huge amounts of tissue are removed. For veins of large diameters, this tissue removal may lead to major bleeding if damaged. The use of a cell saver and the provision of banked blood should therefore be considered. Due to possible postoperative hemodynamic instability, we recommend 48 h of monitoring at an intensive care or intermediate care unit. To avoid wound healing disorders and infections, CINPT should be applied to the wounds. These settings are quite expensive. If not used, wounds should be disinfected several times a day and kept dry. In these two patients, due to obesity, the inguinal wounds were buried under skin folds and were hard to be kept dry with gauze pads. To prevent edema or seroma, custom-made tight compression is recommended in the first 8 weeks.
During the inpatient stay, patients were consistently mobilized by physiotherapists from the first postoperative day on. Due to a lack of motivation on the patient side, mobilization was difficult. As both patients were obese, lifestyle changes, nutrition advice, and bariatric surgery were recommended.
Overall, these patients needed considerable energy and resources in postoperative care. Therefore, surgical treatment of such patients should be performed in hospitals in a stationary setting.
Conclusion
Scrotal elephantiasis has a huge impact on life quality of the affected patients. With the described combination of intense conservative therapy and a standardized surgical procedure, these challenging patients can be helped.
Data Availability
Not applicable.
References
Hara H, Mihara M (2017) Indocyanine green lymphographic and lymphoscintigraphic findings in genital lymphedema-genital pathway score. Lymphat Res Biol 15:356–359
Modolin M, Mitre AI, da Silva JC, Cintra W, Quagliano AP, Arap S, Ferreira MC (2006) Surgical treatment of lymphedema of the penis and scrotum. Clinics (Sao Paulo) 61:289–294
Dayes IS, Whelan TJ, Julian JA, Parpia S, Pritchard KI, D'Souza DP, Kligman L, Reise D, LeBlanc L, McNeely ML, Manchul L, Wiernikowski J, Levine MN (2013) Randomized trial of decongestive lymphatic therapy for the treatment of lymphedema in women with breast cancer. J Clin Oncol 31:3758–3763
C. Executive (2016) The diagnosis and treatment of peripheral lymphedema: 2016 consensus document of the International Society of Lymphology. Lymphology 49:170–184
Foldi E, Sauerwald A, Hennig B (2000) Effect of complex decongestive physiotherapy on gene expression for the inflammatory response in peripheral lymphedema. Lymphology 33:19–23
Keser I, Esmer M (2019) Does manual lymphatic drainage have any effect on pain threshold and tolerance of different body parts? Lymphat Res Biol 17:651–654
Yamamoto T, Koshima I, Yoshimatsu H, Narushima M, Miahara M, Iida T (2011) Simultaneous multi-site lymphaticovenular anastomoses for primary lower extremity and genital lymphoedema complicated with severe lymphorrhea. J Plast Reconstr Aesthet Surg 64:812–815
Thejeswi P, Prabhu S, Augustine AJ, Ram S (2012) Giant scrotal lymphoedema - a case report. Int J Surg Case Rep 3:269–271
Funding
Open Access funding provided by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Daniel Schiltz: wrote the article, involved in planning and performing the operations. Christoph Koch: helped writing the manuscript, involved in planning and performing the operations. Franz-Josef Schingale: Planned and performed the preoperative decongestive therapy. Lukas Prantl: revised the manuscript and helped planning the operations. Christian Taeger: Planned and performed the operations and revised the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Taeger is a consultant for Kinetic Concepts, Inc. The other authors have no financial interest to declare in relation to the content of the article.
Statement of Human and Animal Rights
All procedures performed in this report involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from every patient participating in this report.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schiltz, D., Koch, C., Schingale, FJ. et al. Reduction Scrotoplasty in 100 kg Scrotums. Indian J Surg 83, 562–566 (2021). https://doi.org/10.1007/s12262-020-02429-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12262-020-02429-y