
Abstract
Introduction
The safety and tolerability of nintedanib in patients with idiopathic pulmonary fibrosis (IPF) have been characterized using data from clinical trials.
Methods
We further characterized the safety and tolerability of nintedanib in patients with IPF in clinical practice using the global pharmacovigilance database. The database included spontaneously reported adverse events and data collected via solicited reporting in patients treated with nintedanib from 15 October 2014 to 15 October 2018. Adverse events were coded using the Medical Dictionary for Regulatory Activities. Cumulative exposure to nintedanib was estimated on the basis of sales data.
Results
Cumulative exposure to nintedanib was estimated as 60,107 patient-years. Diarrhea was the most frequent event (301.6 events per 1000 patient-years). Most (97.0%) diarrhea events were non-serious. The median (25th, 75th percentile) time to onset of the first diarrhea event was 60 (11, 182) days. Elevated liver enzyme or bilirubin levels were reported at a rate of 31.5 events per 1000 patient-years. Bleeding was reported at a rate of 36.8 events per 1000 patient-years; 81.0% of events were non-serious. Major cardiovascular adverse events were reported at a rate of 13.4 events per 1000 patient-years and myocardial infarction at a rate of 4.3 events per 1000 patient-years. Gastrointestinal perforation was reported at a rate of 1.0 event per 1000 patient-years.
Conclusions
On the basis of pharmacovigilance data collected over 4 years, the safety profile of nintedanib in patients with IPF was consistent with that observed in clinical trials and described in the product label, with no new safety concerns observed.
Graphical Abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out this study? |
We used data from Boehringer Ingelheim’s global pharmacovigilance program to study the safety and tolerability of nintedanib in patients with idiopathic pulmonary fibrosis (IPF), based on a larger and broader patient population and a longer follow-up period than was feasible to study in clinical trials |
What was learned from the study? |
Diarrhea was the most frequent adverse event, reported at a rate of 301.6 events per 1000 patient-years (lower than the rate observed in clinical trials); the median time to onset of the first diarrhea event was 60 days |
Rates of other adverse events of interest per 1000 patient-years were 31.5 for elevated liver enzyme or bilirubin levels, 36.8 for bleeding events, 13.4 for major adverse cardiovascular events and 4.3 for myocardial infarction; these rates were lower than those observed in clinical trials |
Our analyses suggest that the safety profile of nintedanib in patients with IPF in clinical practice is consistent with that described in the product label; no new safety concerns were observed in the global pharmacovigilance program |
Introduction
Idiopathic pulmonary fibrosis (IPF) is a progressive fibrosing interstitial lung disease associated with decline in lung function, symptoms including dyspnea and cough, impaired quality of life, and high mortality [1, 2]. Data from the European IPF Registry suggest that median life expectancy in patients with IPF not receiving antifibrotic therapy is approximately 5 years [3].
Nintedanib (Boehringer Ingelheim) is an approved treatment for IPF. In the phase II TOMORROW trial and the two phase III INPULSIS trials, nintedanib reduced the rate of decline in forced vital capacity (FVC) over 52 weeks by approximately 50% compared with placebo [4, 5]. In these trials, the adverse events associated with nintedanib were manageable for most patients and characterized predominantly by gastrointestinal events, particularly diarrhea [4, 5]. Data from the open-label extension of the INPULSIS trials, INPULSIS-ON, suggest that the safety and tolerability profile of nintedanib is maintained over long-term use (up to 68 months of treatment) [6].
While the most robust data on the safety and tolerability of a drug in a specific patient population are provided by randomized controlled trials, such trials are limited in their size and duration and tend to exclude patients with the most severe disease and certain comorbidities. Pharmacovigilance programs conducted following the approval of drugs collect safety and tolerability data from a larger and broader patient population and over a longer follow-up period [7, 8]. We used data from Boehringer Ingelheim’s global pharmacovigilance database for nintedanib in patients with IPF to characterize the safety and tolerability of nintedanib in clinical practice.
Methods
Data on adverse events in patients with IPF treated with nintedanib were collected via spontaneous reporting of adverse events and solicited reporting (e.g., through patient support programs). Data collected between 15 October 2014 (the date of the first approval of nintedanib as a treatment for IPF) and 15 October 2018 were included in the analyses. Post-authorization safety data from Japan were excluded as these will be reported separately.
Adverse events were coded using preferred terms in the Medical Dictionary for Regulatory Activities (MedDRA) version 21.0. In the MedDRA, preferred terms are distinct descriptors for a single medical concept; system organ classes are specific groupings by etiology or anatomy; and standardized MedDRA queries (SMQs) are standard sets of preferred terms that relate to a medical condition or area of interest. SMQs can be based on narrow or broad terms; narrow terms are those that are highly likely to represent the condition of interest. Serious adverse events were defined as events that resulted in death, were life-threatening, resulted in hospitalization or prolonged hospitalization, resulted in persistent or clinically significant disability or incapacity, were a congenital anomaly or birth defect, or were deemed serious for any other reason.
On the basis of the mechanism of action of nintedanib [9, 10] and data from clinical trials [4, 5], the following were defined as adverse events of special interest: diarrhea (MedDRA preferred term), liver enzyme and bilirubin elevations including drug-induced liver injury (based on the SMQs “drug related hepatic disorders” [narrow terms] and “liver related investigations, signs and symptoms” [broad terms]), bleeding (based on the SMQ “hemorrhage terms [excluding laboratory terms]” [narrow terms]), major cardiovascular adverse events (MACE; based on fatal adverse events in the MedDRA system organ classes “cardiac disorders” and “vascular disorders”; the SMQ “myocardial infarction” [broad terms]; a list of MedDRA preferred terms for stroke; and the MedDRA preferred terms “sudden death”, “cardiac death” and “sudden cardiac death”), myocardial infarction (based on the SMQ “myocardial infarction” [narrow terms]), and gastrointestinal perforation (based on the SMQ “gastrointestinal perforation” [narrow terms]). Bleeding adverse events were assessed in subgroups of patients by use of medication altering hemostasis (yes/no), as defined by the World Health Organization Anatomical Therapeutic Chemical group “antithrombotic agents”.
Cumulative exposure to nintedanib was estimated on the basis of sales data. Incidence rates of adverse events of special interest in the global pharmacovigilance database and in the INPULSIS trials were calculated as the number of patients with the event divided by the time at risk, expressed per 1000 patient-years. Analyses were based on observed cases and were descriptive. This study did not require institutional review board (IRB) approval as it was based on aggregate, patient de-identified data from a pharmacovigilance database.
Results
On the basis of sales data, the cumulative exposure to nintedanib over the study period was estimated to be 60,107 patient-years.
Diarrhea
Diarrhea was reported at a rate of 301.6 events per 1000 patient-years (Fig. 1). This is lower than the rate described in the INPULSIS trials (1331 events per 1000 patient-years). For most patients (97.9%), the reported events came from solicited rather than spontaneous reporting. Most diarrhea events (97.0%) were non-serious. Among the patients with diarrhea, 6181 (34.1%) reported more than one episode. The median (25th, 75th percentile) time to onset of the first diarrhea event was 60 (11, 182) days.

Incidence rates of adverse events of special interest in the global pharmacovigilance database
Liver Enzyme and Bilirubin Elevations
Elevated liver enzyme or bilirubin levels were reported at a rate of 31.5 events per 1000 patient-years (Fig. 1). This is lower than the rate reported in the INPULSIS trials (162 events per 1000 patient-years). Alanine aminotransferase (ALT), aspartate aminotransferase (AST), and bilirubin levels among patients who had elevations are summarized in Table 1. Of 10 cases with sufficient data to enable categorization of Hy’s law (i.e., ALT and/or AST > 3 × upper limit of normal [ULN] with concurrent total bilirubin > 2 × ULN), none met criteria for Hy’s Law. The median (25th, 75th percentile) time to onset of the first liver enzyme or bilirubin elevation was 60 (29, 136) days.
Bleeding
Bleeding was reported at a rate of 36.8 events per 1000 patient-years (Fig. 1). This is lower than the rate reported in the INPULSIS trials (118 events per 1000 patient-years). For most patients (98.1%), the reported events came from solicited rather than spontaneous reporting. Most bleeding events (81.0%) were non-serious. The median (25th, 75th percentile) time to onset of the first bleeding event was 68 (28, 193) days. The most frequently reported locations of bleeding were respiratory (31.7% of events) and lower gastrointestinal (24.2% of events) (Fig. 2). The most frequently reported types of bleeding event were epistaxis (25.0% of events), contusion (14.4% of events), hematochezia (11.6% of events), and rectal hemorrhage (7.2% of events).

Location of bleeding events in the global pharmacovigilance database
Among the patients with bleeding events, 28.1% were receiving medication altering hemostasis. There were no major differences in the types of bleeding events between patients receiving and not receiving medications altering hemostasis; however, serious bleeding events were more common than non-serious bleeding events in patients receiving such medications, whereas non-serious bleeding events were more common than serious bleeding events in patients not receiving such medications (Table 2).
MACE and Myocardial Infarction
MACE was reported at a rate of 13.4 events per 1000 patient-years (Fig. 1). This was lower than the rate reported in the INPULSIS trials (39 events per 1000 patient-years). For most patients (96.5%), the reported events came from solicited rather than spontaneous reporting. The median (25th, 75th percentile) age at first MACE was 75 (70, 80) years and 69.8% of patients who had MACE were male. The most frequently reported comorbid conditions in patients with MACE were hypertension (8.6% of patients), drug hypersensitivity (5.5% of patients), and coronary artery disease (5.2% of patients) (Fig. 3). Myocardial infarction was reported at a rate of 4.3 events per 1000 patient-years (Fig. 1). This was lower than the rate of myocardial infarction reported in the INPULSIS trials (17 events per 1000 patient-years).

Comorbid conditions in patients with MACE in the global pharmacovigilance database
Gastrointestinal Perforation
Gastrointestinal perforation was reported at a rate of 1.0 event per 1000 patient-years (Fig. 1). This was lower than the rate reported in the INPULSIS trials (3.4 events per 1000 patient-years) (Boehringer Ingelheim, data on file). For most patients (94.9%), the reported events came from solicited rather than spontaneous reporting. The median (25th, 75th percentile) age at first gastrointestinal perforation was 75 (68, 79) years and 61.0% of patients who had gastrointestinal perforation were male. The most frequently reported types of gastrointestinal perforation were intestinal (17.5% of events), gastric (11.1% of events), and perforation of the large intestine (9.5% of events).
Discussion
On the basis of global pharmacovigilance data collected over 4 years, the safety profile of nintedanib in patients with IPF was consistent with that observed in clinical trials, with no new safety concerns observed. The most frequent adverse event reported in the global pharmacovigilance database was non-serious diarrhea, in line with observations from clinical trials [5, 11,12,13,14], observational studies conducted in clinical practice [15,16,17,18,19,20,21,22,23], and post-marketing surveillance data collected in the USA in the year following the approval of nintedanib as a treatment for IPF [24].
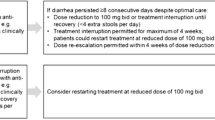
Nintedanib is an intracellular inhibitor of tyrosine kinases that inhibits processes fundamental to the pathogenesis of pulmonary fibrosis [9, 10, 25, 26]. Diarrhea is a known adverse event associated with tyrosine kinase inhibitors. The precise mechanism behind this is unknown, but it may be that inhibition of the vascular endothelial growth factor receptor (VEGFR) causes morphometric changes in the bowel mucosa, altering motility [27]. In the INPULSIS trials, 62.4% of nintedanib-treated patients had at least one adverse event of diarrhea over 52 weeks, with its onset occurring within 3 months in most of these patients [11]. Investigators were provided with guidelines for the management of diarrhea through symptomatic therapy and dose adjustment (dose reduction to 100 mg twice daily and/or treatment interruption) [11]. Diarrhea led to treatment discontinuation in 4.4% of patients over 52 weeks [11].
Elevations in liver enzymes and bilirubin (including drug-induced liver injury) may occur in patients treated with nintedanib and it is recommended that liver function tests (ALT, AST, bilirubin) be conducted prior to the initiation of treatment, at regular intervals during the first 3 months of treatment, and periodically thereafter or as clinically indicated [28]. It is recommended that nintedanib therapy be interrupted or the dose reduced in patients with ALT or AST > 3 but < 5 × ULN without signs of liver damage [28]. Nintedanib should be discontinued in patients with ALT or AST > 3 × ULN with signs or symptoms of liver injury, or with ALT or AST > 5 × ULN [28]. In the majority of cases, liver enzyme and bilirubin elevations in patients treated with nintedanib were reversible with treatment interruption or dose reduction [28].
As an inhibitor of VEGFR, nintedanib is associated with an increased risk of bleeding. It is recommended that patients treated with nintedanib who are on full-dose anticoagulation therapy be monitored so that anticoagulation treatment can be adjusted as necessary [28]. Consistent with findings from the INPULSIS trials [11], most of the bleeding events in the pharmacovigilance database were non-serious and the most common type of bleeding event was epistaxis. Clinical trial data, including those collected in INPULSIS-ON over a treatment duration of up to 68 months, suggest that the risk of bleeding does not increase with prolonged nintedanib treatment [6, 14]. However, patients with increased risk of bleeding (i.e., requiring fibrinolysis, full-dose therapeutic anticoagulation, or high-dose antiplatelet therapy) were excluded from clinical trials of nintedanib. Just over a quarter of patients who had a bleeding event reported in the pharmacovigilance database were receiving medications that alter hemostasis, i.e., antithrombotic agents. Although the dose of these medications was not reported and, as such, use of full-dose therapeutic anticoagulation or high-dose antiplatelet therapy could not be assessed, the types of bleeding event were generally consistent between patients who were and were not receiving these medications. However, serious bleeding events were more common than non-serious bleeding events in patients receiving medications altering hemostasis, whereas non-serious bleeding events were more common than serious events in patients not receiving such medication.
Cardiovascular disorders are common comorbidities in patients with IPF [29]. In the INPULSIS trials, a higher proportion of patients in the nintedanib group than in the placebo group had myocardial infarction (2.7% versus 1.2%), while a lower proportion had other ischemic heart disease (1.7% versus 3.1%) [11]. The incidence rates of MACE and myocardial infarction in the global pharmacovigilance database were lower than those observed in pooled data from the TOMORROW and INPULSIS trials [30]. The incidence rate of myocardial infarction in the database was lower than that observed in an analysis of US healthcare claims data from patients with IPF not treated with nintedanib [31]. Exposure-adjusted event rates of MACE and myocardial infarction in nintedanib-treated patients in INPULSIS-ON (after a median of 32 months of treatment) were similar to those observed in placebo-treated patients in the INPULSIS trials [6]. Overall, these data are reassuring with regards to the cardiovascular safety of nintedanib in patients with IPF.
A small number of patients in the INPULSIS trials and global pharmacovigilance database had gastrointestinal perforation. On the basis of the mechanism of action of nintedanib, caution should be used when treating patients who have had recent abdominal surgery, have a history of diverticular disease, or are receiving corticosteroids or non-steroidal anti-inflammatory drugs. A recent analysis of real-world data suggested that there may be a relationship between nintedanib and ischemic colitis (based on analysis of 10 cases) [32]. A signal assessment for ischemic colitis conducted using the global pharmacovigilance database in early 2020 identified 18 cases following 102,711 patient-years of exposure, a rate consistent with the background rate that would be expected in a population of similar age.
Clinical trial data suggest that nintedanib has a similar safety and tolerability profile across patient subgroups based on age, race, degree of lung function impairment, and use of statins and anti-acid medications [6, 12, 33,34,35]. However, serious adverse events appear to occur more frequently in patients with IPF who have more advanced gas exchange impairment (DLco < 35% predicted) [36]. In addition, observational studies conducted in clinical practice suggest that patients with more advanced disease are more likely to discontinue nintedanib because of adverse events [20, 21, 37]. Proactive counselling regarding possible adverse events and appropriate management through dose adjustment and symptom relief are crucial to optimize adherence and to improve outcomes [38, 39]. Importantly, the dose adjustments used to manage adverse events associated with nintedanib have been shown not to reduce the efficacy of nintedanib in reducing FVC decline [6, 40].
Strengths of our analyses of the global pharmacovigilance database include the cumulative exposure to nintedanib (over 60,000 patient-years compared with 548 patient-years in the INPULSIS trials) and the collection of data from an all-comers population of patients with IPF treated in clinical practice worldwide. Our analyses also have a number of limitations, including the likely under-reporting of non-serious adverse events, the reliance on the data that were reported without the opportunity to verify them, the lack of detailed information captured on adverse events and their impact, the absence of information on nintedanib dose adjustments or discontinuations, and the limited data available on the characteristics of patients who reported adverse events, including on concomitant medication use.
Conclusions
We used data from the global pharmacovigilance database for nintedanib in patients with IPF to characterize the safety and tolerability of nintedanib in clinical practice. On the basis of data collected over 4 years, the safety profile of nintedanib in patients with IPF was consistent with that observed in clinical trials and described in the product label, with no new safety concerns observed. The most frequently reported adverse event in the global pharmacovigilance database was non-serious diarrhea.
References
Raghu G, Remy-Jardin M, Myers JL, et al. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198(5):e44–68.
Kreuter M, Swigris J, Pittrow D, et al. The clinical course of idiopathic pulmonary fibrosis and its association to quality of life over time: longitudinal data from the INSIGHTS-IPF registry. Respir Res. 2019;20(1):59.
Guenther A, Krauss E, Tello S, et al. The European IPF registry (eurIPFreg): baseline characteristics and survival of patients with idiopathic pulmonary fibrosis. Respir Res. 2018;19(1):141.
Richeldi L, Costabel U, Selman M, et al. Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. N Engl J Med. 2011;365(12):1079–87.
Richeldi L, du Bois RM, Raghu G, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370(22):2071–82.
Crestani B, Huggins JT, Kaye M, et al. Long-term safety and tolerability of nintedanib in patients with idiopathic pulmonary fibrosis: results from the open-label extension study, INPULSIS-ON. Lancet Respir Med. 2019;7(1):60–8.
Talbot JCC, Nilsson BS. Pharmacovigilance in the pharmaceutical industry. Br J Clin Pharmacol. 1998;45(5):427–31.
Suvarna V. Phase IV of drug development. Perspect Clin Res. 2010;1(2):57–60.
Hilberg F, Roth GJ, Krssak M, et al. BIBF 1120: triple angiokinase inhibitor with sustained receptor blockade and good antitumor efficacy. Cancer Res. 2008;68(12):4774–82.
Wollin L, Wex E, Pautsch A, et al. Mode of action of nintedanib in the treatment of idiopathic pulmonary fibrosis. Eur Respir J. 2015;45(5):1434–45.
Corte T, Bonella F, Crestani B, et al. Safety, tolerability and appropriate use of nintedanib in idiopathic pulmonary fibrosis. Respir Res. 2015;16:116.
Kolb M, Raghu G, Wells AU, et al. Nintedanib plus sildenafil in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2018;379(18):1722–31.
Maher TM, Stowasser S, Nishioka Y, et al. Biomarkers of extracellular matrix turnover in patients with idiopathic pulmonary fibrosis given nintedanib (INMARK study): a randomised, placebo-controlled study. Lancet Respir Med. 2019;7(9):771–9.
Lancaster L, Crestani B, Hernandez P, et al. Safety and survival data in patients with idiopathic pulmonary fibrosis treated with nintedanib: pooled data from six clinical trials. BMJ Open Respir Res. 2019;6(1):e000397.
Bonella F, Kreuter M, Hagmeyer L, et al. Insights from the German compassionate use program of nintedanib for the treatment of idiopathic pulmonary fibrosis. Respiration. 2016;92(2):98–106.
Hughes G, Toellner H, Morris H, Leonard C, Chaudhuri N. Real world experiences: pirfenidone and nintedanib are effective and well tolerated treatments for idiopathic pulmonary fibrosis. J Clin Med. 2016;5(9):E78.
Galli JA, Pandya A, Vega-Olivo M, Dass C, Zhao H, Criner GJ. Pirfenidone and nintedanib for pulmonary fibrosis in clinical practice: tolerability and adverse drug reactions. Respirology. 2017;22(6):1171–8.
Toellner H, Hughes G, Beswick W, et al. Early clinical experiences with nintedanib in three UK tertiary interstitial lung disease centres. Clin Transl Med. 2017;6(1):41.
Brunnemer E, Wälscher J, Tenenbaum S, et al. Real-world experience with nintedanib in patients with idiopathic pulmonary fibrosis. Respiration. 2018;95(5):301–9.
Fletcher SV, Jones MG, Renzoni EA, et al. Safety and tolerability of nintedanib for the treatment of idiopathic pulmonary fibrosis in routine UK clinical practice. ERJ Open Res. 2018;4(4):00049-2018.
Yoon HY, Park S, Kim DS, Song JW. Efficacy and safety of nintedanib in advanced idiopathic pulmonary fibrosis. Respir Res. 2018;19(1):203.
Pereira CA, Baddini-Martinez JA, Baldi BG, et al. Safety and tolerability of nintedanib in patients with idiopathic pulmonary fibrosis in Brazil. J Bras Pneumol. 2019;45(5):e20180414.
Antoniou K, Markopoulou K, Tzouvelekis A, et al. Efficacy and safety of nintedanib in a Greek multicentre idiopathic pulmonary fibrosis registry: a retrospective, observational, cohort study. ERJ Open Res. 2020;6(1):00172–2019.
Noth I, Oelberg D, Kaul M, Conoscenti CS, Raghu G. Safety and tolerability of nintedanib in patients with idiopathic pulmonary fibrosis in the USA. Eur Respir J. 2018;52(1):1702106.
Hilberg F, Tontsch-Grunt U, Baum A, et al. Triple angiokinase inhibitor nintedanib directly inhibits tumor cell growth and induces tumor shrinkage via blocking oncogenic receptor tyrosine kinases. J Pharmacol Exp Ther. 2018;364(3):494–503.
Wollin L, Distler JHW, Redente EF, et al. Potential of nintedanib in treatment of progressive fibrosing interstitial lung diseases. Eur Respir J. 2019;54(3):1900161.
Bowen JM. Mechanisms of TKI-induced diarrhea in cancer patients. Curr Opin Support Palliat Care. 2013;7(2):162–7.
Boehringer Ingelheim Pharmaceuticals, Inc. OFEV® (nintedanib) prescribing information, 2020. http://bidocs.boehringer-ingelheim.com/BIWebAccess/ViewServlet.ser?docBase=renetnt&folderPath=/Prescribing+Information/PIs/Ofev/ofev.pdf. Accessed 27 Apr 2020.
Kreuter M, Ehlers-Tenenbaum S, Palmowski K, et al. Impact of comorbidities on mortality in patients with idiopathic pulmonary fibrosis. PLoS One. 2016;11(3):e0151425.
Noth I, Wijsenbeek M, Kolb M, et al. Cardiovascular safety of nintedanib in subgroups by CV risk at baseline in the TOMORROW and INPULSIS trials. Eur Respir J. 2019;54(3):1801797.
Collard HR, Ward AJ, Lanes S, Cortney Hayflinger D, Rosenberg DM, Hunsche E. Burden of illness in idiopathic pulmonary fibrosis. J Med Econ. 2012;15(5):829–35.
Chandler RE. Nintedanib and ischemic colitis: signal assessment with the integrated use of two types of real-world evidence, spontaneous reports of suspected adverse drug reactions, and observational data from large health-care databases. Pharmacoepidemiol Drug Saf. 2020. https://doi.org/10.1002/pds.5022.
Kolb M, Richeldi L, Behr J, et al. Nintedanib in patients with idiopathic pulmonary fibrosis and preserved lung volume. Thorax. 2017;72(4):340–6.
Costabel U, Behr J, Crestani B, et al. Anti-acid therapy in idiopathic pulmonary fibrosis: insights from the INPULSIS trials. Respir Res. 2018;19(1):167.
Kreuter M, Costabel U, Richeldi L, et al. Statin therapy and outcomes in trials of nintedanib in idiopathic pulmonary fibrosis. Respiration. 2018;95(5):317–26.
Richeldi L, Kolb M, Jouneau S, et al. Efficacy and safety of nintedanib in patients with advanced idiopathic pulmonary fibrosis. BMC Pulm Med. 2020;20(1):3.
Barczi E, Starobinski L, Kolonics-Farkas A, et al. Long-term effects and adverse events of nintedanib therapy in idiopathic pulmonary fibrosis patients with functionally advanced disease. Adv Ther. 2019;36(5):1221–32.
Bendstrup E, Wuyts W, Alfaro T, et al. Nintedanib in idiopathic pulmonary fibrosis: practical management recommendations for potential adverse events. Respiration. 2019;97(2):173–84.
Maher TM, Strek ME. Antifibrotic therapy for idiopathic pulmonary fibrosis: time to treat. Respir Res. 2019;20(1):305.
Maher TM, Inoue Y, Case AH, Sakamoto W, Stowasser S, Wuyts WA. Effect of dose reductions and/or interruptions on the efficacy of nintedanib in patients with idiopathic pulmonary fibrosis (IPF): subgroup analysis of the INPULSIS trials. Am J Respir Crit Care Med. 2017;195:A5381.
Acknowledgements
Funding
The clinical trials and pharmacovigilance program for nintedanib described in this paper were funded by Boehringer Ingelheim. The journal’s Rapid Service and Open Access Fees for this article were funded by Boehringer Ingelheim Pharmaceuticals, Inc.
Medical Writing Assistance
Writing support was provided by Julie Fleming, BSc and Wendy Morris, MSc of FleishmanHillard Fishburn, London, UK, which was contracted and funded by Boehringer Ingelheim Pharmaceuticals, Inc. Boehringer Ingelheim was given the opportunity to review the manuscript for medical and scientific accuracy as well as for intellectual property considerations.
Authorship
All named authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE), take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published. The authors did not receive payment for the development of this manuscript.
Authorship Contributions
HML, VK and SB contributed to the design of this study. VK and SB were involved in the analysis of the data. All authors contributed to the development of the manuscript. All authors approved the final version.
Prior Abstract Publication/Presentation
Some of the information provided in this manuscript was presented at the CHEST Annual Meeting, New Orleans, LA, USA, 19–23 October 2019 as: Lasky JA, Criner GJ, Lazarus HM, Kohlbrenner V, Bender S, Richeldi L; Safety of nintedanib in patients with idiopathic pulmonary fibrosis (IPF): long-term global pharmacovigilance data.
Disclosures
JAL reports being an advisory board member for Boehringer Ingelheim and Veracyte, a member of speakers bureau for Boehringer Ingelheim, Genentech and Veracyte, a member of a data safety monitoring board for Galecto, and an investigator in the IPF-PRO/ILD-PRO Registry funded by Boehringer Ingelheim. GC reports grants from ALung, Fisher & Paykel Healthcare, and Galapagos; personal fees from BTG, EOLO Pharma, NGM Bio, and Verona Pharma; and grants and personal fees from AstraZeneca, Boehringer Ingelheim, Broncus, Chiesi, GlaxoSmithKline, Lungpacer, Mereo Biopharma, Nuvaira, Olympus, Patara, PneumRx, PulmonX, ResMed, and Respironics. LR reports personal fees from Asahi Kasei, Biogen, Bristol-Myers Squibb, Celgene, CSL Behring, FibroGen, ImmuneWorks, Nitto, Pliant Therapeutics, Promedior, Respivant, and Toray; and grants and personal fees from Boehringer Ingelheim and Roche. VK and SB are employees of Boehringer Ingelheim. HML was an employee of Boehringer Ingelheim when this study was conducted and is now an employee of Altavant Sciences, Inc.
Compliance with Ethics Guidelines
This study did not require IRB approval as it was based on aggregate, patient de-identified data from a pharmacovigilance database. This study was not registered on a clinical trial web site as it was not a clinical trial.
Data Availability
The datasets used and/or analyzed during the current study are not publicly available but are available from Boehringer Ingelheim on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Additional information
Digital Features
To view digital features for this article go to https://doi.org/10.6084/m9.figshare.12666482.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Lasky, J.A., Criner, G.J., Lazarus, H.M. et al. Safety of Nintedanib in Patients with Idiopathic Pulmonary Fibrosis: Global Pharmacovigilance Data. Adv Ther 37, 4209–4219 (2020). https://doi.org/10.1007/s12325-020-01452-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-020-01452-5