
Abstract
Introduction
Cryoballoon ablation (CBA) is a standard catheter ablation technology with demonstrated clinical effectiveness for the treatment of paroxysmal atrial fibrillation (PAF); however, it can be associated with major adverse events, including phrenic nerve paralysis. Pulsed field ablation (PFA) is a novel, minimally thermal technology with comparable effectiveness and low safety risk. This study aimed to compare the safety profiles of PFA and CBA through critical analyses of the literature and indirect treatment comparisons.
Methods
Studies were identified by searching the MEDLINE database and the Clinicaltrials.gov registry. Registered clinical trials and/or Food and Drug Administration Investigation Device Exemption (FDA IDE) studies evaluating PFA or CBA in adult patients with drug-refractory PAF between January 2008 and March 2023 were selected. Comparative safety between PFA and CBA was assessed for major and prespecified adverse events. Indirect comparisons were conducted using the proportion of patients experiencing adverse events and confirmed with single-arm meta-analyses and sensitivity analyses.
Results
Data were extracted from three PFA publications including a total of 497 patients and six CBA studies including a total of 1113 patients. The analysis revealed that PFA was associated with significantly lower risk of major adverse events {risk difference − 4.3% [95% confidence interval (CI) − 5.8, − 2.8]; risk ratio 0.16 [95% CI 0.07, 0.45]} and prespecified adverse events [risk difference − 2.5% (95% CI − 4.4, − 0.5); risk ratio 0.53 (95% CI 0.31, 0.96)]. Meta-analyses confirmed the lower rate of major adverse events for PFA [0.4% (95% CI 0.0, 1.3)] vs. CBA [5.6% (95% CI 2.6, 8.6)] and prespecified adverse events for PFA [2.7% (95% CI 1.2, 4.1)] vs. CBA [5.8% (95% CI 2.7, 9.0)]. Sensitivity analyses exploring heterogeneity across studies confirmed robustness of the main analyses.
Conclusion
The findings of this study show that PFA has a more favorable safety profile than CBA, with significantly lower risks of major and prespecified adverse events. These indirect comparisons help contextualize the safety of PFA compared to CBA for the treatment of drug-refractory PAF in the absence of head-to-head studies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Pulsed field ablation (PFA) is a novel, minimally thermal technology for treating paroxysmal atrial fibrillation (PAF), with effectiveness comparable to cryoballoon ablation (CBA) and low safety risk. | |
With limited direct evidence, the current study aimed to compare the safety profiles of PFA and CBA through indirect treatment comparison. | |
PFA was associated with significantly lower risk of major adverse events and prespecified adverse events (risk ratios of 0.16 and 0.53, respectively). | |
The findings of this study show that PFA has a more favorable safety profile than CBA, providing further insight into treatment strategies for patients with drug-refractory PAF. |
Introduction
Atrial fibrillation (AF) is the most common type of cardiac arrythmia, affecting ~ 3% of the adult population across the world [1]. Atrial fibrillation is associated with a considerable impact on patient quality of life and substantial risk of cardiovascular events, leading to an increased risk of morbidity and mortality among patients [1, 2]. In addition, AF places considerable burden on the healthcare system [2].
Guidelines have recommended using anti-arrhythmic drugs (AADs) as an initial treatment of paroxysmal AF (PAF). Among patients who are drug-refractory or intolerant to AADs, pulmonary vein isolation (PVI) using catheter ablation is recommended. The use of catheter ablation has been increasing in its frequency over the past decade, with higher efficiency rates and better safety profile [3]. Cryoballoon ablation (CBA) is a thermal-based catheter ablation technology that uses cryo, or freezing, energy to freeze tissue and isolate the pulmonary veins to prevent aberrant electrical signals that are responsible for AF [4]. This technology has demonstrated lower recurrence rate and improved quality of life compared to AADs as a treatment of PAF [5]. Despite these clinical advantages, CBA is associated with increased risk of atrio-esophageal injury/fistula [6, 7], phrenic nerve injuries [8, 9], and/or pulmonary vein stenosis [10].
Pulsed field ablation (PFA) is a novel, minimally thermal catheter ablation technology that creates lesions in myocardial tissue through irreversible electroporation [11]. It is currently limited to high-volume centers, but its adoption rate continues to grow for smaller centers. Several single-arm clinical trials have shown the effectiveness of PFA in patients with drug-refractory PAF, with freedom from atrial arrhythmias ranging from 66.2% to 87.4% one year after PVI [12,13,14,15]. Because of the highly selective nature of PFA for myocardial tissue, PFA may prevent potential damage to adjacent tissues [16]. Evidence from clinical trials support favorable safety profiles of PFA, with incidence rates ranging from 0% to 2.5% for early-onset serious adverse events, including phrenic nerve injury, atrio-esophageal fistula, pulmonary vein stenosis, and vascular complications [12, 13].
Most clinical trials assessing PFA technology in patients with drug-refractory PAF are single-arm trials, and head-to-head trials comparing PFA to CBA are limited [17]. Indirect treatment comparisons pooling data from multiple clinical trials present a robust alternative option to compare these technologies. The objective was to conduct a critical literature review and an indirect treatment comparison to evaluate the comparative safety of PFA and CBA for PVI in patients with drug-refractory PAF.
Methods
Search Strategy
Literature searches were conducted in the MEDLINE (PubMed) database and the Clinicaltrials.gov registry from January 2008 to March 2023. Searches were performed using combinations of the following keywords: “pulsed field ablation”, “PFA”, “cryoballoon”, or “cryoablation”, together with “atrial fibrillation”. Only English-language articles were reviewed for eligibility. Identified studies were critically evaluated for inclusion in the final indirect comparison following best reporting practices from PRISMA guidelines [18], based on a qualitative assessment of study design, patient eligibility, patient baseline characteristics, and outcomes criteria.
Study Eligibility
Eligible studies had one of the following study designs: (1) FDA IDE (the Food and Drug Administration Investigation Device Exemption) studies; (2) first-in-human studies; or (3) registered clinical trials. Only the clinical trials that were registered on a clinical trial registry (i.e., clinicaltrials.gov) were considered. Studies had to involve adult patients with PAF who were drug-refractory to at least one class of AAD and received either PFA or CBA. Studies were excluded if they included patients with persistent AF, were not registered on a clinical trial registry, or were observational studies or conference abstracts. Studies were screened by an independent reviewer and checked for accuracy by a second reviewer.
Outcomes
The primary outcome was the composite of major procedure- or device-related adverse events reported at up to 30 days post-procedure. Major procedure- or device-related adverse events included cardiac tamponade or perforation, major vascular access complication or bleeding, myocardial infarction (MI), pericardial effusion, pericarditis, phrenic nerve paralysis, stroke, cerebrovascular accident (CVA), thromboembolism, transient ischemic attack (TIA), atrio-esophageal fistula, device- or procedure-related death, and pulmonary vein (PV) stenosis. Of note, PV stenosis and atrio-esophageal fistula were included in the primary outcome regardless of the timepoint. These events were identified as known potential risks across multiple clinical trials of AF ablation devices [12, 13, 15, 19,20,21,22,23,24], and as per guidance of the 2017 expert consensus statement from the Heart Rhythm Society (HRS) [25]. The secondary outcome was the composite of several prespecified adverse events reported at any timepoint.
Data Extraction and Feasibility Assessment
Data on study design, patient baseline characteristics, treatments, and safety outcomes were extracted into a standardized template by a single reviewer and checked for accuracy by a second reviewer. Cross-trial heterogeneity may contribute to bias within indirect treatment comparisons [26]. To ensure that studies were similarly sufficient for indirect comparison, a qualitative assessment of study design, eligibility criteria, patient baseline characteristics, treatments, and outcome definitions across the studies was conducted in accordance with best practices [27,28,29]. Studies that were deemed sufficiently similar based on clinical opinion were included in the analysis.
Statistical Analyses
Comparative safety between PFA and CBA was assessed through an unadjusted indirect treatment comparison and confirmed through single-arm meta-analyses. The proportion of patients experiencing an adverse event was calculated, and the results were presented using risk differences and risk ratios. Corresponding 95% confidence intervals (95% CI) were calculated using the Wald and the adjusted-log procedures, respectively. Sensitivity analyses were conducted by using other methods (i.e., Katz-log [30], Bailey [31], Noether [32], and Koopman [33]) to estimate the 95% CI.
Single-arm meta-analyses on PFA and CBA were performed separately to confirm the results from the indirect comparison. The overall weighted proportion of patients experiencing an adverse event within the eligible studies was estimated and presented in forest plots. Random effects model was used to account for potential heterogeneity between studies. Heterogeneity between study results was assessed using the τ2 statistic, and the percentage of total variation across studies was assessed using the inconsistency index, I2. Fixed effect meta-analyses were also conducted.
Analyses were conducted using the R packages DescTools [34] and meta [35] for single proportions. All analyses were conducted using the R software version 3.6.1.
Sensitivity Analyses
Sensitivity analyses were performed to assess the impact of cross-trial heterogeneity on the primary outcome. CBA studies with notable outlier values in the baseline characteristics were excluded one at a time from the primary analysis. PFA studies were not excluded to ensure a sufficient sample for analyses.
Statement of Ethics Compliance
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Results
Study Inclusion and Feasibility Assessment
A total of 170 PFA and 158 CBA studies were identified as potentially relevant from literature searches (Fig. 1). After excluding the studies that did not meet the eligibility criteria, a total of three PFA studies representing five trials (InspIRE [12], IMPULSE, PEFCAT, PEFCAT II [13], and PULSED AF [15]) and six CBA studies representing six trials (Cryo versus RF [20], SUPIR [24], plusONE [19], STOP AF Post-Approval Study [21], FreezeAF [23], and Fire and Ice [22]) were deemed eligible for inclusion.

PRISMA flow diagram of the targeted literature review for A pulsed field ablation and B cryoballoon ablation. CBA cryoballoon ablation, PAF paroxysmal atrial fibrillation, PFA pulsed field ablation, T&A title and abstract
All included studies were registered clinical trials (Table 1). All PFA trials were prospective, multi-center, single-arm trials with 12 months of follow-up. Four of the six CBA trials were prospective, randomized controlled trials with 12–18 months follow-up. The remaining two CBA trials were prospective, single-arm trials with 3.4 months (median) and 34.3 (mean) months of follow-up, respectively.
In total, the PFA studies consisted of 497 patients and the CBA studies consisted of 1113 patients. The distribution of baseline characteristics including age, gender, body mass index (BMI), left atrial diameter (LAD), and left ventricular ejection fraction (LVEF) were comparable across the studies (Table 2). The mean age of patients in the included studies ranged between 56 and 64 years. The distribution of male population was between 57.5% and 73.6% across the studies. A slightly lower male proportion (42.9%) was reported for the SUPIR study. The mean LAD values were 38.0–42.0 mm, and the mean LVEF was 57.9–64.2% across studies.
Medical characteristics for the patients were also comparable among the PFA and CBA trials (Table 2). The ranges of proportion for different comorbidities were as follows: diabetes (4.8–16.0%); hypertension (34.6–61.5%); coronary artery disease (CAD; 0.7–20.7%), and stroke/TIA (2.1–9.0%). Overall, the included studies were deemed sufficiently similar by clinical opinion to conduct an unanchored indirect treatment comparison for safety outcomes.
Comparative Safety of PFA and CBA
Composite of Major Adverse Events
The indirect comparison revealed that PFA was associated with a statistically significantly lower risk of major adverse events than CBA, with a risk difference of − 4.3% (95% CI − 5.8, − 2.8) and a risk ratio of 0.16 (95% CI 0.07, 0.45) (Table 3).
Results were confirmed in single-arm meta-analyses, which showed that 0.4% (95% CI 0.0, 1.3) of patients who underwent PFA experienced major adverse events, in contrast to 5.6% (95% CI 2.6, 8.6) of patients who underwent CBA (Table 3, Supplementary Fig. 1). Higher risk of major adverse events with CBA was primarily driven by phrenic nerve paralysis (PFA: 0 event vs. CBA: 33 events) and major vascular access complication or bleeding (PFA: 1 event vs. CBA: 12 events) (Table 4).
Composite of Prespecified Adverse Events
The indirect comparison showed that PFA was associated with a statistically significantly lower risk of prespecified adverse events than CBA, with a risk difference of − 2.5% (95% CI − 4.4, − 0.5) and a risk ratio of 0.53 (95% CI 0.31, 0.96) (Table 3).
Results were confirmed in single-arm meta-analyses, which showed that 2.7% (95% CI 1.2, 4.1) of patients who underwent PFA experienced an adverse event, in contrast to 5.8% (95% CI 2.7, 9.0) of patients who underwent CBA (Table 3, Supplementary Fig. 2).
Sensitivity Analyses
Four studies were identified with potential heterogeneity in baseline patient characteristics: SUPIR (duration of AF), plusONE (CAD and duration of AF), FreezeAF (hypertension), and Fire and Ice (hypertension) (Table 2). Exclusion of these studies one-at-a-time from the main analysis showed statistically significantly lower risk of major adverse events with PFA than with CBA (Supplementary Table 1).
Discussion
Pulsed field ablation (PFA) is emerging as an alternative to thermal-based catheter ablation technologies such as CBA, and multiple PFA systems have demonstrated their clinical effectiveness in single-arm clinical trials [12,13,14,15]. With limited head-to-head evidence comparing PFA to CBA available, an indirect treatment comparison of PFA and CBA was conducted to evaluate the comparative safety for PVI in patients with drug-refractory PAF. The present analysis shows that PFA has a significantly favorable safety profile compared to CBA. PFA was associated with 84% lower risk of major adverse events and 47% lower risk of prespecified adverse events than CBA. Results were driven by higher rates of major vascular access complication or bleeding, phrenic nerve injury, and pericardial effusion with CBA. Notably, there were no phrenic nerve injuries observed in the PFA trials included in the present study. Events of atrio-esophageal fistula or PV stenosis were also not observed in the included PFA trials. To the authors’ knowledge, this is the first indirect comparison of the safety profile between these two technologies using high-quality data from FDA IDE studies and registered clinical trials.
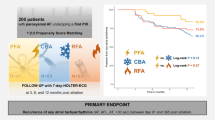
The evidence base supporting PFA in the treatment of drug-refractory PAF is evolving. ADVENT is the first randomized controlled trial to compare the effectiveness and safety of PFA (FARAPULSE; Boston Scientific, USA) (n = 301) or thermal ablation (n = 296) in adults with drug-refractory PAF [17]. Patients randomized to thermal ablation received either CBA (n = 132) or radio-frequency catheter ablation (n = 164), with each method planned to constitute approximately 50% of the aggregated control group [17]. The ADVENT trial showed that PFA was non-inferior to thermal ablation for the primary safety endpoint of acute- and chronic device-related and procedure-related serious adverse events (2.1% vs. 1.5% in thermal ablation, with posterior probability of non-inferiority > 0.999) [17]. In contrast, results from the current indirect comparison that pooled safety events from multiple PFA and CBA studies showed an improved safety profile with PFA relative to CBA, driven by phrenic nerve injury. Interestingly, no phrenic nerve injury was reported with thermal ablation in the ADVENT trial. Results from a real-world, retrospective, observational study comparing PFA (n = 200) and CBA (n = 200) also showed that PFA had an improved safety profile compared to CBA, with a numerically lower overall complication rate than CBA (3.0% vs. 6.5%; p = 0.1) that was driven by a higher rate of phrenic nerve injury with CBA (7.5% vs. 1.0%; p = 0.001) [36].
Overall, safety events across multiple novel PFA systems are reportedly low, with the rates of primary adverse events (assessed at 7 and 30 days after ablation) as low as zero for the VARIPULSE catheter and TRUPULSE generator system (Biosense Webster, USA) [12], 0.7% for PulseSelect (Medtronic, USA) [15], and up to 2.5% for FARAPULSE (Boston Scientific) [13]. Exceptionally low rates of major adverse events such as cardiac tamponade, pericardial effusion, and vascular complications have been reported with the PulseSelect and FARAPULSE systems, while no events were observed with the VARIPULSE/TRUPULSE system [12].
The current indirect comparison provides meaningful insight into the comparative safety profile of PFA and CBA. A strength of this analysis is that it only included patients with PAF who were drug-refractory to at least one AAD from a high-quality evidence base of registered clinical trials. Indirect treatment comparisons rely on the assumption that trials are sufficiently similar such that any underlying differences in patient populations would not bias the comparative effect estimate. A qualitative assessment of cross-trial heterogeneity was conducted a priori, the results of which showed sufficiently similar baseline characteristics across the trials. This was supported by clinical opinion. Nevertheless, this analysis was associated with limitations inherent to naïve indirect comparisons, including increased susceptibility to potential bias stemming from cross-trial heterogeneity. The impact of cross-trial heterogeneity on the analysis was explored in meta-analyses and sensitivity analyses. The results from meta-analyses using the random-effects model to account for cross-trial differences within PFA and CBA studies aligned with those from the indirect comparison. Additionally, the results for major adverse events were robust to excluding studies with outlier baseline patient characteristics one at a time in sensitivity analyses. However, cross-trial heterogeneity could not be fully explored within PFA studies owing to the need for a sufficient sample to conduct analyses. Anchored comparisons were not feasible due to limited randomized trials with a common comparator. Further, the ADVENT trial, which compared PFA to thermal ablation, was published outside the literature search window and therefore not considered for inclusion in this analysis.
Conclusion
Overall, the indirect treatment comparison and meta-analyses of the safety profile of PFA and CBA showed that PFA had significantly lower risks of major and prespecified procedure- or device-related adverse events than CBA, mainly driven by the higher rates of phrenic nerve palsy and vascular complications with CBA. These findings imply that PFA may be a reasonable alternative to CBA for PVI in patients with drug-refractory PAF.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498.
Andrade JG, Aguilar M, Atzema C, Bell A, Cairns JA, Cheung CC, et al. The 2020 Canadian Cardiovascular Society/Canadian Heart Rhythm Society Comprehensive Guidelines for the Management of Atrial Fibrillation. Can J Cardiol. 2020;36(12):1847–948.
Calkins H, Reynolds MR, Spector P, Sondhi M, Xu Y, Martin A, et al. Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: two systematic literature reviews and meta-analyses. Circ Arrhythm Electrophysiol. 2009;2(4):349–61.
Murray MI, Arnold A, Younis M, Varghese S, Zeiher AM. Cryoballoon versus radiofrequency ablation for paroxysmal atrial fibrillation: a meta-analysis of randomized controlled trials. Clin Res Cardiol. 2018;107(8):658–69.
Liu Z, Yang Z, Lu Y, Wang H, Zou C. Short-term and long-term effects of cryoballoon ablation versus antiarrhythmic drug therapy as first-line treatment for paroxysmal atrial fibrillation: a systematic review and meta-analysis. Clin Cardiol. 2023;46(10):1146–53.
Sarairah SY, Woodbury B, Methachittiphan N, Tregoning DM, Sridhar AR, Akoum N. Esophageal thermal injury following cryoballoon ablation for atrial fibrillation. JACC Clin Electrophysiol. 2020;6(3):262–8.
Ha FJ, Han HC, Sanders P, Teh AW, O’Donnell D, Farouque O, et al. Prevalence and prevention of oesophageal injury during atrial fibrillation ablation: a systematic review and meta-analysis. Europace. 2019;21(1):80–90.
Heeger CH, Sohns C, Pott A, Metzner A, Inaba O, Straube F, et al. Phrenic nerve injury during cryoballoon-based pulmonary vein isolation: results of the Worldwide YETI registry. Circ Arrhythm Electrophysiol. 2022;15(1): e010516.
Rottner L, Fink T, Heeger CH, Schluter M, Goldmann B, Lemes C, et al. Is less more? Impact of different ablation protocols on periprocedural complications in second-generation cryoballoon based pulmonary vein isolation. Europace. 2018;20(9):1459–67.
Tokutake K, Tokuda M, Yamashita S, Sato H, Ikewaki H, Okajima E, et al. Anatomical and procedural factors of severe pulmonary vein stenosis after cryoballoon pulmonary vein ablation. JACC Clin Electrophysiol. 2019;5(11):1303–15.
Schaack D, Schmidt B, Tohoku S, Bordignon S, Urbanek L, Ebrahimi R, et al. Pulsed field ablation for atrial fibrillation. Arrhythm Electrophysiol Rev. 2023;12: e11.
Duytschaever M, De Potter T, Grimaldi M, Anic A, Vijgen J, Neuzil P, et al. Paroxysmal atrial fibrillation ablation using a novel variable-loop biphasic pulsed field ablation catheter integrated with a 3-dimensional mapping system: 1-year outcomes of the multicenter inspIRE study. Circ Arrhythm Electrophysiol. 2023;16(3): e011780.
Reddy VY, Dukkipati SR, Neuzil P, Anic A, Petru J, Funasako M, et al. Pulsed field ablation of paroxysmal atrial fibrillation: 1-year outcomes of impulse, PEFCAT, and PEFCAT II. JACC Clin Electrophysiol. 2021;7(5):614–27.
Reddy VY, Neuzil P, Koruth JS, Petru J, Funosako M, Cochet H, et al. Pulsed field ablation for pulmonary vein isolation in atrial fibrillation. J Am Coll Cardiol. 2019;74(3):315–26.
Verma A, Haines DE, Boersma LV, Sood N, Natale A, Marchlinski FE, et al. Pulsed field ablation for the treatment of atrial fibrillation: Pulsed AF Pivotal trial. Circulation. 2023;147(19):1422–32.
Cochet H, Nakatani Y, Sridi-Cheniti S, Cheniti G, Ramirez FD, Nakashima T, et al. Pulsed field ablation selectively spares the oesophagus during pulmonary vein isolation for atrial fibrillation. Europace. 2021;23(9):1391–9.
Reddy VY, Gerstenfeld EP, Natale A, Whang W, Cuoco FA, Patel C, et al. Pulsed field or conventional thermal ablation for paroxysmal atrial fibrillation. New Engl J Med. 2023. https://doi.org/10.1056/NEJMoa2307291.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71.
Ferrero-de-Loma-Osorio A, Garcia-Fernandez A, Castillo-Castillo J, Izquierdo-de-Francisco M, Ibanez-Criado A, Moreno-Arribas J, et al. Time-to-effect-based dosing strategy for cryoballoon ablation in patients with paroxysmal atrial fibrillation: results of the plusONE multicenter randomized controlled noninferiority trial. Circ Arrhythm Electrophysiol. 2017. https://doi.org/10.1161/CIRCEP.117.005318.
Hunter RJ, Baker V, Finlay MC, Duncan ER, Lovell MJ, Tayebjee MH, et al. Point-by-point radiofrequency ablation versus the cryoballoon or a novel combined approach: a randomized trial comparing 3 methods of pulmonary vein isolation for paroxysmal atrial fibrillation (The Cryo versus RF trial). J Cardiovasc Electrophysiol. 2015;26(12):1307–14.
Knight BP, Novak PG, Sangrigoli R, Champagne J, Dubuc M, Adler SW, et al. Long-term outcomes after ablation for paroxysmal atrial fibrillation using the second-generation cryoballoon: final results from STOP AF post-approval study. JACC Clin Electrophysiol. 2019;5(3):306–14.
Kuck KH, Furnkranz A, Chun KR, Metzner A, Ouyang F, Schluter M, et al. Cryoballoon or radiofrequency ablation for symptomatic paroxysmal atrial fibrillation: reintervention, rehospitalization, and quality-of-life outcomes in the FIRE AND ICE trial. Eur Heart J. 2016;37(38):2858–65.
Luik A, Kunzmann K, Hormann P, Schmidt K, Radzewitz A, Bramlage P, et al. Cryoballoon vs. open irrigated radiofrequency ablation for paroxysmal atrial fibrillation: long-term FreezeAF outcomes. BMC Cardiovasc Disord. 2017;17(1):135.
Reddy VY, Sediva L, Petru J, Skoda J, Chovanec M, Chitovova Z, et al. Durability of pulmonary vein isolation with cryoballoon ablation: results from the sustained PV isolation with arctic front advance (SUPIR) study. J Cardiovasc Electrophysiol. 2015;26(5):493–500.
Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: executive summary. Heart Rhythm. 2017;14(10):e445–94.
Dias S, Sutton AJ, Welton NJ, Ades AE. Nice DSU technical support document 3: heterogeneity: subgroups, meta-regression, bias and bias-adjustment 2011 [updated April 2012. Available from: http://www.nicedsu.org.uk
Hoaglin DC, Hawkins N, Jansen JP, Scott DA, Itzler R, Cappelleri JC, et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: report of the ISPOR task force on indirect treatment comparisons good research practices: Part 2. Value Health. 2011;14(4):429–37.
Jansen JP, Fleurence R, Devine B, Itzler R, Barrett A, Hawkins N, et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: report of the ISPOR task force on indirect treatment comparisons good research practices: Part 1. Value Health. 2011;14(4):417–28.
Jansen JP, Naci H. Is network meta-analysis as valid as standard pairwise meta-analysis? It all depends on the distribution of effect modifiers. BMC Med. 2013;11:159.
Katz D, Baptista J, Azen SP, Pike MC. Obtaining confidence intervals for the risk ratio in cohort studies. Biometrics. 1978;34(3):469–74.
Bailey BJR. Confidence limits to the risk ratio. Biometrics. 1987;43(1):201–5.
Noether GE. Two confidence intervals for the ratio of two probabilities and some measures of effectiveness. J Am Stat Assoc. 1957;52(277):36–45.
Koopman PAR. Confidence intervals for the ratio of two binomial proportions. Biometrics. 1984;40(2):513–7.
Signorell A, Alfons A, Anderegg N, Aragon T, Arachchige C, Arppe A, Baddeley A, Barton K, Bolker B et al. DescTools: Tools for Descriptive Statistics; R Package Version 0.99.44. 2021. Available online: https://CRAN.R-project.org/package=DescTools (Accessed on 4 May 2023). 2021.
Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22(4):153–60.
Urbanek L, Bordignon S, Schaack D, Chen S, Tohoku S, Efe TH, et al. Pulsed field versus cryoballoon pulmonary vein isolation for atrial fibrillation: efficacy, safety, and long-term follow-up in a 400-patient cohort. Circ Arrhythm Electrophysiol. 2023;16(7):389–98.
Acknowledgements
The authors would like to acknowledge Leena Patel and Maximiliano Iglesias for their contributions towards strategic discussions on study design, and Colin Vibert for supporting statistical analyses. Maximiliano Iglesias is an employee of Johnson & Johnson. Leena Patel and Colin Vibert are employees of EVERSANA, Canada.
Funding
This work, the Rapid Service Fee of the journal, and the Open Access Fee was funded by Biosense Webster.
Author information
Authors and Affiliations
Contributions
Donghyun D. Lee contributed to the literature review, data collection, analysis, and interpretation of the data. Anja Haltner conducted the statistical analysis. Sonia Maccioni, Reecha Sharma, Rahul Khanna, and Johan Vijgen contributed to the interpretation of the data and critically reviewed the importance of intellectual content for the work. Donghyun D. Lee and Anja Haltner were responsible for drafting the manuscript. Sonia Maccioni, Reecha Sharma, Rahul Khanna, and Johan Vijgen were responsible for reviewing and for providing final approval. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work, and have given their approval for this version to be published.
Corresponding author
Ethics declarations
Conflicts of Interest
Donghyun D. Lee and Anja Haltner are employees of EVERSANA™. EVERSANA™ receives consultancy fees from major pharmaceutical and device companies, including Biosense Webster. Sonia Maccioni, Rahul Khanna, and Reecha Sharma are employees of Johnson & Johnson. Johan Vijgen reports research funding from Daiichi-Sackyo, BMS-Pfizer, Bayer, Biotronik, Boston Scientific, Medtronic, and Abbott. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Ethical Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Maccioni, S., Sharma, R., Lee, D.D. et al. Comparative Safety of Pulsed Field Ablation and Cryoballoon Ablation Technologies for Pulmonary Vein Isolation in Patients with Paroxysmal Atrial Fibrillation: A Critical Literature Review and Indirect Treatment Comparison. Adv Ther 41, 932–944 (2024). https://doi.org/10.1007/s12325-023-02765-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-023-02765-x