
Abstract
Most studies on arsenic toxicity have been conducted among populations exposed to arsenic contained in drinking water. Relatively little research concerns effects of airborne arsenic. The aim of this study was to determine whether there is an association between urinary 15-F2t-isoprostane (u15-F2t-IsoP) levels in relation to renal function (urinary creatinine and N-acetyl-β-d-glucosaminidase––uNAG) and urinary arsenic (uAs) in inhabitants from copper smelter impact zone. The secondary purpose of the analysis was to assess utility of a potential association between uAs and u15-F2t-IsoP as a biomarker of systemic oxidative stress. Urinary 15-F2t-IsoP, NAG, and creatinine were measured in 967 urine samples collected from 649 adult women (51.9 ± 13.2 years old) and 318 adult men (53.8 ± 14.9 years old). Total uAs concentration was measured in 918 samples using HPLC-ICP-MS. Arsenic species, such as inorganic arsenic, methylarsonic acid, dimethylarsinic acid, and arsenobetaine, were measured in urine collected from 255 participants with uAs exceeding the upper norm. Data were analyzed using multivariate linear regression and logistic regression models. In the studied population urinary creatinine was positively associated with uAs. A positive linear correlation (p < 0.0000) between lg(uAs) and u15-F2t-IsoP was found both for normal and elevated uAs. A positive linear correlation was observed also between lg(ΣuAs) and u15-F2t-IsoP (p < 0.0000). In the logistic regression model, after adjustment for confounders, elevated uAs was the only predictor of increased u15-F2t-IsoP (OR = 1.31, 95% CI 1.08–1.59, p < 0.01). Cigarette smoking was associated with renal proximal tubular dysfunction only in people with uNAG concentration above 75th quartile. In the studied population chronically exposed to airborne arsenic, increase in urinary arsenic is associated with renal dysfunction and systemic oxidative stress. Urinary 15-F2t-isoprostane may be useful in the monitoring of health status in populations exposed to airborne arsenic.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
It is estimated that approximately 200 million people worldwide drink water containing arsenic in concentrations exceeding the WHO-accepted norm of 10 μg/L (World Health Organization 2011). The consumption of contaminated water is the most common route of environmental exposure to arsenic. A majority of toxicological studies on arsenic have been carried out on populations exposed to arsenic through drinking water, but few have been carried out on populations exposed to airborne arsenic. However, in several European countries, exposure to arsenic contained in PM10 dust has been recognized as an important local industry-related toxicological issue (report of European Environment Agency: Air quality in Europe 2015). In recent years, in numerous cities located in copper smelter areas, average annual arsenic air concentrations exceeded the target value of 6.0 ng/m3 (Air quality in Europe 2015).
Arsenic is a potent toxin. Most cases of arsenic-induced toxicity in humans are due to exposure to inorganic arsenic. Humans may be also exposed to less toxic organic arsenicals that are used in agriculture (mainly methyl and phenyl derivatives of arsenic acid) or found in fish and shellfish (arsenobetaine and arsenocholine) (Agency for Toxic Substances Disease Registry (ATSDR) 2007). Chronic exposure to inorganic arsenic is associated with clinical symptoms of arsenic toxicity as well as with the development of cancer (World Health Organization International Agency for Research on Cancer IARC 2002)). Both in humans and laboratory animals, arsenic can cause skin changes, black foot disease, peripheral neuropathy, encephalopathy, hepatomegaly, liver cirrhosis, altered heme metabolism, bone marrow depression, diabetes, renal proximal tubule degeneration, as well as papillary and cortical kidney necrosis (World Health Organization 2011; Agency for Toxic Substances Disease Registry (ATSDR) 2007; Hughes et al. 2011). There is sufficient evidence in humans that arsenic causes lung, skin, and urinary bladder cancer. International Agency for Research on Cancer (IARC) classified arsenic and its inorganic compounds as group 1 carcinogens (Straif et al. 2009).
The clinical effects of environmental exposure to arsenic depend on the dose, form (inorganic vs organic), type of compounds (trivalent arsenicals being more toxic than their pentavalent analogs), route of absorption, bioavailability, and intracellular metabolism (Styblo et al. 2000). Confounders, such as nutritional deficiencies, selenium intake, smoking, and genetic factors, all affect these effects. Individuals with a relatively weak immune system, such as infants, young children, pregnant women, elderly individuals, and people with immunodeficiencies, are at an increased risk of arsenic toxicity (Kile et al. 2016; Dangleben et al. 2013).
In most species, including humans, inorganic arsenic in both trivalent and pentavalent states undergoes sequential reduction and methylation reactions leading to the formation of monomethylarsonic acid (MMA) and dimethylarsinic acid (DMA) (Agency for Toxic Substances Disease Registry (ATSDR) 2007; World Health Organization International Agency for Research on Cancer IARC 2002; Cullen et al. 1984). Inorganic As(V) is readily reduced to inorganic As(III), which is taken up by the cell. Within the cell (mainly in the liver), As(III) is methylated to form MMA(V), which is reduced to MMA(III). MMA(III) subsequently undergoes oxidative methylations to DMA(V), which is the primary excretion product in humans (Agency for Toxic Substances Disease Registry (ATSDR) (2007)). In contrast to inorganic arsenic, ingested organic arsenic species undergo limited metabolism, do not readily enter the cell, and are primarily excreted in urine in the unchanged form (Agency for Toxic Substances Disease Registry (ATSDR) 2007). Since 75% of the ingested arsenic is excreted in urine within 3 days of exposure, urine analysis for arsenic is the best screening test to detect arsenic exposure (Pellizzari and Clayton 2006; Zhang et al. 2014).
Inorganic As(V) may replace phosphate in several reactions. Inorganic and methylated arsenic (III) may react with critical thiols in proteins and inhibit their activity (Hughes et al. 2011).
A common mechanism of arsenic toxicity is the generation of intracellular reactive oxygen species (ROS), which mediate multiple changes to cell behavior by altering signaling pathways and epigenetic modifications, or cause direct oxidative damage (Jomova et al. 2011; Hu et al. 2020). Arsenic induces the formation of oxidized lipids, which, in turn, generate several bioactive molecules (ROS, peroxides and isoprostanes) (Jomova et al. 2011). Mitochondria, the main place of ROS generation, may be an important target for arsenic toxicity (Prakash et al. 2015). Potential mechanisms for arsenic carcinogenicity include genotoxicity, altered DNA methylation, oxidative stress, altered cell proliferation, co-carcinogenesis, and tumor promotion (Agency for Toxic Substances Disease Registry (ATSDR) 2007; World Health Organization International Agency for Research on Cancer IARC 2002).
Kidneys are particularly sensitive to the toxic effects of arsenic entering the body via the oral and respiratory routes. Rich vascularization providing kidneys with an extremely good blood supply leads to relatively high renal arsenic accumulation. Arsenic nephrotoxicity generally depends on arsenic blood concentration. However, in some cases, renal dysfunction results from unpredictable, dose-independent idiosyncratic phenomena (Marchewka 2006). In a meta-analysis of 24 epidemiological studies, the authors showed a positive correlation between arsenic exposure and kidney disease-associated mortality and mixed evidence for an association between arsenic exposure and markers of chronic kidney disease, such as N-acetyl-β-d-glucosaminidase (NAG) (Zheng et al. 2015). NAG, similar to leucine aminopeptidase 3, belongs to early markers of proximal tubular damage (Sundaram et al. 2011; Bedir et al. 1996).
Arsenic, a recognized carcinogen in humans, has also been associated with an increasing number of non-cancerous diseases, including cardiovascular disease (CVD) (Farzan et al. 2017; James et al. 2015; Moon et al. 2013). A majority of studies on arsenic toxicity were conducted on populations exposed to high or moderate levels of arsenic in drinking water (Kim et al. 2016a; Huang et al. 2009). The results from recent studies show that not only high but also low and moderate levels of exposure are associated with morbidity (Monrad et al. 2017) and mortality (Farzan et al. 2015; Medrano et al. 2010) due to CVD. Arsenic at high doses affects the cardiovascular system through inflammation, atherogenic lipid and lipoprotein changes, and oxidative stress, as evidenced by both experimental and epidemiological studies (Ledda et al. 2018; Chen et al. 2007; Lemaire et al. 2015). Whether exposure to arsenic in small doses triggers the inflammatory process, endothelial dysfunction, and oxidative stress is still under investigation. Experimental and epidemiological studies have provided evidence for a positive association between arsenic exposure and oxidative stress biomarkers, such as oxidized low-density lipoprotein (LDL), DNA damage biomarker 8-oxo-2′- deoxyguanosine (Karim et al. 2013; Engström et al. 2010), and isoprostane F2 (Farzan et al. 2017).
Isoprostanes are prostaglandin-like compounds produced endogenously predominantly through non-enzymatic, free radical-catalyzed peroxidation of esterified arachidonic acid. Increased urinary levels of isoprostane F2 reflect extensive oxidative stress and systemic levels of lipid peroxidation end products and are positively associated with CVD risk factors, such as smoking and hypertension (Minuz et al. 2002; Morrow et al. 1995). One isoprostane metabolite, 15-F2t-isoprostane (15-F2t-IsoP), is considered to be a reliable marker of systemic oxidative stress (Dorjgochoo et al. 2012; Milne et al. 2015).
The aim of this study was to determine urinary 15-F2t-IsoP (u15-F2t-IsoP) levels in relation to renal function (urinary creatinine and NAG) and urinary arsenic (uAs) in city inhabitants of a copper smelter impact zone, in which arsenic air concentration exceeded accepted values. Given increasing evidence that susceptibility to arsenic may differ between sexes (Zheng et al. 2015; Farzan et al. 2017; Moon et al. 2013), potential differences between men and women were explored. Urinary 15-F2t-IsoP and NAG were also measured in the group of copper smelter workers who had been exposed to arsenic both environmentally and occupationally. The secondary purpose of the analysis was to assess the utility of a potential association between uAs and u15-F2t-IsoP as a biomarker of systemic oxidative stress.
Material and Methods
Participants
The study was carried out as a branch of another study which included nearly 2000 subjects living in the vicinity of a copper smelter (Kozłowska et al. 2019). At present, the main toxicological problem in this area is environmental exposure to airborne arsenic. According to the Provincial Inspectorate for Environmental Protection, the average annual arsenic air concentration in the zone was 12.6 ng/m3 in 2016, 30.2 ng/m3 in 2017 (with average monthly minimal and maximal values of 21.1 ng/m3 and 39.3 ng/m3, respectively) and 10.0 ng/m3 in 2018 (with average monthly minimal and maximal values of 4.2 ng/m3 and 20.0 ng/m3, respectively). The measured average arsenic air concentrations significantly exceeded the established norm of 6 ng/m3. The arsenic concentration in drinking water in the years 2016–2018 was lower than the WHO-accepted norm of 10 μg/L (World Health Organization 2011).
In this sub-study, 967 participants were enrolled. The inclusion criteria were age over 18 and at least 10 years of residence in the vicinity of a copper smelter.
Basic information on age, sex, history of smoking, alcohol consumption, recent fish and seafood consumption (with subjects asked not to consume these foods during the week preceding samples collection), and previous diagnosis of chronic kidney disease (CKD) and cancer was gathered via questionnaires. Participants were divided into sub-groups according to sex, age (< 40, 40–59, and ≥ 60 years old), smoking habits (current smoker, former smoker, and never smoker––the reference group), as well as alcohol consumption (regular––at least once per week, occasional––once per month, and abstinent––the reference group). The number of women who volunteered and qualified for the study was approximately twice as large as the number of men. Among participants, 25 people did not provide information on fish and seafood consumption, 22 people on alcohol drinking and 15 people on smoking, which represented less than 2.7% of data and did not significantly alter results. Chronic kidney disease had been diagnosed in 26 people, while 59 subjects had a history of malignancy, most frequently breast, colon, thyroid, or brain cancer. We had no data on diabetes.
Urinary Arsenic
Total urinary arsenic (uAs) concentrations were measured in 918 samples, whereas various forms of arsenic [inorganic As (iAs), MMA, DMA, and arsenobetaine (AsB)] urinary concentrations were determined in 255 samples. Measurements were performed at the Nofer Institute of Occupational Medicine (Lodz, Poland) using HPLC-ICP-MS and expressed in micrograms per liter. Creatinine concentrations have been measured in the 918 samples in order to estimate the impact of urinary dilution on arsenic concentration. Urinary arsenic was calculated in micrograms per gram of creatinine, by dividing uAs [µg/L] per urinary creatinine concentration [g/L]. Creatinine adjustment was used due to the high precision and accuracy of urinary creatinine analysis for correction of urine dilution (Che-Jung et al. 2018).
Concentrations of arsenic species were presented as sum (ΣuAs) of iAsIII, iAsV, MMAV and DMAV, and as percentage of total arsenic. The proportion of urinary iAs (% uiAs) was calculated as (iAsIII + iAsV)/uAs × 100. The proportion of urinary MMA (% uMMA) and urinary DMA (% uDMA) were calculated as (MMA/uAs) × 100 and (DMA/uAS) × 100, respectively.
Biochemical Measurements
Isoprostane, NAG, and creatinine were measured in 967 urinary samples from 649 adult women (51.9 ± 13.2 years old) and 318 adult men (53.8 ± 14.9 years old), gathered between 29/09/2017 and 08/12/2017. Urine samples were collected in 10 ml tubes with the description code, transported in refrigerators, and placed in a freezer at − 80 °C. Biochemical measurements were performed between January and May 2018.
Urinary NAG was measured by an immunoenzymatic assays using ELISA kits (Wuhan EIAab Science Co., Ltd, Wuhan, CHINA) with the multi-mode reader SYNERGY/LX (BioTekSynergy/LX, Vermont, USA). Concentration of uNAG was expressed in U/L of urine or U/g urinary creatinine.
Urinary 15-F2t-IsoP was measured using a competitive enzyme-linked immunoassay kit (Wuhan EIAab Science Co., Ltd, Wuhan, CHINA). Duplicate samples of 50 μl of centrifuged urine were added successively to each well in a 96-well plate, followed by addition of 50 μl of detection reagent (Detection A) and incubation at 37 °C. Full well plates were shaken at 500 rpm for 1 h. After this time, each well was suctioned off and washed 3 times with the washing solution (wash buffer). Next, 100 μl of detection solution (Detection B) was added to each well, which was then incubated at 37 °C and shaken at 500 rpm for 45 min. After this time, 5 rinses were carried out in each well. At the last rinse, the plate was thoroughly dried. Then 90 μl of substrate was added to every well, which was next incubated for 15 min at 37 °C and shaken at 500 rpm. After this time, 50 μl of the stop solution was added and gently stirred. Urinary 15-F2t-IsoP concentrations were quantified using colorimetric readings at 450 nm against a standard curve with a multi-mode reader SYNERGY/LX. Approximately 10% of wells was reserved for quality control samples and reagent blanks. Replicates of a non-study composite urine sample were included in each plate to account for inter- and intra-plate variability, which turned out to be lower than 10%. Urinary 15-F2t-IsoP values were presented in ng/mL or ng/mg creatinine.
Urinary creatinine (ICD: M37) was measured in accordance with the IB/LAB/1289 research procedure (version II of 2015-09-17) in the laboratory accredited by PCA No. AM003, reference range 28–217 mg/dL.
Statistical Analysis
The normality test was performed for all continuous variables. Data are presented as mean ± standard deviation for normally distributed continuous variables and median (percentile or interquartile range) for non-normally distributed variables. Categorical data are expressed as numbers and percentages. The characteristics of the studied groups were analyzed using the Mann–Whitney U or 2-sample Student t test for continuous variables and the χ2 test for categorical variables. Correlations between urinary arsenic and other parameters were analyzed with the Spearman or Pearson correlation coefficient.
A natural logarithmic transformation was applied to variables with skewed distributions: total uAs, iAs, and sum iAs + MMA + DMA (ΣuAs). Multiple linear regression analysis was used to assess the association between continuous variables. Covariates considered for inclusion in regression models were sex, age, cigarette smoking, alcohol consumption, occupational exposure, co-existing diseases, and creatinine level. The association between qualitative variables (elevated or normal, in the zero–one system) and predictors was analyzed in the multivariable logistic regression model.
For the cross-sectional analysis, logistic regression models were used in order to estimate adjusted odds ratios for prevalence of increased urinary isoprostane (or increased NAG as a marker of proximal renal tubule damage) in adults with elevated urinary arsenic concentrations. In the first regression step, qualitative and quantitative predictors were defined. The coding of qualitative variables with sigma limitations (quasi-experimental) has been applied. Diagnosis of predictors was performed by a one-factor analysis. Multifactorial model was built using backward stepwise approach in linear/logistic regression method involving a validation mechanism based on a V-cross-check. A p value of 0.05 was used as a cut-off to evaluate statistical significance. The program TIBCO Statistica 13.3 was used.
Results
Urinary Arsenic
In the studied population exposed to airborne arsenic median (10th, 90th percentiles), total uAs was 7.5 (2.4–41.8) μg/L, corresponding to 9.9 (3.1–54.7) μg/g creatinine, similar in men and women (Table 1).
Total uAs exceeding the upper norm, i.e. > 15 μg/L (Schulz et al. 2011), was demonstrated in 255 people: 90 men (29%) and 165 women (25%). In this group, total uAs concentration was 57.9 ± 68.2 μg/L and 54.6 ± 64.3 μg/L in men and women, respectively, and arsenic species were determined. Arsenite or arsenate (inorganic As; iAs) levels were below the limit of detection (LOD) in 2 (0.8%) samples, MMA in 1 (0.4%), and DMA in 2 samples.
A positive correlation between age of participants and ln-transformed uAs was shown using linear regression analysis (r = 0.1586, p < 0.001). In the group of people with total uAs exceeding the upper norm, ln-transformed sum of arsenic species [ln(ΣuAs)] increased together with age (r = 0.2445, p < 0.001), whereas there was no significant association between age and inorganic arsenic forms (p = 0.3385).
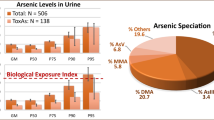
Total uAs expressed in μg/g creatinine did not differ significantly between groups of non-smokers, former, and current smokers (Table 1). However, in current smokers ΣAs expressed in μg/L was higher (p < 0.01) in comparison to non-smokers (Fig. 1). Additionally, iAs presented as % of uAs as well as urinary AsB was significantly higher, whereas MMA presented as % of uAs was lower in smokers vs non-smokers (Table 1).

Total urinary arsenic in the entire group of 918 respondents and sum of arsenic species in the group of 255 subjects with elevated (above 15 µg/L) uAs depending on smoking; non-smokers (N), past smokers (P), and current smokers (S). **Statistically significant difference in comparison to non-smokers group, p < 0.01
Among participants, 79 men had been exposed to arsenic not only environmentally but also occupationally due to work at copper smelters. Median uAs level expressed in μg/g creatinine was similar between workers and the rest of the studied population (Table 1). However, median uAs value without adjustment for creatinine level was significantly higher in the group of workers compared to the rest [12.4 (3.1–101.0) µg/L vs 7.2 (2.3–40.0), p < 0.005].
In order to determine whether cigarette smoking and occupational exposure to arsenic were predictors of increased urinary ΣAs (in μg/g creatinine) or lg(uAs), a linear regression analysis in multivariate models was performed. Sex, age, alcohol drinking, and presence of CKD or cancer were identified as potential confounders. Significant associations between smoking and ΣuAs [95% confidence interval (CI 95%): 1.24–5.62, p < 0.0022, β = 0.1949] as well as between occupational exposure to arsenic and ΣuAs [CI 95%: 0.39–5.33, p < 0.0230, β = 0.1748] were found. Occupational exposure was associated also with lg(uAs) expressed in µg/L; CI 95%: 0.03–0.12, p < 0.0389, β = 0.0765. Furthermore, a significant association between smoking and iAs (in % of uAs) was observed; CI 95%: 2.01–18.05, p < 0.0144, β = 0.1627.
There were no differences in arsenic urinary excretion due to alcohol consumption and presence of CKD or cancer (Table 1). No differences in uAs concentrations were observed between the group of 470 people who had consumed fish or seafood over the week preceding sample collection and 423 participants who denied fish and seafood consumption [7.5 (2.1–36.7) μg/L vs 7.7 (2.4–50.8) μg/L). A positive correlation between urinary creatinine and uAs was shown [b = 0.2089, F(1,916) = 18,027 p < 0.001].
Urinary N-Acetyl-β-d-Glucosaminidase (uNAG)
Median values (10th, 90th percentiles) of uNAG (U/L) in 318 men [19.9 (5.2–89.2)] and in 649 women [17.7 (3.8–85.9)] exposed to airborne arsenic were similar. Median value of uNAG normalized to urinary creatinine concentration was 43.0 (5.5–97.8) U/g creatinine. There was a negative correlation between inhabitants age and uNAG (Spearman’s rho = − 0.1310, p < 0.05). In comparison to male non-smokers, uNAG expressed in U/L was higher in male smokers (41.1 ± 31.2 vs 30.5 ± 28.5 U/L, p < 0.01). However, after adjustment for urinary creatinine level, there were no significant differences in uNAG concentrations between smokers and non-smokers (Table 2).
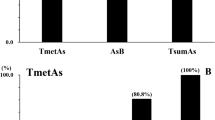
Nevertheless, an interaction between sex and smoking impacting on uNAG (β = 0.11, 95% CI: 0.31 to 6.44, p < 0.05) and borderline interactions between sex, smoking, and arsenic impacting on uNAG (F = 3.7; 95% CI − 6.08 to 0.04, p = 0.05) were shown. In the group of men with normal uAs levels, smoking was associated with increased uNAG (Fig. 2).

Interaction between sex, smoking, and total urinary arsenic in the action on uNAG concentration in sub-populations exposed to airborne arsenic
Urinary NAG values were similar in 79 men occupationally exposed to As (30.8 ± 27.6 U/L) and in 239 men without occupational exposure (32.2 ± 29.5 U/L). At the same time, urinary creatinine levels in men occupationally exposed to arsenic were significantly higher than in men without occupational exposure (142.0 ± 69.1 mg/dL vs 105.2 ± 62.6 mg/dL; p < 0.001). After adjustment for urinary creatinine levels, mean uNAG concentrations in the group of workers exposed to arsenic (26.1 ± 26.9 U/g creatinine) was lower in comparison to men without occupational exposure (45.4 ± 73.8 U/g creatinine; p < 0.05). Alcohol drinking had no effect on uNAG concentration: uNAG was 32.4 ± 32.1 U/L in occasional drinkers (n = 107), 32.3 ± 30.1 U/L in regular drinkers (n = 191) and 30.3 ± 28.8 U/L in abstainers (n = 277). Presence of CKD or cancer had no significant effect on uNAG concentration.
In all studied inhabitants uNAG concentration expressed in U/L increased linearly with urinary creatinine concentration (r = 0.1298, p < 0.001; Spearman’s rho = 0.2537). In multivariate linear regression model uNAG (in U/L) was associated with age and creatinine level. After adjustment for creatinine level, association between age and uNAG was demonstrated (Table 3).
Urinary 15-F2t-Isoprostane (15-F2t-IsoP)
Mean urinary 15-F2t-IsoP was significantly higher in men than that in women (7.98 ± 1.76 ng/mL vs 7.28 ± 2.12 ng/mL, p < 0.001). However, after adjustment for creatinine level, mean value of u15-F2t-IsoP in men (9.7 ± 7.5 ng/mg creatinine) was lower (p < 0.001) in comparison to women (11.4 ± 7.9 ng/mg creatinine).
A positive linear correlation between age and u15-F2t-IsoP concentration expressed in ng/mg creatinine (r = 0.2309, p < 0.001) was found. In smokers mean u15-F2t-IsoP was higher in comparison to non-smokers (7.94 ± 1.87 ng/mL vs 7.47 ± 2.03 ng/mL, p < 0.0228). However, after adjustment for creatinine level, there were no differences in u15-F2t-IsoP concentrations between smokers and non-smokers (Table 2).
Similar to uNAG, in men occupationally exposed to arsenic u15-F2t-IsoP concentrations without adjustment for creatinine level were higher than in men without occupational exposure (8.30 ± 1.34 ng/mL vs 7.44 ± 2.07 ng/mL, p < 0.01). Alcohol drinking had no important effect on u15-F2t-IsoP values which were 10.4 ± 6.28 ng/mL in occasional drinkers (n = 100), 7.50 ± 2.05 ng/mL in regular drinkers (n = 180), and 7.58 ± 2.06 ng/mL in abstainers (n = 636).
The occurrence of CKD also had no significant effect on u15-F2t-IsoP concentration which was 10.9 ± 7.5 ng/mL in subjects without CKD and 10.2 ± 5.9 ng/mL in patients diagnosed with CKD. However, in 59 persons diagnosed with cancer, u15-F2t-IsoP was significantly higher in comparison to people with no history of malignancy (11.8 ± 8.1 ng/mL vs 10.8 ± 7.4 ng/mL, p < 0.05).
Multiple regression analysis showed a positive linear correlation between ln(uAs) and u15-F2t-IsoP (n = 918, r = 0.2338, p < 0.001). Due to this observation, the next analysis was performed after dividing study participants into two groups: subjects with normal uAs (≤ 15 µg/L) and subjects with uAs exceeding the upper norm. In people with elevated uAs, u15-F2t-IsoP concentrations were higher (p < 0.001), whereas uNAG concentrations were similar comparing to normo-arsenic people. However, after adjustment for creatinine level, in people with elevated uAs, u15-F2t-IsoP concentrations were lower (p < 0.001) comparing to normo-arsenic subjects (Table 4). It may be explained by higher creatinine concentrations in the group with elevated uAs vs the group with normal uAs (118.3 ± 66.0 mg/dL vs 90.6 ± 58.5 mg/dL, p < 0.001).
After adjustment for creatinine level, the positive linear association between ln(uAs) and 15-F2t-IsoP was still observed in population with normal (p = 0.000000), as well as elevated uAs (p = 0.000000) (Figs. 3 and 4).

Association between logarithm of total arsenic in urine ln(uAs) and u15-F2t-IsoP concentration in people exposed to airborne arsenic with normal value of arsenic in urine (r = 0.4810, F = 200.8, p = 0.000000)

Association between logarithm of total arsenic in urine ln(uAs) and u15-F2t-IsoP in people exposed to airborne arsenic with arsenic in urine exceeding the norm (r = 0.4984, F = 8496, p = 0.000000)
Additionally, in the group of inhabitants with elevated uAs, a positive correlation between the sum of species ln(ΣuAs) and u15-F2t-IsoP was shown (r = 0.6150, p < 0.001) Fig. 5.

Association between logarithm of the sum of arsenic species in urine ln(uΣAs) and u15-F2t-IsoP in people with arsenic in urine exceeding the norm (r = 0.4984, F = 8496, p = 0.000000)
In the group of people diagnosed with cancer, a positive correlation between the sum of species ln(ΣuAs) and u15-F2t-IsoP was observed (n = 17; r = 0.6686, p < 0.003) (Fig. 6).

Association between logarithm of sum of arsenic species in urine ln(ΣuAs) and u15-F2t-IsoP in group of 17 people with elevated uAs, diagnosed with cancer (r = 0.6150, p < 0.001)
In multivariate linear regression model a significant association between sex (also age, creatinine and uAs) and u15 F2t-IsoP was shown. After adjustment for creatinine level, association between uAs and u15 F2t-IsoP was still significant (p = 0.000) (Table 5).
Moreover, an association between u15-F2t-IsoP and uNAG (r = 0.3267, F = 115.4, p < 0.0000, Spearman’s rho 0.3507) was demonstrated.
Urinary Creatinine Concentration
Urinary creatinine concentration decreased with age (r = − 0.4275, p < 0.001) was higher in men than in women (114.3 ± 66.1 mg/dL vs. 89.2 ± 57.8 mg/dL; p < 0.001), slightly higher in smokers than in non-smokers (105.1 ± 60.9 mg/dL vs 98.4 ± 63.2 mg/dL, p > 0.05), higher in workers exposed to arsenic than in non-exposed men (142.0 ± 69.1 mg/dL vs. 93.4 ± 59.5 mg/dL; p < 0.001), slightly higher in persons diagnosed with CKD than in persons without CKD (105.5 ± 68.9 mg/dL vs 97.2 ± 61.6 mg/dL; p > 0.05), and lower in patients diagnosed with cancer comparing to persons with no history of cancer (87.3 ± 60.9 mg/dL vs 98.1 ± 61.8 mg/dL, p < 0.05). A positive linear correlation between ln(uAs) and urinary creatinine was shown (r = 0.3108, p < 0.001).
Multiple Logistic Regression Models
Multiple logistic regression models were built in order to determine any relationships between elevated uAs (as a qualitative predictor) and increased uNAG or u15-F2t-IsoP concentrations (as dependent variables). For the purposes of this analysis, the value of the 75th quartile (Q75) for uNAG (47.0 U/L = 52.4 U/g creatinine) and u15-F2t-IsoP (9.0 ng/mL = 13.2 ng/mg creatinine) were adopted as cut-off points. Values higher than Q75 were considered to be elevated. Models were adjusted for urinary creatinine level. Influence of confounders, such as sex, age, smoking, alcohol drinking, and occupational exposure to As, was analyzed.
A significant association between cigarette smoking and increased uNAG was shown: ORuNAG = 1.67 (95% CI 1.1 to 2.56, p = 0,01). Total arsenic as an independent variable modifying uNAG remained outside the model.
After adjustment for urinary creatinine level and other confounders, there was a significant association between increased uAs and increased u15-F2t-IsoP: ORu15-F2t-IsoP = 1.31 (95% CI 1.08–1.59, p < 0.01). A significant association between sex and u15-F2t-IsoP, with men at a higher risk of elevated u15-F2t-IsoP was shown: OR15-F2t-IsoP = 1.24 (95% CI 1.03–1.49; p < 0.05). Additionally, an association between occupational exposure to arsenic, overlapping with environmental exposure, and increased u15-F2t-IsoP was demonstrated: OR15-F2t-IsoP = 2.24 (95% CI 1.22–4.11; p = 0.009).
Discussion
In this study involving residents of a copper smelter region, exposure to arsenic in the air is the most likely cause of elevated urinary arsenic levels. Although the most common way of exposure to arsenic is via contaminated drinking water, arsenic concentration in the local tap water was too low to significantly impact on urinary arsenic levels in the studied population. Additionally, to minimize the influence of diet, subjects were asked not to eat fish and seafood in the week preceding urine collection.
An increase in uNAG is linked with proximal renal tubule dysfunction (Zheng et al. 2015; Drake et al. 2002). Elevated uNAG levels have been observed in patients diagnosed with diabetic nephropathy, interstitial nephritis or kidney transplant rejection, and subjects exposed to nephrotoxic agents (Kim et al. 2016a, b; Wang et al. 2019). An increase in uNAG activity may also reflect an increase in lysosomal activity without cell damage (Liangos et al. 2007).
In our study the median (interquartile range) uNAG concentration was 24.0 (11.0–52.6) U/g creatinine. This value was higher than uNAG concentrations observed by authors of studies carried out on populations that had not been exposed to arsenic. The median uNAG concentration was 10.1 (6.11–18.8) U/g creatinine in 561 persons diagnosed with diabetes mellitus (Kim et al. 2016b), 22.55 (13.26–37.75) U/g creatinine in 1025 people hospitalized in intensive care units but without features of acute kidney insufficiency (Wang et al. 2019), 2.27 (0.65–10.67) U/g creatinine in 46 patients diagnosed with bladder cancer (Marchewka et al. 2018), 1.61 (0.94–2.49) U/g creatinine in 349 healthy men, and 2.05 (1.22–3.22) U/g creatinine in 282 healthy women (Solbu et al. 2016).
In our analysis, some relationships between uNAG and factors, such as sex, age, and smoking, changed after uNAG concentration normalization to urinary creatinine concentrations. Urinary NAG levels adjusted for urinary creatinine concentrations were independent of sex, similar to other studies (Udomah et al. 2012; Pennemans et al. 2013), and were negatively correlated with age, in contrast to the Bogalusa Heart Study (Agirbasli et al. 1996). It should be noted that while the Bogalusa study involved subjects under 32, our study participants’ ages ranged from 19 to 82. In our study, a borderline (p = 0.05) interaction between sex, smoking, and arsenic impacting uNAG was found. A clear association between cigarette smoking and elevated (greater than Q75) uNAG was observed (OR uNAG = 1.67, 95% CI 1.1–2.56, p = 0.01). Not only arsenic but also other nephrotoxic metals contained in tobacco smoke, including cadmium, may be responsible for this association. Some studies on sensitive biomarkers of renal dysfunction support the hypothesis that cadmium and inorganic arsenic synergistically cause renal injury (James et al. 2015; Nordberg et al. 2005). In our study, uAs was positively associated with urinary creatinine concentration. However, uAs was not a predictor of increased uNAG.
Nevertheless, uAs in interaction with male sex and smoking was associated with increased uNAG. In other studies, uAs was a significant determinant of uNAG, but only in subjects with uNAG higher than 7.4 U/g creatinine (75th quartile) (Eom et al. 2011). In this study, the Q75 for uNAG was more than 7 times higher (52.4 U/g creatinine), possibly due to a relatively high degree of kidney dysfunction.
It is also worth noting that in people with uNAG concentrations greater than Q75, a significant relationship between uNAG and cigarette smoking was found. In the entire study group, there were no significant differences in uNAG either between smokers and non-smokers or between sub-groups based on sex, age, or the presence of occupational exposure to arsenic. It can be concluded that cigarette smoking does not induce proximal tubular injury but aggravates the existing damage.
On the other hand, in the studied population of inhabitants, uNAG concentration expressed in U/L increased linearly with urinary creatinine concentration. This observation is suggestive of a significant relationship between glomerular filtration and NAG urinary excretion. Simultaneously, a slightly higher urinary creatinine concentration in smokers vs non-smokers may explain the similar uNAG values in smokers and non-smokers, after the uNAG results were adjusted for urinary creatinine levels (Table 2). In the literature, there has been mixed evidence for an association between arsenic exposure and uNAG levels (Zheng et al. 2014). Urinary 15-F2t-IsoP seems to be a better candidate biomarker of airborne arsenic exposure than uNAG. Isoprostanes are natural products of non-enzymatic membrane lipid peroxidation. Due to their long half-life and chemical stability, isoprostanes are considered to be the most reliable indicators of oxidative stress in vivo. There is some evidence that they have a much better diagnostic and prognostic value than thiobarbituric acid reactive substances or malondialdehyde in relation to diseases associated with oxidative stress, such as atherosclerosis or carcinoma (Dorjgochoo et al. 2012; Milne et al. 2015). 15-F2t-IsoP might be a good marker of systemic oxidative stress because it is derived from arachidonic acid. It is neither subject to oxidative artefacts associated with sampling nor influenced by dietary lipid content, and it remains stable at − 80 °C (Morrow et al. 1995).
Although changes in isoprostanes levels are not specific to arsenic toxicity, the relationship between arsenic and isoprostanes seems to be clear. Arsenic induces a loss of mitochondrial membrane potential and induces the generation of ROS (Zhang et al. 2014; Jomova et al. 2011). One of the actions of ROS is non-enzymatic peroxidation of polyunsaturated fatty acids in membrane phospholipids. One of the substrates for this reaction is arachidonic acid, and isoprostanes are primarily products of arachidonic acid peroxidation. Both arsenic and isoprostanes are excreted mainly with the urine.
The results of our study show that among the analyzed parameters, elevated uAs is the only predictor of increased u15-F2t-IsoP (OR = 1.31, 95% CI 1.08–1.59, p < 0.01). Furthermore, a positive linear relationship between total arsenic and u15-F2t-IsoP concentrations was found for both elevated and normal uAs values (Figs. 3 and 4). In a study from Farzan et al., not only total uAs but also % MMA was positively associated with u15-F2t-IsoP. The authors suggested that a higher ability to metabolize inorganic As is negatively associated with oxidative stress markers (Farzan et al. 2015). In our study, a positive correlation between the sum of arsenic species and u15-F2t-IsoP (r = 0.6150) was found in people with elevated uAs (Fig. 5). Simultaneously, % MMA was significantly lower in smokers, whereas urinary ΣAs and iAs were higher in comparison to never-smokers (Table 1). In the linear regression model adjusted for sex, age, urinary creatinine, alcohol drinking, and the presence of occupational exposure to arsenic, CKD, or cancer, smoking was positively associated with ΣuAs (95% CI 1.24–5.62; p < 0.01) as well as with iAs (95% CI 2.01–18.05, p < 0.01). These relationships indicate a significant connection between smoking and urinary inorganic arsenic, whereas increased % iAs co-existing with decreased % MMA suggests impaired inorganic arsenic metabolism in smokers. Since inorganic arsenic is known to be a more potent carcinogen and pro-atherosclerotic factor than organic arsenic, diagnostic measurement of u15-F2t-IsoP may be particularly important in populations of smokers exposed to arsenic. Although in our study a representation of people with elevated uAs and a history of malignancy was relatively small (17 persons), a positive correlation between the sum of arsenic species and u15-F2t-IsoP (Fig. 6) warrants further research.
In the assessment of u15-F2t-IsoP, the significance of factors, such as sex and age, should be considered. In our study, the interpretation of these relationships depended on adjustment for urinary creatinine level. Its concentration was higher in men than in women, positively correlated with uAs and negatively associated with age. After normalization to urinary creatinine, urinary isoprostane concentration increased with age and was higher in women than in men (Table 2). In a study from Taylor et al., plasma isoprostane levels were higher in women than in men and higher in smokers than in non-smokers (Taylor et al. 2008). In our study, u15-F2t-IsoP values were higher in smokers than in non-smokers, similar to other studies (Moon et al. 2013; Morrow et al. 1995), but only when analyzed without adjustment for creatinine level. After the adjustment, no association between smoking and u15-F2t-IsoP was found. Importantly, while adjusting isoprostane level for creatinine concentration had an impact on relationships between gender, age, or smoking and u15-F2t-IsoP, it had no effect on the positive relationship between arsenic and u15-F2t-IsoP (Table 5).
The reference value (RV 95) for uAs is 15 μg/L for both adults and children who have not consumed fish in the 48 h preceding sample collection. The geometric mean concentrations of uAs in European populations range from 4 to 16 μg/g creatinine (Schulz et al. 2011; Wąsowicz 2020). In our study, uAs levels above normal were found in 29% of men and 25% of women. Occupational exposure to arsenic was positively associated with urinary arsenic and its species, indicating that copper smelter workers are at a higher risk of arsenic toxicity.
Our study has several limitations, including the lack of detailed information on participant health status and lifestyle factors (such as diet) potentially influencing the red-ox system, the lack of data on arsenic species concentrations in the group with normal uAs levels, and the lack of repeated measurements of uAs, which would allow us to assess its variability over time. Finally, we evaluated associations between arsenic exposure and oxidative stress using ELISA for u15-F2t-IsoP measurements; however, gas chromatography–tandem mass spectrometry (GC–MS) is considered to be the gold standard (Liu et al. 2009).
Despite the aforementioned limitations, in our research, we have clearly shown that an increase in systemic oxidative stress is associated with an increase in urinary arsenic in a population exposed to airborne arsenic. This finding is supported by observed positive linear correlations between total urinary arsenic or arsenic forms and urinary F2t-isoprostane. We found that elevated total urinary arsenic is a predictor of elevated urinary isoprostane levels. Oxidative stress, which is associated with an increase in urinary arsenic, may be related to the development of diseases, such as atherosclerosis and cancer. Based on the results from our study, it may be hypothesized that chronic exposure to airborne arsenic may lead to kidney damage via oxidative stress. This hypothesis is supported by the observed positive relationship between uAs and creatinine, creatinine and isoprostane, and urinary isoprostane and uNAG. Although cigarette smoking, unlike urinary arsenic, was a predictor of increased uNAG concentration, the association between smoking and uNAG concerned people with uNAG values over the 75th quartile. In this group, cigarette smoking has been shown to be an important factor aggravating renal proximal tubule function. Smoking has also been found to be associated with an increase in urinary inorganic arsenic, which is potentially more carcinogenic than organic forms.
Conclusions
In a population chronically exposed to airborne arsenic, an increase in total urinary arsenic is associated with kidney damage and an increase in systemic oxidative potential. Urinary 15-F2t-isoprostane may be a good biomarker of exposure to airborne arsenic. The monitoring of urinary 15-F2t-IsoP levels in residents of copper smelter zones may be useful in the context of the prevention of diseases potentially related to arsenic exposure, such as atherosclerosis and cancer.
Data Availability
All raw data can be made available to verify applications at the Editorial Board’s request.
References
Agency for Toxic Substances Disease Registry (ATSDR) (2007) Toxicological Profile for Arsenic. U. S. Department of Health and Human Services, Public Health Service, Atlanta
Agirbasli M, Radhakrishnamurthy B, Jiang X, Bao W, Berenson GS (1996) Urinary N-acetyl-β-d-glucosaminidase changes in relation to age, sex, race, and diastolic and systolic blood pressure in a young adult biracial population The Bogalusa heart study. Am J Hypertension 9:157–161
Air quality in Europe 2015 report. European Environment Agency. EEA Report No 5/2015 http://www.eea.europa.eu/publications/air-quality-in-europe-2015/download
Bedir A, Ozener IC, Emerk K (1996) Urinary leucine aminopeptidase is a more sensitive indicator of early renal damage in non-insulin-dependent diabetics than microalbuminuria. Nephron 74:110–113
Che-Jung C, D’Souza P, Ryan P, Dana B (2018) The precision and accuracy of urinary creatinine analysis for correction of urine dilution in biological monitoring measurements. ISEE Conf Abstr. https://doi.org/10.1289/isesisee.2018.P01.2670
Chen Y, Santella RM, Kibriya MG, Wang Q, Kappil M, Verret WJ et al (2007) Association between arsenic exposure from drinking water and plasma levels of soluble cell adhesion molecules. Environ Health Perspect 115:1415–1420
Cullen WR, McBride BC, Reglinski J (1984) The reaction of methylarsenicals with thiols: some biological implications. J Inorganic Biochem 21:179–194
Dangleben NL, Skibola CF, Smith MT (2013) Arsenic immunotoxicity: a review. Environ Health 12:73. https://doi.org/10.1186/1476-069X-12-73
Dorjgochoo T, Gao YT, Chow WH, Shu XO, Yang G, Cai QY et al (2012) Major metabolite of F2-isoprostane in urine may be a more sensitive biomarker of oxidative stress than isoprostane itself. Am J Clin Nutr 96:405–414
Drake PL, Krieg E, Teass AW, Vallyathan V (2002) Two assays for urinary N-acetyl-beta-D-glucosaminidase compared. Clin Chem 48:1604–1605
Engström KS, Vahter M, Johansson G, Lindh CH, Teichert F, Singh R et al (2010) Chronic exposure to cadmium and arsenic strongly influences concentrations of 8-oxo-7, 8-dihydro-2′-deoxyguanosine in urine. Free Radic Biol Med 48:1211–1217
Eom SY, Lee YC, Yim DH, Lee CH, Kim YD, Choi BS et al (2011) Effects of low-level arsenic exposure on urinary N-acetyl-β-D-glucosaminidase activity. Hum Exp Toxicol 30:1885–1891
Farzan SF, Chen Y, Rees JR, Zens MS, Karagas MR (2015) Risk of death from cardiovascular disease associated with low-level arsenic exposure among long-term smokers in a US population-based study. Toxicol Appl Pharmacol 287:93–97
Farzan SF, Howe CG, Zens MS, Palys T, Channon JY, Li Z, Chen Y et al (2017) Urine arsenic and arsenic metabolites in U.S. adults and biomarkers of inflammation, oxidative stress, and endothelial dysfunction: a cross-sectional study. Environ Health Perspect. 125:127002. https://doi.org/10.1289/EHP2062
Hu Y, Li J, Lou B, Wu R, Wang G, Lu C, Wang H, Pi J, Xu Y (2020) The role of reactive oxygen species in arsenic toxicity. Biomolecules 5:240. https://doi.org/10.3390/biom10020240
Huang M, Choi SJ, Kim DW, Kim NY, Park CH, Yu SD et al (2009) Risk assessment of low-level cadmium and arsenic on the kidney. J Toxicol Environ Health 72:1493–1498
Hughes MF, Beck BD, Chen Y, Lewis AS, Thomas DJ (2011) Arsenic exposure and toxicology: a historical perspective. Toxicol Sci 123:305–332
James KA, Byers T, Hokanson JE, Meliker JR, Zerbe GO, Marshall JA (2015) Association between lifetime exposure to inorganic arsenic in drinking water and coronary heart disease in Colorado residents. Environ Health Perspect 123:128–134
Jomova K, Jenisova Z, Feszterova M, Baros S, Liska J, Hudecova D, Rhodes CJ, Valko M (2011) Arsenic: toxicity, oxidative stress and human disease. J Appl Toxicol 31:95–107
Karim MR, Rahman M, Islam K, Al Mamun A, Hossain S, Hossain E et al (2013) Increases in oxidized low-density lipoprotein and other inflammatory and adhesion molecules with a concomitant decrease in high-density lipoprotein in the individuals exposed to arsenic in Bangladesh. Toxicol Sci 135:17–25
Kile ML, Cardenas A, Rodrigues E, Mazumdar M, Dobson C, Golam M, Quamruzzaman Q, Rahman M, Christiani DC (2016) Estimating effects of arsenic exposure during pregnancy on perinatal outcomes in a Bangladeshi cohort. Epidemiology 27:17–181
Kim YD, Eom SY, Yim DH, Kim IS, Won HK, Park CH et al (2016) Environmental exposure to arsenic, lead, and cadmium in people living near Janghang copper smelter in Korea. J Korean Med Sci 31:489–496
Kim SR, Lee Y, Lee SG, Kang ES, Cha BS, Kim J et al (2016) Urinary N-acetyl-β-D-glucosaminidase, an early marker of diabetic kidney disease, might reflect glucose excursion in patients with type 2 diabetes. Medicine. https://doi.org/10.1097/MD.0000000000004114
Kozłowska L, Janasik B, Nowicka K, Wąsowicz W (2019) A urinary metabolomics study of a Polish subpopulation environmentally exposed to arsenic. J Trace Elem Med Biol 54:44–54
Ledda C, Iavicoli I, Bracci M, Avola R, Senia P, Santarelli L, Pomara C, Rapisarda V (2018) Serum lipid, lipoprotein and apolipoprotein profiles in workers exposed to low arsenic levels: lipid profiles and occupational arsenic exposure. Toxicol Lett 282:49–56
Lemaire M, Negro Silva LF, Lemarié CA, Bolt AM, Flores Molina M, Krohn RM et al (2015) Arsenic exposure increases monocyte adhesion to the vascular endothelium, a pro-atherogenic mechanism. PloS One 10:e0136592. https://doi.org/10.1371/journalpone.0136592
Liangos O, Perianayagam MC, Vaidya VS, Han WK, Wald R, Tighiouart H et al (2007) Urinary N-acetyl-ß-(D)-glucosaminidase activity and kidney injury molecule-1 level are associated with adverse outcomes in acute renal failure. J Am Soc Nephrol 18:904–912
Liu W, Morrow JD, Yin H (2009) Quantification of F2-isoprostanes as a reliable index of oxidative stress in vivo using gas chromatography-mass spectrometry (GC-MS) method. Free Radic Biol Med 47:1101–1107
Marchewka Z (2006) Low molecular weight biomarkers in the nephrotoxicity. Adv Clin Exp Med 15:1129–1138
Marchewka Z, Szymańska B, Dembowski J, Długosz A, Piwowar A (2018) Low molecular weight proteins and enzymes in the urinary of patients with bladder cancer—a pilot study. Cent Eur J Urol 71:280–286
Medrano MA, Boix R, Pastor-Barriuso R, Palau M, Damián J, Ramis R et al (2010) Arsenic in public water supplies and cardiovascular mortality in Spain. Environ Res 110:448–454
Milne GL, Dai Q, Roberts LJ (2015) The isoprostanes-25 years later. Biochim Biophys Acta 1851:433–445
Minuz P, Patrignani P, Gaino S, Degan M, Menapace L, Tommasoli R et al (2002) Increased oxidative stress and platelet activation in patients with hypertension and renovascular disease. Circulation 106:2800–2805
Monrad M, Ersbøll AK, Sørensen M, Baastrup R, Hansen B, Gammelmark A et al (2017) Low-level arsenic in drinking water and risk of incident myocardial infarction: a cohort study. Environ Res 154:318–324
Moon KA, Guallar E, Umans JG, Devereux RB, Best LG, Francesconi KA et al (2013) Association between exposure to low to moderate arsenic levels and incident cardiovascular disease. A prospective cohort study. Ann Intern Med 159:649–659
Morrow JD, Frei B, Longmire AW, Gaziano JM, Lynch SM, Shyr Y et al (1995) Increase in circulating products of lipid peroxidation (F2-isoprostanes) in smokers - smoking as a cause of oxidative damage. N Engl J Med 332:1198–1203
Nordberg GF, Jin T, Hong F, Zhang A, Buchet JP, Bernard A (2005) Biomarkers of cadmium and arsenic interactions. Toxicol Appl Pharmacol 206:191–197
Pellizzari ED, Clayton CA (2006) Assessing the measurement precision of various arsenic forms and arsenic exposure in the National Human Exposure Assessment Survey (NHEXAS). Environ Health Perspect 114:220–227
Pennemans V, Rigo JM, Faes C, Reynders C, Penders J, Swennen Q (2013) Establishment of reference values for novel urinary biomarkers for renal damage in the healthy population: are age and gender an issue? Clin Chem Lab Med 51:1795–1802
Prakash C, Soni M, Kumar V (2015) Biochemical and molecular alterations following arsenic-induced oxidative stress and mitochondrial dysfunction in rat brain. Biol Trace Elem Res 167:121–129
Schulz CM, Heudorf WU, Kolossa-Gehring M (2011) Update of the reference and HBM values derived by the German Human Biomonitoring Commission. Int J Hyg Environ Health 215:26–35
Solbu MD, Norvik JV, Storhaug HM, Eriksen BO, Melsom T, Eggen AE et al (2016) The association between adiponectin, serum uric acid and urinary markers of renal damage in the general population: cross-sectional data from the Tromsø study. Kidney Blood Press Res 41:623–634
Straif K, Benbrahim-Tallaa L, Baan R, Grosse Y, Secretan B, El Ghissassi F et al (2009) A review of human carcinogens. Part C: metals, arsenic, dusts, and fibres. Lancet Oncol 10:453–454
Styblo M, Del Razo L, Vega L et al (2000) Comparative toxicity of trivalent and pentavalent inorganic and methylated arsenicals in rat and human cells. Arch Toxicol 74:289–299
Sundaram N, Bennett M, Wilhelm J, Kim MO, Atweh G, Devarajan P et al (2011) Biomarkers for early detection of sickle nephropathy. Am J Hematol 86:559–566
Taylor WA, Bruno RS, Traber MG (2008) Women and smokers have elevated urinary F2-isoprostane metabolites; a novel extraction and LC-MS methodology. Lipids 43:925–936
Udomah FP, Ekrikpo UE, Effa E, Salako B, Arije A, Kadiri S (2012) Association between urinary N-acetyl-beta-D-glucosaminidase and microalbuminuria in diabetic black Africans. Int J Nephrol. https://doi.org/10.1155/2012/235234
Wang L, Deng Y, Zhai Y, Xu F, Li J, Zhang D et al (2019) Impact of blood glucose levels on the accuracy of urinary N-acety-β-D-glucosaminidase for acute kidney injury detection in critically ill adults: a multicenter, prospective, observational study. BMC Nephrol 20:186. https://doi.org/10.1186/s12882-019-1381-3
Wąsowicz W (2019) HBM4 EU Scoping document. Prioritized substance group: Arsenic. Horizont 2020 Programme. pp 10–11
WHO (2011) Arsenic in Drinking-water. Background document for development of WHO Guidelines for Drinking-water Quality, World Health Organization, Geneva
World Health Organization International Agency for Research on Cancer IARC (2002) Some drinking-water disinfectants and contaminants, including arsenic. The views and expert opinions of an IARC Working Group on the Evaluation of Carcinogenic Risks to Humans, Lyon, vol 84. WHO, Geneva
Zhang J, Shen H, Xu W, Xia Y, Barr DB, Mu X et al (2014) Urinary metabolomics revealed arsenic internal dose-related metabolic alterations: a proof-of-concept study in a Chinese male cohort. Environ Sci Technol 2014(48):12265–12274
Zheng L, Kuo CC, Fadrowski J, Agnew J, Weaver VM, Navas-Acien A (2014) Arsenic and chronic kidney disease: a systematic review. Curr Environ Health Rep 1:192–207
Zheng LY, Umans JG, Yeh F, Francesconi KA, Goessler W, Silbergeld EK et al (2015) The association of urine arsenic with prevalent and incident chronic kidney disease: evidence from the Strong Heart Study. Epidemiology 26:601. https://doi.org/10.1097/EDE.0000000000000313
Acknowledgements
The authors thank the authorities of the Copper Health Center for sharing the results of arsenic in urine.
Funding
This work was supported by the Wroclaw Medical University [Grant No. KO/68/U/17].
Author information
Authors and Affiliations
Contributions
AS is the author of the research concept, statistical analysis of data, and made a big contribution to the writing of the manuscript. MSC analyzed and interpreted patient data and took part in writing the manuscript. BT performed biochemical determinations with data analysis. AW performed biochemical determinations with data analysis. MS organized research, participated in the analysis of results. LG organized research and participated in the analysis of results.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Consent to Participate
All subjects provided written, informed consent to participate in this study.
Consent for Publication
This study received the written consent for publication.
Ethical Approval
This work was conducted in accordance with the Declaration of Helsinki (1964). The study received the ethics approval of the local Bioethics Committee.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Skoczynska, A., Skoczynska, M., Turczyn, B. et al. Exposure to Arsenic in the Air and 15-F2t-Isoprostane in Urine in a Sub-population of Inhabitants of a Copper Smelter Region. Expo Health 13, 403–418 (2021). https://doi.org/10.1007/s12403-021-00392-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12403-021-00392-x