
Abstract
Background
Understanding how individuals currently perceive healthy eating is essential for developing food policies and dietary recommendations that improve the health and well-being of populations. The purpose of this qualitative evidence synthesis was to systematically outline the views and understandings of healthy eating, focusing on how foods are classified as healthy and unhealthy and what meanings are attached to food and eating by the general adult population in high-income countries.
Methods
A systematic search of four electronic databases was conducted and yielded 24 relevant primary qualitative studies of generally healthy, community-dwelling adults.
Results
Thematic synthesis of the included studies identified three analytic themes: constructions of healthy and unhealthy eating, considerations on dietary recommendations, and meanings attached to food and eating. Study participants generally understood what constitutes a healthy and unhealthy diet which was in line with dietary recommendations, but those of lower socioeconomic status exhibited gaps in nutrition knowledge. Participants expressed diverse opinions on dietary recommendations, including skepticism and a lack of trust. Food and eating were associated with various meanings, including pleasure, stress relief, and feelings of guilt. Moral, health, and sociocultural considerations also played a role in dietary behaviors.
Conclusions
The findings suggest that improving population diet requires considering how dietary recommendations are phrased and communicated to ensure that healthy eating is associated with pleasure and immediate well-being. This review provides valuable insights for developing consumer-oriented, practicable, and acceptable food policies and dietary recommendations that effectively improve population health and well-being.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is substantial evidence for a strong link between noncommunicable diseases (NCDs) and dietary habits [1,2,3,4]. According to the Global Burden of Disease study group, suboptimal diets are a major risk factor for various NCDs, contributing to a significant proportion of global deaths and disability-adjusted life years [1]. The prevalence of overweight, obesity [5], and NCDs [6] continues to rise worldwide, including in high-income countries, despite efforts to develop and implement strategies and interventions aimed at improving population diets and health [7, 8]. Previously, it has been argued that public health nutrition interventions targeting factors on the individual level (e.g., improving nutrition knowledge through dietary guidelines) will remain ineffective if persisting environmental barriers are not addressed [9]. Therefore, it is crucial to implement effective strategies that account for the real-life experiences of individuals and address the complex interplay of factors that influence dietary behaviors.
It is widely recognized that good health can be attained and maintained by following the commonly named guidelines for healthy eating [10,11,12]. Determinants across the individual, social, lived, and food environments have been found to influence food choices and dietary behaviors [9, 13], and particularly social and environmental factors have been reported as barriers to healthy eating [9]. In addition to these environmental determinants, intrapersonal constructs such as beliefs, attitudes, motivations, meanings attached to foods, values, cultural and social norms, self-identity [13], and nutrition knowledge [13, 14] have also been identified to influence food-related behaviors. For instance, viewing oneself as a healthy eater was a significant predictor for healthy eating behaviors [15, 16], while attitudes toward healthy food-related behaviors and the perceived influence of diet on health were also strong predictors of healthy eating behaviors [17].
However, many of these constructs are dependent on individual perceptions of what constitutes a healthy diet [10]. Quantitative research has provided important observations into laypeople’s conceptualization of a healthy diet. In a study of Japanese adults, maintaining a balanced diet, eating plenty of vegetables, avoiding late-nigh eating, and incorporating a variety of foods were identified as key components of healthy eating [18]. Additionally, it was found that laypeople use criteria similar to experts to evaluate the healthiness of foods but tend to overlook certain factors such as saturated fat, protein, and sodium. In addition, while laypeople were able to evaluate individual food products, they struggled to assess the healthiness of entire meals [19]. Another study found that participants were divided on whether a food can be classified as healthy based on the food’s nutritional content or whether other factors affect whether a food is healthy. Factors influencing perceptions of a food’s healthiness included micronutrient content and freshness/processing [20].
A key limitation of quantitative studies in this domain is the dependence on closed questions. Qualitative research can provide more and more differentiated subjective meanings, beliefs, and attitudes, as these can be highly individual [21]. Quantitative research, such as the one mentioned above, often does not capture subjective concepts of healthy eating. Here, qualitative research provides a more in-depth and flexible approach to, for instance, investigate people’s conceptualization of a healthy diet through semi-structured interviews or focus group discussions. Several primary qualitative studies have previously investigated healthy eating perception and the meanings people attach to food and eating (e.g., [22,23,24,25,26]). Furthermore, evidence derived from qualitative research can be valuable in informing quantitative approaches (and vice versa), such as interventions or the assessment of common themes in large study samples.
Qualitative evidence synthesis (QES) is an umbrella term for methodologies used in the systematic review of primary qualitative research and aims to integrate findings that are often of nuanced or sensitive nature. QES allow researchers to gain a comprehensive and in-depth understanding of people’s experiences, views, beliefs, and priorities for a variety of issues, including health-related topics [27]. They do not allow quantifying or interpreting the sizes of associations, but can be helpful tools to provide systematic overviews over emerging fields with predominantly qualitative research. Recently, researchers have investigated factors perceived to influence healthy eating [9], healthy eating beliefs and the meaning of food in populations with low socioeconomic status [28], and healthy eating strategies for socioeconomically disadvantaged populations [29] by performing QES [30]. However, apart from one review published in 2005 investigating the perceptions of healthy eating [10] and another published in 2012 investigating healthy eating as discussed in qualitative research [11], no qualitative review has been conducted exploring how the general adult population in high-income countries perceive healthy eating and what meanings are attached to food and eating—and whether such perceptions are socially stratified. However, this in-depth understanding is crucial in the development of consumer-oriented, practicable, and acceptable food policies and dietary recommendations, which can effectively improve health and well-being of populations. Additionally, it is important to consider current attitudes to ensure that interventions and recommendations align with people’s needs and preferences [9].
Therefore, this QES aims to synthesize the literature regarding the views and understandings of healthy eating and the conceptualization of a healthy diet. In addition, it will explore which meanings are attached to healthy eating and foods will be explored. If feasible, differences in understanding by socioeconomic status will be investigated. The focus of this review is on the general adult population, as children and adolescents may have less autonomy in making their own dietary choices. Furthermore, the study focuses on individuals in high-income countries due to potential variations in cultural, socioeconomic, and environmental factors between high-income and low- or middle-income countries.
Methods
A systematic review of qualitative literature was conducted according to a pre-specified protocol registered with the International Prospective Register of Systematic Reviews (PROSPERO: CRD42021269656). Thematic synthesis, as described by Thomas and Harden [31], was employed, and reporting was guided by the ENTREQ statement [32]. Ethical approval was not required as this was an evidence synthesis of existing research.
Search Strategy
A first search was conducted in September 2021 across four electronic databases (MEDLINE, CINAHL, PsycINFO, Scopus). The search terms and their combinations were guided by the SPIDER tool for QES [33]. Terms encompassed five key search concepts: “adults,” “high-income countries,” “healthy eating,” “understanding,” and “qualitative research.” These concepts are related to the sample, phenomenon of interest, study design, evaluation, and type of research. Following a previously described approach to identifying high-income countries [9], the literature search was restricted to countries that are classified as high-income by the World Bank [34] and are also members of the Organization for Economic Co-operation and Development (OECD) [35]. The literature search was repeated in January 2023 to include recently published articles. Table S1 in the Electronic Supplementary Material provides a list of search terms.
Eligibility Criteria
Articles were eligible if they focused on community-dwelling adults (18 years or older) as it was assumed that they can make and report on their dietary behaviors independently, and dietary recommendations are generally addressed at this group [12]. Populations composed exclusively of children, adolescents, older adults (60 years or older), migrant, and native or indigenous groups, participants with pre-existing medical conditions, or women who are pregnant or breastfeeding were excluded as these groups were assumed to conceptualize healthy eating differently and would ultimately deserve their own review. Only the layperson’s perspective of healthy eating was of interest for this review; thus, studies examining the opinions of nutrition and health experts were excluded. Studies were excluded if the focus was on participants’ views on the dietary behaviors of others (e.g., parents expressing their views on child nutrition) and perspectives on healthy eating after an intervention. Studies were only included if the objectives or outcomes explored participants’ views and understandings of a healthy diet or their relationship with food and eating and were excluded if the outcomes only indirectly related to their opinions (e.g., external factors influencing dietary behaviors, healthy lifestyles in general, weight maintenance, behavior change) or exclusively focused on the consumption of specific foods, food groups, or diets. Qualitative primary research using methods such as interviews, focus groups, open-ended surveys, and only the qualitative components of mixed methods studies were included in this investigation. Studies were required to have incorporated participant comments or quotes to allow for independent interpretation of their perspectives. Quantitative research was excluded. Non-English full-text publications were excluded from this qualitative review.
Study Selection Process
References identified through the search strategy were uploaded into EndNote version X7 (Thomson Reuters), and duplicate citations were removed by the lead author (UK). In the second search, previously identified publications were retrieved due to no date limit set in some databases and were subsequently removed. The remaining records were uploaded to the Rayyan web application for screening. Two reviewers (UK, VH) independently screened all titles and abstracts retrieved from the literature searches, excluding articles not meeting the eligibility criteria. After comparing results for the title-abstract screening, the full texts of remaining publications were independently screened by the same authors for eligibility. Publications that met the eligibility criteria were included in the qualitative synthesis. Disagreements at each stage of the selection process were resolved through discussion between the two co-authors; a third author (BS) was consulted when consensus was not achieved. Figure 1 shows the PRISMA flow diagram, which summarizes the article identification and selection process [36].

Modified PRISMA 2020 flow chart [36]
Quality Assessment
The Critical Appraisal Skills Program (CASP) qualitative checklist was used to assess the methodological quality of included studies [37]. A qualitative checklist examines the quality across ten items, including results, methodology, research design, recruitment strategy, data collection, reflexivity, ethical considerations, and data analysis. This tool was chosen due to its widespread use in health-related systematic reviews of qualitative studies [37] and to promote consistency across reviews. Although there was an agreement not to exclude studies based on quality assessment, conducting a methodological appraisal offers transparency and insight into the strengths and limitations of the included research [30]. Two reviewers (UK, VH) independently performed the quality assessment, subsequently discussed, and any discrepancies were solved through discussion.
Data Extraction and Synthesis
Key information from eligible studies was extracted into a Microsoft Excel template, including authors and year of publication, aim(s), study location, sample size and characteristics (gender, ethnicity, socioeconomic status), data collection methods, data analysis methods, and outcomes. Two reviewers (UK, VH) independently extracted relevant data from each study and cross-checked for accuracy.
Qualitative synthesis involves gathering and combining results from multiple primary qualitative research studies. For data analysis the thematic synthesis approach described by Thomas and Harden [31] was used. This method was selected over alternative synthesis methods (e.g., framework synthesis, meta-ethnography), as it aims to attain a higher level of analytical abstraction by rigorously investigating overlap and shared elements among studies, can be used to synthesize findings in a wide range of inquiries, and allows for the inductive and deductive identification and development of themes which collectively reflect the findings of the included studies [30]. The synthesis was conducted by following these three steps: (1) open line-by-line coding of article findings; (2) development of descriptive themes to translate concepts between studies; and (3) generation of analytical themes and interpretations to generate further ideas, explanations, and hypotheses [31].
All text under the heading “results,” “findings,” or similar was extracted from each publication and uploaded into MAXQDA Analytics Pro 2020 (Foxit Software Company) for line-by-line coding. The findings sections of five randomly selected publications were inductively coded by one reviewer (UK) to develop a code book. A second reviewer (VH) then cross-checked these codes for quality assurance. Both reviewers met to compare codes for consistency, and consensus was found through discussion. The remaining articles were coded by either UK or VH, cross-checked for accuracy by the other reviewer, and re-checked later on in the process, leading to intensive exploration of the material. New categories were added to the codebook when deemed necessary.
Codes focused on healthy and unhealthy eating, health aspects with regard to eating, dietary recommendations, meanings attached to food, and influencing factors on dietary behaviors. Differences between groups of varying socioeconomic status were checked by comparing attitudes expressed toward a discussed theme for low-income cohorts and cohorts of higher or mixed/unspecified socioeconomic status. Descriptive themes were developed by merging, grouping, and reorganizing codes and categories in an iterative process while remaining close to the original findings. Categories were organized into a thematic structure so that individual codes could be assigned to multiple descriptive themes. The lead author re-read the findings from primary studies throughout this process to ensure themes reflected data from primary studies, and all authors engaged in an ongoing discussion to refine categories and themes.
An iterative process involving inductive and deductive methods was used to develop analytical themes. The descriptive themes were analyzed in terms of their relationships to one another, and this analysis was used to address the research questions. Final descriptive themes were consolidated into mutually exclusive analytical themes.
Results
Summary of Included Studies
After removal of duplicates, a total of 1829 articles were identified during both literature searches, of which 24 met the eligibility criteria of this review. Detailed characteristics of included studies are presented in Table 1. Studies were published between 2007 and 2023, with more than half published within the last ten years (n = 13). Studies were conducted in the USA (n = 8), Australia (n = 7), Europe (n = 5), and Canada (n = 4). Study sample sizes ranged from 12 to 195 participants, totaling to 1322 participants. The populations exhibited a certain degree of diversity and included a wide range of ages (13–81 years). Of the 19 studies that had included men and women and had specified distribution, 15 studies consisted of > 50% women. While several studies (n = 13) did not specify the ethnic background of their population, six studies consisted of relatively ethnically diverse cohorts, and four studies solely included participants of African American or African Canadian ethnicity. Most studies (n = 16) provided some information on socioeconomic indicators (e.g., education, income, employment status). Four cohorts were described as low income by the respective authors. Qualitative data collection methods included interviews (n = 12), focus groups (n = 9), a combination of interviews and focus groups (n = 1), short written essays (n = 1), and online discussions on a message board (n = 1). Direct participant quotations included in the analysis ranged from 2 to 58 quotes per study.
Most studies (n = 18) met at least eight out of ten CASP criteria. Only six of the 24 articles met the criteria for all quality domains. Almost all 24 articles provided clear statements on aims, qualitative methodology, research design, and statement of findings; however, reflexivity was insufficient or unclear in 15 studies. The quality assessment outcomes can be found in Table S2 in the Electronic Supplementary Material.
Results of Synthesis
Thematic synthesis of included primary studies yielded three main themes illuminating understanding and meaning of healthy eating and dietary recommendations: (1) constructions of healthy and unhealthy eating; (2) considerations on dietary recommendations and healthy eating messages; and (3) meanings attached to food and eating. A list of themes and subthemes with supporting participant quotes can be found in Table S3 in the Electronic Supplementary Material.
Theme 1: Constructions of Healthy and Unhealthy Eating
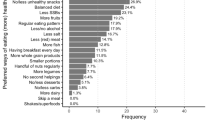
The first theme focuses on the construction of healthy vs. unhealthy eating, specifically considering what nutrients, food, food preparation methods, and food-related behaviors are classified as healthy and unhealthy and specific concepts of healthy eating. Table 2 provides an overview of healthy and unhealthy eating aspects mentioned. To improve readability, citations are omitted from the following two subthemes, but can be found in Table 2.
Construction of Healthy Eating
Healthy eating was viewed as positive and beneficial [38,39,40,41] and as contributing to well-being [38, 39, 42,43,44,45]. Participants discussed the healthiness of food and eating based on nutrients, food groups, food preparation and processing, and food-related behaviors.
Information about which nutrients study participants considered healthy was infrequently provided; however, protein, complex carbohydrates and fiber, healthy fats, and vitamins and minerals were regarded as healthy or essential.
In almost all studies, participants indicated that fruits and vegetables are a vital part of a healthy diet, virtually always mentioning them together. Other food groups, on the other hand, were mentioned less frequently, but wholegrain products, various protein sources, legumes, nuts and seeds, and fish were considered healthy. In some studies, participants expressed uncertainties regarding the healthfulness of certain food groups, which included meats [46, 47], starches [47], and dairy [47]. Apart from one study [47], dairy was neither mentioned as healthy nor unhealthy in any of the included studies. Statements were also made on the healthfulness of various types of meat, with some being considered healthier than others.
Natural foods and foods with a minimal degree of processing as well as home-cooked or homemade meals were considered healthy. Nutrient-saving cooking methods such as steaming and grilling (instead of frying) were also considered healthy.
A variety of food-related behaviors considered healthy were mentioned across included studies. These included eating a variety of (colorful) foods, avoiding or reducing the intake of fat, sugar, and salt, respecting hunger and satiety cues and being mindful of portion size, and eating according to one’s dietary needs.
Construction of Unhealthy Eating
While concepts of healthy eating were frequently described in the included studies, concepts of unhealthy eating were less detailed. In opposition to healthy foods, unhealthy foods were generally seen as negative [40, 41, 43, 48, 49], partly due to their adverse effects on health [48].
Nutrients considered unhealthy were sugar, fat and saturated fat, cholesterol, and salt. While protein was understood to be an important nutrient, overconsumption was considered unhealthy. Various food additives and residues were also mentioned as being unhealthy.
Foods and food groups considered unhealthy included fast foods, junk foods, and a variety of (highly) processed foods, such as confectionery, potato chips, and sugar-sweetened beverages. Additionally, different types of meat, high-fat foods, and, interestingly, “white” foods, such as white vegetables and white pasta, were considered unhealthy.
Similarly, foods that are highly processed, cooked for a long time, fried, or prepared with a lot of fat are considered unhealthy.
Regarding unhealthy eating habits, aspects such as skipping meals, frequent snacking, deviation from what is considered healthy, and overeating were mentioned.
Concepts of Healthy Eating
Balance and moderation were frequently mentioned concepts associated with the regulation of food intake.
Balance was considered a crucial aspect of healthy eating [38, 42,43,44,45, 47, 50, 51]. However, what balance means differed between studies and participants [41,42,43,44, 48, 52, 53]. According to dietary recommendations, “balance” means incorporating all food groups in differing proportions and providing the body with all nutrients required for optimal health [54]. While some studies reported that “balance” was indeed understood as eating meals that included foods from all food groups [38, 42, 43, 50], others believed that “balance” means one could compensate for unhealthy eating with healthy eating or other health behaviors later on [41, 44, 48, 52, 53].
Moderation was named as another relevant concept of healthy eating [39, 43,44,45,46,47, 49, 50]. Generally, foods that were perceived to be less healthy should be eaten “in moderation” [43, 44, 46, 49, 55]. Participants in several studies appeared to use this concept to control their intake of foods they considered unhealthy [41, 43, 44, 49, 50, 55] but also to justify the consumption of these foods [41, 43, 44, 50, 55].
Theme 2: Considerations on Dietary Recommendations and Healthy Eating Messages
The second theme focuses on study participants’ knowledge and awareness of healthy eating messages as well as their diverse attitudes and opinions regarding dietary recommendations.
Knowledge and Awareness of Healthy Eating Messages
Although none of the studies had formally tested participants’ nutritional knowledge, it appears that most study participants had at least a rough idea about what constitutes a healthy diet according to dietary recommendations [38, 40,41,42,43,44,45,46,47, 49,50,51, 53, 55,56,57,58,59], with some demonstrating more comprehensive nutrition knowledge [42, 43, 59]. Participants were aware of dietary guidelines [38, 39, 42, 45, 47, 50, 53, 55,56,57, 59, 60] and identified key messages [38, 39, 45,46,47, 50, 53, 55,56,57, 59, 60], such as eating five servings of fruits and vegetables a day [50, 53, 60] and choosing high-fiber foods [51, 59, 60]. Mentions of specific messages included in dietary recommendations can be found in Table S4 in the Supplementary Material.
Some authors explicitly mentioned gaps in nutrition knowledge in their cohorts. Participants reported inaccurate or superficial nutrition knowledge [40, 46, 47, 51, 53, 57, 58] or were unsure or did not know what foods are healthy besides fruits and vegetables [53, 58]. Particularly low-income [47, 53, 57, 58] and non-tertiary educated [40] participants exhibited a lack of nutrition knowledge, but this was not reported for all low-income participants [48, 55, 56, 61] and not for any of the cohorts or participants with higher socioeconomic status indicators [38,39,40,41,42,43,44, 49, 52, 55, 60], except for a student population [51] and a cohort of men [46]. Indeed, participants with higher formal education were described as having better nutrition knowledge [40, 59].
Participants reported knowing about healthy eating from a variety of sources, including relatives and friends [39, 42, 43, 48, 51, 58, 59], health professionals [55, 58, 59], school health education [43, 58, 59], food labels [43, 60], different media outlets [39, 42, 46, 53, 56, 59, 60], and the Internet [42, 52, 58, 59]. The reliability of information on nutrition from social contacts [42, 43] and various media outlets [42, 46, 58] was questioned as messages can be contradictory. Participants sought out multiple sources and drew from personal experiences to determine what dietary practices most benefitted their individual needs, while also considering cultural food traditions [59].
Attitudes and Opinions Toward Healthy Eating Messages
Participants held diverse views on dietary recommendations, with some expressing a lack of trust, confusion, skepticism, rejection, and resistance to these messages [39, 41, 42, 45, 46, 52, 53, 56, 59, 60, 62].
Participants acknowledged that effort, discipline, and a degree of self-control are required to adhere to dietary recommendations [39, 41, 44, 45, 49, 50, 59, 60] which indicate discrepancies between their requirements, actual dietary behaviors, and barriers in the environment. Furthermore, participants felt that dietary recommendations were unrealistic to achieve [52, 53], and in particular, the recommendation to eat five portions of fruits and vegetables daily, a prominent healthy eating message [12], was viewed as unrealistic [53].
Participants showed a lack of trust, confusion, and skepticism in government-endorsed healthy eating messages [41, 45, 52, 53, 56, 59, 60, 62]. Reasons mentioned were the lack of consideration for Black bodies [56], prioritizing personal preferences over government advice [52, 53], frequent changes in messages [46, 60], contradictory messages [41], the involvement of the meat and dairy industry in their development [59], recommendations being perceived to be based on outdated evidence [62], and putting higher value and trust in one’s physical experiences [41, 45, 59, 62].
It was reported that participants prefer to follow their own rules for healthy eating [41, 45, 56, 60, 62] according to what they perceive to be suitable for their bodies [41, 45, 56, 59, 62] or living circumstances [56, 60]. Healthiness was viewed as individually determined, leading to the conclusion that dietary recommendations are not universally applicable [45, 62], and led some to believe that since every person is different, they should not exist [62]. Scientific evidence should, however, be integrated into personal nutrition [59]. Health advice was also modified to be more applicable and acceptable [52, 53].
Instead of receiving specific instructions on what foods to favor or avoid, study participants preferred to receive specific guidance on which foods are beneficial and affordable and to gain the necessary skills to prepare them [55].
Theme 3: Meanings Attached to Food and Eating
This theme describes the different meanings that are attached to food and eating. A wide range of subthemes were identified, including the significance of healthy eating in daily life, eating as a pleasurable experience, food in stressful situations and as a means to provide comfort, negative feelings around food consumption, moral as well as health and well-being considerations in dietary behaviors, social significance of healthy eating, and lastly, eating as a means to construct cultural identity.
Significance of Healthy Eating in Daily Life
As stated above, most participants had a relatively good understanding of what constitutes a healthy diet [40,41,42,43, 45, 46, 48,49,50,51,52,53, 55,56,57, 59] and of the importance of healthy eating for well-being [40,41,42,43, 45, 46, 48,49,50, 52, 53, 62]. However, healthy eating appeared to be a daily challenge, with other aspects taking priority [41, 42, 48, 49, 51, 52, 59]. For some, healthy eating was of little importance in everyday life [52, 58].
Reviewed studies indicated that healthy eating was not always a priority or possibility [39, 40, 42, 48, 50,51,52,53, 55,56,57,58,59, 61], with other factors deemed more important or prohibitive [39, 40, 42, 48, 51,52,53, 55,56,57,58,59, 61], such as financial [40, 42, 46,47,48, 50,51,52,53, 55, 57, 58, 60, 61] and time constraints [40, 42, 46, 48,49,50,51,52,53, 55, 61], low availability of healthy foods [40, 46, 51, 53, 55,56,57,58, 61], environmental factors [40, 46, 51, 61], sociocultural meanings [41, 43, 48, 55, 56, 59], stressors [42, 51, 60, 61], various commitments [42, 48, 49, 51, 52, 61], taste and personal preferences [39,40,41, 44, 48, 51,52,53, 56, 58, 61], insufficient capacity or volition to eat according to healthy eating rules [42, 48, 49, 52, 55, 58, 62], and difficulty preparing healthy food [46, 48, 49, 51,52,53, 55]. Particularly low-income cohorts [48, 57, 58, 61] and a student population [51] reported insufficient financial resources for food or even food insecurity, likely resulting in poorer food choices due to higher perceived costs for healthy foods [48, 51, 57, 61].
Eating as a Pleasurable Experience
Eating pleasure and enjoyment of food was described as an important factor in food choice [39,40,41, 44, 45, 48, 51, 53, 56, 58]. Different explanations were provided as to why a particular food was viewed as pleasurable [41, 44, 45, 48, 55, 56], including a food’s cultural significance [55, 56], past experiences [41, 48], happy memories related to food [44, 48], the satisfaction they provided [48], and fulfillment of cravings [45]. Food characteristics associated with eating pleasure were taste, aesthetics, and variety [44, 45]. Food context also played a role in eating pleasure [39, 44, 48, 49], such as cooking and eating together [44, 49] or sharing a meal [44].
Some participants described the healthiness of certain foods or dishes as an added value to the pleasure they provided [44, 45]. To some, it was important to include eating pleasure when defining and promoting healthy eating [44].
Participants in other studies described the healthiness of certain foods as a factor reducing eating pleasure [39, 41, 53, 56, 58]. Participants felt that unhealthy foods tasted better than healthy foods [41, 47, 50,51,52,53, 55, 58], such as fried foods [47] and confectionary [41]. Some participants perceived healthy foods as comparatively less tasty [51, 53, 55, 58]. Adhering to healthy eating rules was perceived as a renunciation of eating pleasure [41, 53] and as an “immediate reduction in quality of life” [53].
Food in Stressful Situations and as a Means to Provide Comfort
In various situations, including when participants feel tired, exhausted, stressed, depressed, or experienced low mood, food was used to provide comfort [42, 48, 51, 60, 62]. Comfort-providing foods were consumed to relieve stress [48, 60, 62] or to cope with stressful situations [51, 60, 62] and to regulate mood [51, 62]. Eating was also described as a way to improve mood [62], and food was used as a reward or a treat [41, 44, 45, 50, 51, 53, 61, 62]. Participants found it difficult to adhere to healthy eating rules in stressful or emotional situations [42, 61], resulting in fewer healthy food choices [61].
There was little description of specific types of comfort foods, but some depictions hinted at foods generally understood as unhealthy, and which were also perceived as unhealthy by participants [48, 60, 62], such as chocolate [60, 62] and pizza [48]. The concept of comfort food appeared to be subjective and varied among individuals [44, 48, 62].
Negative Feelings Around Food Consumption
While some participants felt proud when being reminded of their efforts to eat and live healthily [41, 48, 52, 62], others described negative feelings like guilt [40, 41, 52, 62], regret [41], and shame [41, 52, 62] around food consumption. Participants experienced negative feelings due to not adhering to the healthy eating ideal that they have defined for themselves or has been defined by society [41, 52, 62] or when they were not in control [60] or lost control [39, 41, 62] of their food intake, fed children unhealthy food [40], or gained weight as a result of their perceived failings [62]. Not adhering to healthy eating rules was described as “doing something wrong,” thus inducing feelings of guilt [41].
There were also some descriptions of ways to minimize guilt, regret, and shame associated with unhealthy foods [41, 45, 52, 53, 62]. For some, these feelings could be overridden by the pleasure and enjoyment these foods provided [52]. Participants re-interpreted unhealthy foods as a physical necessity when craving these foods, thereby finding a way to justify eating unhealthier foods [45]. Consumption of negatively viewed treats was also limited to occasion and quantity [41]. When unhealthy foods are consumed, this is followed by periods of restraint and moderation, and unhealthy behaviors are balanced with healthy behaviors [41, 53], such as eating a salad after having bacon [53].
Moral Considerations in Dietary Behaviors
In several studies, food and eating situations were referred to as either “good” or “bad” [39,40,41,42, 45, 46, 48, 49, 52, 53, 60], reflecting moral considerations in dietary behaviors. “Good” foods, such as fruits and vegetables [48, 49] and natural foods [49], are considered healthy [39, 40, 48] and should be favored [42, 45]. Conversely, “bad” foods, such as processed foods [49] and those with high fat content [41, 49], were associated with poor health [40, 41, 48, 53] and should be avoided [41, 42, 45, 48]. Consumption of healthy food was viewed positively [39,40,41], while consumption of unhealthy foods [40] or overconsumption [41] was viewed negatively, leading to guilt [41, 52, 53, 60, 62] or a perception of failure [50].
Participants labeled themselves as “good” or “bad” based on their dietary decisions [39, 41, 53, 59, 60], associating being “good” with following well-known dietary guidelines [39] and exercising self-control [39, 49, 50, 59, 60]. People perceived themselves as “bad” when losing control over their eating [39], overly enjoying their food [41], or making “bad” food choices [39, 41, 52, 53], but these could later be balanced out with “good” behaviors [41, 53] or restriction [41].
Participants in several studies reported on implicit norms regarding food consumption [39,40,41, 52, 61]. People felt pressure to eat healthily [51, 52] or felt resented or judged by society if they made the “wrong” dietary choices [41, 52], but in certain social environments, pressure also existed to deviate from the healthy eating ideal [45, 51, 58, 60, 61].
Nonetheless, people justified consuming “bad” foods as physical necessities [45] or justifiable “transgressions from the ideal” [41]. Consumption of “bad” foods considered sinful in a cohort of older Irish adults was also normalized as a part of life [41].
Health and Well-Being Considerations in Dietary Behaviors
Participants recognized the impact of food consumption on health and well-being [40,41,42,43, 45, 46, 48,49,50,51,52,53, 56,57,58,59, 61, 62] and saw a connection between their dietary habits, immediate well-being, and everyday functioning [42, 43, 46, 50, 51, 57,58,59, 62]. Eating healthily provided a foundation to perform daily tasks [42, 50, 51, 56], while consuming unhealthy foods made one feel lethargic and tired [43, 51, 57, 58, 62]. A healthy diet was believed to reduce health problems [50, 51, 56, 57] and that an unhealthy diet was a significant factor in poor health [40, 43, 48, 50, 51, 53, 56]. Participants were also aware of the importance of diet in healthy aging [50, 52] and as a contributing factor in longevity [48, 50, 51, 58].
Participants in several studies expressed a holistic view of health and well-being by linking a combination of health behaviors to well-being [38, 45, 46, 51, 52]. Maintaining a healthy lifestyle was believed to positively affect an individual’s physical and mental well-being [38, 43, 51, 52, 59]. Healthy eating was seen as an integral part of health and well-being [38, 42, 43, 46, 52, 62], while other factors contributing to health status were exercise [38, 41, 46, 50,51,52], sleep [38], and smoking [52]. Consequently, participants described experiencing mental health issues when neglecting some of these health behaviors [42, 43, 62].
Participants felt that diet should be tailored to individual needs [44, 45, 62]. It was believed that each person has different physiological and psychological needs for food and nutrients [44, 45, 59, 62], and what is considered healthy for one person may differ for another [41, 45, 62]. However, it was deemed challenging to determine individual healthy eating rules [62].
Health-related benefits were identified as key incentives for participants to adopt healthy eating habits [42, 46, 50,51,52, 59]. People were motivated to eat healthily in order to feel better and have more energy [42, 46, 51], to maintain health and fitness levels [42, 50, 52], and to prevent or reduce the risk of diseases and/or manage health [46, 59, 61]. Participants noticed physical improvements when engaging in healthy eating, thus further motivating them to eat well [42, 46]. However, in Irish men, it was noted that health is unlikely to be a motivator as participants were optimistic about their future health [41].
Furthermore, participants made the connection that healthy eating helps maintain a healthy body weight [41, 42, 46, 48, 51, 61, 62], and this connection motivated them to eat accordingly [46, 48, 51]. Healthy eating was also equated with weight loss and dieting [61], possibly construing healthy eating as restrictive. Indeed, food restriction for weight loss was understood to negatively impact mental well-being [62].
Social Significance of Healthy Eating
Food and eating play a significant role in social interactions and relationships [39,40,41, 49, 51, 56, 58, 61]. Sharing a meal with family or friends was considered a meaningful way to stay connected and spend quality time together [56], was found to be the ideal food context [49], and an important aspect of eating pleasure [44]. Preparing a meal can also symbolize care and affection, as it requires time and effort [41, 56]. Food consumption was also linked to celebrations and joy [41].
Various social relationships were described to influence one’s eating behaviors [39, 40, 42, 48, 51, 53, 58, 61], and being around others was found to make one eat healthier [40, 49, 51, 52]. Observing others eat healthily led participants to be more mindful of their eating [51], and living with others was believed to influence one’s eating habits positively [49]. However, in some cases, participants described social situations in which eating unhealthy food was expected or encouraged [45, 51, 58, 60, 61].
As indicated by several cohorts, women traditionally hold a significant responsibility for food preparation and provision within the family unit [40, 48, 49, 53, 55, 56, 59,60,61], and female family members or partners were described to have a positive influence on the eating behaviors of the family [40, 49, 51, 61]. However, there were indications that this role may be changing as more men participate in food tasks [40, 49, 60] and is further underlined by the perception that healthy eating is no longer in conflict with masculinity [40]. Nonetheless, women described that they had to negotiate with family members to ensure that their notion of nutritional adequacy was followed and that healthier foods were consumed [53, 55, 58, 61].
Participants reported that childhood food experiences shaped their eating practices and food preferences as adults [41, 48, 50, 55, 60, 61]. In several cohorts, participants believed that eating habits are formed in childhood [48, 51, 55, 61, 62], and parents greatly influence their children’s eating habits [40, 42, 48, 51, 55, 58,59,60,61,62]. Therefore, parents should set a positive example to promote healthy eating habits in their children [40, 42, 51].
Eating as a Means to Construct Cultural Identity
While most included studies lacked discussion on the cultural significance of foods or eating practices, studies involving Black participants [48, 55, 56, 59] revealed distinct perspectives on healthy eating, dietary guidelines, and body image that differed from predominantly White cohorts. Black participants emphasized a “collective identity and cultural pride” [56] associated with their specific eating habits which were also used to demonstrate one’s cultural identity and heritage [59] and were interpreted as a means to resist assimilation [56].
Traditional Black cuisine was often described as Soul food [48, 55, 56, 59] and included flavorful, hot, and spicy foods [55, 56, 59]. Foods are frequently fried and are said to contain high amounts of fat [55, 56, 59]. Some of the traditional Black dishes mentioned in the studies were fried chicken [48, 55, 56], various “throw-away” meats such as ox tails and neck bones [48, 55, 56], salt pork, ham hooks, and cornbread [55]. Participants also identified traditional foods like sweet potatoes, black-eyed peas, and beans as healthy [55].
In contrast, Black participants described White cooking as flavorless and under-seasoned [56]. There was a belief that White people consume higher amounts of salad and vegetables, less fried foods, and opt for smaller portions and lighter meals [56]. Healthy eating was also viewed as the White way of eating [55, 56]. Thus, healthy eating may be perceived as something Black people do not do.
Black participants were aware of the connection between traditional dishes of the African diaspora and poor health outcomes [48, 55, 56, 59]. Foods were often described as unhealthy and fatty, with high amounts of cholesterol [48, 55, 59]. Despite this knowledge, the sociocultural significance of these foods outweighed health concerns [55, 56, 59]. Participants emphasized that their way of eating contributes to well-being by connecting to their culture and heritage [55, 56].
Black participants expressed skepticism toward dietary guidelines, perceiving them to be grounded in research on White individuals and not considering Black culture or bodies [56]. Healthy eating was often associated with White body norms and seen as incompatible with Black identity [55, 56]. However, in one cohort, some of the Black female participants aspired to be thin [48].
Discussion
This systematic review of 24 primary qualitative research studies offers insights into the constructions of a healthy and unhealthy diet, knowledge and views on dietary recommendations, and meanings attached to food and eating by adult populations from high-income countries. To the best of our knowledge, this is the first QES on perceptions of a healthy diet of the general adult population. Collectively, participants of the included studies demonstrated a relatively good understanding of healthy eating by reproducing common components of dietary guidelines [12], but in some cohorts of lower socioeconomic status, gaps in nutrition knowledge could be observed. The content of dietary guidelines was recognized and understood, but participants held diverse opinions, with some rejecting them or mistrusting their messages. Food consumption and the act of eating were attributed with diverse meanings, with some foods being linked to pleasure, stress relief, or feelings of guilt. Participants made a connection between their dietary intake and immediate well-being and understood that their diet affects their long-term health status. In addition, social, cultural, and moral considerations also played a role in dietary behaviors. Overall, this research contributes to the field of behavioral medicine by providing comprehensive insights into individuals' perceptions of healthy eating and the factors that shape their dietary behaviors which can be beneficial for the development of food policies and dietary recommendations and can be further investigated in interventions.
Study participants had a reasonably good comprehension of what defines a healthy diet. Specifically, the regular consumption of fruits and vegetables; the concept of balance; choosing fresh, colorful, and minimally processed over highly processed foods; and avoiding foods of low nutritional quality and with high fat, sugar, and salt contents were named as important components of healthy eating. This finding is in line with guidance universally named in dietary recommendations [12] and what has previously been reported by several authors [10, 28, 63].
Overall, no major differences between groups in adults’ understanding of what constitutes a healthy diet could be identified, but gaps in nutrition knowledge were frequently reported for participants of lower socioeconomic status. It should be noted that this was not reported for all cohorts or participants of low socioeconomic status and cannot be applied to all those of low socioeconomic status. In quantitative research, however, several authors observed a positive relationship between socioeconomic indicators and nutrition knowledge [64,65,66], which in combination with these results highlights a substantial need for more intensive nutrition education interventions targeting low socioeconomic status groups.
Throughout the reviewed studies, there was an underlying notion that although healthy eating is essential for maintaining health and well-being, various factors often take priority or hinder individuals from following healthy eating principles on a day-to-day basis. These factors included time and money restraints, work or family commitments, social influences, sociocultural meanings attached to food, and a lack of motivation, interest, or skills to engage in healthy eating habits. While we did not observe significant differences between cohorts concerning these issues, cohorts with lower income levels, in particular, described having inadequate financial resources for food or even facing food insecurity [48, 51, 57, 58, 61], which might lead to poorer food choices due to higher perceived costs for healthy foods. It has been demonstrated that dietary behaviors are influenced by a variety of determinants, including individual, social, and environmental factors [9], and according to Teuscher et al. [67], individuals have conflicting priorities regarding healthy eating. Factors such as preserving cultural food traditions or ensuring that family members are adequately fed while facing time and money restraints may take precedence over healthy eating, even if it means consuming unhealthy foods [48, 53, 55]. Therefore, it has been emphasized that conflicting priorities, social practices, and daily circumstances need to be considered when promoting health practices [67], and interventions solely focused on individual-level factors like nutrition knowledge may not be effective in an environment that discourages behavior change [9].
Multiple studies were included that consisted of cohorts of predominantly or exclusively Black participants from the USA and Canada. Although it was not discussed in all studies with Black participants [47, 57], in several studies [55, 56, 58, 59] perspectives on healthy eating appeared to differ from those of predominantly White cohorts. It should be noted that most studies with Black participants have been conducted in individuals with low income. Therefore, results may be limited to this specific group. For Black participants, food and eating carried cultural significance, with healthy eating often being described as a White way of eating that is not embraced in Black communities [55, 56, 59]. Comparable observations have been made by one author [68] but were not discussed in other qualitative studies of similar objectives [69, 70]. Specifically, “soul food” can be viewed as a dietary practice that holds great significance for Black individuals, serving as a means of celebrating and affirming their cultural identity [68, 71]. Therefore, resisting dietary guidelines, as described in the reviewed literature [56], may be a form of resistance to cultural dominance or forced assimilation to the dominant culture [56, 72]. In light of the documented health disparities between Black and White individuals in the USA [73], healthy eating interventions should be implemented specifically for this population. It has been suggested that nutrition interventions should address commonly held beliefs regarding health and well-being and resistance to cultural dominance [56]. For interventions to be effective, they should be developed with the involvement of individuals of the target group. They must also be culturally sensitive, tailored to their lifestyles, and should focus on positive aspects of their way of eating, such as emphasizing traditional dishes from the African diaspora that are high in fiber and low in fat [55, 56, 68].
Similarly to findings by Rozin et al. [74, 75], food and eating were associated with ambivalent emotions in most study participants. On the one hand, a food’s taste and its significance in social interactions can bring about pleasure and enjoyment, while on the other hand deviating from the healthy eating ideal can cause worry, concern, and guilt.
Cooking and eating together were frequently regarded as important occasions for socializing, fostering connections, and building relationships. Sharing meals, either as a daily routine or for festivities, was typically associated with positive meanings. According to Contento and Koch [13], the social environment influences food choices and dietary behaviors. In the reviewed literature, it was suggested that being around others can have positive and negative influences on healthy eating behaviors. Indeed, research suggests that the impact of social modeling during shared meals can be beneficial or harmful to diet quality, depending on the type of modeled eating behaviors and the social context in which they occur [44, 76]. Nevertheless, sharing meals with others is linked with favorable dietary outcomes [77], while eating alone was viewed as a barrier to healthy eating [49] and is associated with lower dietary quality [78].
Participants also reported positive feelings, thoughts, and memories regarding food and eating, which led to greater enjoyment of certain foods that appear to go beyond a food's taste. Taste and eating pleasure were also found to be major factors in food choice, aligning with Contento and Koch’s model [13], which emphasizes that an individual’s biologically determined predisposition toward specific foods and past food experiences influence food choices and dietary behaviors. Preferences for certain tastes (e.g., sweet, umami) are biologically determined as a result of evolutionary processes [44, 79, 80]. Therefore, individuals tend to prefer highly palatable foods due to their high fat, sugar, and salt content, which are generally considered unhealthy [44, 81]. In the reviewed literature, participants frequently described healthy foods which are lower in fat, sugar, and salt as less tasty while preferring unhealthy foods, even though they knew of the health effects of a poor diet. This observation is consistent with a study conducted in an US American population [82], while the perception that healthy foods are tastier dominated in a French cohort [83], indicating that sociocultural factors may influence attitudes toward healthy eating. We only observed the perception that unhealthy foods taste better in studies from English-speaking countries; therefore, results may not be transferable to other high-income countries. Indeed, in the sole studies conducted in non-native English-speaking populations [44, 45], the healthfulness of food was described to contribute to eating pleasure, which underlines sociocultural differences in attitudes toward eating pleasure and healthy eating.
Participants frequently described using certain types of food, typically unhealthy ones, as a way to deal with stressful situations because they found comfort in consuming them. In stressful situations individuals were found to consume more palatable high-calorie foods than individuals in stress-free conditions [84,85,86]. Commonly, higher consumption of palatable foods has been attributed to their pleasurable properties which help alleviate the discomfort caused by stressful situations [87]. However, according to Pool et al. [87] stress-related eating is influenced by habits and automatic responses, described as “Pavlovian motivational bursts,” independent of hedonic pleasure or the intention to relieve stress. Therefore, exposure to an environmental stimulus associated with highly palatable food can trigger the compulsive pursuit of such foods, regardless of how enjoyable its consumption is to the individual [87]. The issue of stress-induced overeating needs to be addressed as it may promote rapid weight gain [88]. One way to reduce stress-induced or emotional eating could be to individually develop alternative strategies or habits for coping with emotional situations, as different strategies were shown to be effective [89,90,91]. On a macro level, people in countries with increased rates of overeating and excess weight are consistently exposed to stimuli linked to highly palatable foods, such as advertisements or fast-food restaurants [87]. It has therefore been proposed to regulate the food environment in order to reduce these stimuli [92, 93].
Moral considerations related to dietary behaviors were often reflected in the way study participants talked about food and eating situations, categorizing them as either “good” or “bad” by their perceived healthfulness. Such moral discussions around food often carry religious undertones, with concepts such as restriction being associated with “good” and indulgence being associated with “evil” [41, 52, 94, 95]. Unhealthy eating habits were often depicted as indulgent and enjoyable, while following a healthy diet was viewed as a form of sacrifice, reflecting Christian values like self-control and abstinence [41, 52]. A decline of religion’s significance in Western societies and a growing responsibility individuals face in managing their health amidst an abundance of food and rising rates of obesity have led to a shift toward “healthism” whereby individuals place great importance on health and well-being [41, 96]. Additionally, the scientifically informed discourse around healthy eating which continues to be influenced by traditional and moral codes have been described as the process of “moralization” [97, 98]. Personal food preferences and eating behavior have essentially been turned into moral decisions which was reflected in the discussions of the reviewed literature.
As a result of these moral considerations, consuming food considered unhealthy can lead to feelings of guilt, regret, or shame [41, 52, 94, 95]. Guilt, defined as a self-conscious emotion resulting from a perceived wrongdoing and often accompanied by a desire to take corrective action [99], was caused by deviating from healthy eating ideals or losing control over food intake. The association of unhealthy eating with guilt have been linked to unhealthier eating behaviors and lower levels of perceived behavioral control over eating [100, 101]. Furthermore, guilt did not appear to be a motivator for healthy eating and those who associate unhealthy food with guilt do not have more positive attitudes toward healthy eating [74, 100,101,102].
Based on results of a meta-analysis, it has been suggested that guilt appeal messages may be a possible strategy to promote certain health behaviors [103]. However, our findings and findings from other authors [100, 101] suggest that healthy eating messages should be cautious about inducing feelings of guilt. Instead, they should frame foods high in fat, sugar, and/or salt as occasional treats that can be enjoyed in moderation, rather than banning them altogether, and put emphasis on the pleasure of eating [100]. Indeed, describing a healthy food as both healthy and tasty was found to be a promising and effective strategy as it increased the selection of a healthy food over an unhealthy food item [104].
Growing scientific evidence has suggested the implementation of strategies that prioritize eating pleasure as a way to promote healthy eating behaviors [74, 105,106,107,108]. Further research on the effectiveness of health- vs. pleasure-oriented messages regarding healthy eating has shown that both strategies can be effective [105, 109], while Bedard et al. [108] described that conceptualizing eating pleasure as sensory experiences, mindful eating, memories, social experiences amongst others led to beneficial dietary outcomes. This suggests that strategies that go beyond the traditional health focus of dietary guidelines may be effective in improving dietary behaviors, particular in certain cultural settings.
Dietary guidelines were frequently rejected or mistrusted by participants in the included studies. As these are meant to improve population diet by educating individuals on healthy eating their effectiveness may be in question if they continue to be met by resistance. Here, consumer’s wishes for healthy eating recommendations need to be considered which may increase their credibility [110]. Based on our results, a revised approach may be necessary to improve acceptance, possibly by consistently communicating messages across media outlets and through community gatekeepers, providing strategies to implement recommendations into everyday life, taking frequently experienced barriers into consideration (e.g., financial and time constraints), and being mindful of the sociocultural significance of dietary behaviors. Using community gatekeepers as healthy eating guides can improve healthy eating habits by building trustworthiness in dietary recommendations within the community. However, more research is necessary to determine more effective strategies.
Strengths and Limitations
The QES presented here contributes to the existing literature by offering a comprehensive overview of constructions of healthy eating, attitudes toward dietary guidelines, and the various ways meanings are attached to food and eating by the general adult population of high-income countries. This synthesis can serve as a foundation for further in-depth research on the topic of constructions of healthy eating and the significance of food. The methodical approach to thematic synthesis outlined by Thomas and Harden [4] was followed, and for reporting, the ENTREQ statement as outlined by Tong et al. [5] was adhered to. A wide range of populations in terms of geographic location, socioeconomic background, ethnicity, age, and gender were included. Most studies were published within the last decade, indicating a recent surge of interest in this topic and offering current views on healthy eating. Although the literature search initially did not include a time restriction to investigate whether there had been a change in perception over time, no relevant high-quality studies were found prior to 2007. It was evident that data saturation was reached as the publications identified through a second literature research did not offer additional insights but rather added to data richness.
This review has a few notable limitations. Qualitative reviews commonly rely on the original study author’s pre-selected participant quotes and interpretation which also presents a limitation of this review. However, to ensure this synthesis remains rooted in participant experiences, several supporting original quotes are provided for each theme. This review exclusively included populations from high-income countries which greatly limits transferability of the results to low- and middle-income countries. However, a pre-search yielded a limited number of studies conducted in these countries, therefore only studies from high-income countries were included. Most studies had a larger representation of women than men, which means that the identified themes may be more relevant and significant to women and not necessarily apply to other genders. Although the aim was to incorporate studies from diverse settings, eligible studies could only be identified with English-speaking populations except for one study from Finland [45] and another from Quebec, Canada [44]. Only reports published in English were included which may have limited the number of relevant studies included in the synthesis. Combined, these aspects limit the transferability and generalizability of the findings to other settings and countries, and results should be interpreted and used with caution. Beliefs identified in this review should not be interpreted as a comprehensive representation of how all adult populations in high-income countries perceive health eating. Instead, they should be regarded as a compilation of various attitudes toward healthy eating that can exist, with the most prominent ones highlighted in this review. We also intended to investigate for socioeconomic differences in participants’ views but due to a lack in diversity of low-income populations and a lack of clear specification of socioeconomic status in the included studies and for participants’ quotes, we were unable to do so reliably. Nevertheless, where possible, differences between groups of varying socioeconomic status were noted.
Conclusion
This qualitative evidence synthesis on the perception of healthy eating demonstrates that while individuals are generally able to describe a healthy diet according to dietary recommendations, they attribute diverse meanings toward healthy eating and food in general, likely affecting their dietary behaviors. The results indicate that to enhance the dietary habits of a population, it is important to carefully phrase and consistently communicate dietary recommendations in a way that associates healthy eating with pleasure and immediate well-being, while also taking their daily reality into consideration. However, the current literature on perceptions and meanings of healthy eating remains limited, particularly for underserved populations. Therefore, further in-depth research is needed to gain a better understanding of perceptions and constructions of healthy eating, including specific food-related values held by different populations and their influence on diet-related behaviors. As a first step, this review provides valuable insights for developing consumer-oriented, practicable, and acceptable food policies, behavioral medicine interventions, and dietary recommendations that can effectively improve population health and well-being.
References
Afshin A, Sur PJ, Fay KA, et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2019;393(10184):1958–72.
Willett WC, Stampfer MJ. Current evidence on healthy eating. Annu Rev Public Health. 2013;34(1):77–95.
Micha R, Shulkin ML, Peñalvo JL, et al. Etiologic effects and optimal intakes of foods and nutrients for risk of cardiovascular diseases and diabetes: systematic reviews and meta-analyses from the Nutrition and Chronic Diseases Expert Group (NutriCoDE). PLoS ONE. 2017;12(4):e0175149.
Schwingshackl L, Balduzzi S, Beyerbach J, et al. Evaluating agreement between bodies of evidence from randomised controlled trials and cohort studies in nutrition research: meta-epidemiological study. BMJ. 2021; n1864.
The GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377(1): 13–27.
Benziger CP, Roth GA, Moran AE. The global burden of disease study and the preventable burden of NCD. Glob Heart. 2016;11(4):393–7.
Thow AM, Downs SM, Mayes C, Trevena H, Waqanivalu T, Cawley J. Fiscal policy to improve diets and prevent noncommunicable diseases: from recommendations to action. Bull World Health Organ. 2018;96(3):201–10.
Hyseni L, Atkinson M, Bromley H, et al. The effects of policy actions to improve population dietary patterns and prevent diet-related non-communicable diseases: scoping review. Eur J Clin Nutr. 2017;71(6):694–711.
Zorbas C, Palermo C, Chung A, et al. Factors perceived to influence healthy eating: a systematic review and meta-ethnographic synthesis of the literature. Nutr Rev. 2018;76(12):861–74.
Paquette M-C. Perceptions of healthy eating: state of knowledge and research gaps. Can J Public Health. 2005;96(Suppl 3):S16–21.
Bisogni CA, Jastran M, Seligson M, Thompson A. How people interpret healthy eating: contributions of qualitative research. J Nutr Educ Behav. 2012;44(4):282–301.
Herforth A, Arimond M, Álvarez-Sánchez C, Coates J, Christianson K, Muehlhoff E. A global review of food-based dietary guidelines. Adv Nutr. 2019;10(4):590–605.
Contento IR, Koch PA. Determinants of food choice and dietary change: implications for nutrition education. In: Nutrition Education: Linking Research, Theory, and Practice. 4th ed. Burlington, MA, USA: Jones & Bartlett Learning; 2020. p. 32–64.
Spronk I, Kullen C, Burdon C, O’Connor H. Relationship between nutrition knowledge and dietary intake. Br J Nutr. 2014;111(10):1713–26.
Strachan SM, Brawley LR. Healthy-eater identity and self-efficacy predict healthy eating behavior: a prospective view. J Health Psychol. 2009;14(5):684–95.
Brouwer AM, Mosack KE. Expanding the theory of planned behavior to predict healthy eating behaviors. Nutr Food Sci. 2015;45(1):39–53.
Bogue J, Coleman T, Sorenson D. Determinants of consumers’ dietary behaviour for health-enhancing foods. Br Food J. 2005;107(1):4–16.
Akamatsu R, Maeda Y, Hagihara A, Shirakawa T. Interpretations and attitudes toward healthy eating among Japanese workers. Appetite. 2005;44(1):123–9.
Bucher T, Müller B, Siegrist M. What is healthy food? Objective nutrient profile scores and subjective lay evaluations in comparison. Appetite. 2015;95:408–14.
Lusk JL. Consumer beliefs about healthy foods and diets. PLoS ONE. 2019;14(10): e0223098.
Cheek J, Onslow M, Cream A. Beyond the divide: comparing and contrasting aspects of qualitative and quantitative research approaches. Int J Speech Lang Pathol. 2004;6(3):147–52.
Rooney C, McKinley MC, Appleton KM, et al. How much is ‘5-a-day’? A qualitative investigation into consumer understanding of fruit and vegetable intake guidelines. J Hum Nutr Diet. 2017;30(1):105–13.
McDonald AE, Dawkins-Moultin L, McWhinney SL. Rural parents’ beliefs about healthy eating. Health Educ J. 2018;77(6):705–19.
Krahn VM, Lengyel CO, Hawranik P. Healthy eating perceptions of older adults living in Canadian rural and northern communities. J Nutr Gerontol Geriatr. 2011;30(3):261–73.
Bech-Larsen T, Kazbare L. Perceptions of healthy eating in transitional phases of life: results of four focus groups with adolescents and older adults. Br Food J. 2014;116(4):570–84.
Lea E, Worsley A, Crawford D. Australian adult consumers’ beliefs about plant foods: a qualitative study. Health Educ Behav. 2005;32(6):795–808.
Flemming K, Booth A, Garside R, Tunçalp Ö, Noyes J. Qualitative evidence synthesis for complex interventions and guideline development: clarification of the purpose, designs and relevant methods. BMJ Glob Health. 2019;4: e000882.
van der Heijden A, Te Molder H, Jager G, Mulder BC. Healthy eating beliefs and the meaning of food in populations with a low socioeconomic position: a scoping review. Appetite. 2021;161: 105135.
Gillies C, Super S, Te Molder H, De Graaf K, Wagemakers A. Healthy eating strategies for socioeconomically disadvantaged populations: a meta-ethnography. Int J Qual Stud Health Well-being. 2021;16(1):1942416.
Flemming K, Noyes J. Qualitative evidence synthesis: where are we at? Int J Qual Methods. 2021;20:1–13.
Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):45.
Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol. 2012;12(1):181.
Cooke A, Smith D, Booth A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual Health Res. 2012;22(10):1435–43.
World Bank. “World Bank Country and Lending Groups”. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. Accessed September 2, 2021.
OECD. “Our global outreach: member countries”. https://www.oecd.org/about/members-and-partners/. Accessed September 2, 2021.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–89.
Long HA, French DP, Brooks JM. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res Methods in Med Health Sci. 2020;1(1):31–42.
Banna JC, Gilliland B, Keefe M, Zheng D. Cross-cultural comparison of perspectives on healthy eating among Chinese and American undergraduate students. BMC Public Health. 2016;16(1):1015.
Koteyko N. Balancing the good, the bad and the better: a discursive perspective on probiotics and healthy eating. Health. 2010;14(6):585–602.
Stephens LD, Crawford D, Thornton L, et al. A qualitative study of the drivers of socioeconomic inequalities in men’s eating behaviours. BMC Public Health. 2018;18(1).
Delaney M, McCarthy MB. Saints, sinners and non-believers: the moral space of food. A qualitative exploration of beliefs and perspectives on healthy eating of Irish adults aged 50–70. Appetite. 2014;73:105–13.
Mete R, Shield A, Murray K, Bacon R, Kellett J. What is healthy eating? A qualitative exploration Public Health Nutr. 2019;22(13):2408–18.
Kombanda KT, Margerison C, Booth A, Worsley A. How young adults in Australia classify foods as healthy and unhealthy. Appetite. 2022;175: 106060.
Landry M, Lemieux S, Lapointe A, et al. Is eating pleasure compatible with healthy eating? A qualitative study on Quebecers’ perceptions. Appetite. 2018;125:537–47.
Niva M. All foods affect health: Understandings of functional foods and healthy eating among health-oriented Finns. Appetite. 2007;48(3):384–93.
Caperchione CM, Vandelanotte C, Kolt GS, et al. What a man wants: understanding the challenges and motivations to physical activity participation and healthy eating in middle-aged Australian men. Am J Men’s Health. 2012;6(6):453–61.
Lucan SC, Barg FK, Karasz A, Palmer CS, Long JA. Concepts of healthy diet among urban, low-income. African Americans J Community Health. 2012;37(4):754–62.
Antin TMJ, Hunt G. Food choice as a multidimensional experience. A qualitative study with young African American women. Appetite. 2012;58(3):856–63.
Sellaeg K, Chapman GE. Masculinity and food ideals of men who live alone. Appetite. 2008;51(1):120–8.
Pettigrew S, Pescud M, Donovan RJ. Older people’s diet-related beliefs and behaviours: Intervention implications. Nutr Diet. 2012;69(4):260–4.
Sogari G, Velez-Argumedo C, Gómez M, Mora C. College students and eating habits: a study using an ecological model for healthy behavior. Nutrients. 2018;10(12):1823.
Brennan L, Klassen K, Weng E, et al. A social marketing perspective of young adults’ concepts of eating for health: is it a question of morality? Int J Behav Nutr Phys Act. 2020;17(1):44.
Wood F, Robling M, Prout H, Kinnersley P, Houston H, Butler C. A question of balance: a qualitative study of mothers’ interpretations of dietary recommendations. Ann Fam Med. 2010;8(1):51–7.
Lim S. Eating a balanced diet: a healthy life through a balanced diet in the age of longevity. J Obes Metab Syndr. 2018;27(1):39–45.
Winham DM, Knoblauch ST, Heer MM, Thompson SV, Der Ananian C. African-American views of food choices and use of traditional foods. Am J Health Behav. 2020;44(6):848–63.
Beagan BL, Chapman GE. Meanings of food, eating and health among African Nova Scotians: certain things aren’t meant for Black folk. Ethn Health. 2012;17(5):513–29.
Dong KR, Chen X, Stopka TJ, Must A, Beckwith CG, Tang AM. Food access, dietary intake, and nutrition knowledge of adults on probation. J Nutr Educ Behav. 2022;54(6):510–20.
Fergus L, Roberts R, Holston D. Healthy eating in low-income rural Louisiana parishes: formative research for future social marketing campaigns. Int J Env Res Public Health. 2021;18(9):4745.
Ristovski-Slijepcevic S, Chapman GE, Beagan BL. Engaging with healthy eating discourse(s): ways of knowing about food and health in three ethnocultural groups in Canada. Appetite. 2008;50(1):167–78.
McKenzie JS, Watts D. Food ideals, food rules and the subjective construction of a healthy diet. Food Foodways. 2021;29(1):66–86.
Schoenberg NE, Howell BM, Swanson M, Grosh C, Bardach S. Perspectives on healthy eating among Appalachian residents. J Rural Health. 2013;29(s1):s25–34.
Lee MF, Bradbury JF, Yoxall J, Sargeant S. “It’s about what you’ve assigned to the salad”: focus group discussions on the relationship between food and mood. Int J Env Res Public Health. 2023;20(2):1476.
Cardoso AP, Ferreira V, Leal M, Ferreira M, Campos S, Guiné RPF. Perceptions about healthy eating and emotional factors conditioning eating behaviour: a study involving Portugal, Brazil and Argentina. Foods. 2020;9(9):1236.
Koch F, Hoffmann I, Claupein E. Types of nutrition knowledge, their socio-demographic determinants and their association with food consumption: results of the NEMONIT study. Front Nutr. 2021;8: 630014.
Carbonneau E, Lamarche B, Provencher V, et al. Associations between nutrition knowledge and overall diet quality: the moderating role of sociodemographic characteristics-results from the PREDISE study. Am J Health Promot. 2021;35(1):38–47.
McLeod ER, Campbell KJ, Hesketh KD. Nutrition knowledge: a mediator between socioeconomic position and diet quality in Australian first-time mothers. J Am Diet Assoc. 2011;111(5):696–704.
Teuscher D, Bukman AJ, Van Baak MA, Feskens EJM, Renes RJ, Meershoek A. Challenges of a healthy lifestyle for socially disadvantaged people of Dutch, Moroccan and Turkish origin in the Netherlands: a focus group study. Crit Public Health. 2015;25(5):615–26.
James D. Factors influencing food choices, dietary intake, and nutrition-related attitudes among African Americans: application of a culturally sensitive model. Ethn Health. 2004;9(4):349–67.
Lucan SC, Barg FK, Karasz A, Palmer CS, Long JA. Perceived influences on diet among urban, low-income African Americans. Am J Health Behav. 2012;36(5):700–10.
Baruth M, Sharpe PA, Parra-Medina D, Wilcox S. Perceived barriers to exercise and healthy eating among women from disadvantaged neighborhoods: results from a focus groups assessment. Women Health. 2014;54(4):336–53.
Liburd LC. Food, identity, and African-American women with type 2 diabetes: an anthropological perspective. Diabetes Spectr. 2003;16(3):160–5.
Kumanyika S. Nutrition and chronic disease prevention: priorities for Us minority groups. Nutr Rev. 2006;64(suppl_1):S9-S14.
Mahajan S, Caraballo C, Lu Y, et al. Trends in differences in health status and health care access and affordability by race and ethnicity in the United States, 1999–2018. JAMA. 2021;326(7):637.
Rozin P, Fischler C, Imada S, Sarubin A, Wrzesniewski A. Attitudes to food and the role of food in life in the U.S.A., Japan, Flemish Belgium and France: possible implications for the diet–health debate. Appetite. 1999;33(2):163–80.
Rozin P, Kurzer N, Cohen AB. Free associations to “food:” the effects of gender, generation, and culture. J Res Pers. 2002;36(5):419–41.
Cruwys T, Bevelander KE, Hermans RCJ. Social modeling of eating: a review of when and why social influence affects food intake and choice. Appetite. 2015;86:3–18.
Fulkerson JA, Larson N, Horning M, Neumark-Sztainer D. A review of associations between family or shared meal frequency and dietary and weight status outcomes across the lifespan. J Nutr Educ Behav. 2014;46(1):2–19.
Chae W, Ju YJ, Shin J, Jang S-I, Park E-C. Association between eating behaviour and diet quality: eating alone vs. eating with others. Nutr J. 2018;17(1).
Drewnowski A, Mennella JA, Johnson SL, Bellisle F. Sweetness and food preference. J Nutr. 2012;142(6):1142S-S1148.
Ventua A, Worobey J. Early influences on the development of food preferences. Curr Biol. 2013;23(9):R401–8.
Maclean PS, Blundell JE, Mennella JA, Batterham RL. Biological control of appetite: a daunting complexity. Obesity. 2017;25:S8–16.
Raghunathan R, Naylor RW, Hoyer WD. The unhealthy= tasty intuition and its effects on taste inferences, enjoyment, and choice of food products. J Marketing. 2006;70(4):170–84.
Werle COC, Trendel O, Ardito G. Unhealthy food is not tastier for everybody: the “healthy=tasty” French intuition. Food Qual Prefer. 2013;28(1):116–21.
Tomiyama AJ, Dallman MF, Epel ES. Comfort food is comforting to those most stressed: Evidence of the chronic stress response network in high stress women. Psychoneuroendocrinology. 2011;36(10):1513–9.
Zellner DA, Loaiza S, Gonzalez Z, et al. Food selection changes under stress. Physiol Behav. 2006;87(4):789–93.
Tryon MS, DeCant R, Laugero KD. Having your cake and eating it too: a habit of comfort food may link chronic social stress exposure and acute stress-induced cortisol hyporesponsiveness. Physiol Behav. 2013;114–115:32–7.
Pool E, Delplanque S, Coppin G, Sander D. Is comfort food really comforting? Mechanisms underlying stress-induced eating. Food Res Int. 2015;76:207–15.
Geiker NRW, Astrup A, Hjorth MF, Sjödin A, Pijls L, Markus CR. Does stress influence sleep patterns, food intake, weight gain, abdominal obesity and weight loss interventions and vice versa? Obes Rev. 2018;19(1):81–97.
Unick JL, Dunsiger SI, Leblond T, et al. Randomized trial examining the effect of a 12-wk exercise program on hedonic eating. Med Sci Sports Exerc. 2021;53(8).
O’Connor DB, Armitage CJ, Ferguson E. Randomized test of an implementation intention-based tool to reduce stress-induced eating. Ann Behav Med. 2015;49(3):331–43.
Armitage CJ. Randomized test of a brief psychological intervention to reduce and prevent emotional eating in a community sample. J Public Health (Oxf). 2015;37(3):438–44.
Marteau TM, Hollands GJ, Fletcher PC. Changing human behavior to prevent disease: the importance of targeting automatic processes. Science. 2012;337(6101):1492–5.
Rangel A. Regulation of dietary choice by the decision-making circuitry. Nat Neurosci. 2013;16(12):1717–24.
McPhail D, Chapman GE, Beagan BL. “Too much of that stuff can’t be good”: Canadian teens, morality, and fast food consumption. Soc Sci Med. 2011;73(2):301–7.
McDonald A, Braun V. Right, yet impossible? Constructions of healthy eating. SSM Qual Res Health. 2022;2: 100100.
Crawford R. Health as a meaningful social practice. Health (NY). 2006;10(4):401–20.
Rozin P. The process of moralization. Psychol Sci. 1999;10(3):218–21.
Delaney M, McCarthy M. Food choice and health across the life course: a qualitative study examining food choice in older Irish adults. J Food Prod Market. 2011;17(2–3):114–40.
American Psychological Association. “APA dictionary of psychology: guilt”. https://dictionary.apa.org/guilt. Accessed March 15th, 2023.
Kuijer RG, Boyce JA, Marshall EM. Associating a prototypical forbidden food item with guilt or celebration: relationships with indicators of (un)healthy eating and the moderating role of stress and depressive symptoms. Psychol Health. 2015;30(2):203–17.
Kuijer RG, Boyce JA. Chocolate cake. Guilt or celebration? Associations with healthy eating attitudes, perceived behavioural control, intentions and weight-loss. Appetite. 2014;74:48–54.
Rozin P, Bauer R, Catanese D. Food and life, pleasure and worry, among American college students: gender differences and regional similarities. J Pers Soc Psychol. 2003;85:132–41.
Xu Z, Guo H. A meta-analysis of the effectiveness of guilt on health-related attitudes and intentions. Health Commun. 2018;33(5):519–25.
Forwood SE, Walker AD, Hollands GJ, Marteau TM. Choosing between an apple and a chocolate bar: the impact of health and taste labels. PLoS ONE. 2013;8(10): e77500.
Vaillancourt C, Bédard A, Bélanger-Gravel A, et al. Promoting healthy eating in adults: an evaluation of pleasure-oriented versus health-oriented messages. Curr Dev Nutr. 2019;3(5).
Pettigrew S. Pleasure: an under-utilised ‘P’ in social marketing for healthy eating. Appetite. 2016;104:60–9.
Block LG, Grier SA, Childers TL, et al. From nutrients to nurturance: a conceptual introduction to food well-being. J Public Policy Mark. 2011;30(1):5–13.
Bédard A, Lamarche P-O, Grégoire L-M, et al. Can eating pleasure be a lever for healthy eating? A systematic scoping review of eating pleasure and its links with dietary behaviors and health. PLoS ONE. 2020;15(12): e0244292.
Trudel-Guy C, Bédard A, Corneau L, et al. Impact of pleasure-oriented messages on food choices: is it more effective than traditional health-oriented messages to promote healthy eating? Appetite. 2019;143: 104392.
Brown KA, Hermoso M, Timotijevic L, et al. Consumer involvement in dietary guideline development: opinions from European stakeholders. Public Health Nutr. 2013;16(5):769–76.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
For this type of study, ethical approval is not applicable.
Research Involving Human Participants and/or Animals
This article does not contain any studies with human participants or animals performed by any of the authors.
Consent to Participate
For this type of study, formal consent is not applicable.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Klink, U., Härtling, V. & Schüz, B. Perspectives on Healthy Eating of Adult Populations in High-Income Countries: A Qualitative Evidence Synthesis. Int.J. Behav. Med. (2023). https://doi.org/10.1007/s12529-023-10214-w
Accepted:
Published:
DOI: https://doi.org/10.1007/s12529-023-10214-w