
Abstract
Purpose
Anesthesiologists can use supraglottic airway devices as a rescue technique for failed intubation even in patients with an increased risk of gastric regurgitation. In this randomized study, we aimed to evaluate the effects of cricoid pressure and paratracheal pressure on placement of the i-gel® (Intersurgical Ltd., Wokingham, Berkshire, UK).
Methods
After induction of anesthesia in 76 adult patients, we inserted the i-gel under paratracheal or cricoid pressure, and assessed the success rate of i-gel insertion, resistance during insertion, time required for insertion, accuracy of the insertion location, tidal volumes, and peak inspiratory pressure with or without each maneuver after i-gel insertion.
Results
The overall success rate of insertion was significantly higher under paratracheal pressure than under cricoid pressure (36/38 [95%] vs 27/38 [71%], respectively; difference, 24%; 95% confidence interval [CI], 8 to 40; P = 0.006]. Resistance during insertion was significantly lower under paratracheal pressure than under cricoid pressure (P < 0.001). The time required for insertion was significantly shorter under paratracheal pressure than under cricoid pressure (median [interquartile range], 18 [15–23] sec vs 28 [22–38] sec, respectively; difference in medians, −10; 95% CI, −18 to −4; P < 0.001). Fibreoptic examination of the anatomical alignment of the i-gel in the larynx revealed no significant difference in the accuracy of the insertion location between the two maneuvers (P = 0.31). The differences in tidal volume and peak inspiratory pressure with or without the maneuvers were significantly lower with paratracheal pressure than with cricoid pressure (P = 0.003, respectively).
Conclusions
Insertion of the i-gel supraglottic airway was significantly more successful, easier, and faster while applying paratracheal pressure than cricoid pressure.
Study registration
ClinicalTrials.gov (NCT05377346); first submitted 11 May 2022.
Résumé
Objectif
Les anesthésiologistes peuvent utiliser des dispositifs supraglottiques comme technique de sauvetage en cas d’échec de l’intubation, même chez les personnes présentant un risque accru de régurgitation gastrique. Dans cette étude randomisée, nous avons cherché à évaluer les effets de la pression cricoïdienne et de la pression paratrachéale sur le positionnement du dispositif i-gel® (Intersurgical Ltd., Wokingham, Berkshire, Royaume-Uni).
Méthode
Après l’induction de l’anesthésie chez 76 adultes, nous avons inséré l’i-gel en utilisant une pression paratrachéale ou cricoïdienne, et avons évalué le taux de réussite de l’insertion de l’i-gel, la résistance pendant l’insertion, le temps nécessaire à l’insertion, la précision de l’emplacement d’insertion, les volumes courants ainsi que la pression inspiratoire maximale avec ou sans chacune des manœuvres après l’insertion de l’i-gel.
Résultats
Le taux global de réussite de l’insertion était significativement plus élevé avec une pression paratrachéale qu’avec une pression cricoïdienne (36/38 [95 %] vs 27/38 [71 %], respectivement; différence, 24 %; intervalle de confiance [IC] à 95 %, 7,6 à 39,8; P = 0,006]. La résistance lors de l’insertion était significativement plus faible en utilisant une pression paratrachéale par rapport à une pression cricoïdienne (P < 0,001). Le temps nécessaire à l’insertion était significativement plus court après avoir exercé une pression paratrachéale plutôt que cricoïdienne (médiane [écart interquartile], 18,4 [15,3–23,1] secondes vs 28,4 [22,3 à 37,8] secondes, respectivement; différence dans les médianes, −10,0; IC 95 %, −18,4 à −3,6; P < 0,001). L’examen par fibre optique de l’alignement anatomique de l’i-gel dans le larynx n’a révélé aucune différence significative dans la précision de l’emplacement d’insertion entre les deux manœuvres (P = 0,31). Les différences de volume courant et de pression inspiratoire maximale avec ou sans les manœuvres étaient significativement plus faibles avec la pression paratrachéale qu’avec la pression cricoïdienne (P = 0,003, respectivement).
Conclusion
L’insertion du dispositif supraglottique i-gel a été significativement plus réussie, plus facile et plus rapide lors de l’application d’une pression paratrachéale que d’une pression cricoïdienne.
Enregistrement de l’étude
ClinicalTrials.gov (NCT05377346); soumis pour la première fois le 11 mai 2022.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Supraglottic airway (SGA) devices have become popular in airway management.1 Compared with traditional devices, SGAs provide a less invasive and quicker alternative for securing the airway, especially in patients with difficult airways or in situations when securing an urgent airway is necessary.2,3 Moreover, second-generation SGAs offer improved protection against gastric regurgitation and pulmonary aspiration through a gastric drainage channel, which is positioned at the opening of the esophagus after insertion.4 Therefore, the use of second-generation SGAs such as the i-gel® (Intersurgical Ltd., Wokingham, Berkshire, UK) is recommended as a rescue technique in both difficult airways and routine airway management.3,5,6
Despite the established role of SGAs in difficult airways, their usefulness is questionable in patients with an increased risk of gastric regurgitation. Nevertheless, when tracheal intubation is unsuccessful, SGAs can be inevitably used in them. As a standard technique, application of cricoid pressure has been suggested to prevent gastric regurgitation by compressing and occluding the upper esophagus over the cricoid cartilage during rapid sequence induction of anesthesia. Nevertheless, because the cuff of the SGA occupies the hypopharyngeal space and upper esophagus, cricoid pressure might hinder insertion of the SGA and make ventilation via the SGA difficult.7,8,9
Application of paratracheal pressure is a novel technique proposed as an alternative to cricoid pressure. Paratracheal pressure compresses the esophagus immediately above the clavicle and more effectively prevents gastric insufflation during positive-pressure ventilation than cricoid pressure.10,11 In contrast to cricoid pressure, paratracheal pressure is applied to the lower cervical esophagus; therefore, it might have a limited effect on the hypopharynx and allow more successful insertion of SGAs. A recent study showed the noninferiority of paratracheal pressure compared with cricoid pressure in achieving successful insertion of the LarySeal laryngeal mask airway (LMA) (Flexicare, Inc., Irvine, CA, USA).12 An LMA has a longer cuff and tapered tip, allowing it to protrude more deeply into the upper esophageal sphincter. By contrast, the i-gel, a widely used second-generation SGA with unique characteristics such as a thermoplastic noninflating cuff with a round, blunt tip, does not fully occupy the hypopharyngeal space.13 Therefore, insertion of the i-gel may be much less affected by paratracheal pressure than by cricoid pressure; however, this has not yet been investigated. In the present study, we evaluated the effects of cricoid and paratracheal pressures on the success rate of i-gel insertion, the time required for insertion, accuracy of the insertion location, resistance during insertion, and ventilation after insertion.
Methods
Ethics
The study was approved by the Institutional Review Board of SMG-SNU Boramae Medical Center, Seoul, Republic of Korea (approval no. 10-2022-55; date of approval, 4 July 2022) and registered at ClinicalTrials.gov before patient enrolment (NCT05377346; principal investigator, Jin-Young Hwang; date of registration, 17 May 2022). The study protocol complied with the ethical guidelines of the Declaration of Helsinki. We obtained written informed consent from the study participants. This report conformed to the applicable Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Study design and patient selection
This study involved patients aged > 18 yr who were scheduled for surgery under general anesthesia with a supraglottic airway from September 2022 to April 2023. The exclusion criteria were risk factors for pulmonary aspiration (e.g., achalasia or pregnancy), known or predicted difficult airway, anatomic variation or pathology of the upper airway, requirement for postoperative ventilator care, and surgeries requiring positions other than supine. We recorded the following patient characteristics: age, sex, weight, height, body mass index, American Society of Anesthesiologists Physical Status, and airway characteristics (Mallampati score, thyromental distance, sternomental distance, and neck circumference).
Randomization
We randomly allocated the enrolled patients to one of two groups: those who underwent application of cricoid pressure (cricoid group) and those who underwent application of paratracheal pressure (paratracheal group) during and after i-gel insertion. For randomization, we generated a web-based random sequence with block sizes of 4 and 12 (Research Randomizer, Social Psychology Network, Wesleyan University, Middletown, CT, USA; available from URL: https://randomizer.org; accessed January 2024). We sealed the sequence in an opaque envelope, which was kept by an anesthesiologist who was not involved in the study.
Anesthesia procedure
The patients entered the operating room without premedication. Routine monitoring included electrocardiography, pulse oximetry, and noninvasive blood pressure monitoring. After preoxygenation, anesthesia was induced with lidocaine (30 mg), propofol (1–2 mg·kg−1), fentanyl (1–2 μg·kg−1), and rocuronium (0.6 mg·kg−1). After neuromuscular blockade, we covered the patient’s neck with an opaque drape so that the anesthesiologists who performed the i-gel insertion were blinded to the group allocation. We selected the size of the i-gel according to the manufacturer’s recommendation: size 3 for patients with a body weight of < 50 kg, size 4 for those with a body weight of 50–90 kg, and size 5 for those with a body weight of > 90 kg. In the cricoid group, cricoid pressure was applied with a force of 30 N, equivalent to approximately 3.06 kg (9.8 N = 1 kg), using a three-finger maneuver. While applying cricoid pressure, the patient’s head was maintained in the sniffing position and was supported with the other hand of the clinician performing the maneuver to prevent head flexion (bimanual maneuver).14 In the paratracheal group, paratracheal pressure was applied with a force of 30 N against the vertebral body with a 3–12-MHz linear ultrasound transducer (Vscan with Dual Probe; GE HealthCare, Chicago, IL, USA) while observing the esophageal obstruction, and the clinician performing the maneuver also supported the patient’s neck (Fig. 1). Ultrasound was prepared in both groups for blinding. Two anesthesiologists with experience performing more than 300 i-gel insertions performed the i-gel insertion. After inserting the i-gel, the anesthesiologist attempted positive-pressure ventilation with gentle manual bagging under each maneuver. If an adequate tidal volume could not be achieved, the anesthesiologist repositioned the i-gel, and ventilation was re-evaluated. We defined successful insertion as the presence of a square expiratory carbon dioxide curve on capnography and an adequate tidal volume in the absence of a pharyngeal leakage sound with a peak airway pressure of ≥ 12 cm H2O during gentle manual ventilation.15 We allowed two attempts, and each attempt proceeded for 60 sec. If the i-gel could not be inserted within 60 sec, the anesthesiologist ventilated the patient with a facial mask and attempted i-gel insertion again. If the second attempt was unsuccessful, we recorded the case as a failure and the i-gel was inserted without the allocated maneuver. We defined the time required for insertion as the duration of time from picking up the i-gel to detecting the square waveform on capnography, and it was calculated by adding the time taken for each attempt. In successful cases, the allocated maneuvers were maintained, and we recorded the tidal volume and peak inspiratory pressure while the mechanical ventilation was set in volume-control mode with a tidal volume of 8 mL·kg−1 of ideal body weight, respiratory rate of 12 breaths·min−1, and zero end-expiratory pressure. Subsequently, the tidal volume and peak inspiratory pressure without the allocated maneuver were recorded using the same ventilator settings. The resistance felt by the anesthesiologist while inserting the i-gel was evaluated on a 4-grade scale (1, no resistance; 2, moderate resistance; 3, severe resistance; and 4, impossible to insert the i-gel). Finally, we assessed the accuracy of the insertion location by the anatomical alignment of the i-gel in the larynx using a fibreoptic bronchoscope with an outer diameter of 4.1 mm (Olympus LE-P, Olympus Optical Co., Tokyo, Japan) positioned at the end of the tube section of the i-gel. The accuracy was recorded on a five-grade scale (1, only glottis observed; 2, posterior surface of epiglottis and glottis observed; 3, anterior part or tip of epiglottis and > 50% of glottis observed; 4, down-folded epiglottis and < 50% of glottis observed; and 5, glottis completely obscured by down-folded epiglottis).16

Diagram of cricoid pressure and paratracheal pressure
The primary outcome was the overall success rate of i-gel insertion. The secondary outcomes were the time required for insertion, the accuracy of the insertion location evaluated with a fibreoptic bronchoscope, resistance during insertion, and the tidal volume and peak inspiratory pressure with or without each maneuver after i-gel insertion.
Statistical analysis
All statistical analyses were performed with IBM SPSS Statistics for Windows version 26.0 (IBM Corp., Armonk, NY, USA). We tested continuous variables for normality with graphical methods such as histograms and Q–Q plots, as well as the Kolmogorov–Smirnov test. Values are expressed as mean (standard deviation), median [interquartile range (IQR)], or number (percentage). Point and interval estimates were determined for between-group differences. We tested continuous data with Student’s t test or the Mann–Whitney U test, and categorical data with the Chi square or Fisher’s exact test. In all analyses, P < 0.05 was considered statistically significant.
The sample size calculation was based on a pilot study of 30 patients in our centre. The insertion success rate was 0.93 while applying paratracheal pressure and 0.67 while applying cricoid pressure. With a type I error of 0.05, a power of 0.8, and a dropout rate of 10%, we included 76 patients (38 patients in each group).
Results
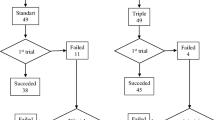
In total, we recruited 81 patients from September 2022 to April 2023. Among the recruited patients, two did not fulfill the inclusion criteria and three declined to participate. The remaining 76 patients were enrolled in the study and included in the analysis (Fig. 2). The patients’ characteristics are presented in Table 1.

CONSORT flow diagram of the study
Data related to the i-gel insertion procedures are presented in Table 2. The overall success rate of insertion was significantly higher in the paratracheal group than in the cricoid group (36/38 [95%] vs 27/38 [71%], respectively; difference, 24%; 95% confidence interval [CI], 8 to 40; P = 0.006). The success rate of insertion on the first attempt was also significantly higher in the paratracheal group than in the cricoid group (36/38 [95%] vs 25/38 [66%], respectively; difference, 29%; 95% CI, 12 to 46; P = 0.002). Repositioning of the i-gel was less frequently required in the paratracheal group than in the cricoid group (14/38 [37%] vs 29/38 [76%], respectively; difference, −39%; 95% CI, −60 to −19; P = 0.001). Resistance during insertion was significantly lower in the paratracheal group than in the cricoid group (P < 0.001). The time required for insertion was significantly shorter in the paratracheal group than in the cricoid group (median [IQR], 18 [15–23] sec vs 28 [22–38] sec, respectively; difference in medians, −10; 95% CI, −18 to −4; P < 0.001). Fibreoptic examination of the anatomical alignment of the i-gel in the larynx revealed no significant difference in the accuracy of the insertion location around the vocal cord between the two groups (P = 0.31). The difference in the tidal volume with or without the maneuvers was significantly lower in the paratracheal group than in the cricoid group (median [IQR], 0 [0–22] mL vs 40 [10–110] mL, respectively; difference in medians, −38; 95% CI, −90 to −8; P = 0.003). The difference in the peak inspiratory pressure with or without the maneuvers was also significantly lower in the paratracheal group than in the cricoid group (median [IQR], 1 [0–2] cm H2O vs 3 [1–7] cm H2O, respectively; difference in medians, −2; 95% CI, −6 to −1; P = 0.003).
Discussion
The present study found that the success rate of i-gel insertion was significantly higher in the paratracheal group than in the cricoid group. Additionally, the insertion time was significantly shorter and easier in the paratracheal group than in the cricoid group. After insertion, the tidal volume and peak inspiratory pressure were less affected by paratracheal pressure than by cricoid pressure. Nevertheless, there was no significant difference in the accuracy of the insertion location between the two groups.
In this study, paratracheal pressure significantly improved both the first-attempt and overall success rates of i-gel insertion compared with cricoid pressure. We did not compare paratracheal pressure to the sham procedure; however, the overall success rate under paratracheal pressure in our study was 36/38 (95%), comparable to the success rate in a multicentre observational study of routine clinical practice (first-attempt and overall success rates of 93% and 96%, respectively).17 In contrast to our results, however, a previous study comparing cricoid and paratracheal pressures for LMA insertion showed no significant difference in the first-attempt and overall success rates between the two maneuvers.12 In that study, the overall success rate of LMA insertion was 76% under paratracheal pressure and 78% under cricoid pressure. Compared with the LMA, the i-gel has a shorter cuff with a round, blunt tip that conforms to the larynx rather than the hypopharynx. A magnetic resonance imaging study of the in vivo position of the i-gel and LMA Supreme™ (Teleflex Inc., Wayne, PA, USA) showed that the tip of the i-gel remained on the upper margin of the upper esophageal sphincter, whereas the LMA Supreme intruded more deeply into the upper esophageal sphincter. These findings indicate that insertion of the i-gel is less affected by paratracheal pressure than insertion of the LMA is.
We also found that the time required to insert the i-gel was significantly shorter under paratracheal pressure than under cricoid pressure. Although the median difference in the insertion time between the two groups was only ten seconds, its clinical significance should not be ignored because our results suggest that insertion of the i-gel can be more rapidly performed in patients with difficult airways during rapid sequence induction.
The i-gel can be used as an intubation conduit, and optimal alignment with the glottic inlet is important for successful tracheal intubation via the i-gel. The i-gel has an epiglottic rest that prevents the epiglottis from down-folding or obstructing the airway. Studies have shown that the i-gel provides an optimal fibreoptic view of the vocal cords (only the vocal cords are visualized) in > 70% of patients.8,18,19 In the present study, however, the glottic view without epiglottic down-folding was observed in eight of 36 (22%) patients in the paratracheal group and five of 27 (19%) patients in the cricoid group. Therefore, when inserted under the application of cricoid or paratracheal pressure, the i-gel may not serve as an effective intubation conduit.
In the present study, cricoid pressure affected the tidal volume and peak inspiratory pressure more strongly than paratracheal pressure. Nevertheless, the accuracy of the i-gel insertion location was similar between the two groups, consistent with a previous study showing that mask ventilation was easier. Peak inspiratory pressure was less affected by paratracheal pressure than by cricoid pressure in anesthetized patients.20 This finding might suggest that airway obstruction is responsible for the deterioration of ventilation during the application of cricoid pressure.
This study had several limitations. First, we did not evaluate laryngopharyngeal damage. Resistance induced by paratracheal pressure or cricoid pressure might lead to laryngopharyngeal damage, thereby causing perioperative complications such as sore throat, hoarseness, and dysphagia. In our study, the resistance felt during insertion was significantly greater during cricoid pressure; therefore, cricoid pressure might result in a higher rate of postoperative laryngopharyngeal complications. Second, this study was conducted in nonobese anesthetized, paralyzed, and fasted patients who were undergoing elective surgery. Therefore, our results may not be generalized to different clinical situations, such as patients with obesity, spontaneously breathing patients, critically ill patients, or nonfasted patients in the emergency setting. Third, as stated above, we did not compare the insertion success rate between paratracheal pressure and a sham procedure. Therefore, further study might be needed comparing the i-gel insertion success rate during paratracheal pressure versus a sham procedure. Fourth, we applied paratracheal pressure with an ultrasound probe because a previous study showed that the esophagus was found on the right side of the lower paratracheal region in 1.4% of patients20 and the actual probability of right-sided esophagus in the paratracheal region has not been accurately investigated. Nevertheless, it might be more reasonable to apply paratracheal pressure with a thumb or index finger instead of the ultrasound probe during an emergency.10 Finally, we did not directly monitor the pressure of 30 N during each maneuver in this study. The investigator who performed each maneuver practiced the application of 30 N based on a previous study showing that 30 N of cricoid pressure is reproducible through proper training.21 Nevertheless, the possibility of errors in the magnitude of a given force cannot be ruled out.
In conclusion, the insertion success rate of the i-gel was higher with the application of paratracheal pressure than with cricoid pressure. Insertion of the i-gel was also significantly easier and faster while applying paratracheal pressure than cricoid pressure. The accuracy of the insertion location was not different between the two maneuvers. When the i-gel is used in patients with an increased risk of gastric regurgitation as a rescue technique for failed intubation, paratracheal pressure can be considered for successful i-gel placement.
References
Woodall NM, Cook TM. National census of airway management techniques used for anaesthesia in the UK: first phase of the Fourth National Audit Project at the Royal College of Anaesthetists. Br J Anaesth 2011; 106: 266–71. https://doi.org/10.1093/bja/aeq339
Apfelbaum JL, Hagberg CA, Connis RT, et al. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology 2022; 136: 31–81. https://doi.org/10.1097/aln.0000000000004002
Frerk C, Mitchell VS, McNarry AF, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth 2015; 115: 827–48. https://doi.org/10.1093/bja/aev371
Cook TM, Kelly FE. Time to abandon the ‘vintage’ laryngeal mask airway and adopt second-generation supraglottic airway devices as first choice. Br J Anaesth 2015; 115: 497–9. https://doi.org/10.1093/bja/aev156
Law JA, Duggan LV, Asselin M, et al. Canadian Airway Focus Group updated consensus-based recommendations for management of the difficult airway: part 1. Difficult airway management encountered in an unconscious patient. Can J Anesth 2021; 68: 1373–1404. https://doi.org/10.1007/s12630-021-02007-0
Law JA, Duggan LV, Asselin M, et al. Canadian Airway Focus Group updated consensus-based recommendations for management of the difficult airway: part 2. Planning and implementing safe management of the patient with an anticipated difficult airway. Can J Anesth 2021; 68: 1405–1436. https://doi.org/10.1007/s12630-021-02008-z
Asai T, Barclay K, Power I, Vaughan RS. Cricoid pressure impedes placement of the laryngeal mask airway and subsequent tracheal intubation through the mask. Br J Anaesth 1994; 72: 47–51. https://doi.org/10.1093/bja/72.1.47
Hashimoto Y, Asai T, Arai T, Okuda Y. Effect of cricoid pressure on placement of the i-gel™: a randomised study. Anaesthesia 2014; 69: 878–82. https://doi.org/10.1111/anae.12731
Aoyama K, Takenaka I, Sata T, Shigematsu A. Cricoid pressure impedes positioning and ventilation through the laryngeal mask airway. Can J Anesth 1996; 43: 1035–40. https://doi.org/10.1007/bf03011906
Gautier N, Danklou J, Brichant JF, et al. The effect of force applied to the left paratracheal oesophagus on air entry into the gastric antrum during positive-pressure ventilation using a facemask. Anaesthesia 2019; 74: 22–8. https://doi.org/10.1111/anae.14442
Kim H, Chang JE, Won D, et al. Effectiveness of cricoid and paratracheal pressures in occluding the upper esophagus through induction of anesthesia and videolaryngoscopy: a randomized, crossover study. Anesth Analg 2022; 135: 1064–72. https://doi.org/10.1213/ane.0000000000006154
Hur M, Lee K, Min SK, Kim JY. Left paratracheal pressure versus cricoid pressure for successful laryngeal mask airway insertion in adult patients: a randomized, non-inferiority trial. Minerva Anestesiol 2021; 87: 1183–90. https://doi.org/10.23736/s0375-9393.21.15779-7
Russo SG, Cremer S, Eich C, et al. Magnetic resonance imaging study of the in vivo position of the extraglottic airway devices i-gel™ and LMA-Supreme™ in anaesthetized human volunteers. Br J Anaesth 2012; 109: 996–1004. https://doi.org/10.1093/bja/aes314
Crowley DS, Giesecke AH. Bimanual cricoid pressure. Anaesthesia 1990; 45: 588–9. https://doi.org/10.1111/j.1365-2044.1990.tb14839.x
Brimacombe J, Keller C, Fullekrug B, et al. A multicenter study comparing the ProSeal and Classic laryngeal mask airway in anesthetized, nonparalyzed patients. Anesthesiology 2002; 96: 289–95. https://doi.org/10.1097/00000542-200202000-00011
Park C, Bahk JH, Ahn WS, Do SH, Lee KH. The laryngeal mask airway in infants and children. Can J Anesth 2001; 48: 413–7. https://doi.org/10.1007/bf03014975
Theiler L, Gutzmann M, Kleine-Brueggeney M, Urwyler N, Kaempfen B, Greif R. i-gel™ supraglottic airway in clinical practice: a prospective observational multicentre study. Br J Anaesth 2012; 109: 990–5. https://doi.org/10.1093/bja/aes309
Joly N, Poulin LP, Tanoubi I, Drolet P, Donati F, St-Pierre P. Randomized prospective trial comparing two supraglottic airway devices: i-gel™ and LMA-Supreme™ in paralyzed patients. Can J Anesth 2014; 61: 794–800. https://doi.org/10.1007/s12630-014-0198-6
Chang JE, Kim H, Lee JM, et al. A prospective, randomized comparison of the LMA-protector™ and i-gel™ in paralyzed, anesthetized patients. BMC Anesthesiol 2019; 19: 118. https://doi.org/10.1186/s12871-019-0785-8
Won D, Kim H, Chang JE, et al. Effect of paratracheal pressure on the glottic view during direct laryngoscopy: a randomized double-blind, noninferiority trial. Anesth Analg 2021; 133: 491–9. https://doi.org/10.1213/ane.0000000000005620
Herman NL, Carter B, Van Decar TK. Cricoid pressure: teaching the recommended level. Anesth Analg 1996; 83: 859–63. https://doi.org/10.1097/00000539-199610000-00036
Author contributions
Dongwook Won and Jin-Young Hwang helped design the study, conduct the study, analyze the data, and write the manuscript. Hyerim Kim, Jee-Eun Chang, Jung-Man Lee, Tae Kyong Kim, and Seong-Won Min helped design the study, conduct the study, and analyze the data. Honghyeon Kim helped conduct the study and analyze the data.
Disclosures
None.
Funding statement
None.
Editorial responsibility
This submission was handled by Dr. Vishal Uppal, Associate Editor, Canadian Journal of Anesthesia/Journal canadien d’anesthésie.
Funding
Open Access funding enabled and organized by Seoul National University.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Won, D., Kim, H., Chang, JE. et al. Comparison of the effects of paratracheal pressure and cricoid pressure on placement of the i-gel® supraglottic airway: a randomized clinical trial. Can J Anesth/J Can Anesth 71, 996–1003 (2024). https://doi.org/10.1007/s12630-024-02741-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-024-02741-1