
Abstract
Background
While prior research has documented intimate partner violence (IPV) and family of origin violence (FOV) experienced by LGBTQ communities at rates at least comparable to heterosexual and/or cisgender populations, little knowledge exists of how this experience occurs within intersections of these communities and who is most at risk.
Methods
This study utilised data from a from a large nationwide Australian survey of the health and wellbeing of 6835 LGBTQ adults aged 18 + years. Multivariable logistic regression analyses were conducted to identify individual factors associated with reporting ever having experienced FOV or IPV.
Results
In total, 2675 (43.18%) participants reported ever experiencing FOV and 3716 (60.7%) reported ever experiencing IPV. Non-binary people, cisgender women, and trans men were most likely to have experienced FOV. Non-binary people and cisgender women were most likely to experience IPV. Participants aged 55 + years (compared to 18–24 years) were less likely to have experienced FOV, while the likelihood of experiencing IPV increased with age. Education was associated with both FOV and IPV (highest among the non-university tertiary educated). Having a moderate or severe disability and ever experiencing homelessness were associated with a greater likelihood of experiencing FOV and IPV. Recent experiences of suicidal ideation, suicide attempt and high/very high psychological distress were associated with experiences of FOV and IPV.
Conclusions
This new knowledge regarding the factors that identify LGBTQ people at greater risk of family or intimate partner violence can ensure the tailoring of family violence practice and policy to those most in need.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Research on the diversity of family violenceFootnote 1 experience among lesbian, gay, bisexual, trans, asexual, or queer (LGBTQ) identifying people is distinctly lacking, both in Australia and abroad, despite growing evidence that experiences of family violence are underreported (Leonard et al., 2008; Workman & Dune, 2019) and widespread among LGBTQ people. Findings from both global and national research suggest the same, if not higher rates of family violence among people who identify as LGBQ compared to non-LGBQ people (Leonard et al., 2008; Victorian Agency for Health Information, 2020; Finneran & Stephenson, 2013; Szalacha et al., (2017), as well as higher rates of family violence among trans and gender diverse people compared to cisgender peers (Calton et al., 2016; Safe Step, 2015; Langenderfer-Magruder et al., 2016). LGBTQ people can face unique forms of family violence that stem from a broader context of stigma around sexual and gender diversity, such as people refusing to acknowledge or threatening to disclose their LGBTQ identity to others or restricting access to social or medical gender affirmation. Moreover, due to entrenched homophobia, biphobia, or transphobia within some communities, coming out to family may lead to experiences of rejection or abuse from family members (Asquith & Fox, 2016; D’augelli et al., 2008; Ryan et al., 2009).
The Royal Commission into Family Violence in Victoria (the second most populous state in Australia), conducted in 2016, recognised the lack of knowledge of LGBTQ experiences of family violence and highlighted the paucity of services available to these communities (State of Victoria, 2016). LGBTQ people face several barriers to accessing support services and may be less likely to report experiences of family violence to authorities or seek help from services (Farrell & Cerise, 2007), in part due to fear of discrimination, homophobia, and transphobia (Kulkin et al., 2007; Bornstein et al., 2006), because they perceive existing family violence services to be for heterosexual, cisgender victim survivors and not available to them (Seymour, 2019), and also due to a lack of services available to support LGBTQ communities (State of Victoria, 2016). Historically, family violence policy and services have often tended to make normative assumptions of the relationship and gender of both perpetrator and survivor, leading to a focus only on violence toward cisgender (i.e., gender identity aligns with that presumed and recorded at birth) women as perpetrated by cisgender men, while overlooking the experiences of LGBTQ people (Seymour, 2019). While there are efforts currently underway to address this situation (Rainbow Health Victoria, 2020), with some emerging promising practice, coverage of LGBTQ-inclusive services is patchy, as is recognition of LGBTQ communities in national and state-level policies and funding frameworks. Findings from a large, national survey of LGBTIQ (lesbian, gay, bisexual, trans, intersex, or queer) people in Australia indicated that among these communities, the perpetrator of intimate partner violence is commonly, though not exclusively, cisgender men (57% of the time) and the survivors of these experiences are not always cisgender women (Hill et al., 2020).
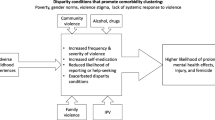
Work on understanding the causes of LGBTQ victimisation can be understood to fall into two approaches: that which focuses on individualistic, psycho-social factors (e.g., minority stress, substance use) and that which focuses on a more sociological approach considering social structural factors (e.g., impacts of institutionalised homo/bi/transphobia, poverty, racism on recognition of family violence and help seeking) (19 for a discussion of these two approaches). Whilst this work is at an early stage there is some evidence that individual characteristics and experiences are, sometimes strongly, associated with higher risk of intimate partner violence (IPV) and family of origin violenceFootnote 2 (FOV). For example, previous research findings suggest that rates of IPV in Australia and internationally may be higher among trans and gender diverse people compared to cisgender sexual minority people (Calton et al., 2016; Safe Steps, 2015; Langenderfer-Magruder et al., 2016). However, this previous research did not disaggregate diverse gender identities, but rather combined trans and gender diverse people into a single sample. Additionally, while LGBTQ people who reside in rural, regional, or remote areas may have greater experiences of social isolation, homophobia, and transphobia (Rosenkrantz et al., 2017), little is known about their experiences of family violence. People from culturally and linguistically diverse (CALD) backgrounds may also be more likely to experience prejudice from family who maintain cultural or religious objections to their LGBT identity, which often leads to feeling unsafe at home (Noto et al., 2014). However, these experiences have yet to be explored in a family violence context. Moreover, findings from research in the general population and a small number of LGBTQ studies, suggest that experiences of family violence may be greater for people with a disability (Jones et al., 2012; McCann et al., 2016; Langenderfer-Magruder et al., 2016), those who have ever experienced homelessness (Langenderfer-Magruder et al., 2016; Giano et al., 2020) and people from a socio-economically disadvantaged background (Kubicek et al., 2016; Steele et al., 2020; Henry et al., 2018). While these studies did not explore family violence experiences among diverse samples of LGBTQ adults, with attention to the intersectional experiences of LGBTQ communities, they provide some insight into factors that may predict experiences of family violence. The limited existing research illustrates a need to explore family violence risk factors among an extensive and diverse sample of LGBTQ people, particularly in an Australian context where experiences of family violence among LGBTQ people are poorly understood.
Furthermore, experiences of FOV and IPV are likely to contribute to poor mental health outcomes for LGBTQ survivors (Szalacha et al., 2017; Ryan et al., 2009; Henry et al., 2018); however, previous literature has yet to explore these associations among a diverse sample of LGBTQ people. Given the already disproportionately poor mental health outcomes within LGBTQ communities compared to the general population (Hill et al., 2020; King et al., 2008), it is important to build new knowledge regarding the intersection of mental health and family violence, particularly with respect to how services within each sector can better understand and respond to co-terminus concerns for this population.
Addressing the considerable lack of knowledge around LGBTQ experiences of IPV and FOV is crucial to informing the targeting and tailoring of victim-survivor support interventions as well as the design of inclusive policy and strategy that seek to prevent such violence occurring. Utilising data from a large national survey of LGBTQ adults in Australia, this paper examines factors that are associated with having ever experienced FOV and IPV, including sexual and gender identity among a range of socio-demographic characteristics, as well as disability, experiences of homelessness, and mental health (suicidality and psychological distress).
Methods
Sample and Procedure
The study sample was drawn from Private Lives 3, a cross-sectional Australia-wide survey examining the health and wellbeing of 6835 LGBTQ Australians aged 18 years or older. PL3 was designed in consultation with an Expert Advisory Group and Gender Advisory Board comprising individuals with expertise in family violence, mental health, and homelessness. Participants were recruited from all states and territories, with the greatest percentage (34.26%) of completions from participants residing in the state of Victoria. The survey was open from July 2019 to October 2019. It was promoted through the networks of LGBTQ community organisations. Targeted paid advertising was also conducted via Facebook and Instagram. Clicking on an advertised or promoted link took potential participants to a landing page that included detailed information about the study and allowed them to indicate their informed consent. Private Lives 3 was granted ethical approval from the La Trobe University Human Research Ethics Committee.
Materials
Demographics
The Private Lives 3 survey comprised items related to demographic characteristics including gender, age, area of residence (inner suburban, outer suburban, regional, and rural or remote), country of birth, level of education, weekly net income, and current engagement in paid employment. Sexual identity was examined by asking participants, ‘Which best describes your sexual orientation?’ Participants were asked to choose from 12 options: ‘gay’, ‘lesbian’, ‘bisexual’, ‘pansexual’, ‘queer’, ‘asexual’, ‘homosexual’, ‘heterosexual’, ‘prefer not to answer’, ‘prefer not to have a label’, ‘don’t know’, and ‘something different.’ For the purposes of analysis, participants who identified as either gay or lesbian were grouped together, and participants who identified as homosexual or preferred not to have a label were grouped into the ‘something different’ category.
Gender identity was examined by asking participants to choose from a list of 17 gender terms that best described them. Gender was then categorised based on responses from participants related to their gender assigned at birth and their response related to the gender identity question. Gender categories included cisgender woman (participants who were assigned female at birth and who chose only ‘female’ as their gender identity), cisgender man (participants who were assigned male at birth and who chose only ‘male’ as their gender identity), trans woman (participants who were assigned male at birth and who chose only ‘female’, ‘trans woman’, or ‘sistergirl’Footnote 3 as their gender identity), trans man (participants who were assigned female at birth and who chose only ‘male’, ‘trans man’ or ‘brotherboy’ as their gender identity), and non-binary (participants who chose only a gender that was not a binary identity or who indicated that they could not choose a single gender identity).
Disability
The Australian Institutes of Health and Welfare’s Standardised Disability Flag Module (SDFM) was used to identify participants with a long-term health condition or disability. Disability or long-term health condition is defined as a condition that limits activity or restricts participation in education and/or employment activities. The SDFM involves eight items regarding difficulties with tasks and need for assistance. Participants are asked to respond on a 4-point scale ranging from ‘have no difficulty’ to ‘always/sometimes need help or supervision’. Responses to the SDFM are categorised into severity of disability including no disability, mild, moderate, or severe disability.
Homelessness
To assess experience of homelessness, participants were asked if they were experiencing or had ever experienced homelessness. Response options included ‘No’, ‘Yes – once and I am not currently experiencing homelessness’, ‘Yes – more than once, and I am not currently experiencing homelessness’, ‘Yes – I am currently experiencing homelessness for the first time’ or ‘Yes – I am currently experiencing homelessness and have also previously experienced homelessness’. For the purposes of the current study, these responses were categorised into a dichotomous variable of whether or not participants had ever experienced homelessness.
Mental Health
To assess experiences of suicidality participants were asked if they had experienced suicidal ideation (‘thoughts about suicide, wanting to die or about ending your life’) and attempted suicide (‘attempted suicide or to end your life’). Response options for these items included ‘No’, ‘Yes, in the past 12 months’, ‘Yes, more than 12 months ago’, and ‘Prefer not to answer’. Multiple responses were permitted. Participants were also given the option to select ‘I prefer not to answer these questions’ without viewing the questions and skip all questions regarding suicidal ideation or suicide attempts. These instances were then coded as missing. The present study focuses on lifetime experiences of suicidality and consequently a variable was computed for each suicidality item to indicate whether participants had ever experienced suicidal ideation or attempted suicide in their lifetime.
Psychological distress was assessed using the ten-item standardised Kessler Psychological Distress Scale (K10) (Kessler at al., 2002). The K10 asks participants to respond to items that cover symptoms of depression or anxiety as experienced over the past 4 weeks, such as ‘Tired out for no good reason’ and ‘Restless or fidgety’. Participants respond to each item using a 5-point scale ranging from ‘None of the time’ to ‘All of the time’. Total scores range from 10 to 50. Scores were then categorised into a dichotomous variable indicating ‘low/moderate’ (scores of 10–21) and ‘high/very high’ (scores of 22–50) psychological distress according to a commonly used classification (Australian Bureau of Statistics, 2017).
Family of Origin Violence
Experiences of FOV were examined by asking participants ‘Have you experienced any of the following from family members? (Choose as many as apply)’. Participants chose from 10 forms of violence, including ‘Physical violence’, ‘Verbal abuse’, ‘Sexual assault’, ‘Financial abuse’, ‘Emotional abuse’, ‘Harassment or stalking’, ‘Property damage’, ‘Social isolation’, ‘Threats of self-harm or suicide’, and ‘LGBTIQ related abuse’. These responses were coded into a dichotomous variable indicating whether or not participants had ever experienced any form of FOV.
Intimate Partner Violence
Similarly, to FOV, experiences of IPV were examined by asking participants ‘Have you experienced any of the following from intimate partner(s)? (Choose as many as apply)?’. Response options included 10 forms of violence as described above for FOV. These responses were then coded into a dichotomous variable indicating whether or not participants had ever experienced any form of IPV.
Statistical Analyses
All analyses were performed using STATA (Version 16.1, StataCorp, College Station, TX, USA). A series of univariable and multivariable logistic regressions with robust standard errors to account for the variance in sample sizes were used to examine factors associated with FOV and IPV. All analyses were conducted separately for FOV and IPV. A range of predictor variables were included in the regression models, including demographic variables, disability, experiences of homelessness, and mental health outcomes (suicidality and psychological distress). Separate univariable regressions were first conducted for each predictor variable to identify significant associations with either FOV or IPV. Two multivariable logistic regression models were then conducted, one to examine correlates of FOV and the other to examine correlates of IPV. All predictor variables were entered into these models to identify significant independent factors. Reference categories for each predictor variables were selected based on sample size, with preference given to larger sample sizes where appropriate, and conceptual framing. For example, cisgender men are one of the larger groups among the gender categories but are also the least likely to report family violence according to the existing literature and were therefore selected as the reference category for this variable. Tests of collinearity resulted in all variance inflation factors (VIFs) < 2, thus indicating no issues in relation to multicollinearity. Results reported from the regression analyses include unadjusted (univariable) odds ratios (OR) and adjusted (multivariable) odds ratios (AORs) along with 95% confidence intervals (CIs). Statistical significance was assessed at p < 0.05.
Results
Frequencies and proportions of sociodemographic characteristics are presented in Table 1. Almost half of the participants identified as gay or lesbian, and more than three-quarters identified as cisgender. The majority were aged under 45 years, born in Australia, and currently engaged in some form of employment. The largest proportion of participants lived in inner-suburban areas. Almost three-quarters of participants had completed tertiary education, and most earned a net income below $2000 per week. In total, 2675 (43.18%) participants reported having ever experienced FOV and 3716 (60.71%) reported having ever experienced IPV.
Correlates of Family of Origin Violence
Table 2 presents factors associated with experiencing FOV. Compared to cisgender men, cisgender women (AOR = 1.44, CI = 1.22–1.71, p < 0.001), trans men (AOR = 1.89, CI = 1.37–2.6, p < 0.001) and non-binary people (AOR = 2, CI = 1.59–2.52, p < 0.001) were up to twice as likely to have experienced FOV. Compared to those aged 18–24 years, participants aged 55 and older were less likely to have experienced FOV (AOR = 0.74, CI = 0.55–1, p = 0.047). Participants with a non-university tertiary education, as compared to secondary school education were more likely to have experienced FOV (AOR = 1.26, CI = 1.04–1.54, p = 0.02), and participants who were currently employed were less likely to have experienced FOV (AOR = 0.75, CI = 0.63–0.89, p = 0.001). Sexual orientation, area of residence, country of birth, and income were not associated with FOV.
Participants who were classified with moderate (AOR = 1.6, CI = 1.36–1.89, p < 0.001) or severe (AOR = 1.54, CI = 1.25–1.89, p < 0.001) disability were more than 1.5 times more likely than those with no disability to have ever experienced FOV. Participants who had ever experienced homelessness were more than 2.5 times more likely to have experienced FOV (AOR = 2.56, CI = 2.19–3.01, p < 0.001).
Associations were found between mental health and FOV. Participants were more likely to have experienced FOV if they had ever experienced suicidal ideation (AOR = 1.74, CI = 1.43–2.11, p < 0.001) or a suicide attempt (AOR = 1.59, CI = 1.37–1.85, p < 0.001) in their lifetime. Additionally, participants who reported high/very high psychological distress in the past 4 weeks (AOR = 1.41, CI = 1.21–1.64, p < 0.001) were also more likely to have experienced FOV.
Correlates of Intimate Partner Violence
Table 3 presents factors associated with experiencing IPV. Compared to gay or lesbian-identified participants, those who identified as asexual were half as likely to have experienced IPV (AOR = 0.51, CI = 0.34–0.75, p = 0.001). Compared to cisgender men, cisgender women (AOR = 1.42, CI = 1.2–1.68, p < 0.001) and non-binary people (AOR = 1.77, CI = 1.38–2.27, p = 0) were up to twice as likely to have experienced IPV. Compared to those aged 18–24 years, the likelihood of experiencing IPV increased with age (25–34 years: AOR = 1.84, CI = 1.5–2.26, p < 0.001; 35–44 years: AOR = 2.05, CI = 1.59–2.64, p < 0.001; 45–54 years: AOR = 2.43, CI = 1.84–3.2, p < 0.001; 55 + years: AOR = 2.62, CI = 1.97–3.47, p < 0.001). Participants with a non-university tertiary education, as compared to secondary school education were more likely to have experienced IPV (AOR = 1.43, CI = 1.16–1.76, p = 0.001). Compared to an income of $0–$399, the likelihood of experiencing IPV was greater with higher incomes ($400–$999: AOR = 1.25, CI = 1.02–1.52, p = 0.029; $1000–$ 1999: AOR = 1.46, CI = 1.15–1.86, p = 0.002; $ 2000 + : AOR = 1.57, CI = 1.16–2.12, p = 0.003). Area of residence, birth country, and current employment status were not found to be significantly associated with IPV.
Participants who were classified with severe disability (AOR = 1.28, CI = 1.01–1.62, p = 0.037) were more likely than those with no disability to have ever experienced IPV. Although not quite significant, there was a trend toward participants with moderate disability being more likely than those with no disability to have ever experienced IPV (AOR = 1.19, CI = 1–1.43, p = 0.053). Participants who had ever experienced homelessness were almost 3 times more likely to have experienced IPV (AOR = 2.59, CI = 2.15–3.14, p < 0.001).
Associations were found between mental health variables and IPV. Participants were more likely to have experienced IPV if they had ever experienced suicidal ideation (AOR = 1.55, CI = 1.29–1.85, p < 0.001) or attempted suicide (AOR = 1.8, CI = 1.52–2.13, p < 0.001) in their lifetime. Additionally, those who had experienced high/very high psychological distress in the past 4 weeks (AOR = 1.69, CI = 1.44–1.98, p < 0.001) were also more likely to have experienced IPV.
Discussion
The present study aimed to expand on the limited knowledge of LGBTQ experiences of IPV and FOV in Australia by exploring a range of sociodemographic and wellbeing factors associated with having ever experienced FOV and IPV among a large sample of LGBTQ adults in Australia. More than a third of our sample (39.1%) reported having ever experienced FOV (34.5% of cisgender, 53.5% of trans or gender diverse), and 60.9% ever experiencing IPV (58.7% cisgender, 68.2% trans or gender diverse). It is difficult to directly compare the rates from the present study to that of the general population in Australia. Firstly, family violence data in the general population are derived from a random, stratified sample whereas our sample is from a self-selecting, community survey. Nonetheless, the prevalence rates are high and of concern. Second, the measure used by the present study to identify family violence involved a comprehensive list of different forms of violence as response items, beyond just physical, sexual, or emotional violence and included LGBTQ-specific violence. While utilising a less nuanced question, general population data from Australia suggest that approximately 17% of (assumed cisgender) women and 6% of (assumed cisgender) men have experienced sexual and physical violence from a partner, and 23% of women and 16% of men have experienced emotional abuse from a partner (AIHW, 2019).
While already high compared to the general population, the experience of both FOV and IPV was observed differently among sections of the LGBTQ population. Cisgender women, trans men, and non-binary participants were the most likely to report experiencing both FOV and IPV. Trans men and non-binary people in the present study were found to be the most likely to experience FOV, followed by cisgender women. Previous studies suggests that LGB people are more likely than heterosexual siblings to have experienced childhood verbal, physical, and sexual abuse (McKay et al., 2019) and may face experiences of rejection, abuse, and violence from families of origin when coming out as sexual or gender diverse (Asquith & Fox 2016; D’augelli et al., 2008; Ryan et al., 2009). These experiences of LGBTQ-specific rejection and related abuse are frequently not recognised as a form of family violence and may therefore go underreported within these populations.
While there is limited research exploring the association of diverse gender identities and experiences of IPV, some previous findings suggest that trans and gender diverse people report higher rates of IPV compared to cisgender LGBQ (lesbian, gay, bisexual, or queer) people (Calton et al., 2016; Safe Steps, 2015; Langenderfer-Magruder et al., 2016). Similarly, the present study found non-binary people were most likely to experience IPV, followed by cisgender women. However, trans men and women were not found to be any more likely to experience IPV than cisgender men. The apparent difference of this finding to that of previous research likely exists in the breakdown of gender in the present study, which compared a number of cis- and trans gender identities, whereas previous research in this space has compared all trans identified people to all cis identified people (Langenderfer-Magruder et al., 2016). The challenges and limitations of collapsing gender categories in this manner have been highlighted previously (Donovan & Barnes, 2020) but still appears commonplace where sample sizes are deemed insufficient to illustrate nuance.
The present study findings suggest a cohort effect on the association between age and FOV, with those aged 55 years or older less likely than younger people to have experienced FOV. This finding may reflect a change in the average age of coming out across age cohorts, with those older than 55 more likely to have come out to family at an older adult age (Dunlap, 2016). This cohort may therefore have already been living out of home and less likely than younger cohorts to be subject to abuse or violence from family members within the home. On the other hand, experiences of intimate partner violence increased with age. Given that this paper reports on ever experiencing violence, increasing age is likely to have led to a greater number of intimate relationships and therefore greater overall exposure to the possibility of IPV. Additionally, older participants may have had a longer period of time since the abusive relationship, providing the opportunity to heal and space to recognise their experience as IPV, as well as greater opportunity to access professionals who might have assisted in supporting them to recognise IPV. Research from England and Wales indicates that IPV (termed ‘partner abuse’ in this context) is most commonly experienced among those aged 16–24 (Elkin, 2021), although there is a pressing need for qualitative research to explore why this may be the case and how this may align with experiences among younger LGBT people.
No association was found between country of birth and experiences of FOV nor IPV in our study. This stands in contrast to previous research, which has found that LGBTQ people within culturally and linguistically diverse communities may be more likely to experience culturally or religiously fuelled abuse or rejection by family members (Asquith et al., 2019; Potoczniak et al., 2009). The lack of similar findings within the present study is perhaps owing to the survey having only been available in English as well as being limited by broad categories of country of birth (Australia, other English-speaking country, other non-English speaking country). It is imperative for future research to explore these experiences among LGBTQ people from culturally diverse backgrounds, including more specific information about participants’ cultural or religious backgrounds.
Socio-economic circumstances were associated with reporting experiences of both FOV and IPV. Previous research has found both within the non-LGBTQ population (Abramsky et al., 2011) and among sexual minority people (Steele et al., 2020; Edwards et al., 2015; West, 2012) that more advantaged socioeconomic circumstances are associated with a lower risk of experiencing IPV. In the present study, those with a non-university tertiary education were most likely to experience both FOV and IPV, and participants who were currently employed were less likely to experience FOV. However, employment status was not associated with IPV, nor was income associated with FOV. Moreover, while an association did exist between income and IPV, the direction of this association was perhaps unexpected, with participants on higher incomes more likely to report having ever experienced IPV. Given that this study explored lifetime experiences of IPV, rather than current experiences, this unexpected finding may reflect a greater ability to recognise and name previous experiences of IPV. People with a higher income are more likely to have better access to health care, which may have resulted in greater access to professionals who might have assisted in identifying or supporting them to recognise experiences of IPV.
In accordance with previous research among the general population (AIHW, 2019) and LGBTQ communities (McCann et al., 2016), participants of the present study with a moderate or severe disability were at the greatest risk of experiencing both FOV and IPV. While little is known about the drivers of violence in this context, these findings further highlight the risk to LGBTQ people with a disability and the need for health providers to run risk assessments for both FOV and IPV in addition to the provision of specific services to support them. Homelessness also had a strong association with both FOV and IPV. These findings reflect those of previous studies (Langenderfer-Magruder et al., 2016; Giano et al., 2020), where it is possible in some instances that leaving a violent relationship or home results in homelessness. For example, previous research suggests that experiences of rejection from family members among young LGBTQ people are associated with higher rates of homelessness, with participants reporting verbal and physical abuse, and attempts from family members to ‘normalise’ their gender or sexuality (Robinson, 2018). These findings suggest a need for integrated services that can recognise and appropriately address the needs of LGBTQ individuals who may be experiencing both homelessness and family violence.
Findings from the present study suggest that LGBTQ people who have ever experienced suicidal ideation or ever attempted suicide in their lifetime are more likely to have experienced FOV and IPV. Additionally, participants who expressed high/very high psychological distress were also more likely to have experienced both FOV and IPV. These findings may indicate the vulnerability of people with poorer mental health to experiences of family violence or, more likely, imply the impact of experiences of family violence on mental health as has been illustrated in previous literature (Szalacha et al., 2017; Ryan et al., 2009; Henry et al., 2018). Importantly, these findings suggest an additional marker that may be used to identify those who may need support/services related to experiences of family violence.
The associations with IPV and FOV outlined in this article reflect a range of individualistic factors (e.g. mental health and suicidal ideation) as well as social ones (e.g. homelessness, unemployment). The extent, or manner, to which they operate as precursors, triggers or impacts is underexamined among LGBTQ communities and should be the subject of future qualitative research or considered within cohort studies that can overcome the cross-sectional limitations of this research design. In considering the range of factors and forces that shape the experience of FOV and IPV for LGBTQ people, it is crucial to consider the wider social context in which this population is othered socially, economically, politically, and culturally (Parker et al., 2018) and how these may inform both experience and response. Both historic and contemporary political and media discourses have advanced a perception that young LGBTQ people are ‘damaged’ in some way (Eckhert 2016; Suess, 2020), which may impact on the likelihood of LGBTQ victim survivors recognising their experience as one involving violence and seeking help, which may contribute to them staying in abusive relationships longer.
Limitations and Strengths
The present study utilised data from the largest nationwide survey of LGBTQ adults in Australia to date. This survey data can be used to paint a detailed picture of experiences of family violence within these communities. However, the family violence data included assessments of ever experiencing FOV and IPV in the participants’ lifetime and did not collect details of recent or current experiences of violence. While this provides evidence of who may be at greater risk of ever having experienced violence, studies are needed to examine correlates of recent or current experiences and to thus provide information to help identify individuals who may be at more immediate risk. Additionally, our measures of FOV and IPV differ from previous studies by providing participants with a comprehensive list of different forms of violence as response items. These were designed to utilise more inclusive definitions of FOV and IPV that are relevant to LGBTQ experiences but may have made our data less comparable to previous findings. That said, this more nuanced approach may have helped to address concerns regarding the commonly cis-heteronormative dominant narrative on family violence leading to underreporting by people within the LGBTQ community, as have been expressed by others (Workman & Dune, 2019; Donovan & Barnes, 2020). It is important to note that our data do not allow us to discern whether the experience of violence was one-off or reflects a pattern of behaviour, which might impact on recognition and help-seeking.
Conclusion
Findings from the present study add considerably to the limited existing knowledge of LGBTQ people’s experiences of family violence. Little research has attended to diversity and intersectionality in the context of LGBTQ communities and thus knowledge relating to groups that are most likely to be at risk of ever having experienced FOV or IPV has been limited. The outcomes of the present study provide details of sociodemographic, disability, homelessness, and mental health factors that are associated with experiences of FOV and IPV. These findings highlight those most at risk in the LGBTQ community and can be used to guide policy and practice in order to better recognise those who may require services or support, as well as tailor family violence intervention efforts to increase service access and to better suit the needs of the LGBTQ community.
Data Availability
Requests for analysis of data from Private Lives 3 can be made to the last author, subject to conditions of use.
Notes
Among policy and practice stakeholders, within the Australian context, the term ‘family violence’ is the preferred term reflecting the circumstances within which violence can occur and recognition that it can involve more than one perpetrator and victim survivor (including children); it is the term used to include both violence from a family of origin (FOV) and from an intimate partner (IPV)
The term ‘family of origin’ draws a distinction between families of birth or childhood as compared to ‘families of choice’, including friends and partners. It is a term utilised by some within the LGBTQ communities and may reflect experiences of rejection from families of origin (19,20)
The terms ‘sistergirl’ and ‘brotherboy’ are used by some Aboriginal and Torres Strait Islander communities to describe trans and gender diverse identities
References
Abramsky, T., Watts, C. H., Garcia-Moreno, C., Devries, K., Kiss, L., Ellsberg, M., et al. (2011). What factors are associated with recent intimate partner violence? findings from the WHO multi-country study on women’s health and domestic violence. BMC Public Health, 11(1), 109.
AIHW. Family, domestic and sexual violence in Australia: Continuing the national story [Internet]. Australia: Australian Institute of Health and Welfare; 2019 [cited 2021 Aug 18]. Available from: https://www.aihw.gov.au/reports-data/behaviours-risk-factors/domestic-violence/overview
Asquith, N. L., & Fox, C. A. (2016). No place like home: Intrafamilial hate crime against gay men and lesbians. In A. Dwyer, M. Ball, & T. Crofts (Eds.), Queering Criminology (pp. 163–182). Palgrave Macmillan UK.
Asquith, N. L., Collison, A., Lewis, L., Noonan, K., Layard, E., Kaur, G., et al. (2019). Home is where our story begins: CALD LGBTIQ+ people’s relationships to family. Curr Issues Crim Justice., 31(3), 311–332.
Australian Bureau of Statistics. Kessler Psychological Distress Scale-10 (K10) [Internet]. 2017 [cited 2021 Jun 4]. Available from: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/4363.0~2014-15~Main%20Features~Kessler%20Psychological%20Distress%20Scale-10%20(K10)~35
Bornstein, D. R., Fawcett, J., Sullivan, M., Senturia, K. D., & Shiu-Thornton, S. (2006). Understanding the experiences of lesbian, bisexual and trans survivors of domestic violence. Journal of Homosexuality, 51(1), 159–181.
Calton, J. M., Cattaneo, L. B., & Gebhard, K. T. (2016). Barriers to help seeking for lesbian, gay, bisexual, transgender, and queer survivors of intimate partner violence. Trauma, Violence & Abuse, 17(5), 585–600.
D’augelli, A. R., Grossman, A. H., & Starks, M. T. (2008). Families of gay, lesbian, and bisexual youth: What do parents and siblings know and how do they react? Journal of GLBT Family Studies, 4(1), 95–115.
Donovan C., & Barnes R. (2020) Queering narratives of domestic violence and abuse. London: Palgrave Pivot Cham.
Dunlap, A. (2016). Changes in coming out milestones across five age cohorts. Journal of Gay and Lesbian Social Services, 28(1), 20–38.
Eckhert, E. (2016). A Case for the demedicalization of queer bodies. The Yale Journal of Biology and Medicine, 89(2), 239–246.
Edwards, K. M., Sylaska, K. M., & Neal, A. M. (2015). Intimate partner violence among sexual minority populations: A critical review of the literature and agenda for future research. Psychology of Violence, 5, 112–121.
Elkin M. (2021) Domestic abuse prevalence and trends, England and Wales: Year ending March 2021. England: Office for National Statistics.
Farrell J., & Cerise, S. (2007). Fair’s fair: A snapshot of violence and abuse in Sydney LGBT relationships 2006 [Internet]. Same Sex Domestic Violence Interagency. Aug [cited 2021 Aug 18]. Available from: https://apo.org.au/node/4676
Finneran, C., & Stephenson, R. (2013). Intimate partner violence among men who have sex with men: A systematic review. Trauma, Violence & Abuse, 14(2), 168–185.
Giano, Z., Williams, A., Hankey, C., Merrill, R., Lisnic, R., & Herring, A. (2020). Forty years of research on predictors of homelessness. Community Mental Health Journal, 56(4), 692–709.
Henry, R. S., Perrin, P. B., Coston, B. M., & Calton, J. M. (2018). Intimate partner violence and mental health among transgender/gender nonconforming adults. Journal of Interpersonal Violence, 21, 0886260518775148.
Hill, A. O., Bourne, A., Mcnair, R., Carman M., & Lyons, A. (2020). Private lives 3: The health and wellbeing of LGBTIQ people in Australia. Melbourne, Australia: Australian Research Centre in Sex, Health and Society, La Trobe University. (ARCSHS Monograph Series No. 122).
Jones, L., Bellis, M. A., Wood, S., Hughes, K., McCoy, E., Eckley, L., et al. (2012). Prevalence and risk of violence against children with disabilities: A systematic review and meta-analysis of observational studies. Lancet, 380(9845), 899–907.
Kessler, R. C., Andrews, G., Colpe, L. J., Hiripi, E., Mroczek, D. K., Normand, S. L. T., et al. (2002). Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine, 32(6), 959–976.
King, M., Semlyen, J., Tai, S. S., Killaspy, H., Osborn, D., Popelyuk, D., et al. (2008). A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry, 8(1), 70.
Kulkin, H. S., Williams, J., Borne, H. F., de la Bretonne, D., & Laurendine, J. (2007). A review of research on violence in same-gender couples: A resource for clinicians. Journal of Homosexuality, 53(4), 71–87.
Kubicek, K., McNeeley, M., & Collins, S. (2016). Young men who have sex with men’s experiences with intimate partner violence. Journal of Adolescent Research, 31(2), 143–175.
Langenderfer-Magruder, L., Whitfield, D. L., Walls, N. E., Kattari, S. K., & Ramos, D. (2016). Experiences of intimate partner violence and subsequent police reporting among lesbian, gay, bisexual, transgender, and queer adults in Colorado: Comparing rates of cisgender and transgender victimization. Journal of Interpersonal Violence, 31(5), 855–871.
Leonard, W., Pitts, M., Mitchell, A., & Patel, S. (2008). Coming forward: The underreporting of heterosexist violence and same sex partner abuse in Victoria. La Trobe University. Australian Research Centre in Sex.
McCann, E., Lee, R., & Brown, M. (2016). The experiences and support needs of people with intellectual disabilities who identify as LGBT: A review of the literature. Research in Developmental Disabilities, 57, 39–53.
McKay, T., Lindquist, C. H., & Misra, S. (2019). Understanding (and acting on) 20 years of research on violence and LGBTQ+ communities. Trauma, Violence & Abuse, 20(5), 665–678.
Noto, O., Leonard, W., & Mitchell, A. (2014). Nothing for them: Understanding the support needs of lesbian, gay, bisexual and transgender (LGBT) young people from refugee and newly arrived backgrounds. Melbourne: La Trobe University, Australian Research Centre in Sex, Health and Society.
Parker, C. M., Hirsch, J. S., Philbin, M. M., & Parker, R. G. (2018). The urgent need for research and interventions to address family-based stigma and discrimination against lesbian, gay, bisexual, transgender, and queer youth. Journal of Adolescent Health, 63(4), 383–393.
Potoczniak, D., Crosbie-Burnett, M., & Saltzburg, N. (2009). Experiences regarding coming out to parents among African American, Hispanic, and white gay, lesbian, bisexual, transgender, and questioning adolescents. Journal of Gay and Lesbian Social Services, 21(2–3), 189–205.
Rainbow Health Victoria ARC in S Health and Society, Latrobe University. (2020). Pride in prevention: A guide to primary prevention of family violence experienced by LGBTIQ communities. [Internet]. [cited 2021 Jul 19]. Available from: https://nla.gov.au/nla.obj-2817963719
Robinson, B. A. (2018). Conditional families and lesbian, gay, bisexual, transgender, and queer youth homelessness: Gender, sexuality, family instability, and rejection. Journal of Marriage and Family, 80(2), 383–396.
Rosenkrantz, D. E., Black, W. W., Abreu, R. L., Aleshire, M. E., & Fallin-Bennett, K. (2017). Health and health care of rural sexual and gender minorities: A systematic review. Stigma Health., 2(3), 229–243.
Ryan, C., Huebner, D., Diaz, R. M., & Sanchez, J. (2009). Family rejection as a predictor of negative health outcomes in white and latino lesbian, gay, and bisexual young adults. Pediatrics, 123(1), 346–352.
Safe Steps. Safe Steps Submission to the Royal Commission into Family Violence [Internet]. Melbourne, Australia: Safe steps family violence response centre; 2015 [cited 2021 Jul 13]. Available from: https://www.safesteps.org.au/wp-content/uploads/2017/10/safe-steps-Royal-Commission-submission-Final.pdf
Seymour, K. (2019). (In)Visibility and recognition: Australian policy responses to ‘domestic violence.’ Sexualities, 22(5–6), 751–766.
State of Victoria. (2016). Royal commission into family violence: Summary and recommendations. Melbourne: State of Victoria. Report No.: 132 (2014–2016).
Steele, S. M., Everett, B. G., & Hughes, T. L. (2020). Influence of perceived femininity, masculinity, race/ethnicity, and socioeconomic status on intimate partner violence among sexual-minority women. Journal of Interpersonal Violence, 35(1–2), 453–475.
Suess, S. A. (2020). Trans health care from a depathologization and human rights perspective. Public Health Reviews, 41(1), 3.
Szalacha, L. A., Hughes, T. L., McNair, R., & Loxton, D. (2017). Mental health, sexual identity, and interpersonal violence: Findings from the Australian longitudinal Women’s health study. BMC Women’s Health, 17(1), 94.
Victorian Agency for Health Information. (2020). The health and wellbeing of the lesbian, gay, bisexual, transgender, intersex and queer population in Victoria: Findings from the Victorian Population Health Survey 2017. Melbourne: Victoria State Government, Victorian Agency for Health Information.
West, C. M. (2012). Partner Abuse in Ethnic Minority and Gay, Lesbian, Bisexual, and Transgender Populations. Partner Abuse, 3(3), 336–357.
Workman, A., & Dune, T. (2019). A systematic review on LGBTIQ intimate partner violence from a Western perspective. Journal Community Safety and Well-Being, 4(2), 22–31.
Acknowledgements
We wish to thank members of the Private Lives 3 ExpertAdvisory Group and Gender Advisory Board, who supportedthis research and gave valuable support, advice,and feedback at various stages of this study, as well asthe many other individuals and organizations who gaveassistance at different stages.
Funding
Private Lives 3 was funded by the Victorian Government Department ofHealth and Human Services and the VictorianGovernment Department of Premierand Cabinet. Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Amos, N., Hill, A., Donovan, C. et al. Family Violence Within LGBTQ Communities in Australia: Intersectional Experiences and Associations with Mental Health Outcomes. Sex Res Soc Policy 20, 1316–1327 (2023). https://doi.org/10.1007/s13178-023-00822-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13178-023-00822-2