
Abstract
Venous thromboembolism (VTE) is common in patients with cancer and is a leading cause of death. In addition to the hypercoagulable state associated with malignancy, cancer-related surgery and subsequent immobilization further increase the risk of VTE. Guidelines suggest extended prophylaxis up to 4 weeks with low-molecular-weight heparin (LMWH) in such patients. This study is conducted to determine the proportion of patients receiving thromboprophylaxis among those undergoing surgery for malignant abdominal or pelvic tumor. This prospective, multicenter, observational study included 300 patients (217 [72.3%] were women). Mean age and duration of cancer were 53.2 and 1.2 years, respectively. A total of 162 (54%) patients received thromboprophylaxis of which only pharmacological in 78 [48.1%], only mechanical in 27 [16.7%], and both pharmacological and mechanical in 57 [35.2%] patients. LMWH (128, 79.0%) and graduated compression stockings (74, 45.7%) were the commonly used modalities. VTE prophylaxis was given in only half of the patients. Physician education to increase adherence to international guidelines is very important. Trial Registration No. CTRI/2013/05/003617.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Venous thromboembolism (VTE) occurs in 4–20% cancer patients and is a leading cause of death in patients with cancer [1]. The risk of first VTE is approximately sevenfold higher in patients with malignancy than in those without it [2]. In Indian patients diagnosed with VTE, malignancy mainly abdominal and pelvic cancer is the most common predisposing factor [3]. Further, patients with cancer undergoing surgical procedures have twice the risk of postoperative VTE and more than three times the risk of fatal pulmonary embolism (PE) than patients who undergo surgery for benign diseases [4]. Recent studies show that incidences of symptomatic deep vein thrombosis (DVT) and PE among Asian colorectal cancer surgery patients are comparable to those in the West [5]. Likewise the prevalence of PE in cancer patients in India is not as low as originally assumed, and PE is associated with high mortality in these patients [6].
A significant percentage of morbidity and mortality in cancer patients can be attributed to hypercoagulation [7]. In addition to the hypercoagulable state associated with malignancy, cancer-related surgery, chemotherapy, and immobilization further increase the risk of VTE [7]. Despite the risk of VTE complications in patients with a malignancy, a large number of hospitalized patients undergoing major abdominal or pelvic surgery for cancer are still not prescribed appropriate thromboprophylaxis [8].
The American Society of Clinical Oncology (ASCO) guidelines recommend that patients undergoing major surgery for malignant disease should be considered for pharmacologic thromboprophylaxis, while patients undergoing major abdominal or pelvic surgery for cancer who have high-risk features, such as restricted mobility, should be administered extended prophylaxis with low-molecular-weight heparin (LMWH) for up to 4 weeks postoperatively [9, 10]. Similarly, the European Society of Medical Oncology (ESMO) guidelines (2011) state that cancer patients undergoing elective major abdominal or pelvic surgery should receive in hospital and post-discharge prophylaxis with subcutaneous LMWH for up to 1 month after surgery [11].
However, there are limited data available on whether these recommendations have impacted the real-world management of cancer surgery patients and led to changes in the routine clinical practice [12]. Although many trials have evaluated the efficacy and safety of anticoagulants for prophylaxis after major abdominal surgery, most of these trials included only a small proportion of patients who were undergoing surgery for cancer [13]. Further there are no India-specific data regarding the proportion of patients who are given thromboprophylaxis when undergoing surgery for malignant abdominal or pelvic tumor. Therefore, this study was conducted to determine the proportion of patients receiving thromboprophylaxis among those undergoing surgery for malignant abdominal or pelvic tumor. The secondary objectives were to determine the proportion of patients who develop symptomatic DVT, to evaluate the profile of the patients (in terms of age, gender, type of malignant tumor, stage of malignancy, and type of admitting hospital), and to determine the reasons for not giving thromboprophylaxis.
Methods
This prospective multicenter observational study (trial registration no: CTRI/2013/05/003617) was conducted in accordance with the principles laid by the 18th World Medical Assembly (Helsinki, 1964) and all subsequent amendments and guidelines for Good Epidemiology Practice. Each participating site ensured that all necessary regulatory submissions (e.g., independent ethics committee) were performed in accordance with local regulations including local data protection regulations.
Eligibility Criteria
Adults (≥ 18 years of age), who were hospitalized for abdominal or pelvic malignant tumor (such as colon, rectum, stomach, liver, pancreas, prostate, urinary bladder, uterus, and ovary) and had undergone surgery for this malignant tumor in the preceding 2 days, were included after undertaking an informed consent. Patients, who had a life expectancy of less than 1 month and were participating in another clinical trial, were excluded.
Data Collection and Validation
The recruitment period was 11 months. The data were recorded prospectively for individual patients during the follow-up period of either 30 ± 7 days or at discharge, whichever was later.
During the course of the study, the investigator assessed the patient for clinical signs of DVT such as pain, swelling, and redness of the leg and dilatation of the surface veins. If the patient showed signs, he/she was evaluated for symptomatic DVT using Doppler ultrasonography.
At baseline visit, details of abdominal or pelvic cancer such as type of cancer, metastasis [14], and anticancer treatment employed; and details of DVT prophylaxis like duration and type of thromboprophylaxis, and reasons for not giving DVT prophylaxis, were recorded. At the mandatory last visit (i.e. at discharge or at 30 ± 7 days, whichever was later), details of DVT prophylaxis and reasons for not giving DVT prophylaxis were recorded. Data were collected using electronic case report forms.
Statistical Analysis
Determination of sample size: Assuming that 44% of the patients would be given thromboprophylaxis [13], with 90% confidence interval (CI) and 5% precision, 265 subjects were required for this study. Considering a drop-out of 10%, it was planned to recruit 295 subjects.
Statistical methods: Cochran–Mantel–Haenszel test and chi-squared test were used to make comparisons between groups. A p value < 0.05 was considered as significant.
Results
Among the 13 recruited investigators, 11 were surgical oncologist, 1 was a medical oncologist, and 1 was a surgical gastroenterologist. They were recruited from different geographical locations in India—1 from the north, 2 from west, 3 from east, and the remaining 7 from the south.
Patient Disposition
Between December 2012 and November 2013, a total of 306 patients were enrolled. Out of 306 patients, 300 patients were considered for analysis as 6 patients did not meet the eligibility criteria (5 patients did not sign the informed consent form within 2 days, and the histopathology report showed a benign ovarian mass for 1 patient). Out of 300 patients, 298 patients (99.3%) completed the study, and 2 patients (0.7%) died during the course of the study.
Baseline Characteristics
Of 300 patients, 217 (72.3%) were women. The mean ± standard deviation (SD) age was 53.2 ± 12.2 years. Ovarian cancer (n = 79, 26.3%) was the most common type of cancer. Among the stages of cancer, stage I (n = 70, 23.3%) was the most common. The most frequently (n = 23, 7.7%) observed metastasis was of “other” type which included metastasis resulting in rectovaginal fistula or ascites, periaortic (around abdominal aorta), and periportal (around portal vein) metastasis, supraclavicular, para-aortic lymph nodes, and metastasis to peritoneum, cervix, omentum, lymph node, rectum, endometrium, and caecum. In total, 63 (21.0%) patients had received chemotherapy, 18 (6.0%) patients had received radiation, 10 (3.3%) patients had undergone surgery (prior to this hospitalization), and 2 (0.7%) patients had taken hormonal therapy. Some patients had taken more than one therapy prior to this study. The mean ± SD duration of cancer was 1.2 ± 0.7 years. (Table 1).
Proportion of Patients Who Were Given Thromboprophylaxis
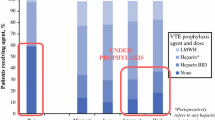
Of the 300 patients, 162 (54%, 90% CI: 0.49–0.59) patients received thromboprophylaxis either at baseline visit or at 30-day visit or at discharge, while 138 patients did not receive thromboprophylaxis. Out of 162 patients who received thromboprophylaxis, most (n = 100; 61.7%) patients received it for ≤7 days, while approximately one-fourth of the patients (42 [25.9%]) received thromboprophylaxis for 8–15 days (online resource: Supplementary Table 1). Seventy-one (43.8%) patients received thromboprophylaxis only at baseline; 4 (2.5%) patients received it only at discharge; 77 (47.5%) patients received at baseline and discharge; and 10 (6.2%) patients received at baseline, discharge, and at 30-day visit. Overall, 78/162 (48.1%) patients were given only pharmacological thromboprophylaxis, 27/162 (16.7%) patients received only mechanical thromboprophylaxis, and 57/162 (35.2%) patients received both pharmacological and mechanical thromboprophylaxis. LMWH (128/162, 79.0%) and graduated compression stockings (74/162, 45.7%) were the most commonly used pharmacological and mechanical thromboprophylaxis, respectively. (Table 2).
Proportion of Patients Who Developed Symptomatic Deep Vein Thrombosis
None of the patients assessed at the end of 30 days or at discharge (after 30 days) had symptoms of DVT.
Evaluation of the Profile of Patients Who Were Given Thromboprophylaxis
Among the age groups analyzed, the age group of ≥ 60 years had the highest proportion (64/107; 59.8%) of patients receiving thromboprophylaxis. Overall, 50/83 (60.2%) men and 112/217 (51.6%) women enrolled received thromboprophylaxis. The most frequently reported type of cancer was ovarian cancer, and 40/79 (50.6%) patients suffering from ovarian cancer received thromboprophylaxis. Of the 299 patients who had cancer for 1–5 years, 161 (53.8%) patients received thromboprophylaxis; one patient had cancer for > 10 years and received thromboprophylaxis. Among patients with stage I and stage II A (the most frequently reported stages of cancer), 31/70 (44.3%) and 39/62 (62.9%), respectively, received thromboprophylaxis. Thromboprophylaxis was given in greater proportion of patients with metastasis than those without metastasis (61.3% vs 53.2%) (online resource: Supplementary Table 2).
Reasons for Not Administering Thromboprophylaxis
For the 138 patients who did not receive thromboprophylaxis throughout the study, “patient was stable,” “the patient was stable and had no signs of DVT,” “early ambulation was encouraged,” and “risk of bleeding” were the major reasons for not administering pharmacological or mechanical thromboprophylaxis. (Table 3).
Discussion
This prospective multicenter observational study showed that of the total 300 patients, who underwent surgery for malignant abdominal or pelvic tumor, approximately half of the patients received thromboprophylaxis. Of the patients who received thromboprophylaxis, nearly 48.1% received only pharmacological thromboprophylaxis, 16.7% received only mechanical, and 35.2% received both pharmacological and mechanical thromboprophylaxis. The proportion of patients, in whom thromboprophylaxis was given, was greater in men, in patients > 60 years, and in those with metastasis. LMWH and graduated compression stockings were the most commonly used thromboprophylaxis. Most patients who did not receive thromboprophylaxis were considered “stable” as per the investigator. None of the patients had symptoms of DVT.
The recommendations for thromboprophylaxis may vary slightly between different guidelines, but all major international guidelines like NCCN (National Comprehensive Cancer Network), ASCO, ESMO, and IMWG (International Multidisciplinary Working Group) broadly recommend postoperative thromboprophylaxis with LMWH for 7–10 days in cancer patients undergoing major surgery and for up to 4 weeks in cancer patients undergoing major abdominal or pelvic surgery [9,10,11]. In this study 54% patients received thromboprophylaxis which is higher than the 44% thromboprophylaxis rate seen in a multicenter prospective cohort study that included patients admitted in medical and surgical ICUs (Intensive care units) in India with at least two risk factors (not including sepsis) for DVT + ICU stay > 24 h or one risk factor (not sepsis) for DVT + ICU stay > 48 h [15]. However, the rate of thromboprophylaxis observed in this study was lower (54% vs 75.2%) than that observed in a retrospective medical record review in 10 teaching/community-based hospitals located in the United States [16]. Also the rate of pharmacological thromboprophylaxis in this study was lower than another prospective, observational study conducted between November 2009 and November 2010 in France in patients undergoing surgery for abdominal or pelvic cancer [12].
Of the patients who received thromboprophylaxis, LMWH was given in 79% of patients in this study. LMWHs are the preferred options over unfractionated heparin (UFH) for primary and secondary VTE prophylaxis on account of a number of benefits such as higher bioavailability (90% vs 30%), longer half-life (4–6 h vs 0.5–1 h), predictable and reproducible anticoagulant response, minimal interaction with non-anticoagulant related plasma proteins, and lesser propensity to cause heparin-induced thrombocytopenia and osteoporosis.
In our study, none of the patients had symptoms of DVT. Likewise, in another study conducted at Tata Memorial Hospital, India, between March 2002 and January 2004, in 99 patients undergoing surgery for colorectal cancer, no DVT was detected, and the study was terminated as the authors felt that the anticipated incidence of DVT may have been overestimated during sample size calculation [17]. In a retrospective study conducted at the Asian Medical Center, Seoul, South Korea, including 3645 patients who underwent colorectal cancer surgery between January 2006 and December 2008, 0.85% patients developed DVT [5]. However a multicenter, double-blind trial conducted at 10 university hospitals in Canada in patients undergoing colorectal cancer surgery showed a considerably higher DVT rate of 13.9% [18]. Genetic factors—like a low prevalence of the thrombophilic trait (known as factor V Leiden mutation) and thrombin gene 20210A, low mean levels of fibrinogen, factor VIIc, and factor VIIIc—may contribute to the low prevalence of VTE in Asian population [19]. However, recent studies show that the incidences of symptomatic DVT and PE are comparable among Asian and Western population [5, 6]. Therefore, the reason for the absence of DVT in our study is not clear as it could either be attributed to a low prevalence of DVT in the study population or indicate adequacy of methods used for thromboprophylaxis and risk stratification or underscore a study limitation in terms of assessing the presence of only symptomatic DVT.
Among the three age groups in the study, the proportion of patients in whom thromboprophylaxis was given was highest for the age group of ≥ 60 years; this can be explained by the high risk of thrombosis observed in patients ≥ 60 years (2.63, 95% CI: 1.21–5.71) [20]. A total of 161/299 (53.8%) patients who had cancer for 1–5 years received thromboprophylaxis. Studies have shown that the risk of VTE is highest in the immediate period after diagnosis of cancer, with the adjusted odds ratio (OR) for developing VTE declining from 53.5 (95% CI: 8.6–334.3) in the first 3 months to 14.3 (95% CI: 5.8–35.2) in the period between 3 months and 1 year and to 3.6 (95% CI: 2.0–6.5) in between 1- and 3-year interval [2, 21]. Most patients who did not receive thromboprophylaxis in this study were considered “stable” as per the investigator or were those in whom early ambulation was encouraged or had contraindications like risk of bleeding.
Strengths and Limitations of the Study
In view of the absence of studies determining the extent of thromboprophylaxis in Indian patients undergoing surgery for malignant abdominal or pelvic tumor, this study presents vital data on the thromboprophylaxis rate in these patients and also explores other key factors like the patient profile and primary reasons for not administering thromboprophylaxis. The study included patients from all four zones (north, south, east, and west) of India, and the 13 participating investigators varied on the basis of professional experience, thus providing diversity to the results. However, the patients were not evaluated for the presence of pulmonary embolism, which could be an important cause of death after discharge. Further, only patients having clinical signs of DVT were further evaluated using Doppler ultrasonography, and therefore, the study only assessed the presence of symptomatic DVT. Further studies to assess the presence of asymptomatic DVT in this population are required as 80% of DVT cases are asymptomatic [22].
Conclusion
Cancer patients undergoing surgery represent very high risk for developing VTE and thromboprophylaxis is crucial in preventing VTE-related events. Physician education to increase adherence to international guidelines and strategies to promote compliance will go a long way in reducing morbidity and mortality in these patients.
References
Lyman GH (2009) Preventing venous thromboembolism in cancer patients: can we do better? Journal of Oncology Practice 5:165–166
Blom JW, Doggen CJ, Osanto S, Rosendaal FR (2005) Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA 293:715–722
Lee A, Stephen E, Agarwal S, Premkumar P (2009) Venous thrombo-embolism in India. Eur J Vasc Endovasc Surg 37:482–485
Kakkar AK, Williamson R, editors. Prevention of venous thromboembolism in cancer patients. Seminars in thrombosis and hemostasis; 1998
Yang S-S, Yu CS, Yoon YS, Yoon SN, Lim S-B, Kim JC (2011) Symptomatic venous thromboembolism in Asian colorectal cancer surgery patients. World J Surg 35:881–887
Sawant S, Banumathy S, Daddi A, Dhir A (2012) Pulmonary embolism in cancer patients. Indian J Cancer 49:119–124
Caine GJ, Stonelake PS, Lip GY, Kehoe ST (2002) The hypercoagulable state of malignancy: pathogenesis and current debate. Neoplasia 4:465–473
Vazquez FJ, Bilbao MS, Saimovici J, Vaccaro C (2015) Improving adherence rate of extended prophylaxis for venous thromboembolic disease after abdominal and pelvic oncologic surgery: a pilot educational study. Clin Appl Thromb Hemost 21:750–754
Lyman GH, Bohlke K, Khorana AA, Kuderer NM, Lee AY, Arcelus JI, Balaban EP, Clarke JM, Flowers CR, Francis CW, Gates LE, Kakkar AK, Key NS, Levine MN, Liebman HA, Tempero MA, Wong SL, Somerfield MR, Falanga A, American Society of Clinical Oncology (2015) Venous thromboembolism prophylaxis and treatment in patients with cancer: American Society of Clinical Oncology clinical practice guideline update 2014. J Clin Oncol 33:654–656
Key NS, Khorana AA, Kuderer NM, Bohlke K, Lee AY, Arcelus JI et al (2019) Venous thromboembolism prophylaxis and treatment in patients with Cancer: ASCO clinical practice guideline update. J Clin Oncol 38:496–520
Mandala M, Falanga A, Roila F, Group EGW (2011) Management of venous thromboembolism (VTE) in cancer patients: ESMO clinical practice guidelines. Ann Oncol 22(suppl 6):vi85–vi92
Samama C-M, Boubli L, Coloby P, Debourdeau P, Gruel Y, Mariette C, Mottier D, Rischmann P, Toubiana L, Steib A (2014) Venous thromboembolism prophylaxis in patients undergoing abdominal or pelvic surgery for cancer—a real-world, prospective, observational French study: PRéOBS. Thromb Res 133:985–992
Carrier M, Lee AY (2009) Prophylactic and therapeutic anticoagulation for thrombosis—major issues in oncology. Nat Clin Pract Oncol 6:74–84
Edge SB, Compton CC (2010) The American joint committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 17:1471–1474
Todi S, Sinha S, Chakraborty A, Sarkar A, Gupta S, Das T et al (2003) Utilisation of deep venous thrombosis prophylaxis in medical/surgical intensive care units. Indian J Crit Care Med 7:103
Stratton MA, Anderson FA, Bussey HI, Caprini J, Comerota A, Haines ST, Hawkins DW, O'Connell MB, Smith RC, Stringer KA (2000) Prevention of venous thromboembolism: adherence to the 1995 American College of Chest Physicians consensus guidelines for surgical patients. Arch Intern Med 160:334–340
Shukla PJ, Siddachari R, Ahire S, Arya S, Ramani S, Barreto SG, Gupta S, Shrikhande SV, Jagannath P, Desouza LJ (2008) Postoperative deep vein thrombosis in patients with colorectal cancer. Indian J Gastroenterol 27:71–73
McLeod RS, Geerts WH, Sniderman KW, Greenwood C, Gregoire RC, Taylor BM, Silverman RE, Atkinson KG, Burnstein M, Marshall JC, Burul CJ, Anderson DR, Ross T, Wilson SR, Barton P, Canadian Colorectal Surgery DVT Prophylaxis Trial investigators (2001) Subcutaneous heparin versus low-molecular-weight heparin as thromboprophylaxis in patients undergoing colorectal surgery: results of the Canadian colorectal DVT prophylaxis trial: a randomized, double-blind trial. Ann Surg 233:438–444
Stein PD, Kayali F, Olson RE, Milford CE (2004) Pulmonary thromboembolism in Asians/Pacific islanders in the United States: analysis of data from the National Hospital Discharge Survey and the United States Bureau of the Census. Am J Med 116:435–442
Agnelli G, Bolis G, Capussotti L, Scarpa RM, Tonelli F, Bonizzoni E, Moia M, Parazzini F, Rossi R, Sonaglia F, Valarani B, Bianchini C, Gussoni G (2006) A clinical outcome-based prospective study on venous thromboembolism after cancer surgery: the @RISTOS project. Ann Surg 243:89–95
Khorana AA, Connolly GC (2009) Assessing risk of venous thromboembolism in the patient with cancer. J Clin Onc 27:4839–4847
Gandharba Ray MB (2010) Venous thromboembolism- Indian perspective. Medicine Update 20:329–334
Acknowledgements
The authors would like to thank the study participants, their family, and caregivers who were involved in this study. We thank the following participating investigators: Dr. Rupesh Mehta (Ahmedabad), Dr. S.R Krishnamurthy (Coimbatore), Dr. Jacob Kurien (Calicut), Dr. Sudhir Rawal (New Delhi), Dr. M.G Nagakishore (Guntur), Dr. Vijay Tuljapurkar (Miraj), Dr. Suchetha Jyotish (Thiruvananthapuram), Dr. M. Gopichand (Vijyawada), Dr. Ritesh Tapkire (Cachar), Dr. Diptendra Sarkar (Kolkata), Dr. Jaydip Biswas (Kolkata), Dr. Arul Raj (Coimbatore), and Dr. Govindaraj (Trichy). Editorial support in the preparation of this publication was provided by Alina Gomes, Anahita Gouri, Rohan Mitra, and Vijay Bhushanam of Sanofi, India. Clinical trial coordination support was provided by Chaitali Sunil Nashikkar of Tata Memorial Hospital. The authors acknowledge Zifo Technologies for data management and Sciformix Technologies Pvt. Ltd. for contribution in statistics and preparation of study report. The authors individually and collectively are responsible for all content and editorial decisions and received no payment from Sanofi directly or indirectly (through a third party) related to the development/presentation of this publication.
Funding
This study was sponsored by Sanofi.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
Gastro-intestinal disease management group of Tata Memorial Hospital received honorarium for conducting this study. Manish Verma is an employee of Sanofi.
Data Availability
Qualified researchers may request access to patient-level data and related study documents including the clinical study report, study protocol with any amendments, blank case report form, statistical analysis plan, and dataset specifications. Patient-level data will be anonymized and study documents will be redacted to protect the privacy of trial participants. Further details on Sanofi's data sharing criteria, eligible studies, and process for requesting access can be found at https://www.clinicalstudydatarequest.com.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
Supplementary Table 1 Duration of thromboprophylaxis, Supplementary Table 2. Patient profile (DOCX 18 kb).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shrikhande, S.V., Verma, M. A Prospective Observational Study to Determine Rate of Thromboprophylaxis in Oncology Patients Undergoing Abdominal or Pelvic Surgery. Indian J Surg Oncol 12, 279–285 (2021). https://doi.org/10.1007/s13193-021-01281-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13193-021-01281-0