
Abstract
Introduction
Dipeptidyl peptidase-4 (DPP-4) inhibitors reduce blood glucose in a dose-dependent manner, but the dose-dependent effect relationship between DPP-4 inhibitors and atherosclerosis has not been investigated.
Methods
Patients with type 2 diabetes mellitus (T2DM) treated with insulin were randomized to the sitagliptin (n = 137) or conventional treatment group (n = 137). In the sitagliptin group, each investigator was allowed to adjust the sitagliptin dose to avoid hypoglycemia. In this post hoc analysis, subjects in the sitagliptin group were divided into two groups based on the average dose of sitagliptin during the study period: greater than or equal to median (higher sitagliptin dose group) or less than median (lower sitagliptin dose group).
Results
In this study, subjects were divided into three groups: the conventional treatment group (n = 137), lower sitagliptin dose group (n = 42), and higher sitagliptin dose group (n = 95). The higher sitagliptin dose group had a significantly larger reduction in HbA1c (−0.62 ± 1.05%) than the conventional treatment group (−0.20 ± 0.91%, P = 0.007). Over 104 weeks, the higher sitagliptin dose significantly reduced the mean intima media thickness-common carotid artery (IMT-CCA) and left max-IMT-CCA relative to baseline. In addition, the higher sitagliptin dose significantly inhibited the progression in mean-IMT-CCA compared with conventional treatment. Multiple linear regression analysis showed that changes in mean-IMT-CCA and left max-IMT-CCA decreased with higher sitagliptin dose.
Conclusions
Addition of sitagliptin to insulin therapy might attenuate the progression of atherosclerosis in patients with T2DM in a dose-dependent manner.
Funding
Mitsubishi Tanabe Pharma Co., Ono Pharmaceutical Co., and Novo Nordisk.
Clinical trial registration
UMIN000007396
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Type 2 diabetes mellitus (T2DM) is a strong risk factor for cardiovascular disease (CVD). One of the main goals in T2DM management is to reduce the incidence of CVD through glycemic control and modification of risk factors for atherosclerosis [1]. To achieve this goal, it is important to choose oral hypoglycemic agents (OHAs) that can slow down the progression of atherosclerosis.
Carotid artery intima media thickness (IMT) and its progression as evaluated by ultrasonography are well-established markers of atherosclerosis [2,3,4]. To evaluate the effect of dipeptidyl peptidase-4 (DPP-4) inhibitors on IMT, we previously conducted the Sitagliptin Preventive Study of Intima-Media Thickness Evaluation (SPIKE). In this study, we demonstrated that sitagliptin attenuates the progression of carotid IMT in patients with T2DM treated with insulin without increasing the risk of hypoglycemia and weight gain compared to patients who received conventional therapy [5].
After DPP-4 inhibitors were launched on the market in Japan in 2009, frequent hypoglycemic events were reported, especially in elderly patients with renal dysfunction treated with high-dose sulfonylureas in routine clinical settings [6]. Taking these adverse effects of DPP-4 inhibitors into consideration, the Japan Association for Diabetes and Education Care committee on adequate use of incretin-based therapy released a warning that the dose of insulin should be reduced when it is used in combination with DPP-4 inhibitors [7]. In response to this recommendation, in the SPIKE study we left the starting dose of sitagliptin to each investigator’s discretion when it was used with insulin to avoid the risk of hypoglycemia. As a result, the dose of sitagliptin varied among patients in the sitagliptin treatment group even though sitagliptin improved glycemic control in a dose-dependent manner [8]. In addition to its dose-dependent glucose-lowering effect, sitagliptin was associated with a dose-dependent reduction of the intima-media ratio in an obese rat model of diabetes [9]. Nevertheless, we have not yet considered whether the dose of sitagliptin affects the progression of atherosclerosis. Thus, the aim of this post hoc analysis is to investigate the dose-dependent effect of sitagliptin on the progression of atherosclerosis.
Methods
Study Population
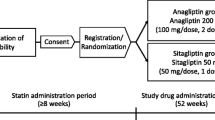
We conducted a post hoc analysis of the SPIKE study, whose methods were described in detail previously [5, 10,11,12,13,14]. Briefly, a total of 282 Japanese patients with T2DM treated with insulin and no past history of apparent CVD were randomly allocated to either the sitagliptin group (n = 142) or the conventional treatment group (n = 140). Randomization was performed using a dynamic allocation method based on age, gender, number of insulin injections daily, and concurrent pioglitazone use. Patients in the sitagliptin group were started on sitagliptin at 25 mg once daily in addition to ongoing insulin therapy. Initiation of sitagliptin at 50 mg once daily was permitted in patients not on any sulfonylureas. After 12 weeks of treatment with sitagliptin at 25 or 50 mg, the dose of sitagliptin was scheduled to increase to a maximum of 100 mg once daily if HbA1c was ≥7.0% (8.6 mmol/l) [15]. However, participating physicians were allowed to reduce sitagliptin to 25 or 50 mg/day if treatment with 50 or 100 mg/day was considered to be poorly tolerated. Insulin dose adjustment was also permitted. In the conventional treatment group, either increasing the dose of current therapy (e.g., insulin) or the addition of OHAs was allowed to achieve optimal glycemic control [15]. The addition of other DPP-4 inhibitors and glucagon-like peptide-1 (GLP-1) analogs was not allowed in either group. All patients who agreed to participate provided written informed consent before being enrolled into the study. The SPIKE study was registered with the University Hospital Medical Information Network Clinical Trials Registry (UMIN000007396) and met the requirements of the International Committee of Medical Journal Editors.
Compliance with Ethical Guidelines
The study protocol was approved by the institutional review board of each participating institutionand complies with the current legal regulations in Japan. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964, as revised in 2013. Informed consent was obtained from all patients for being included in the study.
Measurement of Carotid IMT
Each participant underwent ultrasonography of the carotid arteries by expert sonographers at the start of the study [5, 10]. All scans were electronically stored and emailed to the IMT Evaluation Committee (Osaka, Japan), where a single experienced reader blinded to the clinical characteristics of the patients interpreted them using automated digital edge-detection software (Intimascope; MediaCross, Tokyo, Japan). The software system evaluates an average of approximately 200 IMT values in a segment 2 cm proximal to the dilation of the carotid bulb (mean-IMT-CCA). Maximum IMT, including plaque lesions in the common carotid arteries (max-IMT-CCA), were measured separately.
Statistical Analysis
Results are presented as mean ± SD, medians (interquartile range), or number (proportion) of patients. Patients in the sitagliptin group were further classified into two subgroups based on whether their average dose of sitagliptin during the study period was greater than or equal to the median dose (higher sitagliptin dose group) or less than the median dose (lower sitagliptin dose group). We analyzed the differences between these two groups and the conventional group. Baseline and follow-up group comparisons were assessed using analysis of variance (ANOVA) for continuous variables and Fisher’s exact test for categorical variables. Changes from baseline to 104 weeks were analyzed using a one-sample t test within each group. Differences in delta change in clinical parameters from baseline to 104 weeks among groups were analyzed with ANOVA followed by the Tukey-Kramer test. Differences in delta change in IMT from baseline to 104 weeks among groups were analyzed with analysis of covariance (ANCOVA) followed by the Tukey-Kramer test.
Trends in the change in IMT across the three groups were evaluated using linear regression analysis with an unadjusted model that included only the treatment group (henceforth, model 1) and the following models: model 2 (model 1 + age, gender, and baseline IMT), model 3 (model 2 + HbA1c at baseline, sulfonylurea use, and glinide use), and model 4 (model 3 + change in HbA1c from baseline to 104 weeks).
All statistical tests were two-sided with a significance level of 5%. All analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC, USA).
Results
Results from the Original SPIKE Study
Among a total of 282 participants, 137 in the sitagliptin group and 137 in the conventional treatment group were included in the full analysis set for the original study. Baseline clinical characteristics were comparable between the groups as previously described [5]. In the original study, patients who received sitagliptin had significantly greater reductions in mean-IMT-CCA and left max-IMT-CCA but not right max-IMT-CCA than patients receiving conventional treatment [5].
Baseline Characteristics
In this post hoc analysis, subjects were divided into three groups: the conventional treatment group (n = 137), lower sitagliptin dose group (n = 42; average dose about 5 mg n = 1, about10 mg n = 2, about 15 mg n = 1, about 20 mg n = 3, about 25 mg n = 18, about 40 mg n = 7, about 45 mg n = 10), and higher sitagliptin dose group (n = 95; average dose about 50 mg n = 54, about 55 mg n = 3, about 60 mg n = 1, about 65 mg n = 1, about 70 mg n = 4, about 75 mg n = 4, about 80 mg n = 5, about 85 mg n = 5, about 90 mg n = 18). The mean dose of sitagliptin was 53.2 mg/day (median 50 mg/day) among patients who received sitagliptin in the original study. The mean dose in the higher sitagliptin dose group was 63.3 mg/day, and the mean dose in the lower sitagliptin dose group was 30.5 mg/day. Demographic and baseline characteristics of the three groups were well balanced except for HbA1c, sulfonylurea use, and glinide use (Table 1). During the study, five patients developed CVD (the conventional treatment group, n = 2; lower sitagliptin dose group, n = 1; higher sitagliptin dose group, n = 2, P = 0.85).
Changes in Clinical Parameters in the Three Groups
Although higher sitagliptin dose and conventional treatment both significantly reduced HbA1c levels from baseline, the improvement in HbA1c was significantly greater in the higher sitagliptin dose group (−0.62 ± 1.05%) than in the conventional treatment group (−0.20 ± 0.91%, P = 0.007), but not than the lower sitagliptin dose group (Table 2). On the other hand, body mass index, blood pressure, lipid parameters, and renal function were not significantly different among the three groups during the observation period (Table 2). With respect to hypoglycemic events, there was a significant difference in the mean number of events among the three groups (0.36 ± 0.80 episodes/month/person in the conventional treatment group, 0.67 ± 1.28 in the lower sitagliptin dose group, and 0.20 ± 0.52 in the higher sitagliptin dose group, P = 0.008 by ANOVA). On average, patients in the higher sitagliptin dose group had fewer hypoglycemic events than patients in the lower sitagliptin dose group (P = 0.006 by Tukey-Kramer test).
Changes in IMT-CCA Among the Three Groups
Over 104 weeks, a higher sitagliptin dose was associated with reduced mean-IMT-CCA and left max-IMT-CCA relative to baseline (Table 3), but not a lower sitagliptin dose or conventional treatment. In an ANOVA model that adjusted for group, age, gender, and IMT values at baseline, a higher sitagliptin dose significantly prevented progression of mean-IMT-CCA and tended to prevent progression of left max-IMT-CCA when compared with conventional treatment (Table 4).
Furthermore, we investigated the dose-dependent effect of sitagliptin on the progression of atherosclerosis. Linear regression analysis showed a negative linear trend between treatment group and changes in IMT-CCA and left max-IMT-CCA, but not right max-IMT-CCA, in the unadjusted model (model 1) and adjusted models (models 2–4) (Table 5). Similarly, there was a negative linear trend between the average dose of sitagliptin over 104 weeks (the dose of sitagliptin in the conventional treatment group was defined as 0 mg) and changes in IMT-CCA and left max-IMT-CCA, but not right max-IMT-CCA (Table 6).
Discussion
In this post hoc study, sitagliptin as an addition to insulin therapy attenuated the progression of atherosclerosis in patients with T2DM in a dose-dependent manner. Thus, this finding lends support to the conclusion that this anti-atherosclerotic effect was due to the drug effect of sitagliptin itself.
A previous study demonstrated that sitagliptin inhibited plasma DPP-4 activity over 24 h and increased active GLP-1 levels in a dose-dependent manner after an oral glucose tolerance test, but there was no difference in effect on glucose excursion after an oral glucose tolerance test between a single oral 25- or 200-mg dose of sitagliptin [16]. On the other hand, sitagliptin reduced HbA1c in a dose-dependent manner over 12 weeks in a longer-term study [8]. In that study, the addition of sitagliptin to insulin therapy nearly dose-dependently reduced HbA1c levels over 104 weeks. From this point of view, one might expect that a higher dose of sitagliptin can significantly reduce carotid atherosclerosis through its glucose-lowering effects. In fact, a higher sitagliptin dose attenuated the progression of carotid atherosclerosis along with reducing HbA1c levels. However, sitagliptin treatment still attenuated the progression of mean-IMT-CCA and left max-IMT-CCA in a dose-dependent manner even after adjusting for changes in HbA1c from baseline. This suggests that sitagliptin treatment attenuated the progression of carotid artery atherosclerosis in a dose-dependent manner independent of its glucose-lowering effects.
The exact mechanism by which sitagliptin attenuates the progression of carotid IMT remains unclear in this post hoc analysis. One possibility is that sitagliptin slowed it down by enhancing GLP-1 signaling; a previous study demonstrated that sitagliptin increased GLP-1 activity in a dose-dependent manner after an oral glucose tolerance test [16]. In fact, des-fluoro-sitagliptin was reported to inhibit macrophage inflammation through enhancement of GLP-1 signaling in a dose-dependent manner in an in vitro study [17]. Another possibility is that DPP-4 inhibitors have the potential to inhibit the progression of atherosclerosis in a GLP-1–independent manner. DPP-4 inhibitors have various functions in vascular cells. In a rat model of diabetes [9], sitagliptin reduced neointimal formation after carotid injury in a dose-dependent manner. In the same study, sitagliptin inhibited smooth muscle cell proliferation and monocyte adhesion in a dose-dependent manner independent of GLP-1 activity in vitro. Consistent with these findings, we previously demonstrated that anagliptin, another DPP-4 inhibitor, suppresses smooth muscle cell proliferation and reduces macrophage inflammation almost in a dose-dependent manner [18]. Taken together, the anti-atherosclerotic effect of DPP-4 inhibitors may be independent of their glycemic effects in a dose-dependent manner; however, it is unclear whether the effects are mediated by GLP-1.
In this post hoc analysis, some investigators probably used lower doses of sitagliptin because of concerns about hypoglycemia when sitagliptin is used as an adjunct to insulin therapy. Unexpectedly, the number of hypoglycemic events was significantly higher in the lower sitagliptin dose group than in the higher sitagliptin dose treatment group. This may be associated with imbalances in sulfonylurea use among groups. In other words, add-on sitagliptin therapy increased the number of hypoglycemic events in patients on insulin and sulfonylurea combination therapy even though healthcare providers lowered the dose of sitagliptin. More episodes of hypoglycemia may reduce the beneficial effect of sitagliptin on the changes in carotid IMT. Indeed, we previously demonstrated that a higher frequency of hypoglycemia is associated with increases in carotid IMT [14]. Thus, we should take precautions against potential hypoglycemia when DPP-4 inhibitors are added to insulin and sulfonylurea combination therapy. On the other hand, a higher sitagliptin dose attenuated the progression of carotid IMT without increasing the number of hypoglycemic events. Thus, we may consider using a higher dose of DPP-4 inhibitors from the perspective of preventing the progression of atherosclerosis while reducing the dose of insulin or reducing or discontinuing sulfonylurea therapy.
The present study has certain limitations. First, because this was an exploratory post hoc analysis of a randomized open-label trial, the findings may be limited. In particular, the classification of subgroups based on the average dose of sitagliptin may cause selection bias that interferes the results although we conducted the analysis adjusting for an imbalance in baseline characteristics among groups. Second, because these were exploratory analyses, the issue of multiple statistical comparisons becomes a concern, and findings should be interpreted with caution. Third, the carotid IMT results were not completely consistent, although the results tended to show a similar pattern. These differences may be associated with the underpowered sample and differences in carotid IMT by laterality [19]. Fourth, the evaluation of average IMT by 0.01 mm may be difficult for non-experts in clinical practice although this method is well established and widely used in clinical studies. Fifth, we used surrogate markers for CVD as the primary endpoint. The reduction of IMT with sitagliptin treatment may be expected to be associated with a reduction in the onset of CVD considering the results of a meta-analysis showing that DPP-4 inhibitors have the potential to reduce the onset of CVD [20]. However, our study lacked sufficient power to detect differences in the onset of CVD. Finally, the number of patients in the lower sitagliptin dose group was small.
Conclusions
Our data suggest that sitagliptin treatment is effective in attenuating the progression of carotid atherosclerosis in a dose-dependent manner in patients with T2DM on insulin therapy.
References
Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339(4):229–34 (PubMed PMID: 9673301).
Katakami N, Kaneto H, Shimomura I. Carotid ultrasonography: a potent tool for better clinical practice in diagnosis of atherosclerosis in diabetic patients. J Diabetes Invest. 2014;5(1):3–13 (PubMed PMID: 24843729. Pubmed Central PMCID: 4025224).
Yoshida M, Mita T, Yamamoto R, Shimizu T, Ikeda F, Ohmura C, et al. Combination of the Framingham risk score and carotid intima-media thickness improves the prediction of cardiovascular events in patients with type 2 diabetes. Diabetes Care. 2012;35(1):178–80 (PubMed PMID: 22028278. Pubmed Central PMCID: 3241317).
Okayama KI, Mita T, Gosho M, Yamamoto R, Yoshida M, Kanazawa A, et al. Carotid intima-media thickness progression predicts cardiovascular events in Japanese patients with type 2 diabetes. Diabetes Res Clin Pract. 2013;101(3):286–92 (PubMed PMID: 23835494).
Mita T, Katakami N, Shiraiwa T, Yoshii H, Onuma T, Kuribayashi N, et al. Sitagliptin attenuates the progression of carotid intima-media thickening in insulin-treated patients with type 2 diabetes: the Sitagliptin Preventive Study of Intima-Media Thickness Evaluation (SPIKE): a randomized controlled trial. Diabetes Care. 2016;39(3):455–64 (PubMed PMID: 26822324).
MSD. Sitagliptin post-marketing surveillance study (in Japanese). 2010. https://www.msdconnect.jp/products/januvia/. (PubMed PMID: 23236211). Accessed 26 April 2017.
Inagaki N, Iwakura T, Iwamoto Y, Kadowaki T, Seino S, Seino Y. The committee regarding to adequate use for incretin-based therapy. https://www.nittokyo.or.jp/modules/information/index.php?content_id=19. (PubMed PMID: 22223164). Accessed 29 Sept 2011.
Iwamoto Y, Taniguchi T, Nonaka K, Okamoto T, Okuyama K, Arjona Ferreira JC, et al. Dose-ranging efficacy of sitagliptin, a dipeptidyl peptidase-4 inhibitor, in Japanese patients with type 2 diabetes mellitus. Endocr J. 2010;57(5):383–94 (PubMed PMID: 20332588).
Lim S, Choi SH, Shin H, Cho BJ, Park HS, Ahn BY, et al. Effect of a dipeptidyl peptidase-IV inhibitor, des-fluoro-sitagliptin, on neointimal formation after balloon injury in rats. PLoS One. 2012;7(4):e35007 (PubMed PMID: 22493727. Pubmed Central PMCID: 3320861).
Mita T, Katakami N, Shiraiwa T, Yoshii H, Onuma T, Kuribayashi N, et al. Rationale, design, and baseline characteristics of a clinical trial for prevention of atherosclerosis in patients with insulin-treated type 2 diabetes mellitus using DPP-4 inhibitor: the Sitagliptin Preventive study of Intima-media thickness Evaluation (SPIKE). Diabetol Metab Syndr. 2014;6(1):35 (Pubmed Central PMCID: 3973974).
Mita T, Katakami N, Shiraiwa T, Yoshii H, Gosho M, Ishii H, et al. The influence of sitagliptin on treatment-related quality of life in patients with type 2 diabetes mellitus receiving insulin treatment: a prespecified sub-analysis. Diabetes Ther Res Treat Educ Diabetes Relat Disord. 2017;8(3):693–704 (PubMed PMID: 28516377).
Mita T, Katakami N, Shiraiwa T, Yoshii H, Gosho M, Shimomura I, et al. The effect of sitagliptin on the regression of carotid intima-media thickening in patients with type 2 diabetes mellitus: a post hoc analysis of the sitagliptin preventive study of intima-media thickness evaluation. Int J Endocrinol. 2017;2017:1925305 (PubMed PMID: 28250768. Pubmed Central PMCID: 5303575).
Mita T, Katakami N, Shiraiwa T, Yoshii H, Gosho M, Shimomura I, et al. Changes in carotid intima-media thickening in patients with type 2 diabetes mellitus: subanalysis of the sitagliptin preventive study of intima-media thickness evaluation. J Diabetes Invest. 2017;8(2):254–5 (PubMed PMID: 28256102. Pubmed Central PMCID: 5334297).
Mita T, Katakami N, Shiraiwa T, Yoshii H, Kuribayashi N, Osonoi T, et al. Relationship between frequency of hypoglycemic episodes and changes in carotid atherosclerosis in insulin-treated patients with type 2 diabetes mellitus. Sci Rep. 2017;7:39965 (PubMed PMID: 28067320. Pubmed Central PMCID: 5220284).
Society TJD. Treatment guide for diabetes. In: Editorial Committee Members of “ Treatment Guide for Diabetes”, Araki E, Iwamoto Y, Kadowaki T, Kashiwagi A, Kitaoka M, Nanjo K, Tajima N, Bunkodo Co, Ltd, Tokyo, Japan. 2010. (PubMed PMID: 10698200).
Herman GA, Bergman A, Stevens C, Kotey P, Yi B, Zhao P, et al. Effect of single oral doses of sitagliptin, a dipeptidyl peptidase-4 inhibitor, on incretin and plasma glucose levels after an oral glucose tolerance test in patients with type 2 diabetes. J Clin Endocrinol Metab. 2006;91(11):4612–9 (PubMed PMID: 16912128).
Matsubara J, Sugiyama S, Sugamura K, Nakamura T, Fujiwara Y, Akiyama E, et al. A dipeptidyl peptidase-4 inhibitor, des-fluoro-sitagliptin, improves endothelial function and reduces atherosclerotic lesion formation in apolipoprotein E-deficient mice. J Am Coll Cardiol. 2012;59(3):265–76 (PubMed PMID: 22240132).
Ervinna N, Mita T, Yasunari E, Azuma K, Tanaka R, Fujimura S, et al. Anagliptin, a DPP-4 inhibitor, suppresses proliferation of vascular smooth muscles and monocyte inflammatory reaction and attenuates atherosclerosis in male apo E-deficient mice. Endocrinology. 2013;154(3):1260–70 (PubMed PMID: 23337530).
Plasencia Martinez JM, Garcia Santos JM, Paredes Martinez ML, Pastor AM. Carotid intima-media thickness and hemodynamic parameters: reproducibility of manual measurements with Doppler ultrasound. Med Ultrasonogr. 2015;17(2):167–74 PubMed PMID: 26052566.
Patil HR, Al Badarin FJ, Al Shami HA, Bhatti SK, Lavie CJ, Bell DS, et al. Meta-analysis of effect of dipeptidyl peptidase-4 inhibitors on cardiovascular risk in type 2 diabetes mellitus. Am J Cardiol. 2012;110(6):826–33 (PubMed PMID: 22703861).
Acknowledgements
Financial support was provided by the Japan Society for Patient-Reported Outcome research fund, which received funding from Mitsubishi Tanabe Pharma Co., Ono Pharmaceutical Co., and Novo Nordisk. The funder had no role in study design, data collection and analysis, decision to publish, and manuscript preparation. The study sponsors did not provide funding for the journal’s article processing fees. All named authors meet the International Committee of Medical Journal Editors (ICJME) criteria for authorship for this manuscript. All authors had full access to all of the data in this study, take complete responsibility for the integrity of the data and accuracy of the data analysis, and have given final approval to the version to be published. We confirm that all authors had access to the study data that support this publication. The authors thank all the clinical staff for their assistance with the execution of the clinical trial.
Disclosures
Tomoya Mita received research funds from MSD and Takeda Pharma K.K. and lecture fees from AstraZeneca K.K., Boehringer Ingelheim, Eli Lilly, Kowa Pharmaceutical Co., Mitsubishi Tanabe Pharma Co., MSD, Ono Pharmaceutical Co., and Takeda Pharmaceutical Co. NKa holds an endowed chair (Department of Metabolism and Atherosclerosis) established by funds from Kowa Pharmaceutical Co. In addition, Naoto Katakami has received research funds from MSD and lecture fees from Arkray Co., Ltd., Astellas Pharma Inc., Boehringer Ingelheim, Daiichi Sankyo Inc., Dainippon Sumitomo Pharma Co., Eli Lilly, Kowa Pharmaceutical Co., Kyowa Hakko Kirin Co., Ltd., Mitsubishi Tanabe Pharma Co., Novo Nordisk Pharma, Ono Pharmaceutical Co., Takeda Pharmaceutical Co., Sanofi-Aventis, and Shionogi & Co. Toshihiko Shiraiwa has received lecture fees from Boehringer Ingelheim, Sanofi-Aventis, Novo Nordisk Pharma, Novartis Pharmaceuticals, Eli Lilly, Abbott Japan, Takeda Pharmaceutical Co., Sanwa Kagaku Kenkyusho, Mitsubishi Tanabe Pharma Co., Daiichi Sankyo Inc., Astellas Pharma Inc., Ono Pharmaceutical Co., MSD, Shionogi, Pharma, and Taisho Toyama Pharmaceutical Co. Hidenori Yoshii has nothing to disclose. Masahiko Gosho has received lecture and consultant fees from Daiichi Sankyo Co., Ltd., Ferring Pharma, and Tiho Pharma K.K.; travel fees from Takeda Pharmaceutical Co.; and manuscript fees from Kowa Co., Ltd. Iichiro Shimomura has received lecture fees from Astellas Pharma Inc., AstraZeneca K.K., MSD K.K., Ono Pharmaceutical Co., Kyowa Hakko Kirin Co., Kowa Pharmaceutical Co., Sanofi K.K., Sanwa Kagaku Kenkyusho Co., Daiichi Sankyo Co., Takeda Pharma K.K., Mitsubishi Tanabe Pharma Co., Teijin Pharma, Eli Lilly Japan K.K., Nippon Boehringer Ingelheim Co., Novartis Pharma K.K., Novo Nordisk Pharma, Bayer Yakuhin, Pfizer Japan Inc., Bristol-Myers K.K., Mochida Pharmaceutical Co., Shionogi & Co., and Taisho Toyama Pharmaceutical Co. and research funds from Astellas Pharma Inc., AstraZeneca K.K., Eisai Co., MSD K.K, Otsuka Pharmaceutical Co., Ono Pharmaceutical Co., Kaken Pharmaceutical Co., Kissei Pharmaceutical Co., Kyowa Hakko Kirin Co., Sanofi K.K., Shionogi & Co., Daiichi Sankyo Co., Dainippon Sumitomo Pharma Co., Takeda Pharma K.K., Mitsubishi Tanabe Pharma Co., Teijin Pharma, Nippon Boehringer Ingelheim Co., Novartis Pharma K.K., Novo Nordisk Pharma, Pfizer Japan Inc., Bristol-Myers K.K., Mochida Pharmaceutical Co., Eli Lilly Japan K.K., Kowa Co., Ltd., Kowa Pharmaceutical Co., and Taisho Toyama Pharmaceutical Co. Hirotaka Watada has received lecture fees from Novo Nordisk, Inc., Eli Lilly and Co., Sanofi, Dainippon Sumitomo Pharma Co., Fujifilm, Bayer Health Care, Kissei Pharmaceutical Co., Mochida Pharmaceutical Co., MSD, Takeda Pharmaceutical Co., Boehringer Ingelheim Pharmaceuticals Inc., Daiichi-Sankyo, Ono Pharmaceutical Co., Ltd., Novartis Pharmaceuticals Corp., Mitsubishi Tanabe Pharma Corp., AstraZeneca LP, Kyowa Hakko Kirin Co., Ltd., Sanwa Kagaku Kenkyusho Co., Ltd., Kowa Co., Ltd., Astellas Pharma Inc.; advisory fees from Novo Nordisk, Inc., Mochida Pharma Co., AstraZeneca LP, Kowa Co., Astellas Pharma Inc., Sanofi, Boehringer Ingelheim Pharmaceuticals Inc., MSD, Mitsubishi Tanabe Pharma Corp., Novartis Pharmaceuticals Corp., Dainippon Sumitomo Pharma Co., Takeda Pharmaceutical Co., Ono Pharmaceutical Co., Pfizer Inc., and Kowa Co.; and research funds from Boehringer Ingelheim, Pfizer, Mochida Pharmaceutical Co., Sanofi-Aventis, Novo Nordisk Pharma, Novartis Pharmaceuticals, Sanwa Kagaku Kenkyusho, Terumo Corp., Eli Lilly, Mitsubishi Tanabe Pharma, Daiichi Sankyo Inc., Takeda Pharmaceutical Co., MSD, Shionogi, Pharma, Dainippon Sumitomo Pharma, Kissei Pharma, and AstraZeneca.
Compliance with Ethics Guidelines
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964, as revised in 2013. Informed consent was obtained from all patients for being included in the study.
Data Availability
The analyzed data sets are available from the corresponding author on reasonable request.
SPIKE Trial Site Investigators (Listed in Alphabetical Order)
The SPIKE study is a multicenter collaboration. In addition to the listed authors, the following SPIKE study investigators were involved in this study. Jiyugaoka Medical Clinic: Hiroki Yokoyama; Juntendo Tokyo Koto Geriatric Medical Center (Department of Medicine, Diabetology and Endocrinology): Kanae Ishida, Noriko Inagaki, Tomio Onuma, Keiko Yamashiro, Junko Yokota; Juntendo University Graduate School of Medicine (Department of Metabolism and Endocrinology): Fuki Ikeda, Koji Komiya, Yuko Sakurai, Motoyuki Tamaki; Kansai Rosai Hospital: Daisuke Azuma, Isao Hayashi, Isao Hayashi, Tsunehiko Yamamoto; Misaki Naika Clinic: Nobuichi Kuribayashi; Naka Memorial Clinic: Hidenori Isida, Takeshi Osonoi, Miyoko Saito; Osaka General Medical Center: Masahiro Hatazaki, Ryutaro Kataoka, Yutaka Umayahara; Osaka Police Hospital: Keisuke Kosugi, Ken’ya Sakamoto, Kazutomi Yoshiuchi; Osaka University Graduate School of Medicine (Department of Metabolic Medicine): Hideaki Kaneto, Taka-aki Matsuoka, Ken Ohya, Sae Uno; Sasebo Chuo Hospital: Kazunari Matsumoto, Fumi Mori, Yoshitaka Mori; and Shiraiwa Medical Clinic: Toshihiko Shiraiwa.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/074CF06070B4D456.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Mita, T., Katakami, N., Shiraiwa, T. et al. Dose-Dependent Effect of Sitagliptin on Carotid Atherosclerosis in Patients with Type 2 Diabetes Mellitus Receiving Insulin Treatment: A Post Hoc Analysis. Diabetes Ther 8, 1135–1146 (2017). https://doi.org/10.1007/s13300-017-0309-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-017-0309-9