
Abstract
Introduction
The incidence and prevalence of type 2 diabetes mellitus (T2D) are increasing in Japan, and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are commonly used to treat the disease. The objective of this study was to use a discrete choice experiment (DCE) to characterize patient preferences for clinical treatment features of two GLP-1 RAs—dulaglutide 0.75 mg and semaglutide 0.50 mg—among patients with T2D in Japan.
Methods
Adult patients with T2D in Japan were administered the DCE via a web-based survey. The DCE examined patient preferences for five treatment attributes (each described by two or three levels), including method of administration, HbA1c change, reduction in cardiovascular (CV) risk, weight change, and common side effects (i.e., nausea). Results were analyzed using multinomial and mixed logit models, and predicted choice probability was calculated to determine the overall probability that either dulaglutide or semaglutide DCE levels were preferred. One DCE choice task included a direct comparison of the dulaglutide 0.75 mg versus semaglutide 0.50 mg treatment profiles.
Results
190 subjects completed the survey; 29 were excluded after failing the predefined internal validity assessments. In the final analysis sample (N = 161), the attribute with the largest effect on the subjects’ choices was reduction in CV risk, followed by HbA1c change and common side effects. Patients’ predicted choice probability for the semaglutide profile was 78%, versus 22% for the dulaglutide profile. 28% of patients were “very willing” to initiate treatment with semaglutide’s product profile, versus 6% for dulaglutide.
Conclusion
In this study, reduction in CV risk and HbA1c change were the key drivers of GLP-1 RA medication preference in Japanese patients with T2D. Overall, the majority of the patients preferred a product with attribute levels reflecting the semaglutide 0.50 mg profile, with a known CV risk reduction benefit and superior HbA1c reduction.
Funding
Novo Nordisk.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence and prevalence of type 2 diabetes mellitus (T2D) are increasing in Japan, where an estimated 10 million people have diabetes [1]. Most patients in a non-insulin-dependent state begin T2D management with diet, exercise, and weight management. In the case of worsening glucose control, the next step is to prescribe glucose-lowering agents for patients with non-insulin-dependent T2D, starting with an oral hypoglycemic agent. If glucose levels are still uncontrolled, an add-on of non-insulin therapy may be used. If HbA1c targets are still not achieved after approximately 3 months, a combination of oral hypoglycemic agents and additional therapies can be added, such as sulfonylureas, thiazolidinediones (Tzd), dipeptidyl peptidase-4 (DPP4i) inhibitors, sodium-glucose co-transporter 2 (SGLT2) inhibitors, or glucagon-like peptide-1 (GLP-1) receptor agonists (RA), unless there are contraindications [2]. However, the exact sequence of treatments utilized depends on the pathophysiology of the patient.
Although there are various treatment alternatives, the risk and prevalence of cardiovascular (CV) disease in the T2D patient population is high. CV disease and related complications are the leading cause of death among patients with T2D, which may impact patient treatment selection [3]. Additionally, achieving glycated hemoglobin (HbA1c) targets and avoiding unwanted weight gain remain important treatment considerations, given that they are established risk factors for CV outcomes in patients with T2D [4]. Accordingly, both CV risk and body weight considerations are included in the key patient characteristics to be assessed during the first step in deciding upon the appropriate glycemic management according to the 2018 ADA/EASD Consensus Statement for Management of Hyperglycemia in T2D. However, while appropriate and timely treatment intensification has been shown to be an effective approach to managing HbA1c and microvascular complications, intensive therapy still may not significantly reduce CV events [5, 6].
Unlike most other T2D therapies, GLP-1 RAs can achieve glycemic control and reduce body weight with a low risk of hypoglycemia [7]. The proportion of patients in Japan who are currently treated with GLP-1 RAs has steadily increased over the past decade [8]. Currently, six GLP-1 RAs are approved in Japan, including liraglutide, exenatide ER, lixisenatide, dulaglutide, and semaglutide, all of which are administered via subcutaneous injection. Among these, liraglutide and semaglutide have both been reported to yield a significant CV risk reduction, while its been reported that exenatide ER and lixisenatide demonstrate CV risk neutrality in CV outcomes trials. Two of the newest GLP-1 RAs approved for use in Japan are dulaglutide and semaglutide [9]. However, semaglutide is not yet price listed in Japan. Both medications are administered once weekly.
In clinical studies, both dulaglutide 0.75 mg and 1.5 mg as well as semaglutide 0.50 mg and 1.0 mg have demonstrated efficacy in reducing HbA1c and weight, with limited patient experience of side effects such as nausea [10,11,12]. The efficacy and safety of dulaglutide has been assessed in several phase III studies (the Assessment of Weekly AdministRation of Dulaglutide in Diabetes [AWARD] program) [10] versus different comparators (exenatide [2 studies], insulin glargine [2 studies], metformin, and sitagliptin). In five studies, dulaglutide 1.5 mg had superior results versus comparator products when target HbA1c level was assessed as a primary endpoint. Similar efficacy was demonstrated in four out of five trials that assessed the 0.75 mg dosage (the only dosage available in Japan) [10]. Although CV risk reduction was not assessed in the AWARD program, macrovascular and microvascular complications as well as CV mortality outcomes have recently been examined in the Researching Cardiovascular Events with a Weekly Incretin in Diabetes (REWIND) CV outcomes trial, which evaluated dulaglutide 1.5 mg as an add-on to the standard-of-care treatment regimen [13]. The results of this trial are expected to be published during 2019. The dulaglutide 1.5 mg dose is not an approved dose in Japan, and the magnitude of the CV risk reduction shown for dulaglutide is currently unknown.
Semaglutide has similarly been evaluated in the SUSTAIN (Semaglutide Unabated Sustainability In Treatment for Type 2 Diabetes) program, which consists of multiple phase III global clinical trials that have evaluated the efficacy and safety of semaglutide versus a range of comparators. Similar to the REWIND trial design, SUSTAIN-6 evaluated CV outcomes for semaglutide as an add-on therapy to standard-of-care treatment against placebo. The results of SUSTAIN-6 showed a significant reduction in CV risk for the primary composite endpoint (26% risk reduction), which included cardiovascular death, nonfatal myocardial infarction (MI), and nonfatal stroke over a median 2.1 years of follow-up [11]. Additionally, two clinical trials in the SUSTAIN program have investigated the effect of semaglutide in a Japanese population alone. The results from these studies found semaglutide 0.50 mg and 1.0 mg to be superior to comparators for the primary endpoints of HbA1c change and weight loss [14, 15]. SUSTAIN-7, which was a head-to-head comparison of semaglutide versus dulaglutide, also showed superior outcomes for semaglutide in terms of HbA1c change and weight loss [12].
Understanding patient preferences for clinical treatment attributes of antihyperglycemic regimens may lead to therapeutic decisions that result in greater patient satisfaction and medication adherence, and thereby improve outcomes. While previous patient preference studies have examined similar treatment features of GLP-1 RAs [16,17,18,19,20], little is known about patients’ evaluation of the CV risk reduction benefit that may be obtained with GLP-1 RAs. In addition, no patient preference study has been conducted to evaluate differences in patient preferences between these two most recently approved once-weekly GLP-1 RAs.
The objective of the current study was to use a discrete choice experiment (DCE) to characterize patient preferences for the clinical treatment features of GLP-1 RAs among patients with T2D in Japan. The DCE aimed to provide insight into how patients are willing to trade off medication features that differ between dulaglutide 0.75 mg and semaglutide 0.50 mg. These doses of dulaglutide and semaglutide were selected given that dulaglutide 1.5 mg is not an approved dose in Japan and because semaglutide 0.50 mg is the expected maintenance dose.
Methods
Study Sample
Subjects were recruited by CROèe Inc., a patient recruitment organization based in Japan, which maintains the largest online database of clinical research volunteers in the region. Subjects were recruited from the CROèe Inc. patient database using a standardized recruitment email. In addition, advertisements viewable only to volunteers in the database were placed on the recruitment organization’s website, as well as in their weekly newsletter (sent via regular mail), and interested volunteers responded online. All potential subjects that responded to the email invitation, online advertisement, or newsletter were then screened by the recruitment organization online to determine eligibility.
Subjects were eligible for participation if they met the following inclusion criteria: ≥ 20 years of age at the time of enrollment; self-reported diagnosis of T2D; HbA1c ≥ 7% from the last measurement; oral medication use for T2D at least 6 months prior to screening; able to read and understand Japanese; and willing and able to provide electronic consent. Subjects were excluded if they were diagnosed with type 1 diabetes or gestational diabetes; had T2D currently treated with injectables or diet/exercise only; had participated in a previous DCE study for T2D in the past 3 years; or had a cognitive impairment, hearing difficulty, visual impairment, severe psychopathology, or insufficient knowledge of the Japanese language that could interfere with their ability to provide electronic consent and participation. All procedures performed involving human participants were in accordance with the ethical standards of an institutional review board (Ethical and Independent Review Services) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Electronic informed consent was obtained from all individual participants included in the study.
Survey Design
Five treatment attributes were selected for the DCE, including method of administration, HbA1c change, CV risk reduction, weight change, and transient nausea. Two or three levels were selected for each attribute. The development process for the DCE attributes and levels included a targeted review of published T2D patient preference studies, as well as a review of prescribing information of other GLP-1 RAs. Specifically, attribute levels were selected by using published data from Japanese clinical trial results of dulaglutide 0.75 mg and semaglutide 0.50 mg and available global CV outcomes trial data [10, 15, 21], thus reflecting currently available clinical profiles for each product. Results from dulaglutide’s REWIND CV outcomes trial and semaglutide’s SUSTAIN-7 trial were not yet publicly available at the time of this DCE study. A selection of attribute level values approximating dulaglutide 0.75 mg and semaglutide 0.50 mg profiles, based on the outcomes from clinical trials, were chosen to enable a comparison of semaglutide to the most widely used GLP-1 RA in Japan, as well as to directly assess differences in patient preferences between two products that have the same once-weekly dosing frequency. These attributes are consistent with and similar to those included in previous studies of medication preferences among T2D populations [16,17,18,19, 22].
The experimental design for the DCE was constructed with a Bayesian approach that incorporated directional priors, using NGene v1.1. The DCE was made available on a web-based platform. For the DCE, subjects were presented with two hypothetical medications, composed of the five attributes and one level for each attribute. Each subject was asked to choose between the hypothetical medications by indicating which profile was preferable.
The DCE consisted of 24 total choice sets, but was randomized into two blocks to minimize the number of questions each subject viewed and to obtain statistical efficiency. Specifically, for each subject, the DCE task included 12 randomized choice scenarios as well as a repeated question, a dominance question, a direct preference assessment between profiles representing dulaglutide and semaglutide, and a practice question prior to being presented with the first DCE choice scenario (16 total questions) (see Tables S1 and S2 in the Electronic supplementary material, ESM, for examples of DCE choice tasks).
Additional Questionnaires
Prior to participation and to confirm eligibility, subjects completed an online screening questionnaire that included questions on age, gender, current medications, duration of treatment for T2D, and HbA1c level. Immediately following the DCE, a health literacy and numeracy exercise was administered to identify subjects with low health literacy and/or difficulty with understanding basic probability and mathematical concepts. Health literacy was measured via subjective and objective measurements [23, 24]. Following these assessments, sociodemographic and clinical questions were asked in order to describe the sample, including questions about the subject’s education, work experience, household income, height, weight, and T2D-related comorbidities. Finally, two questions were fielded to ask subjects about their willingness to take a product with a profile approximating dulaglutide and a product with a profile approximating semaglutide, using a five-point response scale from “not willing” to “very willing.”
Study Procedures
Prior to initiating the main study data collection, a pilot study was completed among 10 subjects. While completing the DCE via the web-based system, in-person interviews were conducted to gain feedback regarding subject understanding of the DCE task, the comprehension and relevance of the DCE attributes and levels, and to ensure that the web-based platform was operating correctly. For the pilot study only, subjects were asked to bring their medication notebook to the interview or describe their diagnostic process to confirm the diagnosis of T2D. The Japanese medication notebook is created and updated by a pharmacist when the patient fills a prescription and includes all the medication information for the patient.
Generally, subjects understood the attributes and levels and could describe each using their own words. However, some cultural translation suggestions were provided, including revising the wording of terms such as “profile,” “outcome,” and “attribute.” Additionally, all subjects could easily use and complete the DCE using the web-based portal. After the completion of the pilot study interviews, minor changes were made to the DCE attributes and levels in line with pilot study subject feedback, and the methods and DCE survey were finalized (Table 1).
Statistical Analyses
Descriptive statistics were used to characterize the sample and were reported for the screening, sociodemographics, self-reported clinical characteristics, health literacy and numeracy exercise, and medication preference questions. Categorical variables were summarized by frequency statistics, and continuous variables were summarized using medians and interquartile ratios (IQR).
The internal validity of the DCE results for the overall sample was examined to account for survey non-attendance and to ensure that the subjects were trading off the attributes in the DCE. Validity assessments examined the results for the dominance question, repeated question, response choices for the DCE overall (e.g., always choosing alternative A vs. alternative B), time to complete the survey, and respondents always choosing the alternative better on one attribute. The last of these was conducted for attributes with unambiguous level ordering—a priori, it was expected that subjects would indicate preferences for HbA1c improvement, CV risk reduction, and lower risk of nausea.
Internal validity assessment results were analyzed separately for the overall sample and subgroups based on education, health literacy, and numeracy. The final analysis sample was composed of subjects choosing the non-dominated alternative in the dominance choice question, and choosing both alternative A and alternative B at least once.
The results of the DCE were assessed using multinomial logit (MNL) and panel mixed logit (MXL) models. The MNL model was fitted to the final analysis sample as well as separately after stratifying by subgroups defined a priori, including gender, age (< 60; ≥ 60 years), HbA1c (< 8.5%; ≥ 8.5%), and BMI (< 25 kg/m2 and ≥ 25 kg/m2). The MNL model relates to the probability of choice among two or more alternatives to the characteristics of the attribute levels defining those alternatives. The MXL model considers preference heterogeneity by estimating the distribution of preferences across the sample, and was only fitted to the final analysis sample.
Post-estimation analyses included predicted choice probability and maximum acceptable risk (MAR) computation. Specifically, the predicted choice probability was calculated to determine the overall probability that either dulaglutide or semaglutide DCE levels were preferred. An assessment of the MAR of nausea side effects to obtain treatment benefits was conducted using a model with linear-coded nausea and HbA1c attributes in order to assess the subjects’ willingness to accept risk (of nausea in this case) to achieve a certain level of clinical benefit.
Lastly, descriptive statistics (frequency and percentage) were used to analyze the willingness of the subjects to take a product with a profile reflecting dulaglutide 0.75 mg and a product with a profile reflecting semaglutide 0.50 mg.
R statistical software version 3.4.1 (Vienna, Austria) and Stata 15.0 (StataCorp, College Station, TX, USA) were used to conduct the analyses. All statistical tests employed a significance level of p < 0.05.
Results
Sample Characteristics
A total of 472 subjects were screened, and 243 (51%) were found to be eligible to participate in the survey (Fig. 1). Of those deemed ineligible (n = 229), the most common reasons for exclusion were HbA1c below 7.0% (51%) and less than 6 months duration on medication to treat T2D (20%). A total of 190 subjects provided electronic consent and completed the survey.

Subject disposition
Internal validity assessment results were used to construct the final analysis sample of 161 subjects, excluding those who chose the dominated alternative in the dominance question (n = 27) and always selected either alternative A or alternative B (n = 2). Full internal validity assessment results for the overall sample and final analysis sample can be found in Tables S3a and S3b in the ESM.
The demographic and self-reported clinical characteristics of the final analysis sample of 161 subjects are presented in Tables 2 and 3 (sociodemographic results for the full sample are included in Table S4 of the ESM). The median (IQR) age of the subjects was 55 (48, 63) years, with 84% of the sample male. The median (IQR) BMI was 25.9 kg/m2 (23.9, 28.9). The median (IQR) current HbA1c level was 8.3% (7.4%, 9.1%). Most subjects reported taking either one (31%) or two (42%) oral medications to treat their T2D, and most were diagnosed at least 5–10 years (38%) or more than 10 years (37%) prior to participation. The final analysis sample had both high health literacy (92%) and numeracy (99%). Most passed the repeated question validity assessment, and the time needed for survey completion was in most cases greater than three minutes (Table S3b in the ESM).
Patient Preferences
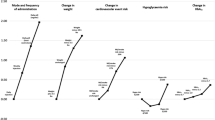
In the final analysis sample (N = 161), the attribute with the largest effect on the subjects’ choices was cardiovascular disease (26% vs. no risk reduction), followed by HbA1c change (− 1.9% vs. − 1.4% change) and avoidance of common side effects (1 out of 19 patients experiencing transient nausea vs. 1 out of 9; Table 4 and Fig. 2). The results reflected preferences in the expected direction for each of these attributes, providing support for the validity of the study. There were significant preferences for the different levels of most attributes (p < 0.001), except the method of administration (p = 0.05). Results from the sensitivity analysis using the overall sample (N = 190) were similar and can be found in Table S5 in the ESM. The results for attribute preferences and ranking were not found to differ significantly in any of the subgroup analyses, showing the robustness of the attribute preference results. There was an observed tendency for subjects with a higher BMI (≥ 25 kg/m2) to place more significance on weight reduction, and subjects with a higher HbA1c (≥ 8.5%) to place more significance on HbA1c change, compared to subjects with a lower BMI (< 25 kg/m2) and a lower HbA1c (< 8.5%), respectively (Figs. S1 and S2 in the ESM; additional subgroup analysis data are available on request).

Multinomial logit regression model results: final analysis sample (N = 161)
Using the MNL results, the predicted choice probability for the dulaglutide 0.75 mg profile was 22%, compared with 78% for the semaglutide 0.50 mg profile. When analyzing the subjects’ direct preferences regarding treatment profiles representing dulaglutide 0.75 mg and semaglutide 0.50 mg, 80% of the sample indicated a preference for the semaglutide 0.50 mg profile over that of dulaglutide 0.75 mg (Fig. 3), which is similar to the predicted choice probabilities. The subgroup analyses did not detect a dependence of this preference for semaglutide over dulaglutide on age (p = 0.25), gender (p = 0.66), HbA1c (p = 0.62), or BMI (p = 0.26). Using the MNL results, the MAR of nausea side effects the subjects were willing to accept was 11.5% to obtain a HbA1c reduction of 1%, 10.5% to obtain a reduction of 26% in the risk of CV disease, 3.9% to obtain a weight loss of − 2.2 kg, and 2.6% to obtain a weight loss of − 1.1 kg (Table 5).

Direct comparison of dulaglutide 0.75 mg vs. semaglutide 0.50 mg: overall analysis sample and analysis by subgroup
Heterogeneity of preferences was explored with a MXL model where HbA1c, common side effects, and weight loss were linear-coded (Table S6 in the ESM). This analysis detected some preference heterogeneity: some patients were willing to accept a very large increase in nausea risk—beyond that presented in the study—to obtain CV risk reduction benefits (Fig. 4). This was also reflected in internal validity assessments, where a considerable share of the patients (27%, Table S3b in the ESM) always chose the treatment alternative that provided a reduction in CV risk. There was considerably less preference heterogeneity for HbA1c and weight loss (Fig. S2 in the ESM).

Distribution of maximum acceptable nausea risk (MAR) to obtain the CV risk reduction benefit (MXL analysis, conditional parameter density estimated with a Gaussian kernel)
Lastly, when asked to indicate willingness to use a product with profiles approximating dulaglutide and semaglutide, most subjects were “very willing” (28%) or “somewhat willing” (39%) to use a product approximating the semaglutide profile, compared with 6% and 34%, respectively, for a product approximating the dulaglutide profile (Fig. 5).

Willingness to initiate treatment with dulaglutide 0.75 mg and semaglutide 0.50 mg
Discussion
Among the attributes relevant to treatment choices between these two most recently approved GLP-1 RAs, dulaglutide 0.75 mg and semaglutide 0.50 mg, the key attribute driving subjects’ medication preferences was the reduction in risk of CV diseases, followed by a reduction in HbA1c, common side effects, and weight reduction. Method of administration (single-use prefilled pen or multi-dose pen) did not significantly affect patient preferences for medication choices. No significant differences were noted in the predefined subgroup analyses.
The findings from this study are notable in light of the results found by Pratley and colleagues [12], who compared dulaglutide to semaglutide in the SUSTAIN-7 trial. The primary endpoint in the trial was change from baseline in percentage HbA1c, and at week 40, semaglutide 0.50 mg was found to be superior to dulaglutide 0.75 mg in mean percentage HbA1c change (semaglutide mean = − 1.5%; dulaglutide mean = − 1.1%; p < 0.0001). In the current study, patient preference for a product for T2D was driven by patient desire for a reduction in CV risk, as well as a reduction in HbA1c, indicating the potential for patients to seek and possibly ask their physician about a medication with a profile similar to semaglutide 0.50 mg. The findings from the direct head-to-head trial were not yet published when attribute levels were developed for this study, so previously published trial results in Japanese T2D patients were used to determine those values. However, the values used in the current study were very similar to the recently published findings from SUSTAIN-7. Based on the results obtained in this study, the publication of the REWIND study—the CVOT analyzing the effect of dulaglutide 1.5 mg—is highly awaited [25]. However, the magnitude of the reduction in CV risk obtained with dulaglutide is still not known, and these outcomes may not be directly transferable to Japanese patients and our study, as the dulaglutide 1.5 mg dose used in the REWIND study is not approved in Japan.
In a previous DCE study among T2D patients in Japan, the most important treatment features of GLP-1 RAs were dosing frequency (with a once-daily preferred over a once-weekly dosing frequency) and the type of delivery system (single-use prefilled pen preferred over a multi-dose pen) [22]. The current study did not include dosing frequency because the dose schedule (i.e., once weekly) is the same for both dulaglutide 0.75 mg and semaglutide 0.50 mg, so dosing frequency is irrelevant when assessing patient preferences for treatment features that differ between the current GLP-1 RAs.
Subjects in this study were willing to accept a much higher increase in the risk of nausea side effects than the risk difference between dulaglutide 0.75 mg and semaglutide 0.50 mg in order to obtain the treatment benefits of semaglutide. These findings are consistent with previous GLP-1 RA DCE studies [18, 22], and further indicate that patients with T2D find high value in a proven CV risk reduction and an improvement in HbA1c levels, and prioritize these benefits over transient nausea side effects. Furthermore, 27% of patients always selected the profile with the greater CV benefit, indicating the importance of this attribute.
Limitations
This study is limited in that there may have been selection bias present; study subjects belonged to a patient panel and self-reported their diagnoses, so they may not be representative of the entire T2D patient population in Japan. A similar limitation of this study was the underrepresented sample size of participants, where only 16% of the analysis sample were females, compared with 84% males. This finding is reflective of the higher prevalence of diabetes in males versus females in Japan. In addition, while DCEs are a common methodology for assessing patient preferences, they may not precisely reflect how patients choose a particular product. However, health literacy and numeracy assessments were completed by all subjects, indicating that 92% and 99% had high health literacy and numeracy, respectively. Furthermore, the predicted choice probabilities (78% and 22%) of treatment profiles approximating semaglutide 0.50 mg and dulaglutide 0.75 mg were very close to the direct choices between their profiles (80% and 20%). These findings suggest that patients were able to understand the DCE choice task and respond appropriately, and that the choice modeling approach was appropriate. Additionally, results from the REWIND trial, which examined CV outcomes of dulaglutide as an add-on therapy to standard-of-care treatment, were not published at the time when the attribute levels were developed for this study or at the time of publication submission, and thus could not be used to generate attribute levels. Lastly, the number of attributes included in the survey was limited to attributes important to patients that were related to method of administration, HbA1c change, side effects, weight change, and CV disease in order to reduce cognitive burden on subjects. However, there may be other aspects of GLP-1 RA treatments that could influence treatment preference but were not investigated in the present study, such as rare adverse events. Additionally, semaglutide is a relatively new treatment and is yet to be price listed in Japan, in contrast to dulaglutide, so the profile of dulaglutide may be more well known to medical doctors in Japan than semaglutide. Further research is needed to understand if these additional treatment features impact patient preference.
Conclusion
In this patient preference study, reduction in CV risk and reduction in HbA1c were the key drivers for the selection of GLP-1 RA medication in Japanese patients with T2D. Due to the increased incidence of CV outcomes among patients with T2D, these findings further confirm the importance of studying CV outcomes among currently available GLP-1 RAs. This result is in line with the 2018 ADA/EASD Consensus Statement for Management of Hyperglycemia in Type 2 Diabetes. Patients were willing to accept an increased risk of transient nausea side effects to obtain these treatment benefits. Overall, 78% of patients were predicted to prefer a product approximating the semaglutide 0.5 mg profile compared to a product approximating the current dulaglutide 0.75 mg profile. Eighty percent (80%) of subjects in this study expressed a direct preference for the semaglutide profile, and this finding remained consistent when assessed across all pre-specified patient subgroups, including age, gender, HbA1c, and BMI. Improved patient preference may be associated with increased adherence and thus improved clinical outcomes.
References
Japanese Ministry of Health, Labour and Welfare. National health and nutrition survey report. 2007. Available from: http://www.mhlw.go.jp/bunya/kenkou/eiyou09/01.html. Accessed 14 Aug 2018.
Haneda M, Noda M, Origasa H, Noto H, Yabe D, Fujita Y, Goto A, Kondo T, Araki E. Japanese clinical practice guidelines for diabetes 2016. J Diabetes Investig. 2018;9(3):657–97.
Matheus AS, Tannus LR, Cobas RA, Palma CC, Negrato CA, Gomes MB. Impact of diabetes on cardiovascular disease: an update. Int J Hypertens. 2013;2013:653789.
Tanaka S, Tanaka S, Iimuro S, Yamashita H, Katayama S, Akanuma Y, et al. Predicting macro- and microvascular complications in type 2 diabetes: the Japan Diabetes Complications Study/the Japanese Elderly Diabetes Intervention Trial risk engine. Diabetes Care. 2013;36(5):1193–9.
The Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358(24):2545–59.
Tanaka N, Kurose T, Seino Y. Therapeutic inertia or individualization? Delay in clinical management of type 2 diabetes mellitus. Curr Med Res Opin. 2016;32(9):1477–8.
Prasad-Reddy L, Isaacs D. A clinical review of GLP-1 receptor agonists: efficacy and safety in diabetes and beyond. Drugs Context. 2015;4:212283.
Japan Diabetes Clinical Data Management Study Group (JDDM). Basic summary data (FY 2017). 2017. Available from: http://jddm.jp/data/index-2017.html#data_09. Accessed 14 Aug 2018.
Pharmaceuticals and Medical Devices Agency (PMDA). List of approved products. New drugs. July 2018. Available from: http://www.pmda.go.jp/english/review-services/reviews/approved-information/drugs/0002.html. Accessed 1 Oct 2018.
Jendle J, Grunberger G, Blevins T, Giorgino F, Hietpas RT, Botros FT. Efficacy and safety of dulaglutide in the treatment of type 2 diabetes: a comprehensive review of the dulaglutide clinical data focusing on the AWARD phase 3 clinical trial program. Diabetes Metab Res Rev. 2016;32(8):776–90.
Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jodar E, Leiter LA, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–44.
Pratley RE, Aroda VR, Lingvay I, Ludemann J, Andreassen C, Navarria A, et al. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol. 2018;6(4):275–86.
Ferdinand KC, Mahata I. Cardiovascular outcome studies with glucagon-like peptide 1 receptor agonists—what will REWIND add? Ann Transl Med. 2017;5(23):476.
Kaku K, Yamada Y, Watada H, Abiko A, Nishida T, Zacho J, et al. Safety and efficacy of once-weekly semaglutide vs additional oral antidiabetic drugs in Japanese people with inadequately controlled type 2 diabetes: a randomized trial. Diabetes Obes Metab. 2018;20(5):1202–12.
Seino Y, Terauchi Y, Osonoi T, Yabe D, Abe N, Nishida T, et al. Safety and efficacy of semaglutide once weekly vs sitagliptin once daily, both as monotherapy in Japanese people with type 2 diabetes. Diabetes Obes Metab. 2018;20(2):378–88.
Gelhorn HL, Poon JL, Davies EW, Paczkowski R, Curtis SE, Boye KS. Evaluating preferences for profiles of GLP-1 receptor agonists among injection-naive type 2 diabetes patients in the UK. Patient Prefer Adherence. 2015;9:1611–22.
Gelhorn HL, Stringer SM, Brooks A, Thompson C, Monz BU, Boye KS, et al. Preferences for medication attributes among patients with type 2 diabetes mellitus in the UK. Diabetes Obes Metab. 2013;15(9):802–9.
Hauber AB, Nguyen H, Posner J, Kalsekar I, Ruggles J. A discrete-choice experiment to quantify patient preferences for frequency of glucagon-like peptide-1 receptor agonist injections in the treatment of type 2 diabetes. Curr Med Res Opin. 2016;32(2):251–62.
Hauber AB, Tunceli K, Yang JC, Gantz I, Brodovicz KG, Alexander CM, et al. A survey of patient preferences for oral antihyperglycemic therapy in patients with type 2 diabetes mellitus. Diabetes Ther. 2015;6(1):75–84.
Polster M, Zanutto E, McDonald S, Conner C, Hammer M. A comparison of preferences for two GLP-1 products—liraglutide and exenatide—for the treatment of type 2 diabetes. J Med Econ. 2010;13(4):655–61.
Miyagawa J, Odawara M, Takamura T, Iwamoto N, Takita Y, Imaoka T. Once-weekly glucagon-like peptide-1 receptor agonist dulaglutide is non-inferior to once-daily liraglutide and superior to placebo in Japanese patients with type 2 diabetes: a 26-week randomized phase III study. Diabetes Obes Metab. 2015;17(10):974–83.
Gelhorn HL, Bacci ED, Poon JL, Boye KS, Suzuki S, Babineaux SM. Evaluating preferences for profiles of glucagon-like peptide-1 receptor agonists among injection-naive type 2 diabetes patients in Japan. Patient Prefer Adherence. 2016;10:1337–48.
Chew LD, Bradley KA, Boyko EJ. Brief questions to identify patients with inadequate health literacy. Fam Med. 2004;36(8):588–94.
Lipkus IM, Samsa G, Rimer BK. General performance on a numeracy scale among highly educated samples. Med Decis Making. 2001;21(1):37–44.
Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P, et al. Design and baseline characteristics of participants in the Researching cardiovascular Events with a Weekly INcretin in Diabetes (REWIND) trial on the cardiovascular effects of dulaglutide. Diabetes Obes Metab. 2018;20(1):42–9.
Acknowledgements
The authors would like to thank the CROèe Inc. team for their work in recruiting subjects and conducting the in-person interviews, as well as the participants in the study.
Funding
Novo Nordisk provided the funding for this study and the article processing charges. Evidera received funding from Novo Nordisk to participate in the study and develop this manuscript. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis.
Editorial Assistance
The authors would like to thank Amara Tiebout at Evidera for her editorial assistance, which was funded by Novo Nordisk.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
Jakob Langer is employed by Novo Nordisk and owns Novo Nordisk stock and/or stock options. Mads Peter Hemmingsen is employed by Novo Nordisk and owns Novo Nordisk stock and/or stock options. Kosei Eguchi is employed by Novo Nordisk. Anne Brooks is employed by Evidera, which provides consulting and other research services to pharmaceutical, medical device, and related organizations. In this salaried position, Anne Brooks works with a variety of companies and organizations, and is precluded from receiving payment or honoraria directly from these organizations for services rendered. Tommi Tervonen is employed by Evidera, which provides consulting and other research services to pharmaceutical, medical device, and related organizations. In this salaried position, Tommi Tervonen works with a variety of companies and organizations, and is precluded from receiving payment or honoraria directly from these organizations for services rendered. Elizabeth Dansie Bacci is employed by Evidera, which provides consulting and other research services to pharmaceutical, medical device, and related organizations. In this salaried position, Elizabeth Dansie Bacci works with a variety of companies and organizations, and is precluded from receiving payment or honoraria directly from these organizations for services rendered.
Compliance with Ethics Guidelines
All procedures performed in studies involving human participants were in accordance with the ethical standards of an institutional review board (Ethical and Independent Review Services) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Electronic informed consent was obtained from all individual participants included in the study.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced Digital Features
To view enhanced digital features for this article go to https://doi.org/10.6084/m9.figshare.7757066.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Brooks, A., Langer, J., Tervonen, T. et al. Patient Preferences for GLP-1 Receptor Agonist Treatment of Type 2 Diabetes Mellitus in Japan: A Discrete Choice Experiment. Diabetes Ther 10, 735–749 (2019). https://doi.org/10.1007/s13300-019-0591-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-019-0591-9