
Abstract
Aim
To develop an evidence-based expert group opinion on the role of insulin motivation to overcome insulin distress during different stages of insulin therapy and to propose a practitioner’s toolkit for insulin motivation in the management of diabetes mellitus (DM).
Background
Insulin distress, an emotional response of the patient to the suggested use of insulin, acts as a major barrier to insulin therapy in the management of DM. Addressing patient-, physician- and drug-related factors is important to overcome insulin distress. Strengthening of communication between physicians and patients with diabetes and enhancing the patients' coping skills are prerequisites to create a sense of comfort with the use of insulin. Insulin motivation is key to achieving targeted goals in diabetes care. A group of endocrinologists came together at an international meeting held in India to develop tool kits that would aid a practitioner in implementing insulin motivation strategies at different stages of the journey through insulin therapy, including pre-initiation, initiation, titration and intensification. During the meeting, emphasis was placed on the challenges and limitations faced by both physicians and patients with diabetes during each stage of the journey through insulinization.
Review Results
After review of evidence and discussions, the expert group provided recommendations on strategies for improved insulin acceptance, empowering behavior change in patients with DM, approaches for motivating patients to initiate and maintain insulin therapy and best practices for insulin motivation at the pre-initiation, initiation, titration and intensification stages of insulin therapy.
Conclusions
In the management of DM, bringing in positive behavioral change by motivating the patient to improve treatment adherence helps overcome insulin distress and achieve treatment goals.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Insulin distress, an emotional response of the patient to the suggested use of insulin, acts as a major barrier to insulin therapy in the management of DM. Addressing patient-, physician- and drug-related factors is important to overcome insulin distress. |
A group of endocrinologists came together at an international meeting held in India to develop a tool kit that would aid a practitioner in implementing insulin motivation strategies at different stages of the patient journey through insulin therapy. |
Bringing in positive behavioral change by motivating the patient to improve treatment adherence helps overcome insulin distress and achieve treatment goals. |
Introduction
Diabetes mellitus is characterized by physiologic insulin resistance and high blood glucose levels and can lead to micro- and macrovascular complications, contributing to significant morbidity and mortality. Insulin therapy is highly effective and could be considered a savior in the treatment of diabetes mellitus and its complications. Despite its efficacy in achieving tight glycemic control, the initiation of insulin therapy is often delayed in patients with type 2 diabetes mellitus (T2DM). This delay is often attributed to psychologic insulin resistance at both the physician and patient levels. The initiation of insulin therapy is often one of the most important decisions that people with diabetes have to make. Because insulin use is associated with several myths, both the decision and treatment path may present as psychologic hurdles, contributing to resistance to treatment [1].
Insulin distress is a major cause of concern in patients with diabetes mellitus as it acts as a roadblock to effective treatment. Several treatment advances in terms of modern insulin analogs, more discrete insulin delivery systems and digital technology have been introduced to reduce insulin distress and improve treatment outcomes. However, the battle is still on and insulin therapy continues to be considered the ‘last resort’ option in the management of diabetes mellitus [2].
At an international meeting, experts from ten countries in the South Asia, Middle East and African regions reviewed the available literature evidence and provided insights based on clinical and research experience in the management of insulin distress. The experts came up with simple and effective solutions to help address insulin distress. Accordingly, the experts categorized the journey of patients’ uptake of insulin into four stages: pre-initiation, initiation, titration and intensification. At each of these stages of insulin therapy, the experts identified unique challenges faced by both physicians and patients, based on their clinical experience. The experts proposed simple solutions to these challenges to allow the patients to embrace the concept of initiating and maintaining insulin therapy to achieve and maintain glycemic control. The key discussion points of the panel were based on scientific evidence and collective clinical judgment from practice. These key discussion points, considered the ‘Practitioner’s Tool Kits,’ were developed for challenges and solutions to insulin therapy at pre-initiation, initiation, titration and intensification stages. This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Insulin Distress: A Barrier to Optimal Insulin Use
Definition
Insulin distress refers to an emotional response of the patient when advised to use insulin. It is characterized by severe apprehension, discomfort, dejection or denial due to a perceived inability to cope with the requirements of insulin therapy. Insulin distress is an entity and a cause of diabetes distress. However, insulin distress is periodic in contrast to diabetes distress, which is present throughout the journey of diabetes [3].
Prevalence of Psychologic Insulin Resistance
Patients diagnosed with diabetes often experience psychologic concerns when insulin therapy is prescribed. Around 25% of the patients with type 2 diabetes mellitus (T2DM) are hesitant to take insulin, seeing it as the ‘last-resort’ option [4]. The prevalence of insulin refusal and rejection is between 20% and 40% among insulin-naïve people with T2DM. Also, adherence to insulin therapy among existing insulin users is suboptimal among one-third of patients with T2DM [5].Timely initiation of insulin therapy reduces the risk of micro- and macrovascular complications. Therefore, the identification of barriers to insulin initiation is important [6].
Patient-Specific Barriers to Insulin Initiation
Patients’ notion and knowledge regarding diabetes and insulin therapy have an impact on the initiation and adherence to insulin therapy. Clinical evidence indicates a high prevalence of refusal of insulin therapy in patients with diabetes. The reasons for psychologic insulin resistance include negative self-perceptions and attitudinal barriers [7]. A survey was conducted from 1-day conferences for people with diabetes at a few centers in North America to identify attitudinal barriers toward insulin therapy. The survey reported that of 3833 patients with diabetes, 708 exhibited a negative attitude toward insulin. The most common reasons for patients to avoid insulin therapy include permanence of therapy (45%), restricted lifestyle (45.2%), life-threatening hypoglycemia (43.3%) and a sense of personal failure and self-efficacy (43.3%) [8].
Healthcare Provider-Specific Barriers to Insulin Initiation
The reasons for delay in insulin initiation from healthcare professionals (HCP) are complex and often overlap with the patient-related barriers. Concerns regarding hypoglycemia, weight gain and adherence are barriers that overlap in both HCP and patient-related groups [6]. In a global survey of 1250 HCPs (600 specialists and 650 primary care physicians) and 1530 insulin-treated patients (180 with type 1 DM and 1350 with type 2 DM), patient and physician beliefs regarding insulin therapy and degree of adherence to insulin regimens were evaluated. The survey was conducted in China, France, Japan, Germany, Spain, Turkey, the UK and USA. Patient were on basal and prandial insulin. The survey reported that 75.5% of the HCPs reported that they would treat patients more aggressively if not for the risk of hypoglycemia. In the survey, 54.5% of HCPs reported that taking insulin at the prescribed time and meal would be difficult and burdensome for patients to adhere to [9]. Another important HCP-specific barrier is patient-HCP interaction and communication in addition to inadequate health literacy. Additionally, studies have documented that patients reported that there are instances when HCPs provided inadequate information regarding the risks and benefits of insulin therapy [6, 10].
Tools for Evaluation of Distress
Problem areas in the diabetes scale (PAID) and diabetes distress scale (DDS) are the two most routinely used tools for evaluation of diabetes distress. DDS is a 17-item scale, and each item is rated on a 6-point Likert scale. A score of 1 for each item indicates ‘no problem,’ whereas a score of 6 indicates ‘a very serious problem’ [8]. DDS measures four critical dimensions of distress that include treatment regimen distress, interpersonal distress, physician distress and emotional burden [11].
Problem areas in diabetes (PAID) is a self-administered 20-item scale. Every item is scored from 0 (‘not a problem’) to 4 (‘serious problem’). The sum of all the item scores multiplied by 1.25 provides the total PAID score, which ranges from 0 to 100. Higher scores indicate greater emotional stress. Furthermore, a score ≥ 40 indicates severe emotional stress [12]. The PAID scale measures emotional distress, such as depressed mood, guilt, anger, worry and fear, in individuals with diabetes [13].
Patient Management Strategies for Improved Insulin Acceptance
The psychologic insulin resistance (PIR) among patients with diabetes can be minimized if healthcare providers explain the possible need for early insulin therapy [14]. Identifying the factors associated with PIR and utilizing intervention strategies to address these factors may aid in timely initiation of insulin therapy at the appropriate time. Patient management strategies for improved insulin acceptance include [14]:
-
Identifying personal obstacles.
-
Overcoming fear of injections.
-
Explaining management of hypoglycemia.
-
Trying to explain to the patient that they have not failed with their diabetes management and try to restore a sense of personal control.
-
Demonstrating the ease of insulin injection and initiation.
The position statement of the American Diabetes Association recommends integrating psychosocial care with collaborative, patient-centered medical care in all people with diabetes, aiming to optimize health outcomes and health-related quality of life. The position statement recommends to routinely monitor people with diabetes for diabetes distress particularly when treatment targets are not achieved and/or at the onset of diabetes complications. According to the position statement, diabetes distress should be assessed at regular intervals using appropriate validated scales; if diabetes distress is identified, the patient should be referred for diabetes education to address areas of diabetes self-care. In patients whose self-care remains impaired after tailored diabetes education, referral to a behavioral health provider for evaluation and treatment is recommended [15].
Behavior Change in Persons with Diabetes: Does It Really Matter?
Management of diabetes is complex and challenging. Although medications and the approach to diabetes management are constantly changing, behavior is one component of diabetes management that remains constant. Behaviors associated with diabetes management among patients include timely administration of medication, calculating the appropriate dose based on available information, talking with others about diabetes, taking supplies and being prepared for unexpected events, and making timely appointments and ordering supplies. Behavioral management of diabetes has a positive impact on health outcomes [16].
The first step for a successful behavioral change in patients with diabetes includes providing information about the desired behavior change. The key considerations for advice on behavior change include [16]:
-
Maintaining clarity in communication: Clearly communicating information on the desired behavior change may eliminate misunderstandings between physicians and patients with diabetes. Strategies to facilitate accurate understanding of recommendations include the following:
-
Simplifying the message: Focusing on a single recommendation at a time and providing a small quantity of information in multiple formats depending on the literacy level of the patient [16].
-
Focusing on a single recommendation at a time with small chunks of information.
-
Providing information in multiple formats (e.g., spoken, written, etc.) and at the literacy level of the individual.
-
Applying the teach-back method: For better comprehension of patients with low health literacy, they may be asked to teach the provider the key information that they have understood [16]. In a direct observation study, which included 38 physicians and 74 patients with diabetes, it was reported that good glycemic control was achieved among patients with diabetes in whom the teach-back method was employed compared with those for whom this method was not used [17].
-
Avoiding ‘one-size-fits–all’ recommendations: Tailoring recommendations according to the patient's characteristics, such as gender, ethnicity, age and resources, help in successful behavior change [16]. Motivational interviewing is one of the clinical approaches that provides health behavior advice in the context of individual beliefs and preferences, with potential applications and benefit in diabetes. In a randomized controlled trial, which included 66 teenagers (14–17 years) with type 1 DM attending a diabetes clinic in South Wales, UK, motivational interviewing facilitated improved behavioral changes in terms of positive well-being and improved quality of life and subsequent improvement in glycemic control [18].
-
Planning proper timing for health behavior message delivery: Diabetes care visits are often scheduled quarterly, making it difficult to provide timely behavioral recommendations. Advising patients to pair the recommended behavior with an existing daily routine (e.g., pairing blood glucose monitoring with brushing teeth in the morning and evening) can help in sustaining the recommended behavior [16, 19].
-
Being empathetic and supportive: Healthcare providers should be compassionate and supportive while communicating about self-management of diabetes. For example, the tone of the healthcare provider while providing recommendations for behavior change should be encouraging instead of discouraging. Shaming, guilt trips and scaring the patients do not help in implementing and sustaining behavior change [16].
Along with the strategies implemented for behavior changes, redesigning the existing care system can help patients with diabetes reach their therapeutic goals. The recommendations for healthcare providers in empowering behavior change in patients with diabetes mellitus include (Table 1) [20]:
Motivational Interviewing in Diabetes Care: Because the Word Still Matters
Four Pillars of Motivational Interviewing (MI)
Motivational interviewing (MI) is an evidence-based intervention to counsel patients about behavioral change. It is a diversified entity consisting of philosophies, principles and techniques gathered from several existing models of psychotherapy and health behavior change theory. The key elements of MI address both ‘what’ and ‘how’ clinicians discuss with patients: Motivational interviewing is built on four pillars: (1) express empathy, (2) roll with resistance, (3) develop discrepancy and (4) support self-efficacy [21].
-
Expressing empathy is a simple and effective tool for communicating respect and empowerment. It involves the clinician asking permission before proceeding with advice or providing information if the patient has not asked for it [21].
-
Rolling with resistance is a type of empathy, where the clinician avoids arguing and tries to understand patients’ reluctance to change [21].
-
Developing discrepancy is another key MI element that is considered critical to the patient’s behavioral change through effective listening. The element ‘developing discrepancy’ depends on the patient’s current behavior, personal goals and values [21].
-
Supporting self-efficacy acknowledges that showing the willingness to change is only half of the behavior change battle. Clinicians should boost the patients' confidence in this regard. They must explain to the patients that one can succeed at health behavior change with persistence [21].
Key Points of Spirit of MI
The key points of the spirit of MI include collaboration, empowering, evocation, caring and nonjudgmental attitude, a patient-centered approach and active listening [13, 14]. Motivational interviewing should be patient-centered and focus on empathy. During MI the physician needs to empower and collaborate with the patient in solving issues and should skillfully use evocative questions to help the patient understand the discrepancies between the current situation and personal goals [21, 22].
Skills and Strategies of Motivational Interviewing: OARS
Motivational interviewing involves the use of skills such as reflective listening and avoiding confrontation or unsolicited advice [13]. A key skill of MI is the ability to explain to the patient in a clear manner. Motivational interviewing comprises strategies, such as open-ended questions, affirmation, reflection and summarization (OARS) (Table 2) [22].
Impact of Motivational Interviewing on Clinical Outcomes in Patients with DM
Clinical evidence indicates that patients with diabetes can benefit from MI, resulting in significant improvement in fasting blood glucose, glycated hemoglobin (HbA1c) level, diabetes self-management and Homeostatic Model Assessment–Insulin Resistance (HOMA–IR) scores [23, 24].
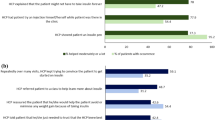
A meta-analysis conducted by Song et al. reported that short-term (< 6 months) MI successfully decreases HbA1c levels in T2DM patients [25]. A study assessed the treatment adherence of patients with T2DM who were on polypharmacy. Also, the effect of counseling on treatment adherence was assessed. The results of the study indicated that a significant proportion of patients with T2DM who were nonadherent to treatment prior to counseling became adherent after proper counseling (Fig. 1) [26].

Final adherence after 1 month of counseling among a group of 116 patients with T2DM who were initially non-adherent to therapy [26]
The number of participants adhering to the recommended physical activity level was significantly increased using motivational interviewing intervention (MII) in a study that involved African American adults with T2DM. The authors reported that 66.7% of the participants adhered to the recommended physical activity levels when counseled using MI as opposed to 38.8% in the non-MI group [odds ratio = 2.92, 95% confidence interval = (1.6, 14.3), p = 0.018]. Furthermore, significantly decreased glucose levels (p = 0.043) and body mass index (p = 0.046) were reported in the MI group compared with usual care (UC). This study supports the use of MI as a tool for improving health outcomes in patients with T2DM [27].
In a meta-analysis by Palacio et al., the impact of MI on medication adherence was evaluated in comparison to a control group. The analysis reported that medication adherence was significantly higher in the MI than the control group (for studies reporting categorical measures: pooled RR: 1.17, p < 0.01; for studies reporting continuous measures: pooled SMD: 0.70, p < 0.01) [28].
The Insulin Conversation
General Challenges in Insulin Therapy in Clinical Practice
-
Delay in Initiation of Insulin Therapy: Delay in initiating insulin therapy has been a major challenge in real-world clinical practice. Many Asian and international studies have shown that even when there was no significant improvement in glycemic control, initialization of insulin therapy was always delayed [29].
-
Insufficient Dose Titration: Timely initiation of insulin therapy is not the only factor that provides optimal glycemic control. Insufficient dose titration, even after timely insulin initiation, may also contribute to inadequate glycemic control. The International Diabetes Federation guidelines recommend a self-titration regimen of initiation of a low-dose insulin (usually 10 U/day) and increasing the start dose by two units every 3 days until the target of < 6.0 mmol/l (< 108 mg/dl) premeal blood glucose has been achieved [29].
-
Uncertainties Regarding Insulin Titration: In routine clinical practice, titration of the insulin dose is determined based on patient characteristics. Based on the physician’s clinical judgment about an individuals’ condition, a decision is made about the titration regimen. In developing countries like Asia, lack of support and inappropriate use of titration algorithms may contribute to dosing errors or insufficient dose titration [29].
-
Adherence and Persistence to Therapy: Adhering to insulin therapy is a key determinant of glycemic control. Poor adherence to insulin therapy is associated with lower glycemic control and complications. Studies indicate that the rate of hospitalizations and mortality is higher in nonadherent patients with T2DM than in adherent patients. Also, significantly higher HbA1c levels were observed in patients with T2DM who missed insulin injections compared with those who never missed a dose [29].
Patient and Physician Barriers
As discussed in the earlier sections, several factors contribute to insulin resistance. They are injection phobia, doubting the clinical benefits of insulin, misconceptions about developing insulin dependence and a notion that insulin is the last option in diabetes management and fear of complexities of using insulin [29].
Clinical inertia is a key physician barrier to initiating insulin therapy. Around 87.6% of physicians report that adequate glycemic control is not observed in many patients with T2DM who are already on insulin therapy. Physician barriers also include concern about hypoglycemia, which limits treatment aggressiveness [29].
Myths Associated with Insulin Therapy
When an insulin therapy is initiated, many patients with T2DM face a complex mix of emotions due to their belief of the myths about insulin therapy. Some of the myths regarding insulin therapy are [30]:
-
Insulin means I am a failure.
-
Insulin does not work.
-
Insulin causes complications or death.
-
Insulin causes weight gain.
-
Insulin injections are painful.
-
Insulin causes hypoglycemia.
-
Insulin is addictive.
-
Insulin is too expensive.
-
Insulin will change my life.
Attitudes among patients with T2DM willing or unwilling to accept insulin therapy include [8]:
-
Can never stop insulin.
-
Patient care not good enough.
-
Not confident about therapy.
-
Lack of fairness.
-
Problematic hypoglycemia.
-
Life will be restricted.
-
My diabetes will be more serious.
-
Insulin causes problems like blindness.
-
Anticipated pain (injections).
Perceptions of insulin therapy among treatment-naïve/experienced patients with T2DM included [31]:
-
Fear of injections.
-
Diabetes worsens.
-
Seen as sick.
-
Weight gain.
-
Less flexibility.
When Should This Conversation Be Initiated?
A conversation about insulin initiation should be started shortly after diagnosis. Timely conversation provides an opportunity to set a positive context for insulin therapy. This helps prevent a sense of guilt or personal failure regarding insulin initiation among patients with T2DM. During the initial conversation, a healthcare provider should emphasize the patient’s lifestyle, habits, concerns about insulin and short- and long-term goals for diabetes management. The right conversation at the right time helps HCPs to convince patients about insulin initiation, which is a key factor in the success of insulin therapy [32].
The Concept of Euthymia
The Greek scholar Democritus defined euthymia as: “One is satisfied with what is present and available, taking little heed of people who are envied and admired and observing the lives of those who suffer and yet endure.” The concept of euthymia is also reflected in positive mental health, psychologic well-being and eustress. Euthymia is a tool and target for diabetes care. It is a state of mental well-being or optimal mood and implies not only a lack of psychiatric illness but also an absence of diabetes distress [33].
Importance of Patient-provider Communication in Diabetes
Patient-provider communication emphasizes achieving diabetes euthymia rather than avoiding diabetes distress. Thus, it is important to apply the biopsychosocial model of health vs. a purely glucocentric or biomedical approach while treating patients with diabetes. In this context, patient-reported outcomes, as well as psychologic measures, need to be assessed as a part of routine diabetes care [33].
Evidence suggests that physician empathy is associated with positive clinical outcomes in patients with T2DM. In a study, the association between physicians’ level of empathy scores and patient outcomes was examined in an outpatient setting (n = 891). The study noted that patients of physicians with high empathy scores were significantly more likely to have good control of HbA1c (56%) than patients of physicians with low empathy scores (40%, p < 0.001). The study concluded that physician empathy could be considered a key factor associated with clinical competence and outcomes [34].
Effective Insulin Initiation: ‘A Good Start for Good Adherence to Insulin’
-
Effective Insulin Conversation
Healthcare providers should have an appropriate conversation with patients regarding insulin initiation shortly after the diagnosis of diabetes. An effective conversation helps patients with T2DM perceive insulin treatment in a positive way. Healthcare providers should focus on open-ended questions to identify the needs of the patient and address any concerns regarding insulin therapy [32].
-
Timely Self-management Education
Timely self-management education can help patients with T2DM set realistic goals and have a feeling of more control over their diabetes and treatment regimens. Effective glycemic control can be achieved when a patient has a clear understanding of the condition. A diabetes educator should be assigned to educate patients with T2DM on insulin use in all the HCP offices. Diabetes educators include registered nurses, dietitians, pharmacists, clinical nurse specialists, physician assistants, social workers and counselors. After the initiation of insulin therapy, the patient should be educated on diet, exercise, self-monitoring of blood glucose, blood glucose targets, appropriate injection technique and site rotation [32].
-
Effective Titration
Insulin titration is critical in helping patients with T2DM reach their glycemic goals. It can be done by a healthcare team or patients themselves depending on their ability, motivation and willingness. Titration algorithms can be individualized by the HCP according to the patient’s needs. The Implementing New Strategies with Insulin Glargine for Hyperglycemia Treatment (INSIGHT) study provides an easy-to-use self-titration algorithm in which the insulin dose is increased by 1 unit/day until the required glycemic target is achieved. This titration can be followed if SMBG is not a concern. A family member or caregiver of the patient should also be educated on using the titration algorithm. Clear instructions should be provided in a written format to the patient as well as the caregiver and the teach-back method should be used to confirm the understanding of the patient/caregiver. Providing hypothetical scenarios can also help a patient practice calculating the insulin dose. A simple insulin regimen should be prescribed if the patient is unwilling to follow a self-titration algorithm [32].
In the randomized, multinational Asian Treat to Target Lantus Study (ATLAS) study, the change in mean glycated hemoglobin (HbA1c) in the patient-led vs. physician-led titration groups in insulin-naïve type 2 diabetes mellitus (n = 555) patients initiated on insulin glargine 10 units per day was assessed. The study indicated that a patient-led titration resulted in a marked reduction in the HbA1c value at 24 weeks compared with physician-led titration (− 1.40% vs. − 1.25%; p = 0.043). The study noted that mean reduction in FBG was greatest in the patient-led group (− 2.85 mmol/l vs. − 2.48 mmol/l; p = 0.001). From the study, it can be concluded that, in Asian patient with uncontrolled type 2 diabetes on two oral glucose-lowering drugs, patient-led insulin glargine (Gla-100) titration could be considered an effective strategy to achieve glycemic goals [35].
In the ATLAS study, findings suggested that severe hypoglycemia occurred in 0.7% of patients and no major difference was observed between the two treatment groups regarding hypoglycemia rates. The study noted more frequent occurrence of nocturnal and symptomatic hypoglycemia in the patient-led arm; between-group risk differences were 9.77% (p = 0.002) and 9.16% (p = 0.022), respectively. Country-wise, the rates of nocturnal and symptomatic hypoglycemia were significantly lower in India (2.7% and 8.0%, respectively) than in other countries of the intent-to-treat population [35].
Following optimum basal insulin titration, options for intensification include addition of mealtime insulin (one to three injections of rapid-acting insulin), changing to twice- and then thrice-daily premixed insulin or addition of a glucagonlike peptide-1 (GLP-1) receptor agonist. The addition of a GLP-1 receptor agonist to basal insulin in patients with T2DM with high HbA1c levels, despite optimum dose titration, is recommended by the ADA/EASD guidelines [36].
Key Behaviors of Healthcare Providers that Motivate Insulin-reluctant Patients with Diabetes to Start Insulin Treatment
A qualitative analysis identified the key behaviors of HCPs that motivated patients with T2DM reluctant to start insulin therapy. The study reported that the most common HCP behaviors that motivated patients with T2DM to overcome insulin resistance included [37]:
-
Making the patient understand that insulin helps in controlling diabetes and associated complications in the future.
-
Establishing trust with the patient.
-
Providing support and being available to discuss any concerns.
-
Demonstrating the insulin injection process.
-
Assuring the patient that the insulin injecting process is easy.
-
Referring the patient to a specialist if warranted.
Best Practices for Insulin Motivation at the Pre-initiation, Initiation, Titration and Intensification Stages
Proposed Toolkits for Practitioners for Insulin Use in DM Patients
The expert group proposed a tool kit for the practitioners to address the queries and key challenges faced by the patients with diabetes at different stages of their journey through insulin therapy. These toolkits are based on the clinical experiences of the experts in their day-to-day practice.
Tool Kit for Pre-initiation of Insulin Therapy

Patient Queries and Recommended Responses

Toolkit for Initiation of Insulin Therapy
Patient education while initiating insulin therapy should be simple and focus on a single topic at a time for better retention. A step-wise approach should be followed for insulin-specific diabetes education, and all patient queries should be answered [23].

Titration and Intensification: Best Practices
-
Titration inertia can be a result of reluctance/inaction or the HCP or patient, or both.
-
Simpler titration algorithms and educational self-management programs for diabetic individuals are essential for optimizing clinical outcomes.
-
Most physicians believe that insulin is the most effective agent for achieving glycemic goals, yet they are reluctant to intensify insulin therapy.
-
Insulin intensification inertia can be addressed by using better insulins with good efficacy and safety profiles and newer medications for type 2 diabetes as well as through patient education and effective communication between HCPs and patients with diabetes.
Toolkit for Titration
In addition to the fear of hypoglycemia and poor self-management, a lack of adequate insulin titration contributes to poor glycemic control among patients with T2DM on insulin [6, 38]. Titration of insulin doses is as important as the initiation of insulin treatment. However, in practice, once insulin has been initiated, an increase in dose is not recommended. Insulin dose irregularities can be due to a missed dose, untimely administration of a dose or reduced doses [39].

Toolkit for Intensification
Following initiation of a basal/bolus insulin regimen, titration of the insulin dose becomes important. Insulin dose adjustments should be made in both mealtime and basal insulin based on blood glucose levels. Home glucose monitoring or HbA1c levels aid in titration of insulin doses. Reduction of the basal insulin dose should be considered following titration of the prandial insulin dose, the evening meal dose in particular [40].

Panel Recommendations for Initiation
-
Patient concerns at this stage still focus on the impact on the quality of life; therefore, the safety and tolerability of insulin must be reinforced at this stage.
-
A few concerns that need to be addressed include the proper injection technique, site rotation and self-monitoring as well as insulin usage during religious fasts.
-
Lack of diabetes educators is a major challenge at this stage.
-
Innovative solutions for delivery of open-channel communication as well as user-friendly insulin delivery devices can help at this stage.
-
Tools that can be used by physicians include starter kits and device usage demonstrations.
Improving Compliance and Adherence
Impact of Empowerment on Medication Adherence and Self-care Behaviors
Empowerment is defined as a process that helps patients gain control over themselves and can influence the quality of life. Empowerment as a treatment approach not only aids in effective self-management but also results in optimal treatment outcomes. Clinical evidence indicates that interventions based on empowerment and self-management result in improved diabetes-related quality of life. Furthermore, patients educated in self-management that emphasized empowerment were more motivated and addressed their own concerns [41].
Hernandez-Tejada et al. evaluated the effect of empowerment on treatment adherence and self-care behaviors in adults with type 2 diabetes from two primary care clinics in the southeastern USA. Data were obtained from 378 subjects with type 2 diabetes. Diabetes empowerment, treatment adherence, knowledge about diabetes and diabetes self-care behaviors were assessed using validated scales. The study results indicated that diabetes empowerment was associated with increased medication adherence, increased knowledge and effective self-care behaviors, including diet, physical activity, blood sugar testing and foot care (Table 3). Emphasizing empowerment and self-efficacy as a part of the treatment process improves the outcomes of diabetes management [41].

Conclusion
Insulin distress is a major hurdle in the treatment of diabetes mellitus. In treating insulin distress, strategies beyond diabetes education should be aimed at and multiple components of behavioral change should be implemented through simple measures of motivation. Positive behavioral changes improve treatment compliance and adherence to insulin therapy. Identifying patients who might need insulin and walking them through various phases of initiation, titration and intensification may help achieve optimal glycemic target outcomes. Additionally, this approach will also go a long way toward mitigating emotional issues associated with insulin therapy.
References
Home P, Riddle M, Cefalu WT, et al. Insulin therapy in people with type 2 diabetes: opportunities and challenges? Diabetes Care. 2014;37(6):1499–508.
Sorli C, Heile M. Identifying and meeting the challenges of insulin therapy in type 2 diabetes. J Multidiscip Healthc. 2014;7:267–82.
Kalra S, Balhara YPS. Insulin distress. US Endocrinol. 2018;14(1):27–9.
Bai X, Liu Z, Li Z, et al. The association between insulin therapy and depression in patients with type 2 diabetes mellitus: a meta-analysis. BMJ Open. 2018;8:e020062. https://doi.org/10.1136/bmjopen-2017-020062.
Luk A. Psychological insulin resistance: scope of the problem. Hong Kong Med J. 2016;22:304–5.
Russell-Jones D, Pouwer F, Khunti K, et al. Identification of barriers to insulin therapy and approaches to overcoming them. Diabetes Obes Metab. 2018;20:488–96.
Brod M, Kongso JH. Psychological insulin resistance: patient beliefs and implications for diabetes management. Qual Life Res. 2009;18:23–32.
Polonsky WH, Fisher L, Guzman S, et al. Psychological insulin resistance in patients with type 2 diabetes. Diabetes Care. 2005;28(10):2543–5.
Peyrot M, Barnett AH, Meneghini LF, Schumm-Draeger PM. Insulin adherence behaviours and barriers in the multinational global attitudes of patients and physicians in insulin therapy study. Diabet Med. 2012;29(5):682–9.
Karter AJ, Parker MM, Subramanian U, et al. Barriers to insulin initiation. Diabetes Care. 2010;33:33–735.
Behavioural Diabetes Institute (BDI). Tools to face the psychological demands of diabetes. https://behavioraldiabetes.org/scales-and-measures/#1448435050704-6e22e4b0-81ec. Accessed 17 Dec 2019.
Venkataraman K, Tan LS, Bautista DC, et al. Psychometric properties of the problem areas in diabetes (PAID) instrument in Singapore. PLoS One. 2015;10(9):e0136759.
Welch GW, Jacobson AM, Polonsky WH. The problem areas in diabetes scale. An evaluation of its clinical utility. Diabetes Care. 1997;20(5):760–6.
Clark M. Psychological insulin resistance: a guide for practice nurses. Diabetes Nurs. 2007;11(2):53–6.
Young-Hyman D, de Groot M, Hill-Briggs F, et al. Psychosocial care for people with diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2016;39(12):2126–40.
Hood H, Hillard M, Piatt G, et al. Effective strategies for encouraging behavior change in people with diabetes. Diabetes Manag (Lond). 2015;5(6):499–510.
Schillinger D, Piette J, Grumbach K, Wang F, Wilson C, Daher C. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163:83–90.
Channon SJ, Huws-Thomas MV, Rollnick S, et al. A multicenter randomized controlled trial of motivational interviewing in teenagers with diabetes. Diabetes Care. 2007;30(6):1390–5 Epub 10 Mar 2007.
Reach G. Role of habit in adherence to medical treatment. Diabet Med. 2005;22(4):415–20.
Marrero DG, Mayer-Davis EJ, Ard J, et al. Twenty-first century behavioral medicine: a context for empowering clinicians and patients with diabetes. Diabetes Care. 2013;36(2):463–70.
Welch G, Rose G, Ernst D. Motivational interviewing and diabetes: what is it, how is it used, and does it work? Diabetes Spectr. 2006;19(1):5–11.
Gabbay RA, Durdock K. Strategies to increase adherence through diabetes technology. J Diabetes Sci Technol. 2010;4(3):661–5.
Racic M, Katic B, Joksimovic BN, et al. Impact of motivational interviewing on treatment outcomes in patients with diabetes type 2: a randomized controlled trial. J Fam Med. 2015;2(1):1–6.
Li M, Li T, Shi BY, et al. Impact of motivational interviewing on the quality of life and its related factors in type 2 diabetes mellitus patients with poor long-term glycemic control. Int J Nurs Sci. 2014;1:250–4.
Song D, Xu T, Sun Q. Effect of motivational interviewing on self management in patients with type 2 diabetes mellitus: a meta-analysis. Int J Nurs Sci. 2014;1:291–7.
Mathew EM. Assessment of medication adherence in type-2 diabetes patients on poly pharmacy and the effect of patient counseling given to them in a multispecialty hospital. J Basic Clin Pharm. 2014;5(1):1–15.
Chlebowy DO, El-Mallakh P, Myers J, et al. Motivational interviewing to improve diabetes outcomes in African Americans adults with diabetes. West J Nurs Res. 2015;37(5):566–80. https://doi.org/10.1177/0193945914530522Epub 14 Apr 2014.
Palacio A, Garay D, Langer B, et al. Motivational interviewing improves medication adherence: a systematic review and meta-analysis. JGIM. 2016;31(8):929–40.
Chan WB, Chen JF, Goh S, et al. Challenges and unmet needs in basal insulin therapy: lessons from the Asian experience. Diabetes Metab Syndr Obes. 2017;10:521–32.
Insulin myths and facts. Patient information. Clin Diabetes. 2007;25(1):39–40.
Snoek FJ, Skovlund SE, Pouwer F. Development and validation of the insulin treatment appraisal scale (ITAS) in patients with type 2 diabetes. Health Qual Life Outcomes. 2007;5:69.
Polonsky WH, Arsenault J, Fisher L, et al. Initiating insulin: How to help people with type 2 diabetes start and continue insulin successfully. Int J ClinPract. 2017. https://doi.org/10.1111/ijcp.12973.
Kalra S, et al. Euthymia in diabetes. Eur Endocrinol. 2018;14(2):18–9.
Hojat M, Louis DZ, Markham FW, et al. Physicians’ empathy and clinical outcomes for diabetic patients. Acad Med. 2011;86(3):359–64.
Garg SK, Admane K, Freemantle N, et al. Patient-led versus physician-led titration of insulin glargine in patients with uncontrolled type 2 diabetes: a randomized multinational atlas study. Endocr Pract. 2015;21:143–57.
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38:140–9.
Stuckley HL, Polonsky W, Fisher L, et al. Key factors for overcoming psychological insulin resistance—an examination of a large international sample through content analysis. Diabetes. 2018. https://doi.org/10.2337/db18-221-OR.
Dalal MR, Kazemi M, Ye F, et al. Hypoglycemia after initiation of basal insulin in patients with type 2 diabetes in the United States: implications for treatment discontinuation and healthcare costs and utilization. Adv Ther. 2017;34(9):2083–92.
Brod M, Rana A, Barnett AH. Adherence patterns in patients with type 2 diabetes on basal insulin analogues: missed, mistimed and reduced doses. Curr Med Res Opin. 2012;28(12):1933–46.
Association The American Diabetes. Standards of medical care in diabetes—2019. Diabetes Care. 2019;42(Suppl. 1):S4–6.
Hernandez-Tejada MA, Campbell JA, Walker RJ, et al. Diabetes empowerment, medication adherence and self-care behaviors in adults with type 2 diabetes. Diabetes Technol Ther. 2012;14(7):630–4.
Pearson TL. A practical review of insulin pen devices. J Diabetes Sci Technol. 2010;4(3):522–31.
Reach G. Can technology improve adherence to long-term therapies? J Diabetes Sci Technol. 2009;3(3):492–9.
Baser O, Tangirala K, Wei W, et al. Real-world outcomes of initiating insulin glargine-based treatment versus premixed analog insulins among US patients with type 2 diabetes failing oral antidiabetic drugs. Clinicoecon Outcomes Res. 2013;5:497–505.
Acknowledgements
Sanofi India helped in the organization and logistic support for this expert forum meeting. The content published herein represents the views and opinions of the various contributing authors and does not necessarily represent the views or opinion of Sanofi and/or its affiliates. The details published here are intended for informational, educational, academic and/or research purposes and are not intended to be a substitute for professional medical advice, diagnosis or treatment.
Funding
This expert opinion initiative has been funded by Sanofi India. The Rapid Service Fee received by the journal was funded by Sanofi India.
Medical Writing and Editorial Assistance
Medical writing and editorial support was provided by Dr. Rajshri Mallabadi and Dr. Kavitha Ganesha from BioQuest Solutions Pvt. Ltd., which was paid for by Sanofi, India.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
Sanjay Kalra is is a member of the journal’s Editorial Board. Sarita Bajaj, Surendra Kumar Sharma, Gagan Priya, Manash P. Baruah, Debmalya Sanyal, Sambit Das, Tirthankar Chaudhury, Kalyan Kumar Gangopadhyay, Ashok Kumar Das, Bipin Sethi, Vageesh Ayyar, Shehla Shaikh, Parag Shah, Sushil Jindal, Vaishali Deshmukh, Joel Dave, Aslam Amod, Ansumali Joshi, Sunil Pokharel, Faruque Pathan, Faria Afsana, Indrajit Prasad, Moosa Murad, Soebagijo Adi Soelistijo, Johanes Purwoto, Zanariah Hussein, Lee Chung Horn, Rakesh Sahay, Noel Somasundaram, Charles Antonypillai, Manilka Sumanathilaka and Uditha Bulugahapitiya have nothing to disclose.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced Digital Features
To view enhanced digital features for this article go to: https://doi.org/10.6084/m9.figshare.11527839.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Kalra, S., Bajaj, S., Sharma, S.K. et al. A Practitioner’s Toolkit for Insulin Motivation in Adults with Type 1 and Type 2 Diabetes Mellitus: Evidence-Based Recommendations from an International Expert Panel. Diabetes Ther 11, 585–606 (2020). https://doi.org/10.1007/s13300-020-00764-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-020-00764-7