
Abstract
Introduction
In this podcast, we present the result of the 2023 scheduled update of the 2019 guidelines of the International Working Group of the Diabetic Foot (IWGDF) addressing the use of systems to classify foot ulcers in people with diabetes in routine clinical practice.
Methods
These guidelines were based on a systematic review of the available literature that identified 28 classifications addressed in 149 articles and, subsequently, expert opinion using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) methodology. We first assessed the value of each system independently and, in the second stage, chose the best one or two to be used in each clinical scenario.
Results
We recommend (1) for communication among healthcare professionals to use the Site, Ischaemia, Neuropathy, Bacterial infection, Area, Depth (SINBAD) classification (first option) or consider using Wound, Ischaemia, foot Infection (WIfI) system (alternative option, when the required equipment and level of expertise are available and it is considered feasible) and in each case the individual variables that compose the systems should be described rather than a total score; (2) for predicting the outcome of an ulcer in a specific individual: no existing system could be recommended; (3) for characterising a person with an infected ulcer: the use of the IDSA (Infection Diseases Society of America)/IWGDF (first option) classification or consider using the WIfI system (alternative option, when the required equipment and level of expertise are available and it is considered as feasible); (4) for characterising a person with peripheral artery disease: consider using the WIfI system as a means to stratify healing likelihood and amputation risk; (5) for the audit of outcome(s) of populations: the use of the SINBAD score.
Conclusion
Although there is no classification that fits all purposes, it is crucial that healthcare professionals standardize the way they characterise diabetes-related foot ulcers and guide their decision-making process by using validated classification systems.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
In 2023, the International Working Group on the Diabetic Foot (IWGDF) updated their previous guidelines published in 2019, including those on how to classify foot ulcers in people with diabetes. |
Adequate characterization of foot ulcer(s) in people with diabetes is crucial for communication between healthcare professionals and with the person affected, choosing and monitoring the efficacy of treatment strategies and auditing health services. |
We recommend the use of SINBAD (Site, Ischaemia, Neuropathy, Bacterial infection, Area, Depth) as the first-line wound classification system for interprofessional communication (describing each composite variable) and clinical audits (using the full score). |
When in the presence of infection, we recommend the use of IDSA (Infection Diseases Society of America)/IWGDF and, when in the presence of peripheral artery disease or when resources exist in addition to an appropriate level of expertise, we recommend the use of WIfI (Wound, Ischaemia, foot Infection). |
Podcast Video (MP4 116607 KB)
Digital Features
The podcast and transcript can be viewed below the abstract of the online version of the manuscript. Alternatively, the podcast can be downloaded here: https://doi.org/10.6084/m9.figshare.24793452.
Podcast Transcript
MMS: Matilde Monteiro-Soares, Portuguese Red Cross Health School Lisbon & Oporto University Faculty of Medicine, Portugal.
FG: Fran Game, University Hospitals of Derby and Burton NHS Foundation Trust, UK.
MMS: Hello, my name is Matilde. I am from Portugal. I am a podiatrist, and I’m also a teacher at the Portuguese Red Cross Health School in Lisbon and also in the Oporto University Faculty of Medicine.
FG: Hi, my name is Fran Game. I’m an endocrinologist. I work in Derby in the UK where I run a multidisciplinary foot clinic, and I’m also the Clinical Director of Research and Development at the Hospital Trust.
Today, Matilde and I are going to be discussing the up-to-date 2023 International Working Group of the Diabetic Foot (IWGDF) update on classifying diabetic foot ulcers [1]. This is an update from the 2019 guidelines but we’ve made a significant number of changes both in the methodology, not necessarily in our recommendations but in the methodology. Actually, one of the things we really struggled with (wasn’t it Matilde?) was people knowing what we meant by classification and what we were actually talking about.
MMS: Yes, one of the major changes that we’ve done was to develop a glossary of terms [2] and also to try to explain what these concepts mean. So, when we are talking about a foot ulcer in a person with diabetes, we will always be referring to a break of the skin of the foot that will involve, as a minimum, the epidermis and part of the dermis in a person with currently or previously diagnosed diabetes. Usually, it should be accompanied by peripheral neuropathy and/or peripheral artery disease in the lower extremity or even other complications.
The other question is "what do we mean by classification?" because we have seen a lot of different types of tools and publications. But when we are discussing this, we are always meaning a tool that has the goal to create more homogeneity between groups of patients, for which similar levels of care should be provided. The idea should be to try to standardize the modifiable factors that a healthcare professional should focus on so that they can improve clinical outcomes. But this does not mean that you need to treat everyone in the same group in exactly the same way and it will not limit the role of clinical expertise. But at least it guides you for the basic things that you should do and at least try to guide your decision-making in a more critical way.
The other thing that we also had a lot of doubt about is the need to understand if the clinical scenarios that we envisioned in 2019 were still valid and yes, we still maintained the same five clinical scenarios. We believe that the main goals of [a] classification are for us to help us communicate between health professionals in the same or different levels, to try to establish an individualized prognosis to guide and assess people with artery disease and/or infection along with their ulcer, but also to allow clinical audit and benchmarking so that you can understand if your clinical care is up to date and if you are doing the best you can do for your patients.
One of the things that we found out is that although we have different scenarios with different purposes, it still will not be possible to have one classification system that would fit all the purposes. So, no classification will save the day such that you can use it everywhere and every time.
FG: So, Matilde, going through this process, we confirmed with our working group members and our external stakeholders that we were going to look at the same five scenarios, and we will discuss what they are a little bit later, but at the outset we said that we changed our methodology. If we use the same five scenarios, what did we change in terms of our methodology?
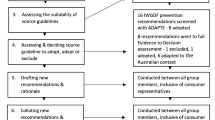
MMS: We started by using a really more thorough GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) methodology [3]. GRADE is a way of doing and grading recommendations, to try to develop them and evaluate them in a more standardized way, and so for that we have a really more complex process involved in doing this.
So, we started by defining key clinical questions to define what should be the important outcomes and for this we have used not only health professionals but also patient representatives. We conducted a systematic review [4] instead of just a critical review, which was what we have done in 2019, and for that reason, we assessed 28 different classifications and included 149 studies that developed or validated these classifications. So, this also brought a lot of complexity because this is not an intervention question. So, in this case, it’s more like diagnostic and prognostic so it was really complicated to have a standardized methodology. And so we decided to first assess the value of each system independently, so to see if they were just developed, or if they were validated, and what were the measures involved in them.
And then, in the second stage, from these 28 different classifications, we tried to choose the best one or two that could be used in each clinical scenario. And this is also a change because in the previous round, we had one classification for each scenario, but now we have decided that to better mimic clinical practice and the different settings, [so] that we could have an alternative classification for each one of the scenarios. That is why we added two recommendations—one for the communication scenario and the other for the characterization of a person that has an infected ulcer. In this case, WIfI (Wound, Ischaemia, foot Infection) was recommended as the alternative system for both of these scenarios. So the question is, how can we sum this up? How can we translate to the audience what were the recommendations that we made, Fran?
FG: Yes, I mean having gone through that rather complex process and finding the five clinical scenarios that we previously used, and had been considered important by the working group members and our stakeholders, we then, having been through that methodology, looked at which classification systems best fitted those scenarios.
We started off by saying that the SINBAD (Site, Ischaemia, Neuropathy, Bacterial infection, Area, Depth) classification should be used as the first-line wound classification in people with diabetes and a foot ulcer where we’re looking for interprofessional communication, but it requires that each consisting variable should be described completely, not just a total score. This SINBAD classification, which is a very simple, 6-point scale, should also be used for clinical audit and benchmarking. However, we recognize that for people with foot ulcers that are infected, when communicating with other healthcare professionals, a little bit more detail about the severity of that infection might be important, and so we included for people with infected foot ulcers the use of the IDSA (Infectious Diseases Society of America)/IWGDF classification for wound infection.
Again, when we looked at people with peripheral artery disease, where there are resources and where there are vascular surgeons available to see those people, those vascular surgeons may need a little bit more detail, and so we suggested, in addition, to use the WIfI classification.
So the SINBAD system was considered the bare minimum for most scenarios in audit and healthcare professional communication, because it’s very easy to use and it’s quite complete. It has the 6 points, the site, ischaemia, neuropathy, bacterial infection, area and depth either 0 or 1, so it’s a very easy to use scoring system and it’s being used in the National Diabetes Foot Audit of England and Wales, so it’s very easy to use in clinical practice. However, this doesn’t derive management, and certainly, in management, we should always look at tackling ischaemia and infection first, and so taking those variables into account, along with the site and presence of neuropathy, we then move to different techniques of management.
As I say, we recognize that in many healthcare settings and with more professionals, more complex assessments are required. But we know as a global organization, that it’s not feasible or accessible in many parts of the world and so simple systems that can be done by the bedside with no specialist equipment are also available. As Matilde has also said, no single classification will ever be sufficient for healthcare professionals in every clinical context and scenario, but this bare minimum information is useful to standardize audits and guide clinical care.
However, Matilde, as we went through this process, we noticed a low level of evidence and we really do need some of these classifications to be better studied and validated, or even for someone to refine existing classifications. But one of the scenarios we struggled with was the prognosis of an individual ulcer or a person in front of us. So what do you think we can do in the future about supporting this clinical scenario?
MMS: Yeah, as you said Fran, we really need further studies validating the existing classifications. [Not as much] for the other four scenarios because we already have an idea of what works. But for individual prognostication, this is the tricky one, because if you need something to be more individualized then you will need more detail and more inclusion of different variables. This is where I think that new technologies and the use of machine learning techniques will be the future. We have seen already some classifications using these systems although still in a very early stage. We also acknowledge that this may be difficult to use in some specific scenarios, but in those where you can have really easy access to health records, then you should use that information to learn and to better have this individualized estimation of prognostication using these techniques. So I believe this will be the future and the only way to answer these clinical scenarios. So at the moment, please read our 2023 guidelines, but I believe that in 2027, we will have some news about this clinical scenario, because we are seeing the rise of artificial intelligence and the way that we can improve the prognostication for a specific individual.
FG: Thank you. Matilde, it’s been a pleasure chatting to you about this subject.
MMS: Always a pleasure to chat with you about this, Fran. See you in 2027 and until then please go and read our recommendations that are currently used. Thank you.
FG: Thank you.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
References
Monteiro-Soares M, Hamilton EJ, Russell DA, et al. Guidelines on the classification of foot ulcers in people with diabetes (IWGDF 2023 update). Diabetes Metabol Res Rev. 2023:e3648.
van Netten JJ, Bus SA, Apelqvist J, et al. Definitions and criteria for diabetes-related foot disease (IWGDF 2023 update). Diabetes Metabol Res Rev. 2023:e3654.
Moberg J, Oxman AD, Rosenbaum S, et al. The GRADE Evidence to Decision (EtD) framework for health system and public health decisions. Health Res Policy Syst. 2018;16:1–5.
Monteiro-Soares M, Hamilton EJ, Russell DA, et al. Classification of foot ulcers in people with diabetes: a systematic review. Diabetes Metab Res Rev. 2023:e3645.
Funding
No funding was received for the creation or publication of this podcast.
Author information
Authors and Affiliations
Contributions
Matilde Monteiro-Soares conceived the manuscript, Fran Game revised the manuscript.
Corresponding authors
Ethics declarations
Conflict of Interest
Both authors have been involved in the development, validation and reviews of classification systems of foot ulcers in people with diabetes.
Ethical Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Monteiro-Soares, M., Game, F. Podcast on How to Classify Foot Ulcers in People with Diabetes (2023 Update of the IWGDF Guidelines on Classification). Diabetes Ther (2024). https://doi.org/10.1007/s13300-023-01521-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s13300-023-01521-2