
Abstract
Mosaicism for unbalanced chromosomal rearrangements segmental mosaicism (SM) is rare, both in patients referred for cytogenetic testing and in prenatal diagnoses. In contrast, in preimplantation embryos SM is a frequent finding and, therefore, is even more challenging. However, there is no consistency among results of published studies on the clinical outcomes of embryos with SM, primarily due to the small number of reported cases. Moreover, there is the problem of predicting the potential for the optimal development of a mosaic embryo to a healthy individual. Therefore, we suggested comparing factors predisposing to favorable and poor prognoses, identified in postnatal and prenatal cohorts of SM carriers, with those obtained from studies on preimplantation embryos. We analyzed 580 published cases of SM including (i) postnatally diagnosed affected carriers, (ii) clinically asymptomatic carriers, (iii) prenatally diagnosed carriers, and (iv) miscarriages. We observed a concordance with preimplantation diagnoses regarding the clinical significance of the extent of mosaicism as well as a predominance of deletions over other types of rearrangements. However, there is no concordance regarding excessive involvement of chromosomes 1, 5, and 9 in unbalanced rearrangements and a preferential involvement of larger chromosomes compared to short ones. Paternal age was not found to be associated with SM in postnatally disease-defined individuals. We have identified maternal age and preferential involvement of chromosome 18 in rearrangements associated with clinical manifestations. Male predominance was found among normal pregnancy outcomes and among disease-defined carriers of rearrangements resulting in a gain of genomic material. Female predominance was found among abnormal pregnancy outcomes, among disease-defined carriers of loss and gain/loss rearrangements, and among transmitting carriers of gonadal SM, both affected and asymptomatic. According to data obtained from “post-embryo” studies, clinical manifestations of chromosomal imbalance are associated with a high proportion of abnormal cells, female gender, the type of rearrangement and involved chromosome(s), and maternal age. We believe these data are instructive in the challenging medical genetic counseling of parents faced with no option other than transfer of an embryo with segmental mosaicism.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Mosaicism is the presence of more than one genetically distinct cell line in a single organism that originates from a genetically homogenous zygote. Until recently, mosaicism for chromosomal rearrangement (Rea), i.e., segmental SM, was considered extremely rare both in patients referred for cytogenetic testing and in prenatal diagnoses, and therefore its epidemiology had not been studied. Prior to recent publications (Kovaleva and Cotter 2016, 2017a, b), the basic characteristics such as population frequency, cytogenetic profiles, and sex ratio (SR, male-to-female ratio) in various groups of carriers were not identified.
Segmental mosaicism appears to be more frequent than previously thought. For example, a normal cell line was detected in 6–20% of patients with microscopically determined disease-causing deletions (Niebuhr 1978; Cassidy et al. 1984; Munier et al. 1989; Robinson et al. 2008; Kotzot et al. 2005; Shinawi et al. 2010) and in 10% of patients with a ring chromosome (Guilherme et al. 2013). The application of molecular technologies resulted in the detection of more carriers of segmental mosaicism.
Mosaicism is particularly frequent (up to 30% of the cases) in preimplantation embryos (Munné and Wells 2017). Until recently, mosaic embryos had not been considered for transfer. Greco et al. (2020) were the first to demonstrate that mosaic embryos may have the potential for giving birth to healthy offspring. Among mosaic embryos, one-third of the mosaic cases were segmental mosaics (Liu et al. 2017; Nakhuda et al. 2018; Coll et al. 2020). There is no consistency among results of published studies on the clinical outcomes of segmental mosaicism regarding their capacity to implant and develop to a fetus (Liu et al. 2017; Fragouli et al. 2017; Victor et al. 2019). In addition, there is the problem of predicting the potential for the optimal development of a mosaic embryo to a healthy individual, without physical and mental disorders.
Kahraman and colleagues (Kahraman et al. 2020) stated: “The transfer of mosaic embryos marks a new era in ART and future studies and reports of cases are needed to help guide clinicians to make safe decisions regarding mosaic embryos. PGT-A is widely used for a number of indications and with the introduction of Next Generation Sequencing (NGS) and increased identification of mosaicism, clinicians require more informative data to guide them to make safe decisions when considering transfer of mosaic embryos… Patient counseling regarding mosaic embryo transfer is extremely important. Additional reports and data including postpartum karyotype analysis of the newborns are necessary to provide conclusive decisions.”
Munné and Wells (2017) suggested that the types of mosaicism observed during preimplantation development and those that affect the fetus and the newborn might represent different phenomena. They declared that “This is probably one of the most important questions remaining to be answered.” We suggested that it might be reasonable and helpful to compare factors predisposing to favorable and poor prognoses, identified in postnatal and prenatal cohorts of SM carriers, with those obtained from studies on preimplantation embryos.
The aim of this study was to determine the risk factors for clinical manifestation of chromosomal imbalance based on previously obtained and additional data on the SM carriers. The objectives were to compare types of rearrangement, the proportion of abnormal cells, involvement of specific chromosomes in rearrangements, sex ratio, and parental ages in groups of postnatally disease-diagnosed carriers and clinically asymptomatic carriers, as well as in the group of prenatally diagnosed carriers, stratified by the outcome of pregnancy. The data obtained were intended to be compared with the published results of studies carried out on mosaic embryos.
Methods
The material for the study was published cases of mosaicism on microscopically detectable autosomal non-centromeric Reas with the presence of a normal cell line, diagnosed by conventional cytogenetics with a resolution of up to 850 bands and/or molecular cytogenetics. Overall, more than one thousand publications had been scanned and 434 articles were selected for the analysis. The cases were identified from various sources including PubMed. The following cases were excluded from the analysis: unknown sex of the carrier; Reas in which both breakpoints are localized in the pericentromeric region (since females predominate among the carriers of such Reas [19, 20] and inherited chromosome instability. Cases of SM with reproductive disorders were extracted only from cytogenetic surveys of couples; reports on exclusively male or female contingents were not considered.
A total of 580 SM carriers were evaluated, including 272 disease-defined carriers of somatic SM and 16 affected carriers of generalized (somatic and gonadal SM), 75 clinically asymptomatic carriers of somatic and/or gonadal SM with offspring with a chromosomal abnormality, 9 carriers identified by chance; 46 clinically asymptomatic carriers of somatic SM with reproductive disorders presumably due to gonadal mosaicism; 130 prenatally diagnosed carriers; 32 cases of fetal deaths. According to Barber (2005), individuals were considered phenotypically affected when any type of phenotypic anomaly was reported even if the etiological role of the chromosome abnormality in the same individual is questionable. The studied variables were those readily available prior to and upon genetic testing, i.e., parental ages, indication for the testing, results of the testing, outcome of the tested pregnancy, and gender of SM carriers. All the cases, along with the data on their chromosome constitution, patient’s age at testing/ascertainment, parental ages at the birth/diagnosis of the proband, the proportion of abnormal cell line(s), and indication for testing are tabulated in Supplemental information files S1–S19. References for files S1–S19 are listed in the S20 file. Rearrangements were classified as a loss, gain, and loss/gain of genomic material. Deletion represented the “loss,” duplication, and additional material was categorized as “gain,” derivative chromosomes, isodicentrics, complex rearrangements, and cases with two abnormal cell lines, one of which with deletion, another one with duplication, were classified as “loss/gain.” In some instances, derivatives and other rearrangements were considered apparent or suggestive “gain” or “loss.” Statistical analysis was performed using programs LePAC (https://eris62.eu/ErisLePAC.html) for estimation of 95% confidence intervals (CI) for proportions and/or their ratios, Fisher’s exact test p-value calculator, 2 × 2 and 2 × 3 (https://www.cog-genomics.org/software/stats) for estimation of the mid-p-values for the Fisher’s exact tests, and StatXact (https://www.cytel.com/software/statxact) for the homogeneity of contingency tables RxC.
Results and discussion
Cytogenetic profile of segmental mosaicism
Unbalanced rearrangements
The results of the comparison of the distribution of various types of unbalanced Reas in studied groups of SM are shown in Table 1. The most common type of Rea in all studied groups, except fetal deaths, was the “deletion.” The proportion of deletions in asymptomatic carriers appeared to be the highest (31 46 62%) among compared groups while the contribution of “unbalanced translocation” was the least common (3 9 22%). Overall, the difference between affected carriers and asymptomatic carriers is not statistically significant. Interestingly, the category “other chromosome rearrangements” is prevalent in fetal deaths (16 38 64%) but the difference between asymptomatic carriers and fetal deaths is not statistically significant, probably due to the small sample size of the last group.
Detailed analysis of cytogenetic profiles in asymptomatic carriers (Table 2) shows a difference between transmitting carriers and those with reproductive disorders in the rate of unbalanced translocations, 7 16 27% (7 out of 48) versus 0.2 5 22% (0 out of 14), correspondingly, however again, the samples are too small.
Balanced rearrangements
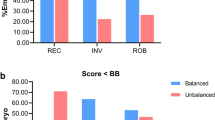
In disease-defined patients with somatic SM, carriers of balanced Reas were found, though relatively rare, in 6% (14 of 237 patients). This can be due to various reasons, including chance coincidence, microstructural abnormalities in the rearranged chromosome(s) involved (De Gregori et al. 2007), position effect (Zepeda-Mendoza et al. 2017), or undetected cell line with an unbalanced derivative (Raimondi et al. 1983; Dufke et al. 2003). Among 16 affected patients with generalized (somatic and gonadal) mosaicism, individuals with balanced Reas were not found. Among both fetal deaths and in prenatal diagnoses, there were similar proportions of balanced Rea carriers: 25% (8 out of 32) and 26% (34/130). A remarkable difference was found among asymptomatic carriers, an apparent predominance of balanced Reas over unbalanced Reas in patients with reproductive disorders: 55 73 86% (22 out of 30) with repeated miscarriage and 38 62 82%), (10 out of 16) with infertility (statistically nonsignificant, mid-p = 0.41), while in transmitting carriers of gonadal mosaicism, the proportion of these Reas was twofold lower: 26 37 48% (27 out of 74) the difference is statistically significant, mid-p = 7•10−4. At this stage of our research on the Rea types distributions, we conclude that the main difference between the studied groups is the contribution of balanced Rea, but not unbalanced Rea.
The overwhelming majority of balanced Reas were reciprocal translocations, with a low proportion of inversions. Among asymptomatic carriers of gonadal mosaicism and individuals with reproductive disorders, carriers of inversions accounted for 11% (3 out of 27) and 16% (5 out of 32), respectively, while in disease-defined patients − 21% (3 out of 14), and in prenatal diagnoses − 24% (8 out of 34). Among miscarriages, carriers of inversion were not found.
Involvement of single chromosomes in rearrangements
Data on the involvement of single chromosomes according to types of Rea, in disease-defined carriers and in asymptomatic carriers are summarized in Tables 3 and 4.
The analysis showed that the compared groups differ statistically significantly in this indicator. In disease-defined patients, chromosome 18 is affected significantly more likely (14%) in comparison to other chromosomes. In addition, there is a difference in the involvement of chromosomes in various types of Reas. For example, chromosome 18, being the most frequent among both deleted chromosomes and ring chromosomes (13 and 11 cases, respectively), was found to have few duplications (1 case) and no involvement in balanced translocations. In contrast, chromosome 1 is more frequently found to be duplicated than deleted (6 cases vs. 1). Chromosome 21 appeared to be the least affected, with only 4 of 246 instances (1.5%).
In asymptomatic carriers, the distribution is statistically significantly different from that in carriers with clinical manifestations, at p = 0.003. Chromosomes most frequently involved in unbalanced Reas are chromosome 5 (11%), chromosome 13, chromosome 21, and chromosome 22 (10% each).
Rearrangements in chromosome 3, chromosome 7, and chromosome 9 are the most rarely detected (0% each). The rate of involvement of chromosome 18 (4.2%) does not differ from the expected figure of 4.5%. In prenatal diagnoses (Table 5), the distribution of involved chromosomes is more homogenous, with an apparent prevalence of chromosome 18 (13%).
Such analysis is of potential significance for the evaluation of the fitness of mosaic preimplantation embryos. It might be possible that rearrangements of certain chromosomes (for example, deletion of chromosome 18) are not tolerated by the embryo while others, being involved in segmental mosaicism (for example, chromosomes 5 and 21), might have good prospects. Again, we would like to stress that more cases should be collected for such a study.
When comparing the data of our study to the spectrum of chromosomal abnormalities with those obtained from preimplantation diagnostics (Coll et al. 2020), in both, it is noted that the most common chromosomal abnormality was deletion. However, we did not find exceptionally high involvement of chromosomes 1, 5, and 9, in contrast to the data presented by Coll et al. (2020).
Moreover, our data on the frequency of involvement in chromosome rearrangements as a function of their length contradicts the findings of Munné and Wells (2017) and Coll et al. (2020). They reported the predominant involvement of large chromosomes in mosaic unbalanced rearrangements in preimplantation embryos. According to our data (Table 6), large chromosomes are not more likely than short chromosomes to be involved in unbalanced Reas, in both disease-defined patients (6 11 20 vs. 7 13 25) and in asymptomatic carriers (1.3 2.4 4.8 vs. 4 9 23), as well as in prenatal diagnoses (2.2 4.0 7.7 vs. 2.8 5.2 11). Conversely, large chromosomes tend to be involved in balanced Reas more often than short ones, both in disease-defined carriers (0.7 1.5 31 vs. 0.2 0.6 1.6) and in asymptomatic carriers (2.8 6.5 12 vs. 2.2 4.2 8.6), as well as in prenatal diagnoses (2.0 3.7 7.1 vs. 0.6 1.3 2.9).
Besides, some increase in the involvement of chromosomes 1, 9, and 5 in balanced Rea was observed in the group of asymptomatic carriers. However, it is reasonable to suggest that mosaicism for balanced Reas was not a matter of concern in preimplantation diagnostics; moreover, it is not readily identified by molecular technologies.
Extent of mosaicism for unbalanced rearrangement
The proportion of cells with Reas, in addition to the number of cells studied, was not specified in all published cases; therefore, only individuals with a high (≥ 50%) frequency of cells with Reas were analyzed. In the disease-defined cohort, such individuals were found more often than among asymptomatic carriers: 43 47 50% (119 of 235) versus 16 23 30% (8 of 52); the difference is highly statistically significant since confidential intervals are not overlapped. In affected carriers of gonadal mosaicism, a high proportion of cells with an unbalanced Rea was detected even more frequently, in 35 59 80% (9 out of 15).
In prenatal diagnoses, the proportion of amniocytes with unbalanced Rea was reported in 66 cases. A high frequency of abnormal cells was found in 20 out of 39 (42 53 64%) fetuses with an unfavorable pregnancy outcome and in 7 out of 27 (18 27 26%) fetuses with a normal pregnancy outcome. Interestingly, the majority of affected carriers of balanced Rea (11 out of 13) showed low levels of mosaicism.
We believe that these data are in good accordance with reported results (Spinella et al. 2018; Viotti et al. 2020): mosaic embryos with an aneuploidy rate of < 50% had more favorable clinical outcomes than those containing > 50% aneuploidy. However, other authors reported that the degree of trophectoderm mosaicism was a poor prediction of ongoing pregnancy and miscarriage (Kushnir et al. 2018; Victor et al. 2019; Viotti et al. 2020). Moreover, Popovic et al. (2020) claimed to estimate the precise degree and prevalence of mosaicism based on a single biopsy to be conceptually unachievable.
Sex ratio among carriers of segmental mosaicism
Data on SR in studied cohorts, according to two general categories, as carriers of unbalanced Rea and carriers of balanced Rea are presented in Table 7. It is evident that in almost all groups, there is a female predominance among carriers of unbalanced Rea, unlike the slight male prevalence among carriers of balanced Rea, both prenatally diagnosed and postnatally disease-defined, as well as among carriers with reproduction disorders. Unlike this general trend, miscarriages and transmitting carriers of balanced rearrangement demonstrate apparent female predominance.
Data from the more detailed analysis of SR among carriers with clinical abnormalities according to the specific types of Rea are presented in Table 8. A notable predominance of female individuals was already stated in Table 7. This shift appears to be mainly due to the contribution of Reas that cause the loss of chromosomal material; in this collective group including deletions, apparently deleted rings, etc., 47♀/85♀ were found, the SR is 0.39 0.55 0.79. Also, a deficit of males is observed among carriers of Reas with gain/loss of chromosomal material: 15♂/21♀ (SR = 0.37 0.72 1.4). But for Reas characterized by a gain of chromosomal material, some predominance of males is noticeable: 46♂/36♀, SR = 0.8 1.3 2.0. Among the carriers of balanced Reas (including ring chromosomes without deletions), there are slightly more males: 21♂/17♀, SR = 0.7 1.2 2.3. Among fetuses with unbalanced Rea, there are slightly more female carriers: 45♂/ 51♀, SR = 0.6 0.9 1.3. Overall, carriers of unbalanced Rea (referred for genetic testing as a result of special indications including the abnormal US) are characterized by poor pregnancy outcomes (Table 8). A favorable pregnancy outcome was more often observed in male carriers: 21♂/11♀, SR = 0.9 1.9 3.9. Among unfavorable outcomes, female carriers predominated: 20 males/29 females, SR = 0.4 0.7 1.2, the difference is statistically significant at mid-p = 0.032. Proportions of abnormal outcome are practically evenly distributed over various Rea types (Table 9), which might be explained by small sample sizes.
It is interesting to note that in prenatal diagnoses, as well as in other studied cohorts (except miscarriages), male patients predominated among the carriers of inversions. Among 7 prenatally diagnosed carriers of inversion, 6 were males. Overall, the SR among inversion carriers was 1.0 2.8 7.4 (14♂/5♀). Carriers of balanced Rea diagnosed prenatally are usually born normal. Of the 29 fetuses with reported outcomes, only four (2♂/2♀) were born with anomalies. In this group, as well as among postnatally diagnosed carriers, with or without clinical manifestations, there is a typical predominance of males: 19♂/15♀.
Analysis of data from cytogenetic surveys of fetal deaths revealed a female prevalence among carriers of unbalanced SM: 8♂/18♀ in cases where the likelihood of contamination with maternal cells was either excluded or being very small, and 8♂/24♀ in the total sample.
While sex ratio in the general population is considered paramount genetic, medical, and social essence, the association of SR deviations with chromosome abnormalities is still apparently underappreciated. Previous studies demonstrated SR may be considered an effective tool for recognition and examination of pathologic processes, and risks prediction. For example, the predominance of the females, found among carriers of rearrangements with breakpoints in the pericentromeric regions, was explained by sex-specific instability of pericentromeric regions as the earliest manifestation of sexual dimorphism (Kovaleva and Shaffer 2003). SR-based studies suggested low-level mosaicism for a normal cell line in homologous Robertsonian translocation carriers which would alter their reproductive options (Kovaleva 2007), indicated that gender affects clinical suspicion of Down syndrome (Kovaleva 2011), and suggested an impact of paternal rearrangement on maternal chromosomes’ segregation after fertilization (Kovaleva 2013)]. Recently, the predominance of female individuals among newborn carriers of non homologous Robertsonian translocations was discovered, which was explained by the mechanism of sex-specific correction of the initial trisomy. Uniparental disomy resulting from trisomy correction was female-biased too (Kovaleva 2017). Therefore, we opted to apply the examination of SR as a useful tool when studying the epidemiology of segmental mosaicism, though the unusual sex ratios among carriers of SM due to noncentromeric breakpoints were not readily predictable.
What can explain the excess of female individuals among carriers of unbalanced SM, which is especially pronounced in asymptomatic carriers? At least three mechanisms can be considered: sex-specific (inherent in female embryos) genomic instability, intrauterine selection of male carriers, or sex-specific (inherent in male embryos) elimination of abnormal cells.
Poszygotic instability of the female genome as an explanation for the shift in the sex ratio presupposes the prevalence of female individuals also among carriers of balanced rearrangements. However, in almost all studied groups, among the carriers of balanced rearrangements, males predominated, and the sex ratio is close to the population value. The high intrauterine mortality of male fetuses can also be excluded from consideration since, among fetal deaths with segmental mosaicism, a clear predominance of female abortions was observed.
The results of our previous and present studies suggest sex-specific elimination of chromosomal abnormalities. It was reported that early female embryos develop somewhat more slowly than male embryos (Pergament et al. 1994; Alfarawati et al. 2011), possibly due to the process of X chromosome inactivation, which occurs at the stage of ≤ 10 cells (Pergament et al. 1994). More active proliferation of male cells can facilitate the efficient elimination of the abnormal cell line. It can be assumed that the age of the mother influences the rate of elimination of abnormal cells. The discovered phenomenon deserves further study, including a comparative analysis with the age of the parents of carriers of asymptomatic mosaicism. Unfortunately, such data are practically absent in the literature. Studies of the parental origin of rearranged chromosomes would be of considerable theoretical interest.
Sex ratio in asymptomatic carriers suggested that the prognosis for male carriers of segmental mosaicism for normal development and reproductive health is more favorable than for female carriers. This assumption is supported by data on the sex ratio among fetuses with a normal pregnancy outcome. However, it should be borne in mind that the male cells, apparently, are tolerant to an excess of chromosomal material, and such an anomaly as duplication may “go unnoticed.”
Parental ages of segmental mosaicism carriers
Maternal age was known for 147 disease-defined patients and paternal age for 120 patients. It is noteworthy that the maternal age of female carriers of almost all types of Reas appeared to be higher than in mothers of male carriers. Overall, the mean maternal age of 83 female carriers was 27 29 29 years and of 64 male carriers 24 25 27 years. The proportion of women of 35 years and older is 12 21 32% and 3 7 15%, correspondingly. The difference between distributions is statistically significant at p < 0.0092.
At the same time, no difference in the paternal age depending on the sex of the abnormal offspring was found: in both male and female groups, the paternal average age was similar, 29.7 and 30 years, correspondingly. The sex ratio displays an apparent tendency to decrease with the increase of maternal age from 3.2 in the group < 20 years to 0.2 in the group aged 40 years and older (Table 10), with an exact p-value for the trend of 2.10−4. No such trend was found when analyzing SR according to paternal ages.
There is no consensus in the literature regarding parental age as a factor influencing embryo segmental mosaicism. Some indicate that advanced maternal age was not seen to be correlated with a higher prevalence of mosaicism (Munné and Wells 2017; Nakhuda et al. 2018). Other reports observed a significant maternal age effect on the success of mosaic embryos (Victor et al. 2019; Greco et al. 2020), while Coll et al. (2020), found that a positive association with mosaicism showed only paternal age. Our data demonstrate meaningful differences in the maternal age distributions between disease-defined males and females, while paternal ages did not differ. This data cannot be compared with that obtained from studies on pre-implantation embryos, since these reports persist in ignoring such important genetic parameters as gender. This, unfortunately, is typical for research on prenatal diagnostics and fetal death. We would propose the desirability of consensus protocols for the presentation of survey data submitted to publication, including information about gender, parental ages, and reproductive history.
Conclusions
Our study showed that the type of rearrangement, the chromosomes involved, the frequency of abnormal cells, the gender of the carrier, and the maternal age may be factors influencing the clinical manifestation of chromosomal imbalance. The introduction of molecular methods for the diagnosis of chromosomal abnormalities will inevitably cause an increase in the number of diagnosed cases of segmental mosaicism and, accordingly, the number of challenges in genetic counseling. Consequently, the general goal of future studies should be not just an increase in the amount of knowledge useful for medical and genetic counseling of families of carriers of segmental mosaicism, but the development of algorithms for optimization of the prognosis. This requires representative samples of carriers of segmental mosaicism, together with the registration of all known significant/potentially significant variables. Therefore, we emphasize the need to publish every single detected case of segment mosaicism and invite colleagues to join the international consortium “Segmental mosaicism: determination of factors affecting the clinical manifestation of chromosomal imbalance” (see Research Gate).
Availability of data and materials
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
References
Alfarawati S, Fragouli E, Colls P et al (2011) The relationship between blastocyst morphology, chromosomal abnormality, and embryo gender. Fertil Steril 95:520–524. https://doi.org/10.1016/j.fertnstert.2010.04.003
Barber JCK (2005) Directly transmitted unbalanced chromosome abnormalities and euchromatic variants. J Med Genet 42:609–629. https://doi.org/10.1136/jmg.2004.026955
Cassidy SB, Thuline HC, Holm VA (1984) Deletion of chromosome 15 (q11–13) in a Prader-Labhart-Willi syndrome clinic population. Am J Med Genet 17:485–495. https://doi.org/10.1002/ajmg.1320170211
Coll L, Parriego M, Mateo S, García-Monclús S, Rodríguez I, Boada M, Coroleu B, Polyzos NP, Vidal F, Veiga A (2020) Prevalence, types and possible factors influencing mosaicism in IVF blastocysts: results from a single setting. Reprod Biomed OnlineS1472–6483(20)30530–7. https://doi.org/10.1016/j.rbmo.2020.09.025
De Gregori M, Ciccone R, Magini P, Pramparo T et al (2007) (Cryptic deletions are a common finding in “balanced” reciprocal and complex chromosome rearrangements: a study of 59 patients. J Med Genet 44(12):750–762. https://doi.org/10.1136/jmg.2007.052787
Dufke A, Leipoldt M, Enders H (2003) Chromosomal mosaicism in familial reciprocal translocation carriers: necessity of karyotyping different tissues. Am J Med Genet 121A(3):292. https://doi.org/10.1002/ajmg.a.20288
Fragouli E, Alfarawati S, Spath K, Babariya D, Tarozzi N, Borini A, Wells D (2017) Analysis of implantation and ongoing pregnancy rates following the transfer of mosaic diploid-aneuploid blastocysts. Hum Genet 136(7):805–819. https://doi.org/10.1007/s00439-017-1797-4
Greco E, Litwicka K, Minasi MG, Cursio E, Greco PF, Barillari P (2020) Preimplantation genetic testing: where we are today. Int J Mol Sci 21(12):4381. https://doi.org/10.3390/ijms21124381
Guilherme R, Klein E, Hamid A, Bhatt S, Volleth M, Polityko A, Kulpanovich A, Dufke A, Albrecht B, Morlot S, Brecevic L, Petersen MB, Manolakos E, Kosyakova N, Liehr T (2013) Human ring chromosomes - new insights for their clinical significance. Balkan J Med Genet 16:13–20. https://doi.org/10.2478/bjmg-2013-0013
Kahraman S, Cetinkaya M, Yuksel B, Yesil M, Cetinkaya CP (2020) The birth of a baby with mosaicism resulting from a known mosaic embryo transfer: a case report. Hum Reprod 35(3):727733. https://doi.org/10.1093/humrep/dez309
Kotzot D, Haberlandt E, Fauth C, Baumgartner S, Scholl-Bürgi S, Utermann G (2005) Del(18)(q12.2q21.1) caused by a paternal sister chromatid rearrangement in a developmentally delayed girl. Am J Med Genet 135A(3):304–307. https://doi.org/10.1002/ajmg.a.30727
Kovaleva NV (2007) Nonmosaic balanced homologous translocations: some may be mosaic. Am J Med Genet 143A:2843–2850. https://doi.org/10.1002/ajmg.a.31745
Kovaleva NV (2013) Increased risk of trisomy 21 among the offspring of the carriers of balanced autosomal rearrangements not involving chromosome 21, is not associated with interchromosomal effect. Russ J Genet 49(2):259–268. https://doi.org/10.7868/S0016675812110045
Kovaleva NV (2017) An overlooked phenomenon: female-biased sex ratio among carriers of Robertsonian translocations detected in consecutive newborn studies. Russ J Genet 53(12):1444–1452. https://doi.org/10.7868/S0016675817120062
Kovaleva NV, Cotter PD (2017a) Mosaicism for structural non-centromeric autosomal rearrangements in disease-defined carriers: sex differences in the rearrangements profile and maternal age distributions. Mol Cytogenet 10:18. https://doi.org/10.1186/s13039-017-0321-9
Kovaleva NV, Cotter PD (2017b) Mosaicism for structural non-centromeric autosomal rearrangement in prenatal diagnoses: evidence for sex-specific selection against chromosomal abnormalities. Mol Cytogenet 10:45. https://doi.org/10.1186/s13039-017-0346-0
Kovaleva NV, Shaffer LG (2003) Under-ascertainment of mosaic carriers of balanced homologous acrocentric translocations and isochromosomes. Am J Med Genet 121A(2):180–187. https://doi.org/10.1002/ajmg.a.20156
Kovaleva NV, Cotter PD (2016) Somatic/gonadal mosaicism for structural autosomal rearrangements: female predominance among carriers of gonadal mosaicism for unbalanced rearrangements. Mol Cytogenet 8. https://doi.org/10.1186/s13039-015-0211-y
Kovaleva NV (2011) Gender affects clinical suspicion of Down syndrome. In: Prenatal diagnosis and screening for Down syndrome. Chapter 13, Subrata Dey (ed) InTech, Vienne, p. 203–216. ISBN: 978–953–307–355–2. Available from: http://www.intechopen.com/articles/show/title/gender-affects-clinical-suspicion-of-down-syndrome30
Kushnir VA, Darmon SK, Barad DH, Gleicher N (2018) Degree of mosaicism in trophectoderm does not predict pregnancy potential: a corrected analysis of pregnancy outcomes following transfer of mosaic embryos. Reprod Biol Endocrinol 16(1):6. https://doi.org/10.1186/s12958-018-0322-5
Liu E, Tarozzi N, Borini A, Becker A, Zhang J, Maxwell S, Grifo J, Babariya D, Wells D, Fragouli E (2017) Detailed investigation into the cytogenetic constitution and pregnancy outcome of replacing mosaic blastocysts detected with the use of high-resolution next-generation sequencing. Fertil Steril 108.https://doi.org/10.1016/j.fertnstert.2017.05.002
Munier F, Pescia G, Jotterand-Bellomo M, Balmer A, Gailloud C, Thonney F (1989) Constitutional karyotype in retinoblastoma. Case report and review of literature. Ophthalmic Paediatr Genet 10:129–150. https://doi.org/10.3109/13816818909088353
Munné S, Wells D (2017) Detection of mosaicism at blastocyst stage with the use of high-resolution next-generation sequencing. Fertil Steril 107(5):1085–1091. https://doi.org/10.1016/j.fertnstert.2017.03.024
Nakhuda G, Jing C, Butler R, Guimond C, Hitkari J, Taylor E, Tallon N, Yuzpe A (2018) Frequencies of chromosome-specific mosaicisms in trophoectoderm biopsies detected by next-generation sequencing. Fertil Steril 109(5):857–865. https://doi.org/10.1016/j.fertnstert.2018.01.011
Niebuhr E (1978) Cytologic observations in 35 individuals with a 5p- karyotype. Hum Genet 42:143–156. https://doi.org/10.1007/BF00283634
Pergament E, Fiddler M, Cho N et al (1994) Sexual differentiation and preimplantation cell growth. Hum Reprod 9(9):1730–1732. https://doi.org/10.1093/oxfordjournals.humrep.a138783
Popovic M, Dhaenens L, Boel A, Menten B, Heindryckx B (2020) Chromosomal mosaicism in human blastocysts: the ultimate diagnostic dilemma. Hum Reprod Update 26(3):313–334. https://doi.org/10.1093/humupd/dmz050
Raimondi SC, Luthard FW, Summitt RL, Martens PR (1983) High-resolution chromosome analysis of phenotypically abnormal patients with apparently balanced structural rearrangements. Hum Genet 63(4):310–314. https://doi.org/10.1007/BF00274751
Robinson DO, Howarth RJ, Williamson KA, van Heyningen V, Beal SJ, Crolla JA (2008) Genetic analysis of chromosome 11p13 and the PAX6 gene in a series of 125 cases referred with aniridia. Am J Med Genet 146A:558–569. https://doi.org/10.1002/ajmg.a.32209
Shinawi M, Liu P, Kang S (2010) Recurrent reciprocal 16p11.2 rearrangements associated with global developmental delay, behavioural problems, dysmorphism, epilepsy, and abnormal head size. J Med Genet 47:332–341. https://doi.org/10.1136/jmg.2009.073015
Spinella F, Fiorentino F, Biricik A, Bono S, Ruberti A, Cotroneo E, Baldi M, Cursio E, Minasi MG, Greco E (2018) Extent of chromosomal mosaicism influences the clinical outcome of in vitro fertilization treatments. Fertil Steril 109(1):77–83. https://doi.org/10.1016/j.fertnstert.2017.09.025
Victor AR, Tyndall JC, Brake AJ, Lepkowsky LT, Murphy AE, Griffin DK, McCoy RC, Barnes FL, Zouves CG, Viotti M (2019) One hundred mosaic embryos transferred prospectively in a single clinic: exploring when and why they result in healthy pregnancies. Fertil Steril 111(2):280–293. https://doi.org/10.1016/j.fertnstert.2018.10.019
Viotti M, Victor A, Barnes F, Zouves C, Besser AG, Grifo JA, Cheng E-H, Lee M-S, Lin P-Y, Corti L, Fiorentino F, Spinella F, Minasi MG, Greco E, Munne S (2020) New insights from one thousand mosaic embryo transfers: features of mosaicism dictating rates of implantation, spontaneous abortion, and neonate health. Fertil Steril 114(suppl 3):e1–e2
Zepeda-Mendoza CJ, Ibn-Salem J, Kammin T et al (2017) Computational prediction of position effects of apparently balanced human chromosomal rearrangements. Am J Hum Genet 101(2):206–217. https://doi.org/10.1016/j.ajhg.2017.06.011
Acknowledgements
We wish to thank Dr. Nikita N. Khromov-Borisov (R.R.Vreden Russian Research Institute of Traumatology and Orthopedics) for statistical analysis of the data.
Author information
Authors and Affiliations
Contributions
N.V.K. and P.D.C. performed the literature search, analyzed the data, and wrote the manuscript. The authors alone are responsible for the content and writing of the paper. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Communicated by: Michal Witt
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kovaleva, N.V., Cotter, P.D. Factors affecting clinical manifestation of chromosomal imbalance in carriers of segmental autosomal mosaicism: differential impact of gender. J Appl Genetics 63, 281–291 (2022). https://doi.org/10.1007/s13353-021-00673-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13353-021-00673-w