
Abstract
Introduction
The risk of herpes zoster (HZ) increases with age. In countries with an ageing population such as Mexico, a rise in the risk of HZ and complications is expected. The goal of this study was to provide an updated estimate of the potential burden of HZ and associated complications in Mexico.
Methods
A retrospective database study was performed using data from the national surveillance database of the Ministry of Health (Secretaría de Salubridad y Asistencia/Dirección General de Información en Salud). HZ cases and associated complications were identified via the International Classification of Diseases 10th Revision codes. Emergency room (ER) visits, hospitalizations, and deaths were extracted and analyzed by age group and year. The observation period was between 2011 and 2020 for ER visits and hospitalizations and between 2011 and 2019 for deaths. Cumulative incidence per 1000 people and case fatality rate were estimated.
Results
During the observation period, 53,030 ER visits, 4172 hospitalizations, and 263 deaths due to HZ were reported nationwide. The cumulative incidence of HZ based on ER visits was 1.04 per 1000 people aged ≥ 50 years but increased in older age groups (1.47 per 1000 people aged ≥ 65 years). The most common complications were neuralgia (10.9%), ocular disease (7.0%), meningoencephalitis (2.9%), and disseminated disease (3.1%). Patients ≥ 65 years accounted for 37% of hospitalizations and 81% of deaths.
Conclusion
In Mexico, HZ and its complications impose a considerable burden on the population and the healthcare system. Prospective surveillance studies are required to obtain an accurate picture of the current epidemiology of HZ in Mexico and to estimate the benefits of future vaccination strategies against HZ.
Plain Language Summary
Herpes zoster (HZ), also called shingles, is a disease typically characterized by a painful skin rash. It affects mostly older adults and immunocompromised populations. Approximately 30% of patients have complications such as prolonged, severe pain; eye disease; or disease affecting parts of the body other than the skin. In this study, we analyzed national passive surveillance data for HZ disease and related complications in Mexico. Over the last 10 years (2011–2020), more than 50,000 cases and 4000 hospitalizations have been observed. In those, 263 people died, and most of the deaths (81%) occurred in people aged 65 years or older. Since the proportion of older people in the Mexican population will increase over the next decades, herpes zoster will probably become more frequent and complicated. Vaccination against HZ could help protect the older population against this serious disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Updated estimates of the real burden of disease of herpes zoster (HZ) in Mexico are limited. |
This retrospective analysis of national surveillance data in Mexico showed that older adults bear the highest burden of HZ disease with patients aged ≥ 65 years accounting for 37% of hospitalizations and 81% of deaths. |
Available data indicate region-variable reporting of HZ. |
Considering HZ underreporting, prospective surveillance studies are needed to provide accurate estimates of HZ incidence in Mexico. |
Introduction
Primary infection with varicella zoster virus (VZV) causes chickenpox and affects more than 90% of the population during childhood or adolescence [1]. In tropical climates, a larger proportion of individuals may contract chickenpox later in life, i.e., early adulthood. In Mexico, the seroprevalence of VZV was 85.8% in 2010 in people aged 1–95 years, based on data from a cross-sectional study representative of the entire population [2].
Herpes zoster (HZ) arises when latent VZV reactivates from neurons in the trigeminal and dorsal root ganglia. In the absence of endogenous or exogenous boosting, VZV-specific cell-based immunity wanes with age to a point where T cell-mediated immunity is insufficient to control VZV latency [3, 4]. Consequently, the risk of HZ increases as a function of age with approximately 68% of HZ cases occurring after the age of 50 years [5, 6]. Reported annual HZ incidence values range between 2.9 and 19.5 cases per 1000 people with a clear age-related gradient [7]. In a recent systematic literature review including Latin American and Caribbean countries, the cumulative incidence ranged between 3.2 and 34.2 cases per 1000 people [8]. In this review, in line with other reports, an increase in the incidence of HZ was observed after the age of 50 years. These findings emphasize the impending rise in HZ incidence and HZ-related healthcare resource use (HCRU) due to an ever-ageing population [9].
From a pathophysiological perspective, VZV replicates in neuronal cells upon reactivation, before traveling anterograde along the neuroaxis to the skin area that is innervated by the corresponding ganglion [10]. Inflammation in the affected dermatome leads to blistering and the development of a typical unilateral, painful rash. However, development of skin lesions is often preceded by prodromal pain, itching, headache, and sometimes fever, which may lead to wrong or delayed diagnosis [11, 12]. While the rash itself heals within 2–4 weeks, several complications may occur that inflate the burden of disease as well as direct and indirect costs [13, 14]. The most frequently reported HZ-related complication occurring in approximately 20% of people is post-herpetic neuralgia (PHN), defined as pain persisting beyond 3 months after the onset of rash [13, 15]. Other complications include bacterial superinfection, ophthalmologic involvement with severe sequelae that may lead to vision loss, neurological complications such as meningoencephalitis and stroke, and disseminated zoster with more than one dermatome affected or visceral disease including hepatitis, arthritis, or myocarditis [10,11,12,13, 16]. The risk of HZ-related complications increases with age with up to 35% of patients aged > 65 years reporting complications [13].
Demographic projections of the Mexican population predict an increase in the median age from 28 years in 2015 to 44 years in 2055. By 2055, a third of the population will be > 60 years old [17]. This age shift may lead to an increase in HZ incidence and associated HCRU. To understand the impact of changing HZ epidemiology on HCRU and associated costs in Mexico, an accurate estimate of HZ disease trends is needed. Few studies have reported HZ incidence and HZ-related health impact. In a retrospective study, Vazquez et al. analyzed data from national surveillance and health system databases [18]. Between 2000 and 2013, the number of patients with HZ identified on the basis of hospitalization discharge records was 7042; among these patients, most were aged > 65 years. Complications such as ocular involvement, meningoencephalitis, and disseminated HZ were reported in 7%, 5.4%, and 2.8% of patients, respectively. In addition, 11% of patients were treated for HZ-related neuralgia, and 5.4% had other complications [18]. More recent epidemiological data for HZ in Mexico would be valuable to estimate trends in HZ disease burden and to assess the potential benefit of future preventive strategies.
The objective of this study was to provide a updated picture of HZ disease epidemiology and to describe the trends in the burden of disease and associated complications of HZ in Mexico.
Methods
This was a retrospective observational database study covering the time period between 2011 and 2020. Since number of deaths for the year 2020 were not yet published at the time of the analysis, only deaths between 2011 and 2019 were included in this study.
Data Sources
Information regarding HZ-related emergency room (ER) visits, hospitalizations, and deaths was retrieved from the national surveillance database of the Ministry of Health (Secretaría de Salubridad y Asistencia/Dirección General de Información en Salud) accessed through the cubos dinámicos (dynamic cubes) [19]. This database covers all the public health system institutions (including the social security institute), which represents around 90% of all the health system in Mexico.
Dynamic cubes store data according to type of information (e.g., births, deaths, hospitalizations), supplemented by demographic and clinical data. ER data (outpatient cases), hospitalizations, and clinically confirmed deaths due to HZ were identified using International Classification of Diseases 10th Revision (ICD-10) codes (Table 1). Patients with HZ who had a primary diagnosis for death other than HZ were not captured by this methodology.
Demographic data were obtained from the National Institute for Statistics, Geography and Informatics and the National Population Council (Instituto Nacional de Estadística, Geografía e Informática/Consejo Nacional de Población) [20].
Statistical Considerations
Descriptive statistical analyses were used to describe HZ burden by year, sex, clinical diagnosis, state, and age group.
Cumulative incidence (CI) per 1000 people was calculated according to the following equation:
For CI, the time interval refers to the total study period from 2011 to 2020. The denominator is the average yearly population (of each respective age group) from 2011 to 2020. We averaged the population for the total study period in order to adjust population trends to calculate the cumulative incidence for the 9-year period (and age-stratified).
Case fatality rate (CFR) was calculated according to the following equation:
For CFR, both hospitalized cases and ambulatory cases were considered in the denominator because some inpatient cases are not linked to the outpatient cases. Average length of stay was estimated on the basis of aggregated data of the number of hospitalizations and total length of stay in patients aged ≥ 15 years. Duration of inpatient stay for children and adolescents < 15 years was not available. Since aggregated data were associated with ICD-10 codes, the average length of stay by HZ-related complication category was calculated. Data by sex for ER visits were not accessible, but a sex-stratified analysis was carried out for ambulatory cases in the age groups ≥ 15–64 years and ≥ 65 years.
Compliance with Ethics Guidelines
This noninterventional, retrospective study was based on anonymized data extracted from public sources. According to national regulations, this study did not require informed consent nor approval by ethics committee.
Results
HZ Ambulatory Cases and Incidence
During the observation period, there were 53,030 ER visits, 4172 hospitalizations, and 263 deaths associated with HZ. HZ incidence was similar for age groups between 1 and 49 years. There was a marked increase in incidence in the 50–54 age group with approximately half of all ER visits reported in people aged ≥ 50 years; however, the reported HZ incidence decreased again in age groups ≥ 75 years (Fig. 1). During the observation period (2011–2020), the cumulative incidence rate was 1.04, 1.47, and 1.91 cases per 1000 people in adults aged ≥ 50 years, ≥ 65 years, and ≥ 80 years, respectively. Incidence rates per year per age group are shown in Supplementary Material (SI) Fig. 1.

Number of HZ cases by age group and by year. HZ herpes zoster, y years. Patients for whom age was not available were not included in this figure (n = 47)
Reported HZ cases varied across regions with the highest reports registered for Mexico State (5274 HZ cases), Guanajuato (4804 HZ cases), and Veracruz (4120 cases) (Fig. 2).

HZ cases by region (2011–2020). HZ herpes zoster. Map adapted from https://d-maps.com/pays.php?num_pay=288&lang=en with permission
Overall, there were more ambulatory cases registered for female patients than male patients with an overall sex ratio of 1.2 (SI Fig. 2A). Up to the year 2016, this trend was even more pronounced, with a female to male sex ratio ranging between 1.5 and 1.6 in people aged ≥ 15–64 years and between 1.2 and 1.3 in people aged ≥ 65 years (SI Fig. 2B). Thereafter, the sex ratio was inverted with more male patients receiving ambulatory treatment for HZ (SI Fig. 2B).
Most ambulatory cases (88.7%) were for HZ without complications (SI Fig. 3), and the remaining diagnoses were ocular or eye disease (2.7%), neuralgia (1.8%), disseminated disease (1.4%), and 1.2% cases that developed PHN.
Hospitalizations and HZ-related Complications
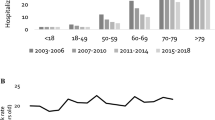
Among the 4172 HZ-related hospitalizations reported, most occurred either in children and adolescents or in people aged ≥ 55 years (Fig. 3). In terms of hospitalizations, 59% occurred in adults aged ≥ 50 years and 37% in adults aged ≥ 65 years.

Number of HZ-related hospitalizations by age group and by year. HZ herpes zoster, y years
Most hospitalizations (65.9%) were for HZ without complications (Fig. 4a). The most frequently reported HZ-related complications were neuralgia (10.9%), eye disease (7.0%), meningoencephalitis (2.9%), and disseminated disease (3.1%). The length of inpatient stays in patients aged ≥ 15 years varied between 3.2 and 13 days and the longest stays were observed for HZ-related encephalitis (13 days), followed by disseminated HZ (6.4 days) and ophthalmologic HZ (5.6 days) (SI Table 1).

Distribution of diagnosis for a HZ-related hospitalizations (2011–2020) and b deaths (2011–2019). The nomenclature of complications corresponds to ICD-10 codes. HZ herpes zoster, ICD-10 International Classification of Diseases 10th Revision
Deaths
Of the 263 deaths due to HZ observed between 2011 and 2019, 81% occurred in people aged ≥ 65 years and most deaths (82.1%) were not associated with any complication. Zoster with other nervous system involvement accounted for 7.2% of deaths, while ocular HZ, zoster encephalitis, and zoster meningitis were reported for 3.0%, 1.9%, and 0.4% of deaths (Fig. 4b).
The number of deaths per year ranged between 20 in 2017 and 2018 and 48 in 2012 without a visible trend over the years (SI Fig. 4). The estimated case fatality rate was 0.46%.
Discussion
In this retrospective database study, the number of patients hospitalized for HZ was 4172 and 263 died from HZ during the observation period; 37% of hospitalizations and 81% of deaths occurred in adults aged ≥ 65 years.
The increase in the burden of HZ in older age groups reflects the well-known epidemiology of HZ, which is characterized by a sudden increase of HZ incidence in adults aged ≥ 50 years [6, 7, 11]. This increase can mostly be explained by the age-related waning of cell-based immunity [21]. Up to 2016, HZ-related ambulatory cases were more common in female patients than male patients, especially in the younger age group (≥ 15–64 years). Previous studies have identified gender as an independent risk factor of HZ, with women being at higher risk of developing HZ [22]. After 2017, we observed an inversion of the sex ratio with more male patients seeking ambulatory care compared with female patients. There is no explanation for this sudden change; active surveillance studies might be useful to investigate the impact of gender on the risk of HZ in the Mexican population.
The incidence rates and nature of complications observed in the present study are in agreement with a previous healthcare database study conducted in Mexico, covering the time period between 2000 and 2013 [18]. The main complications reported in this previous study included neuralgia in 11% of patients, eye involvement in 7%, meningoencephalitis in 5.4%, and disseminated disease in 2.8% of patients. In the present study, the most frequently reported HZ-related complications in hospitalized patients were neuralgia (10.9%) and ophthalmologic disease (7.0%). Meningitis and encephalitis due to zoster occurred in 1.0% and 1.9% of patients, respectively, and disseminated disease was reported in 3.1% of patients. This suggests that the burden of disease remained relatively stable during the last two decades in Mexico. In a prospective, multicenter cohort study in Mexico, Ortiz-Covarrubias evaluated the impact of HZ on quality of life in adults aged > 50 years at different timepoints during 6 months from the onset of rash [23]. After an initial decrease in pain (median EQ-visual analogue scale score 63.8, corresponding to moderate pain), pain increased progressively, reaching greater than 80 (severe pain) at day 21. Pain interfered with activities of daily living and could lead to anxiety and depression. Indeed, HZ has been identified as an independent risk factor for developing major depression [24]. In a pooled analysis of three prospective cohort studies conducted in Brazil, Argentina, and Mexico including 383 patients, PHN was reported in 38.6% of patients, but the risk of PHN increased with increasing age [25]. Direct and indirect costs were significantly higher in patients with PHN compared with those without (direct costs $1227.67 vs $421.52 for patients with/without PHN; indirect costs $773.46 vs $446.20 for patients with/without PHN). These data suggest that PHN, the most common complication of HZ, may become more frequent as the proportion of older people grows, further adding to the burden of HZ on the healthcare system.
In Mexico, HZ is a non-notifiable disease, meaning that reporting will depend on institutional practice and local requirements. This could lead to underreporting and regional variations. Indeed, reported HZ frequency varied significantly between regions, which supports the hypothesis of underreporting. Regional variations in reported HZ incidence were also noted in the previously published healthcare database study conducted by Vazquez et al. [18], with lowest HZ numbers reported for the states of Aguascalientes, Baja California Sur, Colima, Morelos, Nayarit, Querétaro, Quintana Roo, and Tlaxcala. In the present study, the lowest HZ reported cases were observed for Querétaro, Baja California Sur, Yucatan, and Coahuila. Because of the risk of non-uniform reporting of HZ cases, comparison of HZ incidence rates per region may be misleading. Indeed, in the present study, the calculated HZ cumulative incidence for adults aged ≥ 50 years was considerably lower compared with cumulative incidence reported in other countries and regions (0.74–1.91 cases per 1000 people vs 2.9–19.5 cases per 1000 people [7]). Besides uncertainty due to potential underreporting, other factors may influence the observed HZ incidence rate: in the present study, only HZ-related outpatient and inpatient ER visits were considered if they were coded as primary diagnosis. A secondary diagnosis of HZ or related complications would not be captured directly by the surveillance system; thus, patients with comorbidities that developed HZ were not entirely quantified. HZ episodes that prompt people to visit their general practitioner (GP), either in the private or public setting, would not be captured by this methodology. In the pooled analysis of three prospective studies conducted in Brazil, Argentina, and Mexico, 79.1% of patients visited a GP, 48.8% went to the ER, and 5.7% of patients were hospitalized [25]. Based on these data, HZ incidence relying on ER records only could miss approximately 50% of HZ cases. Even though healthcare-seeking behavior may differ between countries, observations in other regions of the world confirm that omission of HZ-related GP visits may lead to underestimation of HZ incidence rates. In a retrospective study in Italy analyzing hospitalization discharge records, a decrease in HZ hospitalization rate was observed between 2003 and 2018 [26]. The authors hypothesized that changes in hospitalization criteria, directing people towards primary healthcare, may have led to this decrease. Prospective studies conducted in Spain and Germany, including GP offices and primary care centers, showed low hospitalization rates, suggesting that in these countries, a significant proportion of patients with HZ are treated in the outpatient setting [27, 28].
Some limitations of this study are inherent because of the nature of a passive surveillance system, particularly for non-mandatory notifiable diseases. As discussed above, factors like underreporting, misdiagnosis, and under-ascertainment (cases not seeking healthcare [29]) add a degree of underestimation when attempting to estimate a “true” population-wide incidence and mortality of HZ. However, these surveillance data sources are often the most reliable and complete databases for most national retrospective disease evaluations. To improve understanding of the HZ-related healthcare burden in Mexico, prospective surveillance studies are needed to collect incidence of HZ and associated HCRU in both the hospital and the GP setting.
Despite the uncertainty regarding HZ incidence rate in Mexico, our study highlights that HZ remains a concern, especially in the older population, which bears the largest disease burden in terms of complications and deaths. Demographic projections taking into account the longer life expectancy of the Mexican population predict an increase in median age and in the proportion of people aged > 60 years, with more than 30% belonging to this category by 2055 [17, 18]. Prospective studies including both primary and secondary healthcare may be informative to obtain a more realistic picture of the burden of HZ and HCRU pattern in Mexico. Vaccination programs against HZ could protect older age groups effectively and reduce the burden of disease associated with HZ, which is of particular interest in the context of a demographic shift towards older age groups.
Conclusion
The burden of disease due to HZ and associated HCRU is highest in older age groups. Active surveillance studies are needed to obtain an accurate estimate of the HZ incidence in Mexico and evaluate the potential impact of HZ in an ageing population. Prevention of HZ through vaccination may be an approach to reduce the burden of disease and HCRU, as it could prevent ER visits, hospitalizations, and HZ-related complications.
References
Gershon AA, Breuer J, Cohen JI, et al. Varicella zoster virus infection. Nat Rev Dis Primers. 2015;1:15016.
Conde-Glez C, Lazcano-Ponce E, Rojas R, et al. Seroprevalences of varicella-zoster virus, herpes simplex virus and cytomegalovirus in a cross-sectional study in Mexico. Vaccine. 2013;31(44):5067–74.
Gerada C, Campbell TM, Kennedy JJ, et al. Manipulation of the innate immune response by varicella zoster virus. Front Immunol. 2020;11:1.
Sorel O, Messaoudi I. Varicella virus-host interactions during latency and reactivation: lessons from simian varicella virus. Front Microbiol. 2018;9:3170.
Yawn B, Gilden D. The global epidemiology of herpes zoster. Neurology. 2013;81:928–30.
Kawai K, Gebremeskel BG, Acosta CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective. BMJ Open. 2014;4(6): e004833.
van Oorschot D, Vroling H, Bunge E, Diaz-Decaro J, Curran D, Yawn B. A systematic literature review of herpes zoster incidence worldwide. Hum Vaccine Immunother. 2021;17(6):1714–32.
Bardach AE, Palermo C, Alconada T, et al. Herpes zoster epidemiology in Latin America: a systematic review and meta-analysis. PLoS ONE. 2021;16(8): e0255877.
Varghese L, Standaert B, Olivieri A, Curran D. The temporal impact of aging on the burden of herpes zoster. BMC Geriatr. 2017;17(1):30.
Nagel MA, Gilden D. Neurological complications of varicella zoster virus reactivation. Curr Opin Neurol. 2014;27(3):356–60.
Johnson RW, Alvarez-Pasquin MJ, Bijl M, et al. Herpes zoster epidemiology, management, and disease and economic burden in Europe: a multidisciplinary perspective. Ther Adv Vaccines. 2015;3(4):109–20.
García-González AI, Rosas-Carrasco O. Herpes zoster (HZ) and postherpetic neuralgia (PHN) in the elderly: particularities in prevention, diagnosis and treatment [Herpes zoster (HZ) y neuralgia posherpética (NPH) en el adulto mayor: particularidades en la prevención, el diagnóstico y el tratamiento]. Gac Med Mex. 2017;153:92–101.
Volpi A. Severe complications of herpes zoster. Herpes. 2007;14:35–9.
Meyers JL, Candrilli SD, Rausch DA, Yan S, Patterson BJ, Levin MJ. Costs of herpes zoster complications in older adults: a cohort study of US claims database. Vaccine. 2019;37(9):1235–44.
Gater A, Abetz-Webb L, Carroll S, Mannan A, Serpell M, Johnson R. Burden of herpes zoster in the UK: findings from the zoster quality of life (ZQOL) study. BMC Infect Dis. 2014;14:402.
Yawn B, Saddier P, Wollan PC, St Sauver JL, Kurland MJ, Sy LS. A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction. Mayo Clin Proc. 2007;82(11):1341–9.
World Population Review. Mexico population 2019. https://worldpopulationreview.com/countries/mexico-population. Accessed 21 Sept 2022.
Vazquez M, Cravioto P, Galvan F, Guarneros D, Pastor VH. Varicella and herpes zoster: challenges for public health. Salud Publ Mex. 2017;59(6):650–6.
Secretaria de Salud (SS). Hospital discharges, emergencies and deaths - dynamic cubes [Egresos Hospitalarios, Urgencias y Defunciones. Cubos dinámicos] Mexico. http://www.dgis.salud.gob.mx/contenidos/basesdedatos/BD_Cubos_gobmx.html. Accessed 28 June 2021. (The link is only accessible in Mexico).
CONAPO. Projections of the population of Mexico and the federal entities, 2016–2050 [Proyecciones de la Población de México y de las Entidades Federativas, 2016–2050]. https://datos.gob.mx/busca/dataset/proyecciones-de-la-poblacion-de-mexico-y-de-las-entidades-federativas-2016-2050. Accessed 28 June 2021.
Chlibek R, Pauksens K, Rombo L, et al. Long-term immunogenicity and safety of an investigational herpes zoster subunit vaccine in older adults. Vaccine. 2016;34(6):863–8.
Opstelten W, Van Essen G, Schellevis F, Verheij T, Moons K. Gender as an independent risk factor for herpes zoster: a population-based prospective study. Ann Epidemiol. 2006;16(9):692–5.
Ortiz-Covarrubias A. Measurement of the burden, resources use and health costs associated with herpes zoster and post-herpetic neuralgia in Mexico. Master study. Value Health. 2015;18(7):PA870. https://doi.org/10.1016/j.jval.2015.09.009.
Chen MH, Wei HT, Su TP, et al. Risk of depressive disorder among patients with herpes zoster: a nationwide population-based prospective study. Psychosom Med. 2014;76(4):285–91.
Rampakakis E, Pollock C, Vujacich C, et al. Economic burden of herpes zoster (“culebrilla”) in Latin America. Int J Infect Dis. 2017;58:22–6.
Amodio E, Marrella A, Casuccio A, Vitale F. Decline in hospitalization rates for herpes zoster in Italy (2003–2018): reduction in the burden of disease or changing of hospitalization criteria? Aging Clin Exp Res. 2022;34:881–6.
Schmidt-Ott R, Schutter U, Simon J, et al. Incidence and costs of herpes zoster and postherpetic neuralgia in German adults aged >/=50 years: a prospective study. J Infect. 2018;76(5):475–82.
Cebrián-Cuenca AM, Díez-Domingo J, San-Martín-Rodríguez M, Puig-Barberá J, Navarro-Pérez J. Epidemiology and cost of herpes zoster and postherpetic neuralgia among patients treated in primary care centres in the Valencian community of Spain. BMC Infect Dis. 2011;11(302). https://doi.org/10.1186/1471-2334-11-302.
Gibbons CL, Mangen M-JJ, Plass D, et al. Measuring underreporting and under-ascertainment in infectious disease datasets: a comparison of methods. BMC Public Health. 2014;14(1):147.
Acknowledgements
Funding
This work was supported by GlaxoSmithKline Biologicals SA. GlaxoSmithKline Biologicals SA was involved in all stages of study conduct, including analysis of the data. GlaxoSmithKline Biologicals SA also took charge of all costs associated with the development and publication of this manuscript, including the journal’s Rapid Service.
Medical Writing and Editorial Assistance
The authors would also like to thank Business & Decision Life Sciences platform for editorial assistance and manuscript coordination, on behalf of GSK. Katrin Spiegel provided writing support on behalf of GSK. The authors would like to thank Angel Flores for his contributions to this study.
Author Contributorship
AGH: Conceptualization (equal); methodology (lead); formal analysis (lead); interpretations (supporting); writing—original draft (supporting); writing—review and editing (equal). MYCA: Conceptualization (equal); interpretations (supporting); writing—review and editing (equal). JCT: Interpretations (supporting); writing—review and editing (equal). GHG: Conceptualization (equal); formal analysis (supporting); interpretations (supporting); writing – original draft (supporting); writing – review and editing (equal).
Prior Presentation
The results of this manuscript were previously presented at the 5th GeriatrIMSS congress held virtually, from 22 to 24 September 2021.
Disclosures
GHG, MYCA, and AGH are employed by GSK. GHG, MYCA, and AGH hold shares in GSK. GHG, MYCA, and AGH declare no other financial and non-financial relationships and activities. JCT declares no financial and non-financial relationships and activities and no conflicts of interest.
Compliance with Ethics Guidelines
This noninterventional, retrospective study was based on anonymized data extracted from public sources. According to national regulations, this study did not require informed consent nor approval by ethics committee.
Data Availability
The data used for this study were extracted from the national surveillance database of the Ministry of Health via dynamic cubes, which can be freely accessed within Mexico under the following link: http://www.dgis.salud.gob.mx/contenidos/basesdedatos/BD_Cubos_gobmx.html. The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Guzman-Holst, A., Cervantes-Apolinar, M.Y., Favila, J.C.T. et al. Epidemiology of Herpes Zoster in Adults in Mexico: A Retrospective Database Analysis. Infect Dis Ther 12, 131–141 (2023). https://doi.org/10.1007/s40121-022-00692-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-022-00692-y